From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
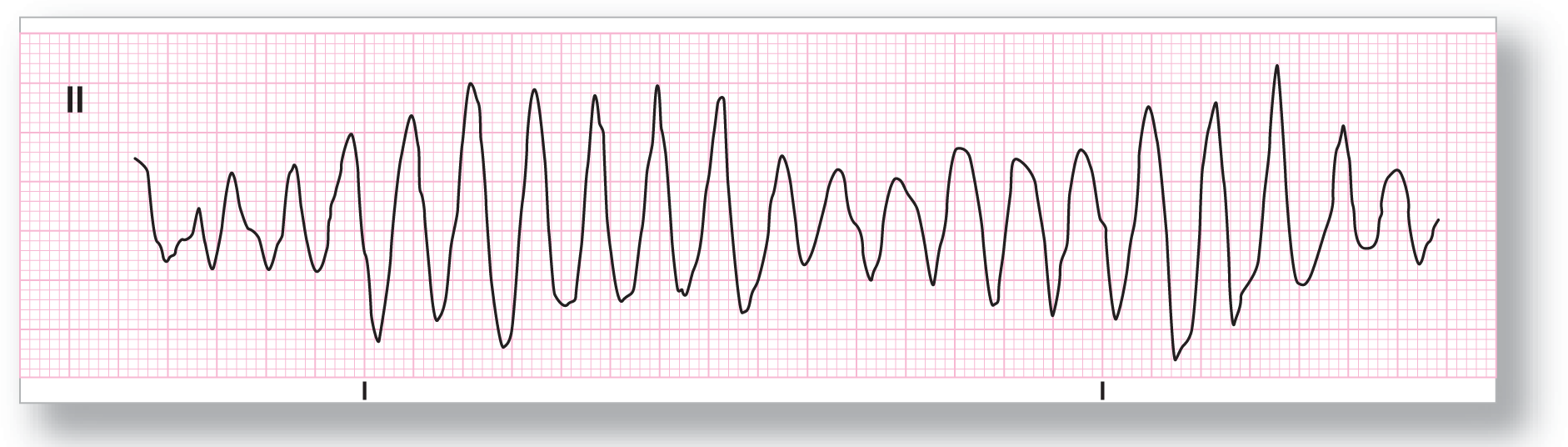
Rate: About 250 BPM |
PR intervals: None |
|
Regularity: Irregular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: Ventricular complexes |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Torsade de pointes |
Discussion:
ECG 33-1 shows the typical undulating pattern that is classic for torsade de pointes. The rate varies from beat-to-beat as expected from a completely irregular rhythm. Note the morphology differences between most of the complexes. The morphology varies not only in amplitude and polarity, but also in the actual makeup of each of the ventricular complexes.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
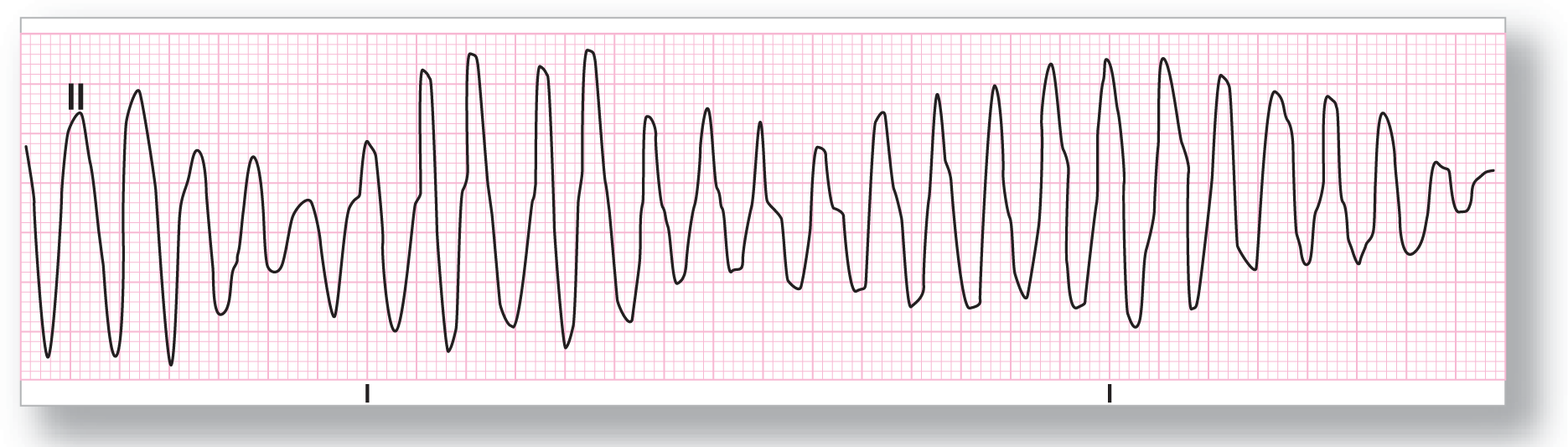
Rate: About 170 BPM |
PR intervals: None |
|
Regularity: Irregular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: Yes |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Torsade de pointes |
Discussion:
ECG 33-2 also shows the same undulating pattern that is classic for torsade. In this example, the polarity of the two groups is very evident, with the group on the left showing a negative polarity (the QRS complexes are negative and point downward), while the group on the right shows a positive polarity (the QRS complexes are positive and point upward).
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 260 to 280 BPM |
PR intervals: None |
|
Regularity: Irregular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: Ventricular complexes |
|
Dropped beats: Absent |
|
|
P:QRS ratio: None |
Rhythm: Torsade de pointes |
Discussion:
This is another classic example of torsade de pointes. Once again, the morphologic differences mentioned previously are also applicable to ECG 33-3. Note that the number of complexes in each group can vary and is a normal finding in almost all strips showing torsade.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: See discussion |
PR intervals: See discussion |
|
Regularity: Irregular |
QRS width: Variable |
|
P waves: Present at start Morphology: Normal Axis: Upright |
Grouping: None |
|
Dropped beats: Absent |
|
|
P:QRS ratio: See discussion |
Rhythm: Torsade de pointes |
Discussion:
ECG 33-4 shows a patient who is having a run of bigeminy. It is unclear from this strip if the bigeminy is composed of premature junctional complexes or PVCs, because we do not see the start of the complex. The patient then begins to show a very rapid, irregular rhythm. At this point, an argument can be made as to whether this is VTach or torsade de pointes. This is because the rate is very, very fast—greater than 300 BPM in some places. Additional leads demonstrated a more traditional torsade pattern that, as mentioned, is not clearly apparent on this strip.