
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
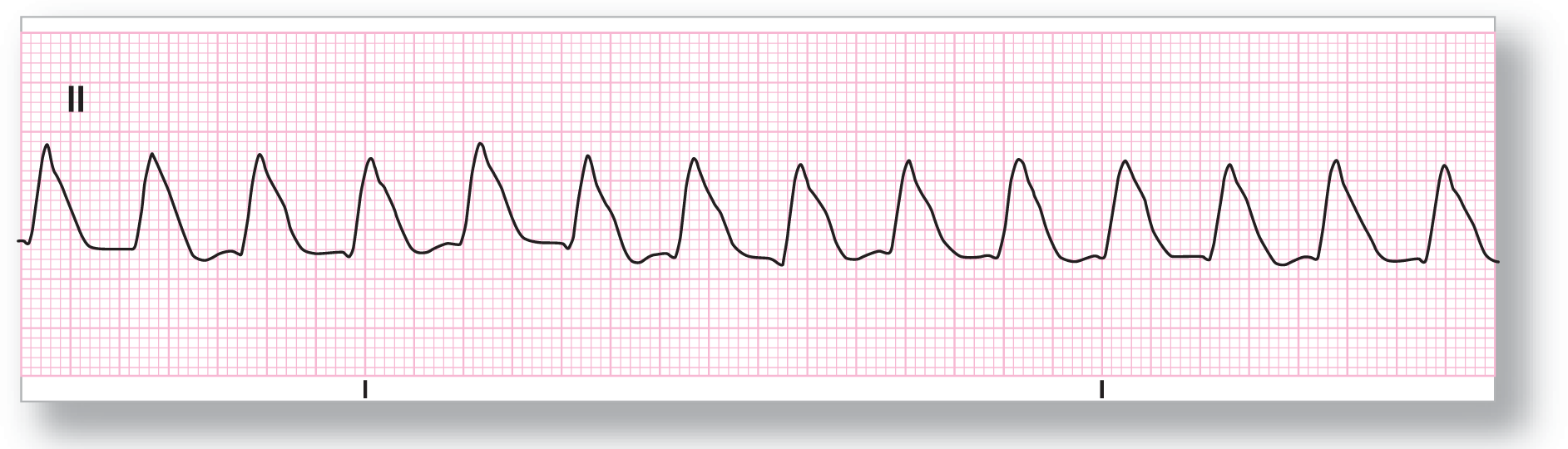
Rate: About 200 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-1 shows a wide-complex tachycardia at about 200 BPM. The rhythm is very regular and all of the complexes are almost identical morphologically. This is an example of VTach. This could easily be labeled ventricular flutter, and you would not be wrong. The reason that ventricular flutter is not completely correct is that there is still some semblance of demarcation between the QRS complexes and the ST segments and T waves (although this is debatable).
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-2 shows a wide-complex tachycardia clipping along at about 135 BPM. The morphology of the QRS complexes is definitely wide, even though there appears to be some fusing with the elevated ST segments. Indeed, the patient was having a large AMI. There are no discernible P waves noted. A 12-lead ECG would be invaluable in further diagnosing the rhythm and in evaluating the AMI that appears to be present on this strip.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 140 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-3 shows a wide-complex tachycardia at about 140 BPM. The blue arrow is pointing toward a constant irregularity in the morphology of the S wave. This irregularity could be a retrograde inverted P wave or it could be part of the morphologic features of the S wave itself. It is unclear from this strip. Perhaps a 12-lead ECG could shed some light on this issue. There is no evidence of AV dissociation present on the strip.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 112 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-4 is also a wide-complex tachycardia. This time, the rate is around 112 BPM and there are no obvious P waves. Remember, a wide-complex tachycardia is VTach until proven otherwise! VTach is the working diagnosis. Other possibilities for this strip include a junctional tachycardia in a patient with a preexisting bundle branch block or in a patient with some aberrancy. An old ECG or rhythm strip while the patient was in sinus rhythm would be very helpful in establishing the definitive diagnosis.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 115 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
Here is another example of VTach until proven otherwise. ECG 32-5 shows a wide-complex tachycardia at about 115 BPM. Take a close look at the end of the T wave. Notice that there is a slight bump (see blue arrow). Double-humped T waves are not very common and this could represent a P wave with a prolonged PR interval. But, since VTach is the diagnosis of exclusion, you should continue the treatment strategy along those lines. This was VTach. A 12-lead ECG is very helpful in these cases.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 150 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-6 is a wide-complex tachycardia at about 150 BPM. Always think of atrial flutter when the ventricular rate is 150 BPM. There is no evidence for atrial flutter in this strip. Notice, however, that most of the complexes have a very definite hump in the downstroke of the S wave (see blue arrow). Could this be a Josephson’s sign? Probably, because it is seen on almost every complex. If it only recurred on a regular pattern, such as every third or fourth complex, then it would probably be a sign of AV dissociation.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
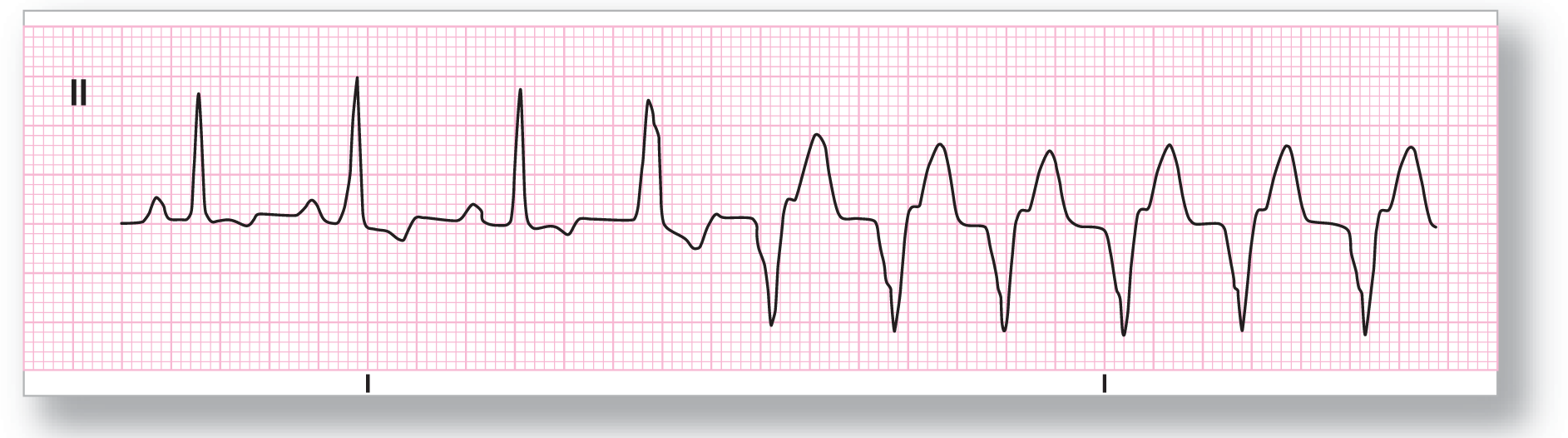
Description|
Rate: See discussion below |
PR intervals: Normal |
|
Regularity: See discussion below |
QRS width: See discussion below |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: 1:1 in beginning |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-7 starts out as a normal sinus complex. The second complex shows some mild aberrancy with some slurring at the onset. The third complex appears to be sinus. The fourth complex is a PVC or an aberrantly conducted premature junctional contraction. This starts a run of a wide-complex tachycardia at about 120 BPM. There are no obvious P waves or irregularities that could represent P waves with AV dissociation on this part of the strip. Each of the complexes is nearly identical in morphology. This is a monomorphic VTach triggered by a premature complex, either ventricular or junctional.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
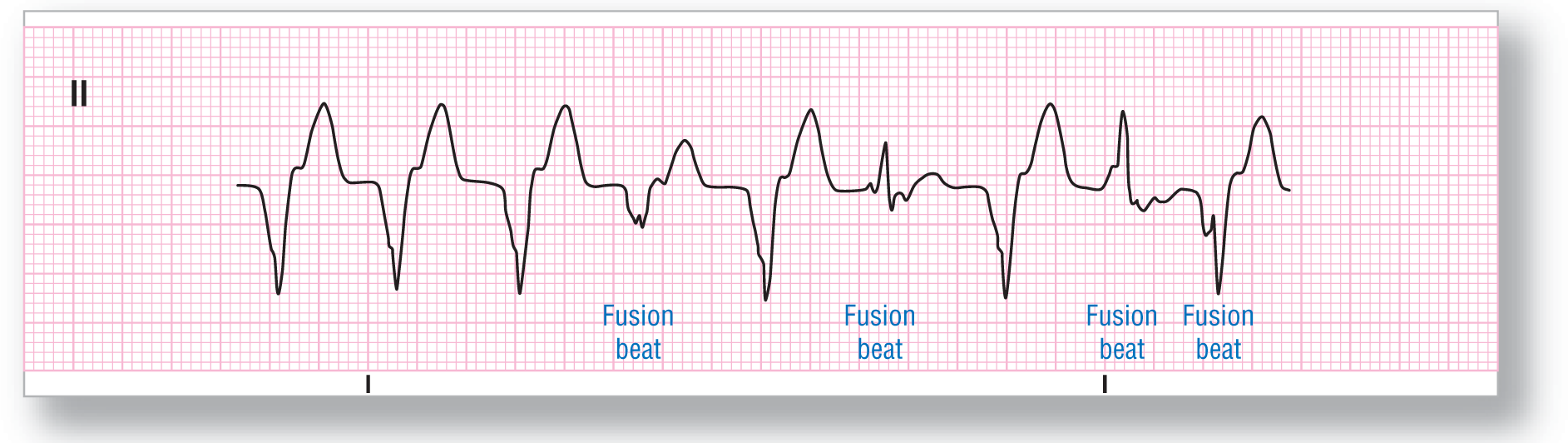
Rate: About 115 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-8 is a continuation of the preceding strip. Note that there are different morphologies for the complexes in the latter two-thirds of the strip. These are fusion complexes interspersed among the monomorphic complexes. This is indirect evidence of AV dissociation. We attempted to map out the P-P interval above throughout the strip, but there were no associated “bumps” in the area. However, the presence of fusion beats is clear evidence of the presence of AV dissociation.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
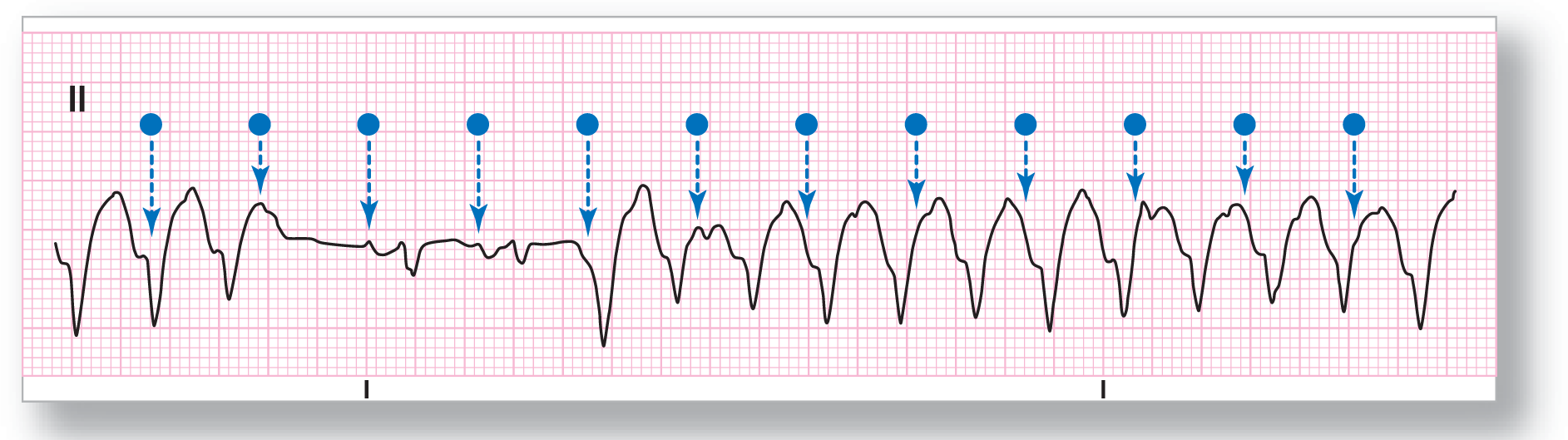
Rate: About 190 BPM |
PR intervals: None |
|
Regularity: See discussion below |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular tachycardia |
Discussion:
ECG 32-9 shows a wide-complex tachycardia at about 190 BPM. There are some fusion beats present and obvious AV dissociation. Here is how you should approach the AV dissociation. Place the pins on your calipers over the two obvious P waves (third and fourth blue dots). Now, just walk your calipers in both directions, noting any irregularities in the complexes below. The presence of fusion of the P waves with the underlying complex will be apparent.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 215 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Ventricular flutter |
Discussion:
ECG 32-10 shows a rapid, wide-complex rhythm with a sinusoidal pattern. All of the waves are nearly morphologically identical. This is a very rapid monomorphic VTach. The loss of the morphologic identity of each of the components of the complex makes the more accurate diagnosis ventricular flutter.