There are quite a large number of criteria that have been developed to help us differentiate between VTach and the SVTs-A in the literature. For this text, we will concentrate on two of the major criteria or algorithms that are in common use today clinically: the Brugada criteria9 and the Vereckei aVR criteria.10 Both of them apply four simple questions or observations. The idea is to answer them sequentially so that any positive answer will make the diagnosis of VTach most likely. If all are negative, then the rhythm would be consistent with an SVT-A.
The Brugada Algorithm
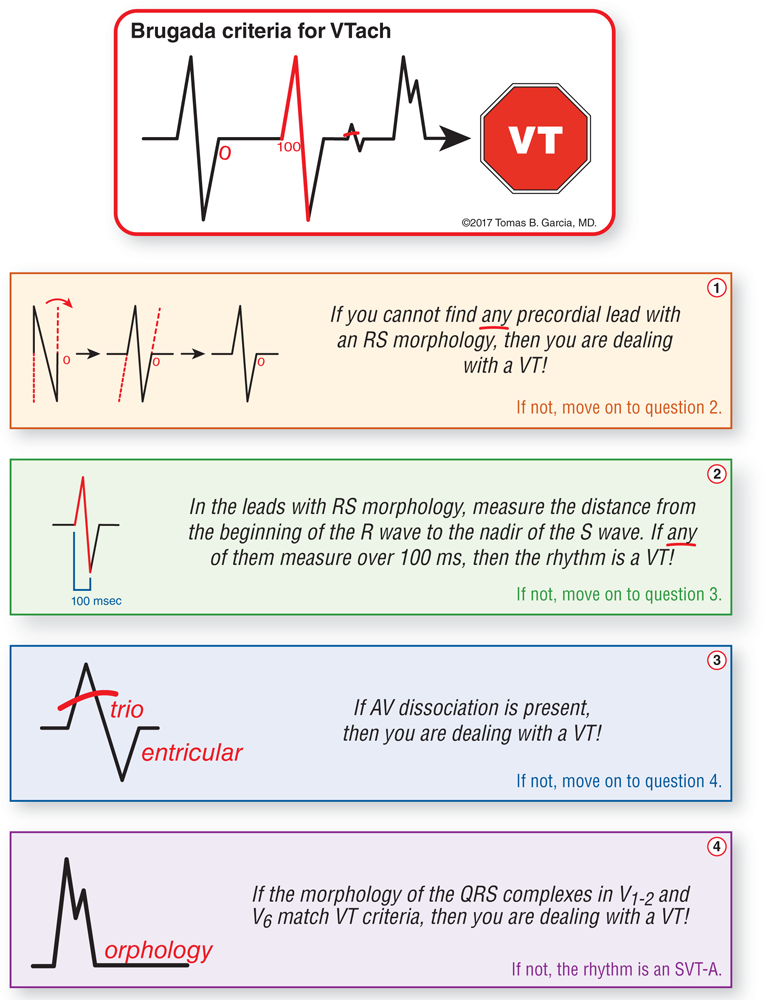
The Brugada algorithm9 was first published in 1991 and is the most commonly known and used of the algorithms today. It evaluates four decision points:
Look for RS complexes in all the precordial leads. If you cannot find any precordial lead with RS morphology, then you are dealing with a VTach! If not, move on to question 2.
Remember, an RS complex has both a significant R wave and a significant S wave. Other wave combinations like QR, QS, monophasic R, rSR′, or even QRS complexes should not be considered RS complexes.
Observation 1 states very clearly that you need to examine every single precordial lead for the presence of an RS-wave morphology. If you cannot find the RS morphology in any of them, then you are looking at a nearly 100% chance that it is VTach. You need to be very clear on these points since they are a major source of error in dealing with this criterion. You are looking for the complete absence of any RS complexes anywhere in the precordial leads!
If conduction or partial conduction occurs through the HPS, at least one precordial lead will show RS-complex morphology. This is because the six precordial leads are arranged in such a way that there is a transition from anterior to posterior somewhere among them. The leads around this transition will typically be RS waves. The QRS complexes in VTachs, however, do not need to form RS complexes. Thus, the absence of an RS in any precordial lead would point heavily toward a diagnosis of VTach. This presentation occurs in 15% of VTachs, but it has a specificity of 100%.
As a final comment, please note that we are talking about a morphologic appearance that is found throughout an entire lead and not one that affects just a single complex. Single complexes with RS morphology could represent a PVC or an aberrantly conducted supraventricular beat.
In the leads with RS morphology, measure the distance from the beginning of the R wave to the nadir of the S wave (the RS interval). Do any of them measure over 100 ms (or 2½ small blocks)? If any of them measure over 100 ms, then the rhythm is a VTach. If not, move on to question 3.
The RS interval is considered to be that distance from the beginning of the R wave to the nadir (or lowest point) of the S wave. This is, in our opinion, a very confusing term, since most people would think that the RS interval would be from the start of the R wave to the end of the S wave. For that reason, we have simplified some of the wording.
Speaking of wording, the original wording asks you to measure the RS interval of the widest lead with RS morphology. However, this just requires you to invest more memory power trying to remember these criteria correctly. Common sense dictates that if any of the RS intervals measure over 100 ms, then either it is the widest one or the widest one is going to be even wider than the one you are measuring. In either case, just look at the RS intervals in leads with RS morphology present; if any of them are wider than 2½ small blocks, you have VTach. This can be determined with a quick eyeballing of the precordial leads, or remember that calipers can make your life a lot easier when evaluating intervals of any kind.
If any of the RS intervals are greater than 100 ms, you have 98% specificity that you are dealing with a VTach. In other words, you are 98% sure that you are dealing with a VTach.
Look for evidence of AV dissociation. If there is AV dissociation, then it is a VTach. If not, move on to question 4.
As we discussed earlier, the presence of AV dissociation makes us almost 100% sure that we are dealing with a VTach. Just in case you need a refresher, we covered AV dissociation in Chapter 32, Ventricular Tachycardia, and in an earlier part of this chapter.
Look at the morphology of the rhythm in leads V1-2and V6. If the morphologic criteria we covered previously are present in leads V1-2and V6, then it is a VTach. If not, then the answers to all four questions are negative and you are dealing with an SVT-A.
Note that the presence of more than one of the individual criteria increases the sensitivity and specificity of the presence of VTach being the culprit rhythm. Finally, take a few minutes to read the Additional Information box about the Brugada criteria. In it, we provide a graphical mnemonic to assist you in remembering these criteria quite easily. Remember, the key is not to know this information when you finish reading about it. The key is to be able to recall it and use it when you actually need it clinically. Re-review the mnemonic every couple of days for a week. If you do this, you will probably never forget it and will have a functioning knowledge of the principles involved.
Additional Information ADVANCED
The Brugada Criteria
Data from: Brugada P, Brugada J, Mont L, Smeets J, Andries EW. A new approach to the differential diagnosis of a regular tachycardia with a wide QRS complex. Circulation. 1991;83:1649-1659.
The Vereckei algorithm was first published in 2007 and then revised in 200810 in an attempt to simplify the algorithm and avoid costly mistakes. The 2008 version is also known as the Vereckei aVR algorithm10 and completely succeeded in making the criteria easier to remember and much more clinically useful. Once again, if the answer to any of the four main observations is “yes,” you can make the diagnosis of VTach. In the absence of these four criteria, the diagnosis would be an SVT-A. In the following section and in the Additional Information box, we have further simplified the language and terminology of the algorithm while maintaining the spirit intended.
One of the major drawbacks to this algorithm is that you cannot fully differentiate between VTach and an SVT-A due to conduction through an accessory pathway. However, since this is a fairly uncommon diagnosis, the algorithm is still very clinically useful.
This algorithm is near and dear to our hearts since it bases many of its elegant findings on the vectors generated by the heart. We will discuss these further under their individual headings. The four decision points involve only lead aVR and are as follows:
Do the QRS complexes in aVR begin with a large R wave? If they do, then you are dealing with a VTach! If not, move to decision point 2.
Here’s a mnemonic to help you remember:
A “big R in aVR”
Why do we get a large R wave in lead aVR? To start off with, under normal circumstances, aVR is considered to be the exact mirror image of lead aVL (when the mirror is placed along a horizontal plane). Therefore, what is positive in aVL is negative in aVR. Since aVL is usually positive, aVR is usually negative.
In VTach, the point of origin is from an ectopic ventricular focus or reentry loop. Vectors typically head upward toward aVR, causing a large positive aVR. To put it another way, a positive aVR is seen quite often in any ventricular complex, and in WCTs the odds are even greater. Note that in most SVTs, the depolarization waves typically come from above. The two main rhythms that are wide, tachycardic, and appear to be generated in the ventricles are VTach and antidromic AVRT. As a matter of fact, distinguishing between them on a 12-lead ECG is often impossible.
Looking at the Additional Information box for the Vereckei aVR algorithm, this decision point is represented by that first stick figure admiring that large, mountainous R wave.
Do the QRS complexes in aVR start off with smaller q or r waves that are over 40 ms wide (0.04 seconds, or one small block)? If they do, then the rhythm is a VTach! If not, move to decision point 3.
VTs that originate along different areas of the ventricles may produce smaller vectors that move toward or away from lead aVR. These can lead to either small q or r waves. It is important to note, however, that since they originate within the myocardium itself, their transmission occurs via the slow cell-to-cell depolarization pattern, making these smaller q or r waves wide. How wide? The criterion clearly states that they are greater than 40 ms (0.04 seconds, or one small block).
Note that the first two decision points cover the creation of the ventricular depolarization waves from anywhere within the ventricular myocardium. The exception, as noted previously, occurs when the depolarization of the ventricles is through the HPS.
This decision point is symbolically represented in the mnemonic in the Additional Information box by the stick figure jumping over the hole or bump with the help of the “small block.”
Is there a notch on the descending limb of a completely negative QS complex in lead aVR? If there is, then you are dealing with a VTach! If not, move to question 4.
In the first decision point, we saw how the location of the ectopic focus in the inferior and apical areas gives rise to large R waves in aVR. When we have the ectopic focus in the other regions of the ventricles, the vectors created by the depolarization wave will form an expanding depolarization wave front that extends in all directions from the central ectopic focus. Think of it like a pebble hitting a still pond. The wave travels outward concentrically from the point where the pebble hit the water.
Notice how this ripple effect will always create some positive-heading vectors regardless of the location of any ectopic focus outside of the inferior and apical zones. The fusion of the large vectors heading away from aVR and the small vector heading toward aVR will create either a slow, gradual negative start to the negative complexes or a notch to form in the initial descending limb. The variety in morphologies of these fused negative complexes with negative starts is actually limitless. For the sake of simplicity, we’ll take a look at some of the most common ones in the Additional Information box on the Vereckei aVR algorithm.
If the Vtis bigger in lead aVR, you have a VTach (Vi/Vt ≤ 1)! If not, you are dealing with an SVT-A.
Additional Information ADVANCED
Vereckei aVR Algorithm
Data from: Vereckei A, Duray G, Szenasi, G, Altemose GT, Miller JM. New algorithm using only lead aVR for differential diagnosis of wide QRS complex tachycardia. Heart Rhythm. 2008;5:89-98.
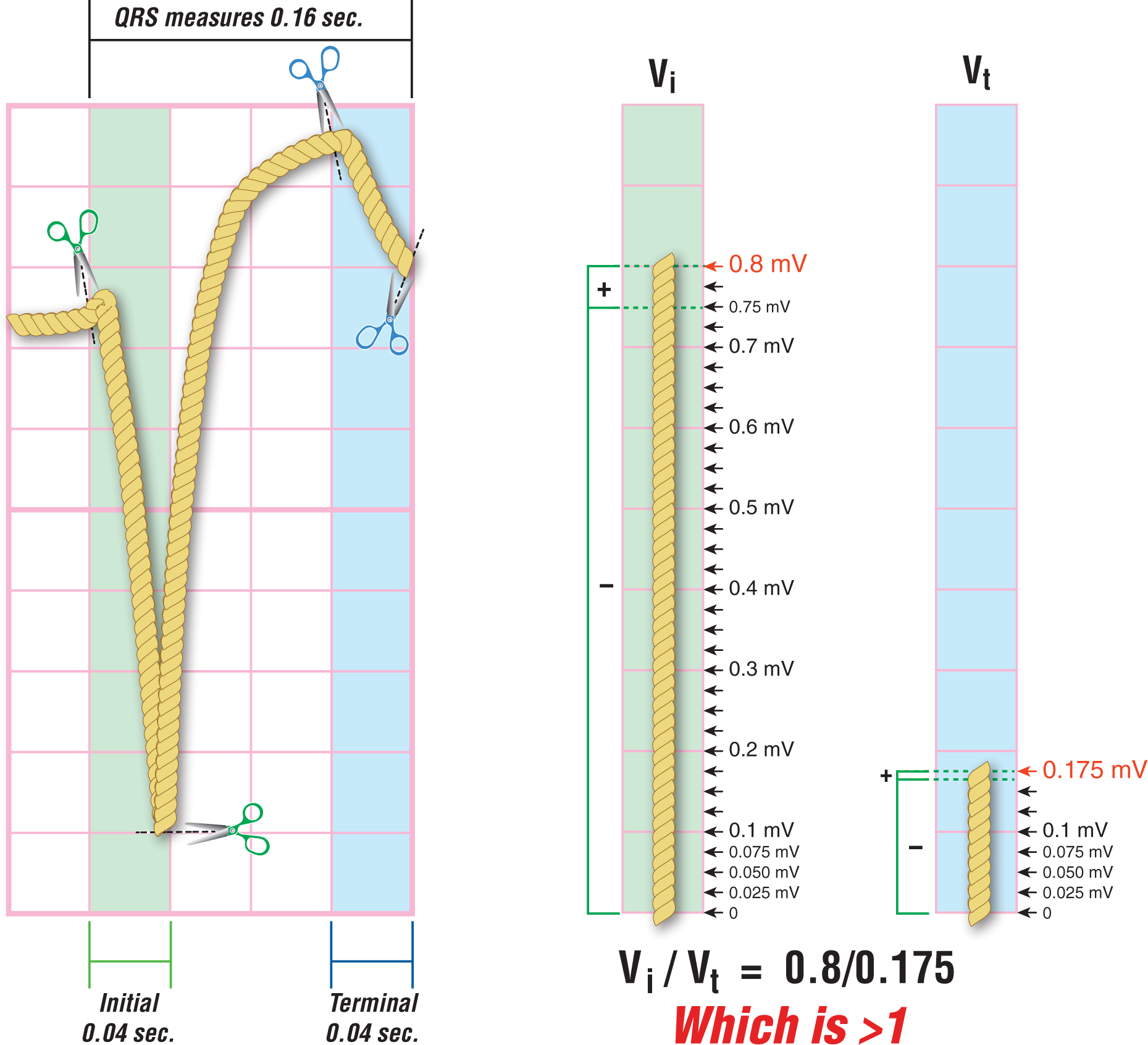
Instead of thinking of the QRS complex as a line, think of it as a rope. If you think of it as a rope, it is easier to think of cutting it at the beginning and end of the initial or terminal 0.04 seconds of the QRS complex in aVR, then stretching it out and measuring how long the rope is. This is what is meant by “calculating the absolute value of the amount traveled in the allotted space (0.04 seconds).” In other words, take out the + and – part of the number and just calculate the total measurement regardless of direction. To help you identify the initial and terminal 0.04 second intervals, in the figure, the initial 0.04 seconds is the area covered in green while the terminal 0.04 seconds is covered in blue.
To calculate the Vi, we would add the distance traveled upward (0.05 mV) in the initial 0.04 seconds to the amount traveled downward (0.750 mV). This gives us a grand total of 0.800 mV. So, Vi = 0.8 mV.
To calculate the Vt, we would add the distance traveled upward (0.010 mV) in the terminal 0.04 seconds to the amount traveled downward (0.165 mV). This gives us a grand total of 0.175 mV.
With these figures, we end up with a Vi/Vt of 0.8/0.175. Since Vi is larger than Vt in lead aVR, the mathematical result of Vi/Vt is greater than 1, making this rhythm an SVT-A. If, on the other hand, our strip showed that the Vt was larger than Vi in lead aVR, then the result of Vi/Vt would be less than 1, making this rhythm a VTach. Shortening that up, we come to our conclusion that a larger Vt = VTach.
ADVANCED
The ventricular activation velocity ratio (Vi/Vt) is the amount of vertical distance traveled by the tracing during the first 0.04 seconds, or one small block (Vi), over the distance traveled during the last 0.04 seconds (Vt) of the QRS complex in lead aVR. Officially, the measurements are calculated by taking the absolute value of the distance in millivolts (one small block is 0.1 mV high). Whether the distance traveled is positive or negative is of no significance. We are just taking the number, not the orientation of the deflection (positive and negative), to calculate the number. In addition, the number is easier to think about as a fraction rather than a long-division problem.
After having looked at the Additional Information box on calculating the Vi/Vt ratio, we know how to calculate the Vi, the Vt, and the Vi/Vt. Now, let’s figure out what we can do with it. By calculating the Vi/Vt ratio, we can figure out if we are dealing with either an SVT-A or a VTach. This is a critical concept that lies at the core of decision point 4 of the Vereckei aVR algorithm and one that we cover further in the Additional Information box on calculating the Vi/Vt.
Vi is determined by the absolute distance that the waves travel during the initial 0.04 seconds (1 small block). It doesn’t matter if the wave went up in a straight line or if it took a detour through another state, the total distance traveled during the first 0.04 seconds is the number we care about, the Vi. In SVTs and SVTs-A, ventricular depolarization occurs via the normal HPS and provides a steep angle to the rise and/or fall of the complex. In contrast, Vt may be slower than Vi and, therefore, the distance would be shorter. So, in SVTs-A, we will have a Vi/Vtratio that is greater than 1.
In VTachs, the initial depolarization spreads through direct cell-to-cell contact and the rise and/or fall of the initial component is much slower and more gradual. Afterwards, if the depolarization wave reconnects with the HPS, it may conduct the Vt faster than the initial Vi, giving us a larger number. So, in VTachs, we will have a Vi/Vtratio that is less than 1.
We can simplify all of this alphabet soup even further by just stating, “If the Vt is bigger, you have a VTach.” Why? As we saw earlier, in VTachs, the smaller Vi is over (divided by) the larger Vt, meaning that the ratio is always less than 1. In other words, the denominator (the bottom number in the fraction) will always be bigger than the numerator (the upper number in the fraction)! Try it with as many numbers as you like, the ratio is always less than 1 (1/2, 3/4, 23/67, 1,637/10,197, etc). In other words, Vi/Vt < 1 = VTach.
CLINICALPEARL
Since we didn’t make the hidden mnemonic in the fourth step of the algorithm very clear…
a bigVt = VTach
The strengths of the Vereckei aVR algorithm are in its simplicity and ease of use in clinical settings. This is especially true in the urgent and the nonurgent phases when we need to verify the diagnosis once the patient is stabilized and a long-term therapy plan is being considered. Remember, the more findings that point toward VTach as the final diagnosis, the more secure we can be in our decision.