
Figure 40-1 A mnemonic to remember the approach to analyzing a rhythm strip.
© Jones & Bartlett Learning.
It may seem a bit strange to put a chapter at the end of the text that shows you how to read a rhythm strip. The reason that this chapter appears at the end is because most of the advice we can give you about how to interpret strips cannot be fully appreciated until you have a strong foundation in the principles of arrhythmia recognition and the rhythms themselves.
Interpreting arrhythmias is an abstract and very individual system for each clinician. There are some principles, like obtaining the rate and looking at regularity, that are practiced routinely by everyone. However, the clinicians who are really good at interpreting rhythms practice some very subjective principles, and these change from strip to strip. As you can imagine, teaching these skills is very difficult and putting them on paper is even more of a challenge.
We are going to make every attempt to give you an overall system to look at arrhythmias. Some of the information will be very straightforward. Some will require a bit of imagination on your part. All in all, we are going to prepare you for the process of interpreting arrhythmias. How good you get at it depends on you.
We have narrowed the approach to analyzing a rhythm strip or an arrhythmia on a 12-lead ECG down to a few basic concepts. These concepts can be summed up by using the mnemonic: Always think about your patient’s IQ points (Figure 40-1). The rest of this section is only intended as a short explanation of the concepts involved, and we will be addressing them individually later on.
Figure 40-1 A mnemonic to remember the approach to analyzing a rhythm strip.
© Jones & Bartlett Learning.
The word “patient’s” should always be foremost in your mind when you are approaching a rhythm strip because it is about your patient. Clinical correlation with their presenting complaints, hemodynamic status, history (present and past), physical examination, and any other pertinent information is mandatory to arrive at a correct interpretation of any rhythm strip.
“I” stands for impression. It is there to remind you to always formulate a quick impression of your strip before moving on. This does not mean, however, that this initial impression is set in stone and cannot be changed. Quite the contrary—it is basically a work in progress that needs to be either ruled in or ruled out by answering some simple questions (Figure 40-2).
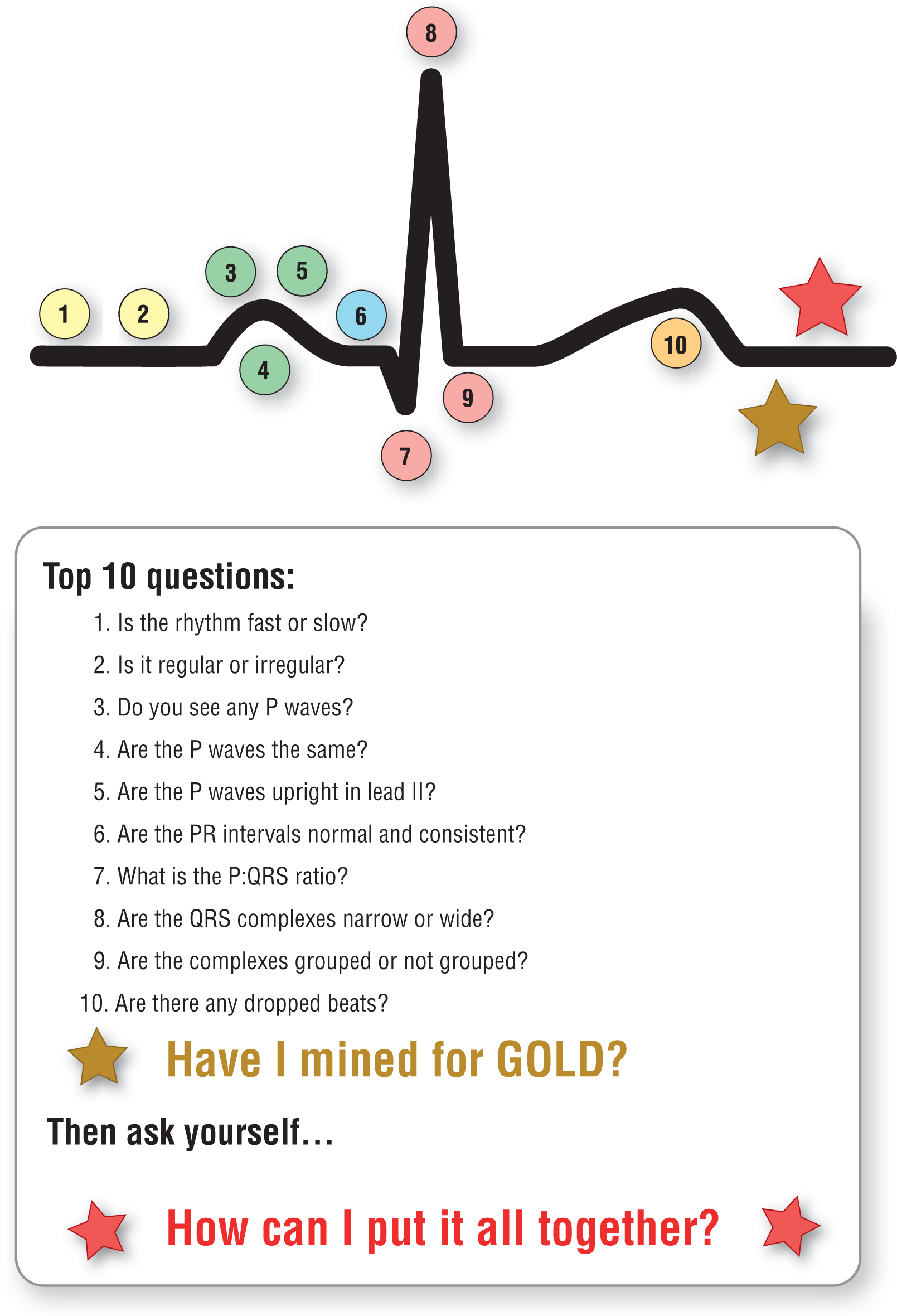
Figure 40-2 The top 10 questions to ask when analyzing a rhythm strip.
© Jones & Bartlett Learning.
DescriptionNotice that in Figure 40-2, the questions relate to different parts of a typical complex. For example, the rate mostly affects the TP segment by making it shorter or longer; Questions 7, 8, and 9 are all related to the QRS complexes. We set up the questions this way so that they would be easy to remember when looking at any QRS complex. You don’t need to actually memorize them in any set order or to actually memorize the figure, but many people remember them a bit more easily with these visual cues to focus on.
Since this is the final review section for the text, we added “Have I mined for GOLD?” after the top 10 questions. As we will expand on later in the chapter, this is to remind us to look at things that don’t fit in with the rest of the strip. It is those small discrepancies, or “golden nuggets,” that can help solidify our evaluation and narrow down the differential diagnosis.
The last part of the mnemonic (points) is a bit of a stretch. “Points” stands for getting a full 12-lead ECG and/or multiple leads and comparing them to an old ECG when needed. Why “points”? Because you want to compare the points or waves between the new strip and the patient’s baseline old strip.