
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
AUTHOR’S NOTE
If the paper speed is set to 25 mm/sec, you can calculate the intervals on a regular rhythm strip. However, you should not get used to reading into the morphology of the complexes, as rhythm strips are not calibrated to the general standards used for 12-lead ECGs. In our descriptions, we comment on morphology for educational purposes and because we have used calibrated strips. For now, concentrate primarily on the rhythm and think about whether a 12-lead ECG is indicated for that patient.
Test ECG-1
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-2

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-3

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-4

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-7

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-9

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-10

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-12

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-13

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-14

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-15

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-16

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-17

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-18

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-19

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-20

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
SECTION 2 Self-Test Answers
Test ECG-1

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Mid-30s to 40s BPM |
PR intervals: Prolonged, first-degree AV block |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus arrhythmia |
Discussion:
Test ECG-1 is clearly bradycardic. The rate slowly changes between the mid-30s to the upper 40s. It is, however, not just simple sinus bradycardia. If you notice, the R-R intervals are slowly decreasing but the PR intervals, though prolonged, are exactly the same. The morphology of the P waves is unchanged throughout the strip. The QRS complexes are all the same and within the normal range. The diagnosis is sinus arrhythmia.
By the way, a longer rhythm strip taken shortly afterward showed the traditional slowing down and speeding up of the rate, as expected. The patient remained bradycardic but hemodynamically stable.
Test ECG-2

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 50-70 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regularly irregular |
QRS width: Wide |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus arrhythmia |
Discussion:
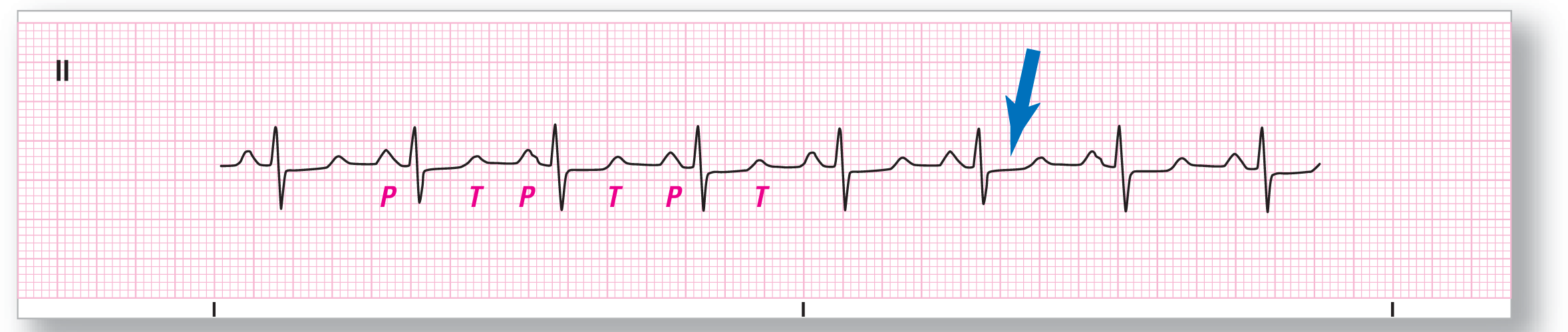
If you use your calipers on Test ECG-2, you will notice that the rhythm is regularly irregular but there is a progressive lengthening and then shortening of the R-R intervals. The P-wave morphology is the same throughout the strip and the PR intervals remain constant. Based on these findings, the diagnosis is sinus arrhythmia.
There is an additional finding which is of interest in this strip. If you notice, the ST segments are elevated and flat (see blue arrow). A 12-lead ECG showed that the patient was having an acute myocardial infarction at the time the strip was taken. Remember to always be suspicious!
Test ECG-3

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 135 BPM |
PR intervals: Short, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
Test ECG-3 shows a sinus tachycardia. The strip is even more impressive because of the very tall QRS complexes that are found in this patient. These very tall QRS complexes can be found in young people, hypertrophy, and cardiomyopathies, to name a few possible sources.
The T waves are almost isoelectric in this lead and are almost not visible. The P waves are tall and peaked and the morphology is consistent throughout the strip. The PR interval is also consistent but markedly shortened at 0.08 seconds.
Test ECG-4
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 85 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Normal sinus rhythm |
Discussion:
You have to be a little careful not to confuse the T waves and the P waves in Test ECG-4. Careful identification of the different waves would be helpful in preventing mistakes that could arise due to mislabeling. Do you notice anything peculiar about the third and seventh P waves? They have a slightly different morphology than the others. They are not ectopic complexes, however, because the PR intervals are identical and the cadence of the rhythm is not altered by their appearance. Perhaps they represent a slight alteration of the pacemaker site within the SA node itself. In any case, they are of no clinical significance. On the other hand, the ST depressions (see blue arrow) and the prolonged QT should be evaluated further with a 12-lead ECG.
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 50 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus bradycardia |
Discussion:
Test ECG-5 shows sinus bradycardia. There is some slight variation in the cadence of the rhythm, but the variation is well within the accepted upper limit of 0.12 seconds. The P waves all show the same basic morphology with a consistent PR interval. The PR interval is right at the borderline of 0.20 seconds. The slight morphologic differences in the appearance of the waves can be accounted for by the baseline which is not exactly straight. The QRS complexes are all within normal ranges and similar in morphology. The ST segments are troubling because they are elevated and concave downward (see blue arrow and diagram). These ST segments can be commonly found in ischemia or infarction and may be the cause of the patient’s bradycardia. Further evaluation with a 12-lead ECG is indicated.
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 65 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Normal sinus rhythm |
Discussion:
Test ECG-6 is a good example of normal sinus rhythm. Note the consistency in the P-wave morphology and the recurrence of the identical PR intervals throughout the strip. The QRS complex is within normal limits for duration and morphology. There is some very slight ST-segment depression noted throughout, which could be an abnormality of the rhythm strip itself. As mentioned before, rhythm strips are notorious for the presence of slight abnormalities that are not present on a full 12-lead ECG. If there are any questions or if the patient is exhibiting any symptoms, a full 12-lead can be obtained for further evaluation just to be sure.
Test ECG-7

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 145 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
Test ECG-7 shows a very rapid sinus tachycardia. The P waves are upright and morphologically similar throughout the strip. The PR intervals are consistent and within acceptable limits. There is no evidence for any buried P waves noted on the strip which could confuse the diagnosis. The QRS intervals are within the normal limit and are consistent with the diagnosis of sinus tachycardia.
Note the ST-segment depression labeled by the blue arrow. ST-segment depression is common in tachycardias and is not necessarily a sign of ischemia. Clinical correlation with the patient and his or her presentation is indicated, however, to rule out more dangerous causes for the depression.
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 45 BPM |
PR intervals: Prolonged, first-degree AV block |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus bradycardia |
Discussion:
Test ECG-8 shows the characteristics of a typical sinus bradycardia. The P waves all show similar morphology and the PR intervals are prolonged but consistent. The QRS complexes are wide, which could be due to a bundle branch block; further correlation is indicated with an old strip, or an ECG would be helpful in this evaluation.
The P waves show a double-humped morphology, which could be consistent with a left atrial abnormality if the finding were present on a 12-lead ECG. Once again, you should be very careful about evaluating wave morphology on a rhythm strip.
Test ECG-9

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Discussion:
Test ECG-9 shows a regular rhythm with an event. The rhythm strip has consistent P-wave morphology, upright P waves in lead II, and normal, consistent PR intervals. There is some slight discrepancy in the cadence of the rhythm during the first six complexes, which is within acceptable limits, and then there is a much longer pause. The pause is followed by a complex with an identical P wave and PR interval to the rest of the strip. The longer pause is due to a delay in the impulse from exiting the SA node and is consistent with a sinus pause.
|
Rate: About 70 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular with an event |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus rhythm with a sinus pause |
Test ECG-10

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 90 BPM |
PR intervals: Prolonged, first-degree AV block |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus rhythm (see discussion below) |
Discussion:
Test ECG-10 shows very prominent P waves that are double humped and notched (see blue arrow). The morphology of the P waves is consistent throughout the strip. The PR intervals are slightly over 0.20 seconds and, therefore, slightly prolonged (first-degree AV block will be covered fully in Chapter 28, Atrioventricular Blocks). The QRS complexes are of normal duration. The ST segments are depressed and the T waves are inverted. Clinical correlation of these findings and a full 12-lead ECG are suggested for further evaluation.
For completeness, this rhythm strip cannot be called normal sinus rhythm because of the prolonged PR interval. Instead, we will simply call it sinus rhythm (with a first-degree AV block, for you more advanced students).
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Around 40 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus bradycardia |
Discussion:
The P waves on the complexes in Test ECG-11 are not very prominent. However, they are positive in lead II and are consistent throughout the strip. The PR intervals are also consistent and within normal limits. The heart rate is around 40 BPM. Putting it all together, we have a sinus bradycardia.
Test ECG-12

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 125 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
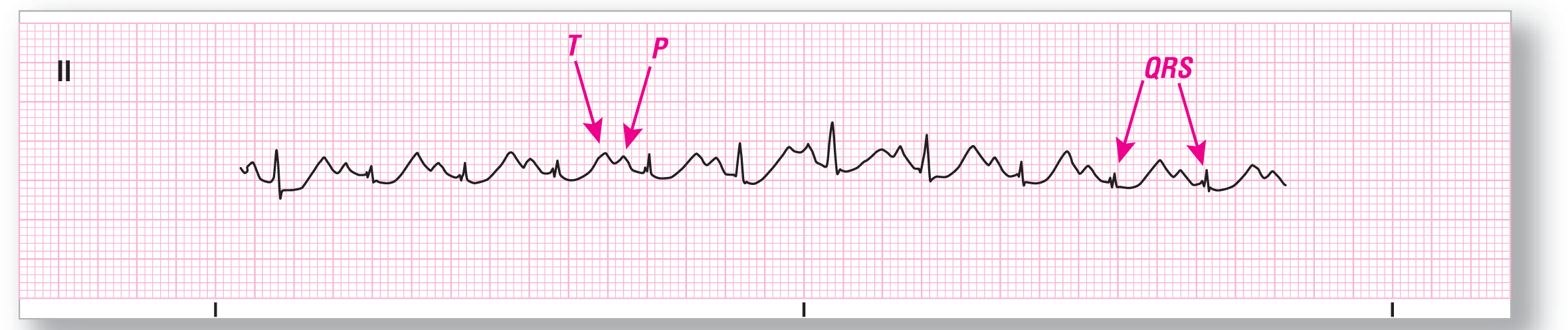
Test ECG-12 can be quite confusing to interpret. The reason for the confusion is the near fusion of the T waves and the P waves. The main reason for this near-fusion to develop is that tachycardias typically cause the TP segment to shorten. In this example, the TP segment is basically nonexistent and the T waves and the P waves become superimposed on each other. Take a look at the waves labeled on the strip and imagine a vertical line drawn right between the two waves. This will help you see the individual waves a bit more clearly.
The strip is consistent with sinus tachycardia at about 125 BPM. The ST-segment depressions may be due to the tachycardia, but clinical and ECG correlation should be considered.
Test ECG-13

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: Around 100 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus arrhythmia |
Discussion:
Test ECG-13 is obviously irregular. The presence of identical P-wave morphology and PR intervals throughout the strip cinch the diagnosis of sinus arrhythmia.
When you have a wandering baseline, always take a few extra seconds to look at the strip a bit closer. Morphologic changes of premature or ectopic complexes can be hidden within the wandering baseline or in artifact. If there continue to be questions about the rhythm, obtaining a longer strip or simply readjusting the leads on the patient will often clear the issues right up.
Test ECG-14

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 130 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright, tall, and peaked Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
Test ECG-14 also shows complexes with fairly prolonged QT intervals. In this example, however, the P waves and the T waves are distinct. Using your calipers to map out the various waves and then marching them through the strip can be quite helpful in these cases.
The relatively low amplitude of the QRS complexes in this strip can also lead to some confusion. Changing leads on the monitor or obtaining a 12-lead ECG will address this potential problem.
Test ECG-15

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Around 80 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Normal sinus rhythm |
Discussion:
Test ECG-15 also shows a wandering baseline. In this case, however, it does not affect our interpretation in any way. The P waves are clearly seen and show the same morphology throughout the strip. They are upright in lead II, as would be expected. The PR interval is consistent throughout the strip as well. The strip is a good example of a normal sinus rhythm.
Did you pick up the ST-segment abnormality in this strip (see blue arrow)? Once again, the ST segments are elevated and flat. These are very troublesome and consistent with injury or infarct. Clinical correlation and a full 12-lead ECG should be obtained emergently on this patient.
Test ECG-16

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 60 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Normal sinus rhythm |
Discussion:
Test ECG-16 is another example of normal sinus rhythm. The rate is slightly over 60 BPM, putting it within the normal range. The PR interval gives you the impression of being short. Careful measurement, however, will show you that it is 0.12 seconds long and in the normal range.
Once again, there is some slight ST depression noted on this strip. Clinical and electrocardiographic correlation should be considered.
Test ECG-17

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Around 140 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
Test ECG-17 is a tough one! Take a close look at the area between the end of the QRS complex and the start of the next one. Use a magnifying glass if you need to see it more clearly. You will notice that there are distinct P waves but, once again, they are nearly buried in the preceding T wave.The consistent P-wave morphology and PR interval, along with a heart rate of around 140 BPM, makes the rhythm a sinus tachycardia. Note that the width of the QRS complexes (greater than 0.12 seconds) does not affect the rhythm in any way; it is still a sinus tachycardia.
Test ECG-18
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Slightly over 120 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia |
Discussion:
In Test ECG-18, we are showing you another example of prolonged QT interval with P-on-T phenomenon because they can be quite confusing. This strip has waves that are a bit more distinct, which helps with evaluation. The P waves are all upright in lead II and the morphology is consistent throughout the strip. The PR intervals are also consistent throughout the strip. The QRS complexes vary in amplitude, demonstrating a common occurrence in tachycardias: electrical alternans. This can normally be seen in many tachycardias. There is some ST segment depression noted on the strip. Clinical and electrocardiographic correlation should be considered in this case for further evaluation of the abnormal findings and to determine the cause of the tachycardia.
Test ECG-19

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 55 BPM |
PR intervals: Normal, consistent |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus arrhythmia |
Discussion:
Unless you have a very good eye or used your calipers, it would be very difficult to spot the small amount of narrowing that occurs between each of the complexes in Test ECG-19. The key in this strip is to see the difference between the first two and the last two complexes in the strip. The difference is 0.16 seconds, which makes the variation abnormal. On a long rhythm strip, the undulation of the distances with the patient’s respirations becomes more obvious.
For those who have studied electrocardiography, note the slight PR depressions and the scooping ST segments, which could be an early repolarization pattern or early pericarditis.
Test ECG-20

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 75 BPM |
PR intervals: Prolonged |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus rhythm |
Discussion:
We are throwing a bit of a curve ball Test ECG-20. There are a few of reasons for this: (1) The small amplitude and the morphology of the QRS complexes can cause some confusion when examining this rhythm strip. (2) The PR interval is prolonged at 0.24 seconds. (3) The QRS complexes are wider than 0.12 seconds. Recall that part of the criteria for normal sinus rhythm is to have intervals within the normal range. This patient has a prolonged PR interval—which as we shall see later on, makes this a first-degree heart block—and a wide QRS complex. Note that this is still a sinus rhythm, but not normal sinus rhythm. This slight difference in nomenclature is usually overlooked by many clinicians and authors, but is the correct terminology.