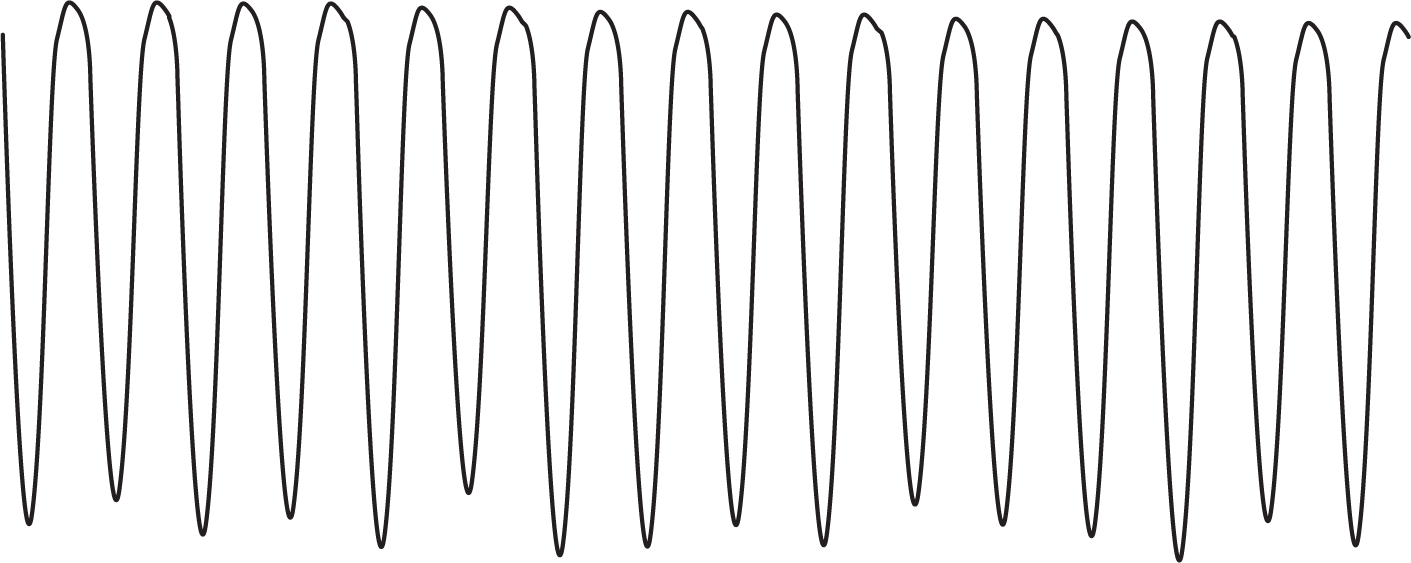
Figure 32-20 An episode of ventricular flutter. Note that the morphology of the various components of the complexes is lost and the rhythm almost becomes sinusoidal in nature.
© Jones & Bartlett Learning.
When an episode of VTach comes so fast as to obscure the morphology of the individual waves and segments (QRS, ST segment, and T wave), it is known as ventricular flutter (Figure 32-20). At this point, the rhythm resembles a very fast sinusoidal pattern.
Figure 32-20 An episode of ventricular flutter. Note that the morphology of the various components of the complexes is lost and the rhythm almost becomes sinusoidal in nature.
© Jones & Bartlett Learning.
The rates at which the morphologic features become blurred vary depending on the patient and the clinical scenario. The typical rate at which the blurring occurs is usually above 200 BPM. However, the ventricular rates are found at rates from 150 to 300 BPM (most commonly between 235 and 250 BPM). Rates above 250 BPM are uncommon, and when they occur, should raise the suspicion of an accessory pathway being involved.
Clinical manifestations are the same as for sustained VTach, but the patients are typically more unstable because of the higher rates. Once again, pharmaceutical intervention should take the possibility of accessory pathways into consideration. If the patient is hemodynamically unstable, electrical cardioversion or defibrillation is strongly recommended.
ARRHYTHMIA RECOGNITION
Monomorphic Ventricular Tachycardia
| Rate: | 100 to 250 BPM |
| Regularity: | Regular (may be slightlyirregular at onset) |
| P wave:
Morphology: Upright in II, III, and aVF: |
Retrograde or in AV dissociation
Variable Variable |
| P:QRS ratio: | None |
| PR interval: | Variable, if present |
| QRS width: | ≥ 0.12 seconds |
| Grouping: | None |
| Dropped beats: | None |
DIFFERENTIAL DIAGNOSIS
Monomorphic Ventricular Tachycardia
This list is not inclusive but reflects the most common causes of the rhythm disturbance.