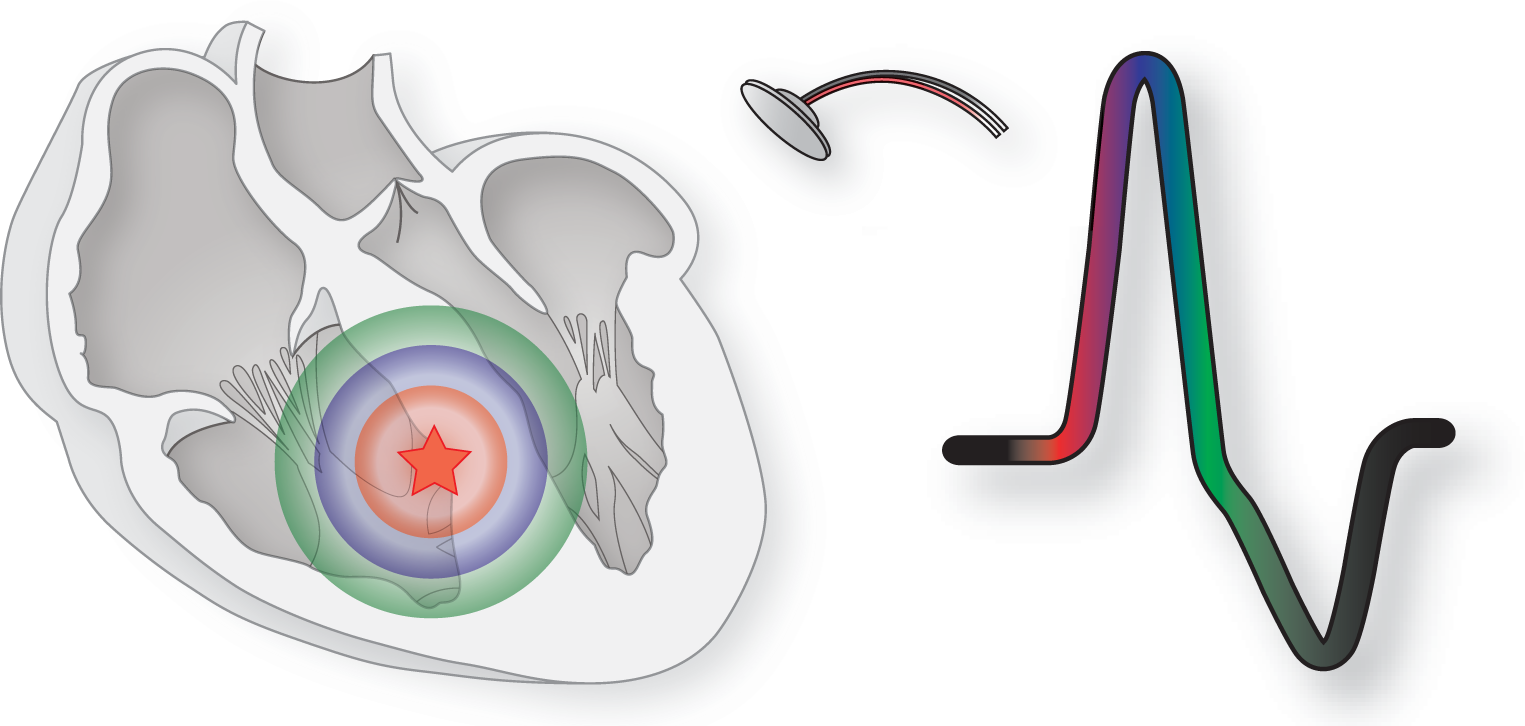
As mentioned previously, the typical form of transmission of the ventricular impulse is by direct cell-to-cell contact. As you can see in Figure 29-1, as the impulse spreads, it forms bioelectrical energy that is picked up by the ECG leads and begins to form the electrocardiographic pattern for that particular ectopic focus. The site of the ectopic focus is one of the main determinants of morphology in a ventricular complex.
Figure 29-1 An irritable focus, represented by the red star, acts as a pacemaker and causes an impulse to occur. This gives rise to a depolarization wave that radiates outward by direct cell-to-cell transmission until all of the ventricles are depolarized. Note the color-coded sections of the depolarization wave and the complex.
Therefore, the first determinant of a ventricular depolarization is that the QRS complexes will be greater than or equal to 0.12 seconds (or three little blocks) and wide and bizarre in appearance. The “greater than” part of that statement is very critical to keep in mind because these complexes can be very, very wide. Many times ventricular complexes are even wider than 0.20 seconds. In general, ventricular depolarizations that originate in the ventricular myocardium and spread by direct cell-to-cell transmission only will tend to be in the wider end of the spectrum. Ventricular depolarizations that have some transmission through the electrical conduction system will tend to be toward the narrower end of the spectrum.
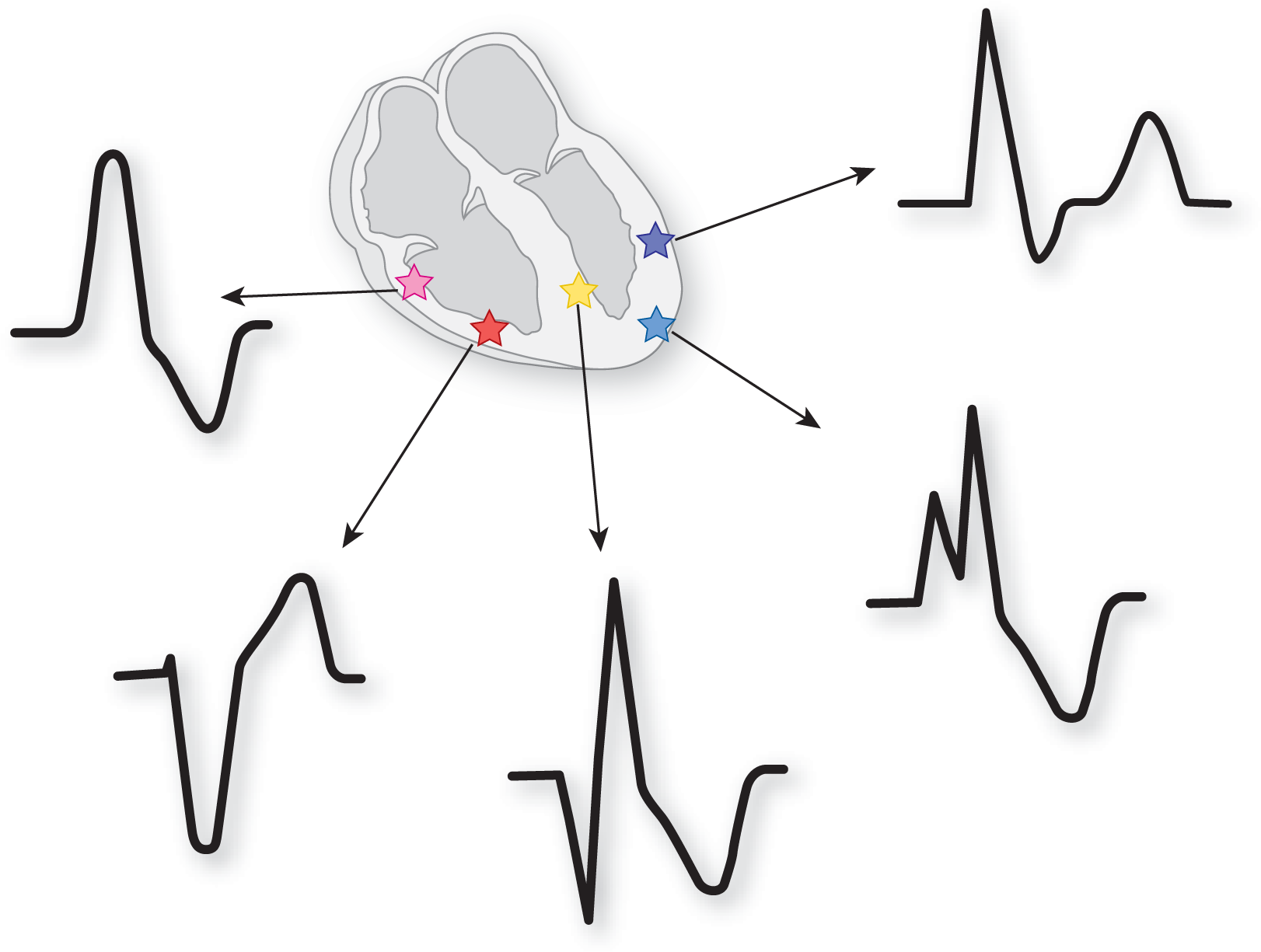
The ventricular QRS complexes are bizarre in appearance because of the delay caused by the direct cell-to-cell depolarization waves that form them and because of the atypical routes of ventricular depolarization that are taken by these waves. The vectors that are formed by these spreading waves are always abnormal; therefore, they give rise to abnormal patterns on the ECG (Figure 29-2). (It is interesting to note that one ectopic focus can lead to many different morphologic presentations depending on the route taken outward from the site. For example, on one complex the route may start off spreading superiorly, while on the next complex the route may start off inferiorly. Both of those presentations will lead to remarkably different morphologies on the ECG.)
Figure 29-2 The firing of a ventricular ectopic focus leads to the formation of wide, bizarre-looking QRS complexes. The Figure shows various types of possible QRS morphologies, but the actual appearance of a QRS cannot be predicted completely based on the location of the ectopic focus. In addition, the morphology will change based on the lead used to view the complexes.
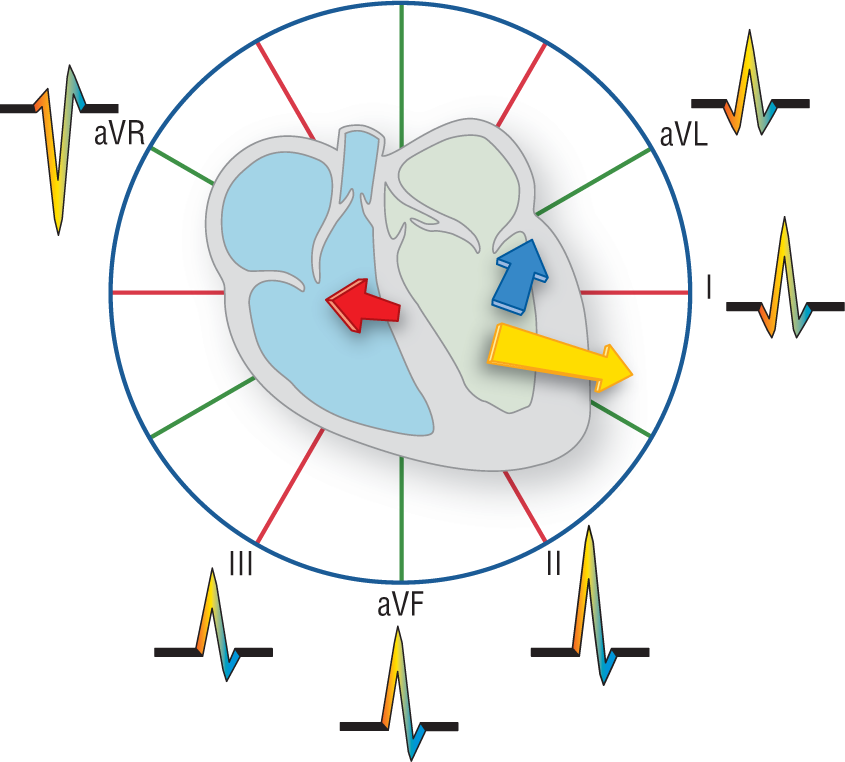
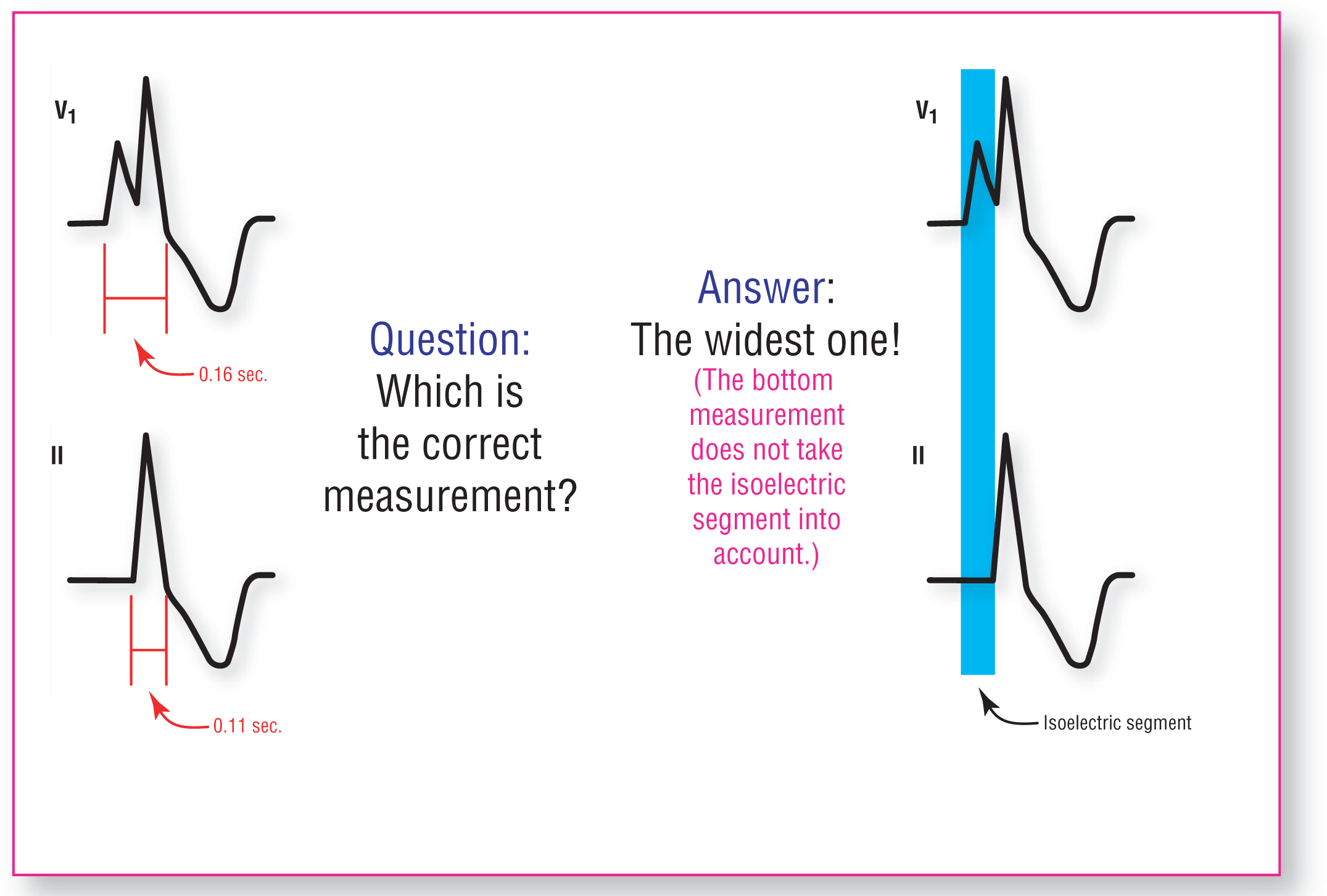
Another factor that can drastically alter the morphology of a ventricular complex is the lead in which you view it. If you remember from Chapter 4, Vectors and the Basic Beat, leads are like cameras taking “pictures” of the vectors from their particular vantage point (Figure 29-3). Depending on the vantage point, the same complex can appear markedly different. In addition, isoelectric segments may actually lead to errors in the correct determination of a complex’s true width (Figure 29-4). Multiple leads will greatly improve the accuracy of your measurement. Always remember to use the widest complex to take your measurements (thereby avoiding the mistake of not including isoelectric segments into your measurement).
Figure 29-3 The same complex can appear drastically different based on which lead it is viewed in.
Figure 29-4 The same complex can have different widths due to isoelectric segments that can develop in certain leads. But, remember, interval widths are actually the same in every lead! Get used to always measuring the widest interval—it is the true interval without any isoelectric segments.
In a ventricular complex, the ST segment and T waves will always be abnormal and often may be inverted, elevated, or depressed. This occurs because of abnormal patterns of repolarization associated with these complexes. Why this occurs is a topic for a book on electrocardiography. For a further discussion of the topic, see 12-Lead ECG: The Art of Interpretation by Garcia.