
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 100 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
ECG 39-1 shows a paced ventricular rhythm at a rate of 100 BPM. The rhythm is very regular as you would expect with an artificial pacemaker. The pacemaker spike is obvious right before the ventricular complexes. The only troubling thing about this strip is the rate of 100 BPM, which is set very high. This could represent pacemaker malfunction. Clinical correlation is indicated.
NOTE
If you are at the beginner level, you should focus on identifying the pacer spike for the moment. Later, you can come back and identify the pacing system present.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
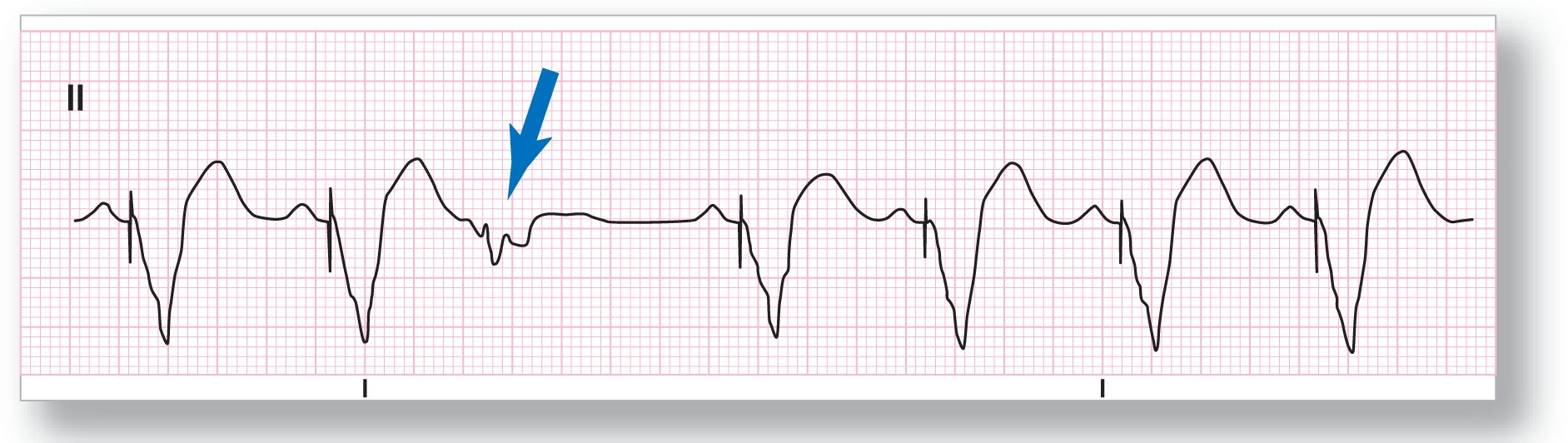
Rate: About 72 BPM |
PR intervals: None |
|
Regularity: Regularly irregular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
ECG 39-2 shows a sinus rhythm at about 72 BPM. This is obvious from the constantly recurring P waves with the same morphology. The conduction of the sinus complex to the ventricles is obviously blocked because the pacemaker has to pace the ventricles sequentially in most cases. The third complex is a PVC (see blue arrow).
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
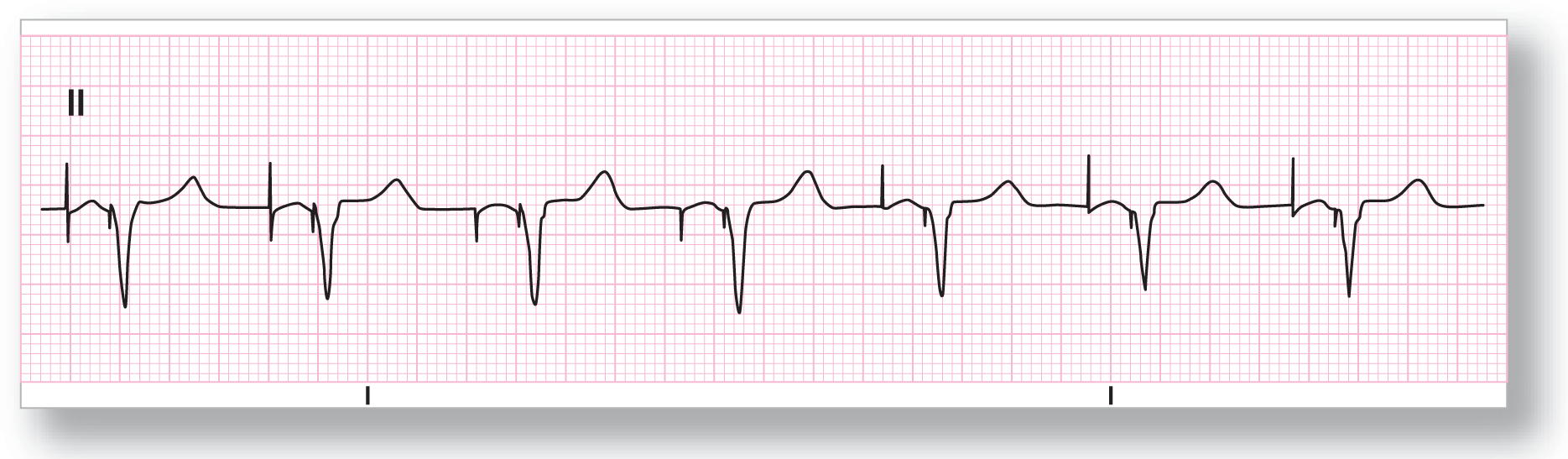
Rate: About 72 BPM |
PR intervals: None |
|
Regularity: Regularly |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
Unless you are very sure of your findings, get used to calling any paced rhythm just simply a paced rhythm. It usually doesn’t pay to try to figure out what type of pacemaker you are dealing with. ECG 39-3 shows both atrial and ventricular pacing in a sequential manner. The pacer appears to be functioning normally. Even though the ventricular complexes appear narrow, they have to be wide with isoelectric segments because they are artificially paced.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 70 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
ECG 39-4 also shows a paced rhythm with atrial and ventricular pacing in a sequential manner. The pacemaker appears to be functioning normally.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 62 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: See discussion below |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: NSR and paced rhythm |
Discussion:
ECG 39-5 shows a patient in a normal sinus rhythm that suddenly stops and is replaced by a paced ventricular rhythm. Notice that if you take the first P-P interval and transfer that exact distance to that area between the second and third complexes, you will see that just an extra 0.05 seconds is all that is needed for the pacemaker to reach the end of the escape interval and fire. This pacemaker is functioning normally.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 80 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm and PVCs |
Discussion:
ECG 39-6 shows a ventricular rhythm that is obviously paced. The pacemaker spike is very obvious in this lead, making the diagnosis simple. The second and sixth complexes are PVCs. Note the different polarity of the PVCs compared with the paced rhythm. The pacemaker is obviously inhibitory in nature since the pacer was suppressed from firing by the PVCs.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
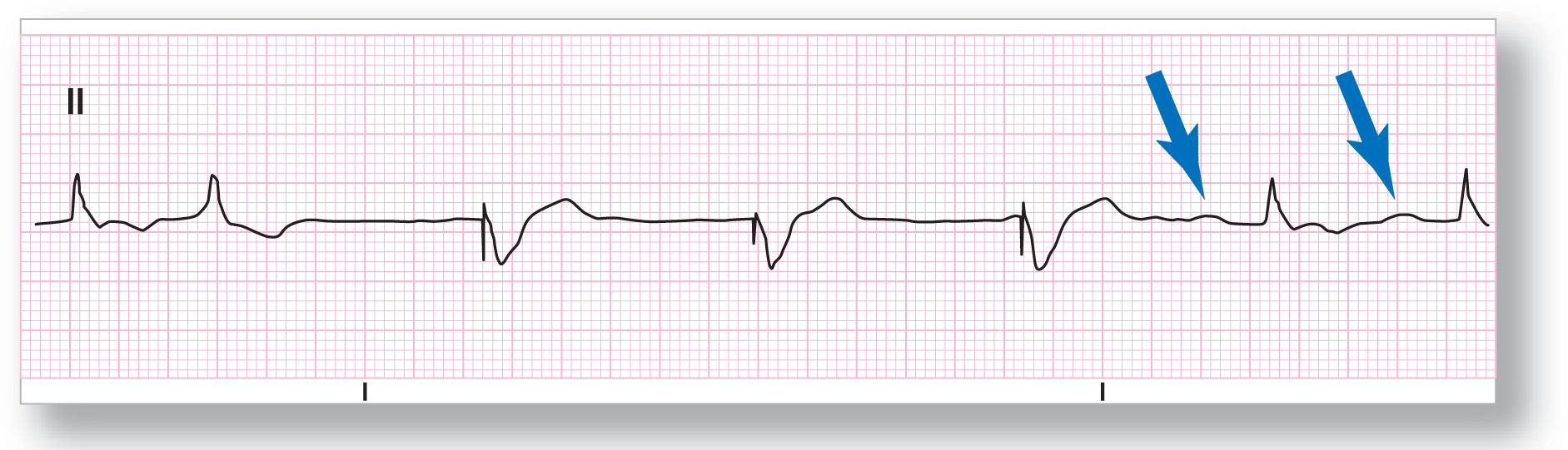
Rate: About 55 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
From ECG 39-7, it is impossible to confidently identify the first complex. The second complex, however, does not have any visible P waves and is the same morphology as the previous one and the sixth and seventh complexes in the strip. It is most probably a PJC. The third through fourth strips are obviously paced. The sixth and seventh complexes show NSR with P waves, which are fairly flat in this lead (see blue arrows). Multiple leads verified the existence of those bumps as P waves.
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
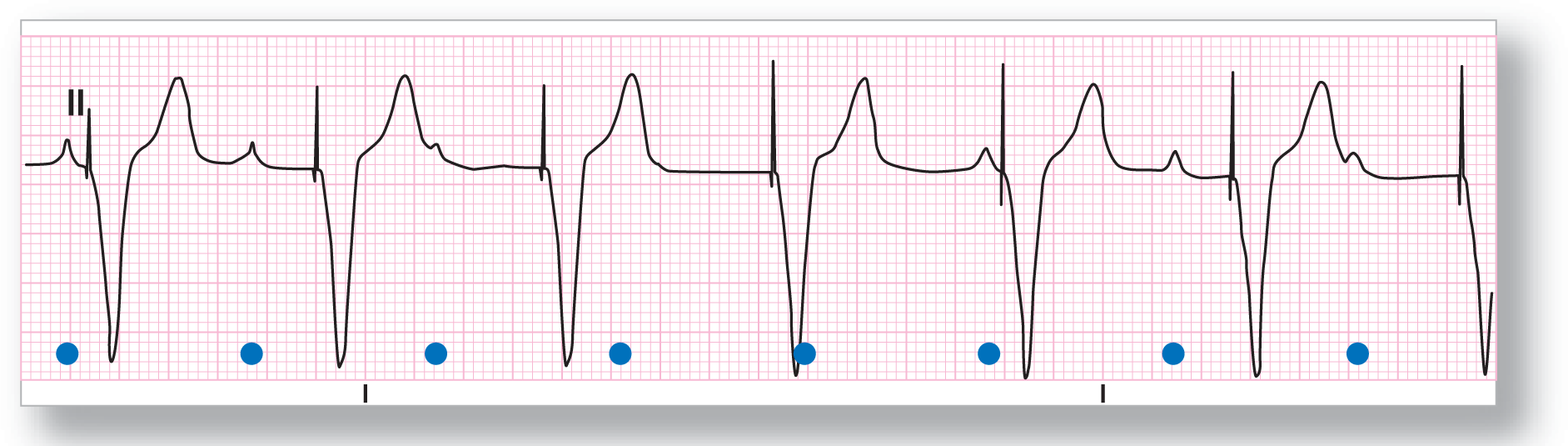
Rate: About 65 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
ECG 39-8 shows the presence of a paced ventricular rhythm. The interesting thing is the presence of P waves (see blue dots) peeking out between some of the ventricular complexes. These P waves are occurring at a regular pattern and have constant P-P intervals. Obviously this pacemaker is not sensing those atrial complexes at all. On obtaining the patient’s history, a VVI pacemaker was confirmed.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 62 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: See discussion below |
Discussion:
We figured that we would end this chapter with a bit of a diagnostic dilemma. Could ECG 39-9 be a ventricular escape rhythm—for example, accelerated idioventricular? Could this be a junctional rhythm with a preexisting bundle branch block or aberrancy? Are the P waves isoelectric in this lead, and if so, could this be a sinus rhythm in somebody with a preexisting bundle branch block? These questions are difficult to answer. You need a few extra leads to make the correct diagnosis.

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 62 BPM |
PR intervals: None |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Paced rhythm |
Discussion:
ECG 39-10 is a strip taken from the same patient in ECG 39-9 after a full 12-lead ECG showed that lead V2 was the best one to see the pacer spike. Here it becomes obvious that this rhythm is a paced rhythm. It is critical to obtain multiple leads to fully evaluate any complex, or potentially complex, arrhythmia. This is just another example of a patient who would have been misdiagnosed, and probably inappropriately treated, for a rhythm abnormality he or she didn’t have.