
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Test ECG-1
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-2

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-3

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-4

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-7

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-9

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-10
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-12

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-13

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-14

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-15

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-16
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-17

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-18

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-19

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-20
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
SECTION 3 Self-Test Answers
Test ECG-1

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 75 BPM |
PR intervals: Normal, different interval in event |
|
Regularity: Regular with an event |
QRS width: Normal |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
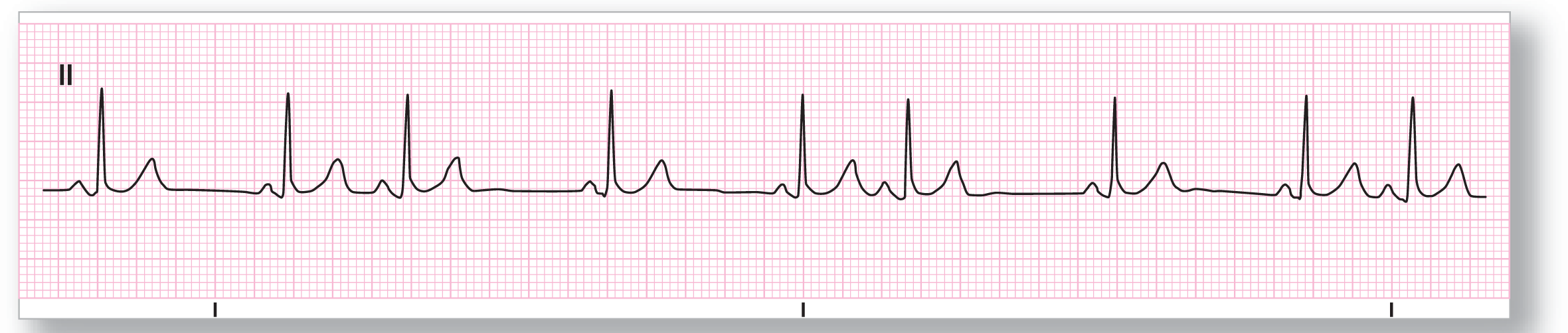
Rhythm: Sinus rhythm with a PAC |
Discussion:
Test ECG-1 shows an underlying sinus rhythm with one PAC (see blue arrow). Note that the morphology of the ectopic P wave is different from the other sinus P waves. The cadence of the underlying sinus rhythm is not affected by the PAC. This happens when the sinus node is not reset by the ectopic beat. This pause, therefore, is a full compensatory pause and is two times the R-R interval of the preceding complexes. It is interesting to note that most PACs are associated with noncompensatory pauses, making this particular case a bit unusual.
Test ECG-2
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 63 BPM |
PR intervals: Normal |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
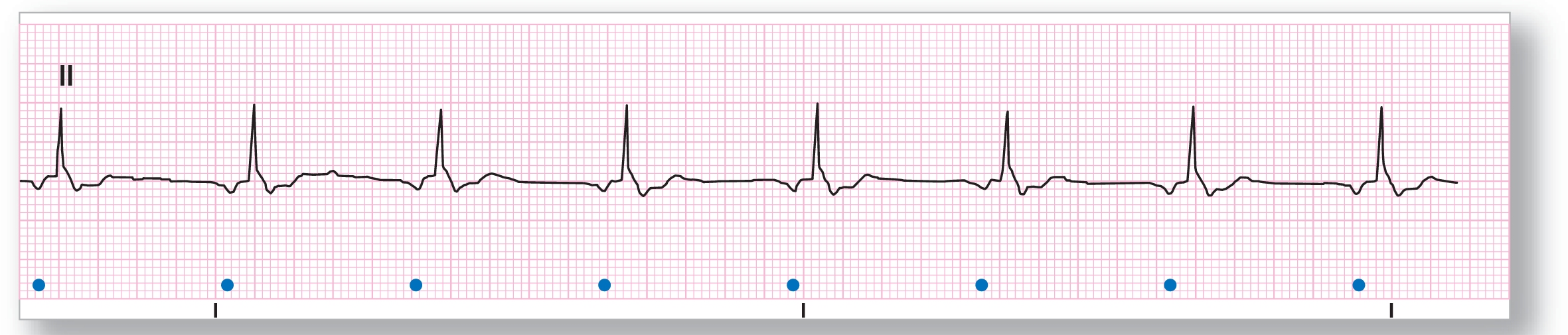
Rhythm: Ectopic atrial rhythm |
Discussion:
In Test ECG-2, the P waves are where the money is on this strip (see blue dots). The P waves are inverted in lead II, which means that the P wave axis is grossly abnormal. The rhythm is about 63 BPM and regular. There is no grouping or dropped beats and the QRS complexes are within the normal range. In these cases, you have one major difficulty: Is this an ectopic atrial rhythm or a junctional rhythm? The main deciding factor that many people use to distinguish between the two is the length of the PR interval. If the PR interval is normal, it is suggestive of an ectopic atrial pacemaker. If the PR interval is short, then a junctional rhythm is more likely. In this case, the PR interval is normal, making the final diagnosis an ectopic atrial rhythm.
Test ECG-3
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: 260 BPM; Ventricular: 66 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None, F waves are visible Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 4:1 |
Rhythm: Atrial flutter with 4:1 conduction |
Discussion:
Test ECG-3 shows an obvious flutter wave pattern at the baseline. The F waves are occurring at a rate of about 260 BPM and the ventricular response is about 66 BPM. The conduction ratio is 4:1. Here is an easy way to calculate the conduction ratio in atrial flutter: Take the number of visible F waves and add one to that figure (there is always going to be one F wave buried in the QRS complex). In this case, the morphology of the QRS complex is widened because of an underlying right bundle branch block. But, be careful! The QRS complexes, in some strips, may be widened because of fusion with the underlying F waves, aberrancy, or because of a ventricular escape rhythm. A full 12-lead ECG will help answer the question of bundle branch block or aberrancy, and an old ECG would be invaluable in these cases.
Test ECG-4

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 80 BPM |
PR intervals: None |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
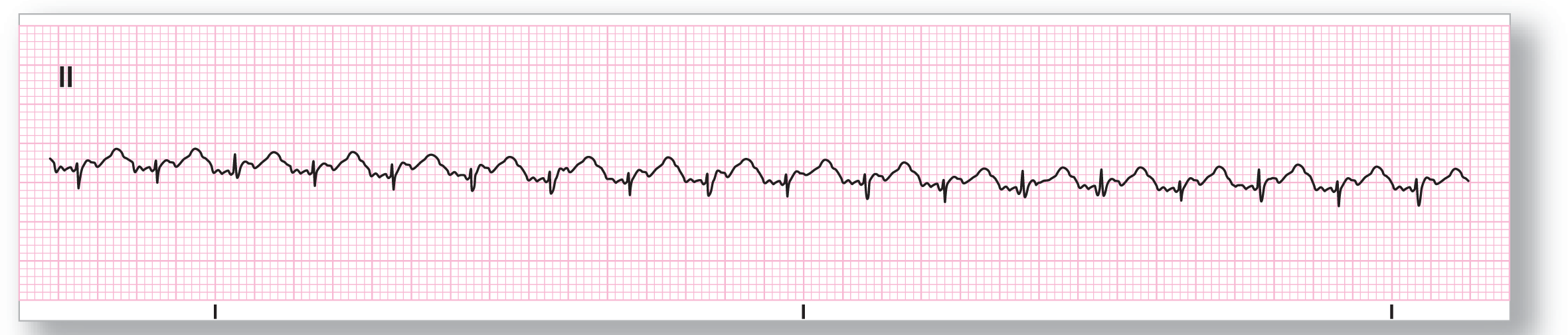
Rhythm: Atrial fibrillation |
Discussion:
Test ECG-4 shows an irregularly irregular rhythm occurring at a rate of about 80 BPM. There are no visible P waves anywhere on the strip. Remember, the three main irregularly irregular rhythms are atrial fibrillation, wandering atrial pacemaker, and multifocal atrial tachycardia. Wandering atrial pacemaker and multifocal atrial tachycardia both have P waves. By a process of elimination, the answer is controlled atrial fibrillation. Other possibilities for irregularly irregular rhythms exist, but are not commonly found. These include variable conduction atrial flutter, very frequent premature complexes (usually regularly irregular), and the initial period at the onset of many tachycardias, just to name a few. Other clues will help you out to make the final diagnosis in those cases. The wandering baseline is due to the fine f waves.
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 150 to 160 BPM |
PR intervals: Variable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Variable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Multifocal atrial tachycardia |
Discussion:
Test ECG-5 shows some pretty impressive P waves (see blue dots)! They are actually taller than the R wave of the QRS complex. We included this strip to make a point. Sometimes the morphology of a part of the complex will be very unusual and will distract you from the evaluation of the rest of the strip. Just remember, a P wave is a P wave is a P wave. The same applies to the other waves in the complex, as well. In this strip, the rhythm is irregularly irregular and there are varying P-wave morphologies (at least three) and PR intervals throughout the entire strip. These criteria are compatible with either multifocal atrial tachycardia or wandering atrial pacemaker. Since the rhythm is a tachycardia, the correct answer is multifocal atrial tachycardia.
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 110 BPM |
PR intervals: Variable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Variable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Multifocal atrial tachycardia |
Discussion:
Test ECG-6 shows a series of complexes that each contain a P wave and a QRS complex with a 1:1 conduction ratio. The P-wave morphology and the PR intervals, however, are constantly changing and there are at least three different P-wave morphologies and PR intervals. The cadence of the rhythm is completely irregularly irregular. As we have mentioned before, there are three main irregularly irregular rhythms to consider: atrial fibrillation, multifocal atrial tachycardia, and wandering atrial pacemaker. Since there are P waves present, we can throw out atrial fibrillation. The other two rhythms have the same criteria except for the rate. The strip shows a tachycardic rhythm with a rate a little over 110; this means that it has to be multifocal atrial tachycardia. Note the blue arrow, which is pointing out a buried P wave.
Test ECG-7
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: 270 BPM; Ventricular: 135 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 2:1 |
Rhythm: Focal atrial tachycardia with block |
Discussion:
Test ECG-7 shows a rapid atrial tachycardia at a rate of about 270 BPM. Notice that there is a flat baseline between the atrial complexes in this lead. There is a 2:1 conduction ratio throughout the strip. So, is this atrial flutter with 2:1 block? Flutter waves are in constant motion due to the macroreentry circuit that creates them in the right atrium. The baseline in atrial flutter is never flat. Sometimes, however, the baseline may be a little flatter, but there should still be a constant undulation present. Lead II, in this case, also showed a flat baseline, which is inconsistent with atrial flutter. Technically, even though this is above the usual atrial range for focal AT with block (150 to 250 BPM), this is the correct answer. Subsequent clinical information did confirm that diagnosis in this patient.
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 110 BPM |
PR intervals: Variable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Variable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Multifocal atrial tachycardia |
Discussion:
The cadence of Test ECG-8 is irregularly irregular and there are P waves present throughout the strip. The P waves are dissimilar to each other and they have different PR intervals. The rhythm is also tachycardic. Putting this information together, we have a multifocal atrial tachycardia. Note the presence of some mild aberrancy throughout the strip and one complex (see blue arrow) with gross aberrancy. This is a common finding in multifocal atrial tachycardia, and it usually occurs because of fusion between the components of surrounding complexes. Another frequent cause is aberrancy due to refractoriness of some part of the electrical conduction system. The most frequent culprit is the right bundle branch, but any section of the system may be at risk.
Test ECG-9

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 45 BPM |
PR intervals: Normal, except in event |
|
Regularity: Regular with an event |
QRS width: Normal |
|
P waves: Present, except in event Morphology: Upright, except in event Axis: Normal, except in event |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus bradycardia with a PAC |
Discussion:
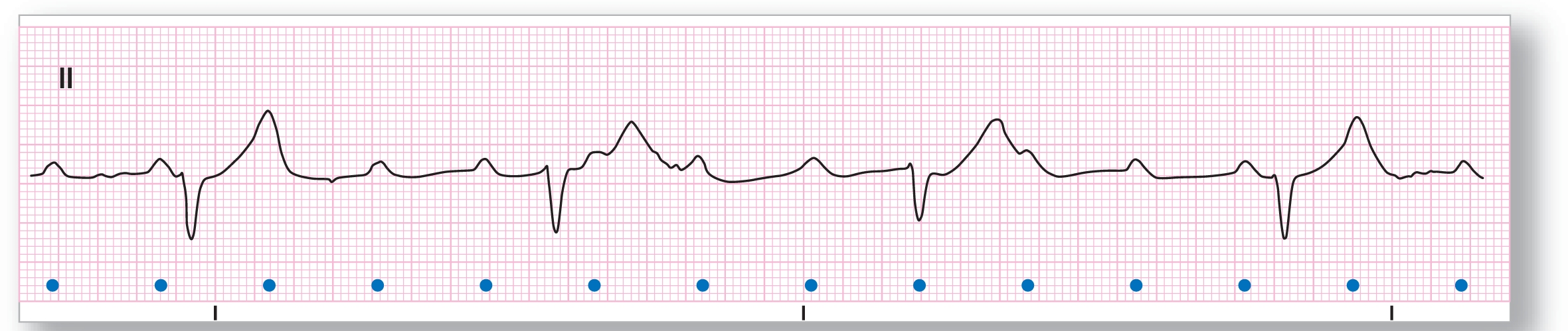
Test ECG-9 shows a regular rhythm that is markedly bradycardic with one event that occurs prematurely. The P waves and PR intervals are all the same, except for the ones in the premature complex. The premature complex has a shorter PR interval (but still within the normal range) and an inverted P wave. These findings are consistent with a premature atrial contraction. The interval is close to being compensatory and the rate subsequent to the PAC is almost the same. This is a borderline compensatory pause, but you can also argue in favor of a noncompensatory pause. It really doesn’t matter too much in this case because the complex is obviously a PAC.
Test ECG-10
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 70 BPM |
PR intervals: Variable |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Normal |
Grouping: Yes |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus rhythm with a supraventricular trigeminy |
Discussion:
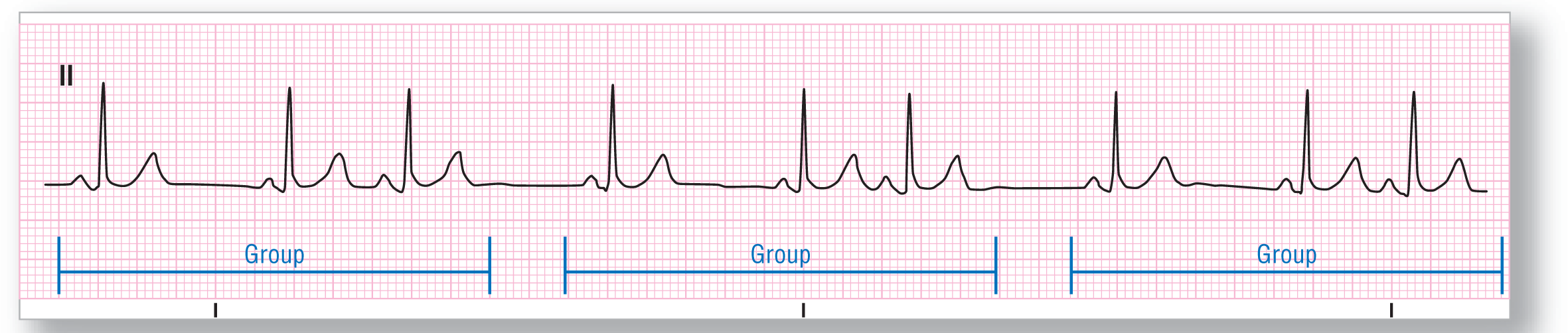
Test ECG-10 can be a little troubling at first glance. The frequent PACs are easy to spot but the grouping can be a little tougher to pick out. If you notice, there is a recurrent pattern of sinus-sinus-PAC that is found throughout the strip. The first thought in your mind when you see grouping should be: Is there an AV block of some kind? Well, the answer is no (AV blocks are covered in Chapter 28, Atrioventricular Blocks; for now, just take our word for it). The third complex is simply a PAC. The rhythm can either be called a sinus rhythm with frequent PACs or, more specifically, a supraventricular trigeminy (a PAC every third complex). The actual description of the strip should be sinus rhythm with an overlying supraventricular trigeminy, to be exact.
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: See discussion below |
PR intervals: Variable |
|
Regularity: See discussion below |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Variable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: See discussion below |
Discussion:
Even though there are three different P-wave morphologies on Test ECG-11, this is not a wandering atrial pacemaker. The reason is that the rhythm is not irregularly irregular. It is regularly irregular. Notice that the first four complexes are a sinus or an ectopic atrial rhythm (need an old ECG to compare) firing at a rate of 70 BPM. Then, there is a premature atrial complex (marked by the blue arrow) that triggers a different pacemaker to begin to fire. This pacemaker is obviously an ectopic pacemaker because of the completely different morphology and PR interval from the first one on the strip. The last pacemaker is firing at a tachycardic rate of 105 BPM, making this section of the strip a focal atrial tachycardia. The PAC merely acted as the trigger for the new rhythm.
Test ECG-12

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 160 BPM |
PR intervals: None |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Atrial fibrillation |
Discussion:
Test ECG-12 shows an example of an uncontrolled atrial fibrillation. The rate is very fast at about 160 BPM, and is completely random or irregularly irregular. There are no P waves visible throughout the strip. There are a couple of fluctuations in the baseline, which could be interpreted as an occasional P wave, but there is no consistency and these are simply fluctuations in the baseline. The QRS morphology also varies throughout the strip, which could lead to some incorrect diagnoses. This variation is caused by aberrancy and possibly fusion with other waves, including coarse f waves. A full 12-lead ECG and a longer rhythm strip would be very helpful in evaluating this patient further. The ST segments in the strip appear somewhat scooped, raising the possibility of digitalis effect.
Test ECG-13

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 90 BPM |
PR intervals: Variable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Variable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Wandering atrial pacemaker |
Discussion:
Test ECG-13 shows an irregularly irregular rhythm with P waves of at least three different morphologies. The rate is mostly within the normal range, with a few complexes occurring more rapidly. These criteria are consistent with wandering atrial pacemaker. The slight discrepancies in the morphologies of the QRS complexes is consistent with the fusion and aberrancy that is commonly seen in both wandering atrial pacemaker and multifocal atrial tachycardia. A 12-lead ECG should be obtained to evaluate the slight ST depression that is evident throughout the strip.
Test ECG-14

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 300 BPM |
PR intervals: Not applicable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: None, f waves Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Variable |
Rhythm: Atrial flutter with variable conduction |
Discussion:
Test ECG-14 shows an irregularly irregular rhythm. Are there any visible P waves? No. What is visible are flutter waves with a continuously undulating baseline at a rate of 300 BPM. This is atrial flutter. The randomness of the ventricular response is because of the variable conduction of the impulses through the AV node. This is not a common presentation for atrial flutter, but does occur often enough that you have to be ready to spot it clinically. The key to the diagnosis is the presence of the flutter waves. The morphologic differences in the QRS complexes comes from aberrancy and fusion with the underlying flutter waves. A high index of suspicion would be needed if the flutter waves were not so obvious. Additional leads would greatly aid in the diagnosis in those cases.
Test ECG-15
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: About 105 BPM; Ventricular: About 32 BPM |
PR intervals: Not applicable |
|
Regularity: Regularly irregular |
QRS width: Wide |
|
P waves: Present Morphology: Upright Axis: Normal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Variable |
Rhythm: Focal atrial tachycardia with block |
Discussion:
Test ECG-15 shows a variation in the rate of the atria and the ventricles. The atrial complexes are easily identified and occur at a rate of 105 BPM. The ventricular complexes are wider than 0.12 seconds and at a rate of about 32 BPM. The ventricular rate and the width of the complexes are compatible with a ventricular origin. The ventricular rhythm is actually a ventricular escape rhythm. In order for the atria and the ventricles to vary so widely and to not exert any influence on each other, there has to be a complete lack of communication between them. That is exactly what occurs in a complete heart block (see Chapter 28, Atrioventricular Blocks). The final diagnosis for this rhythm strip is focal atrial tachycardia with a complete heart block and a ventricular escape rhythm.
Test ECG-16

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: 300 BPM; Ventricular: 150 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter with a 2:1 conduction |
Discussion:
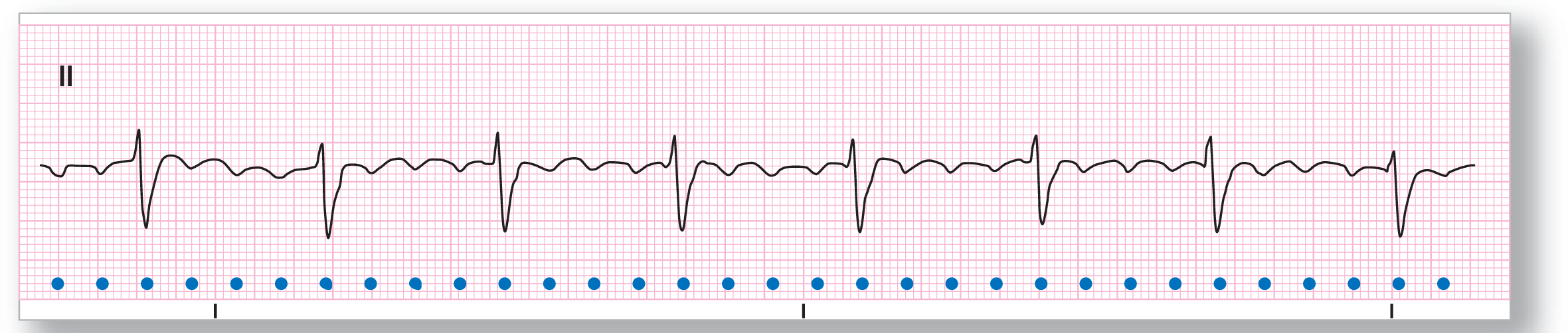
Test ECG-16 is rather deceptive. What is the rate of the ventricular complexes? 150 BPM. That rate should immediately spark a question: Am I dealing with atrial flutter? Remember, the most common rate for atrial flutter is 300 BPM with a 2:1 conduction, giving you a ventricular response of 150 BPM. Looking closely at the complexes, we see a deflection a little bit before the QRS complex (see red arrow) and a deflection buried in the ST segment (see blue arrow). These deflections occur at a rate of 300 BPM and are the flutter waves for this patient. Additional leads would be very helpful in confirming your suspicions. In addition, vagal maneuvers such as carotid massage or having the patient Valsalva (push down like they are having a bowel movement) or a little IV adenosine could slow the ventricular response and uncover the flutter waves.
Test ECG-17

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 160 BPM |
PR intervals: None |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
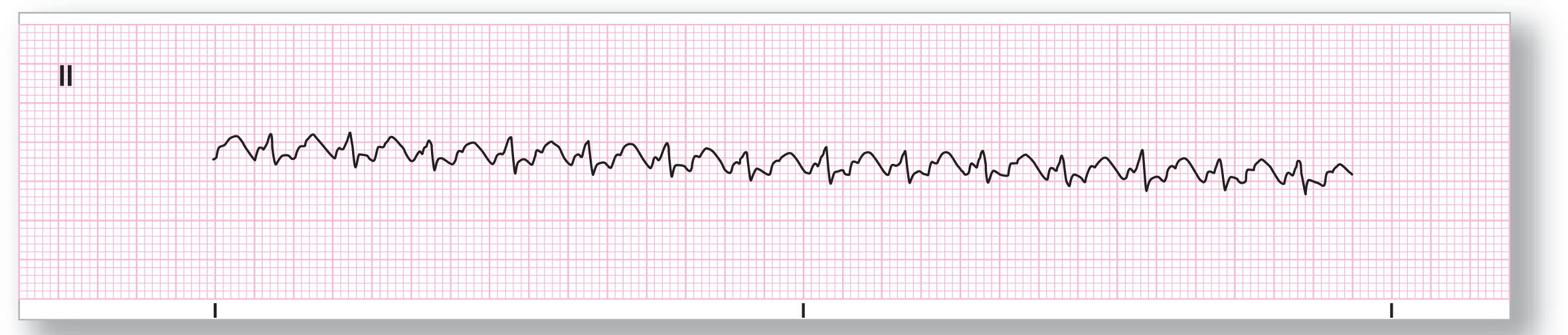
Rhythm: Atrial fibrillation |
Discussion:
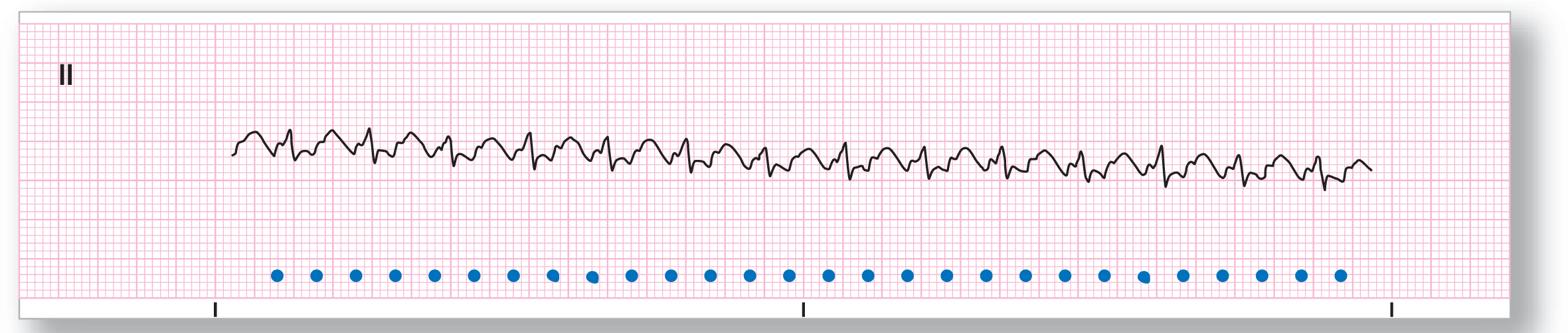
Test ECG-17 shows an uncontrolled atrial fibrillation at a rate of about 160 BPM. Be careful of just quickly eyeballing a rhythm strip and calling it regular, especially a rapid atrial fibrillation. The faster the rate in an uncontrolled atrial fibrillation, the less the variability that exists from beat to beat. In this case, there are a couple of wider R-R intervals that let you get away with a quick eyeball, but you should get into the habit of using your calipers. After all, what would you rather do: Use your calipers or spend a few months in court discussing issues of malpractice?
Test ECG-18
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: Atrial: 290 BPM |
PR intervals: Not applicable |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: None |
Rhythm: Atrial flutter with variable (Wenckebach) conduction |
Discussion:
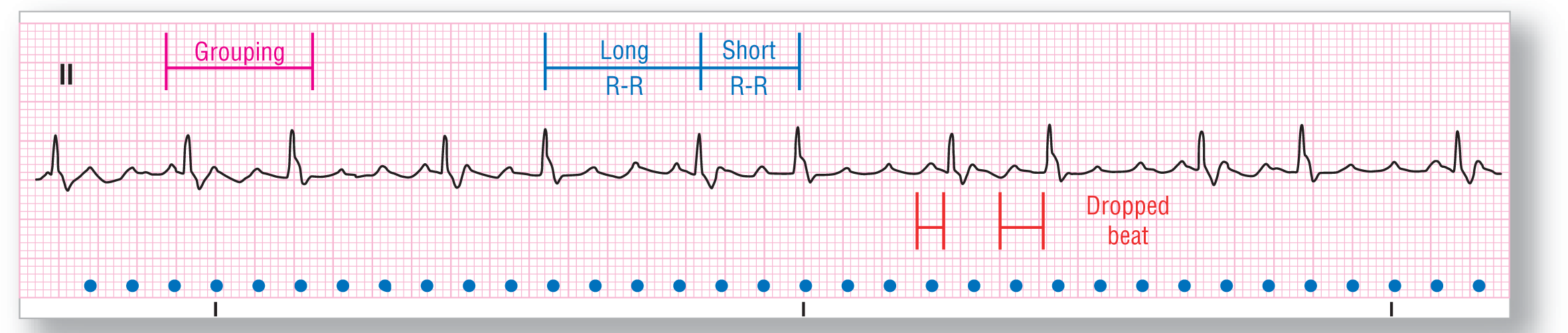
Test ECG-18 shows a fairly advanced arrhythmia, but we can figure it out. There are obvious F waves present. What is the cadence of the strip? It is regularly irregular. Once again, calipers are invaluable. Using the R-R intervals, we see that every other complex is long and every other one is short. This phenomenon recurs throughout the strip. This is a variation of a variable conduction aflutter. (For advanced students: Looking at the F waves and their relation to the QRSs, we see that the F-R interval increases between the long complex and the short one. The long pause is caused by the dropping of one of the QRS complexes. This type of AV block is called Wenckebach AV block; see Chapter 28, Atrioventricular Blocks.)
Test ECG-19

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 75 BPM |
PR intervals: Normal |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present Morphology: Inverted Axis: Abnormal |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
Rhythm: Ectopic atrial rhythm |
Discussion:
Test ECG-19 shows a regular rhythm at about 75 BPM with inverted P waves in lead II. The inverted P waves and the rate of 75 BPM make the diagnosis ectopic atrial rhythm. There is a slight variation in between the various R-R intervals but it is within acceptable limits.
Test ECG-20
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Atrial: 300 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None, F waves are visible Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 2:1 |
Rhythm: Atrial flutter with 2:1 conduction |
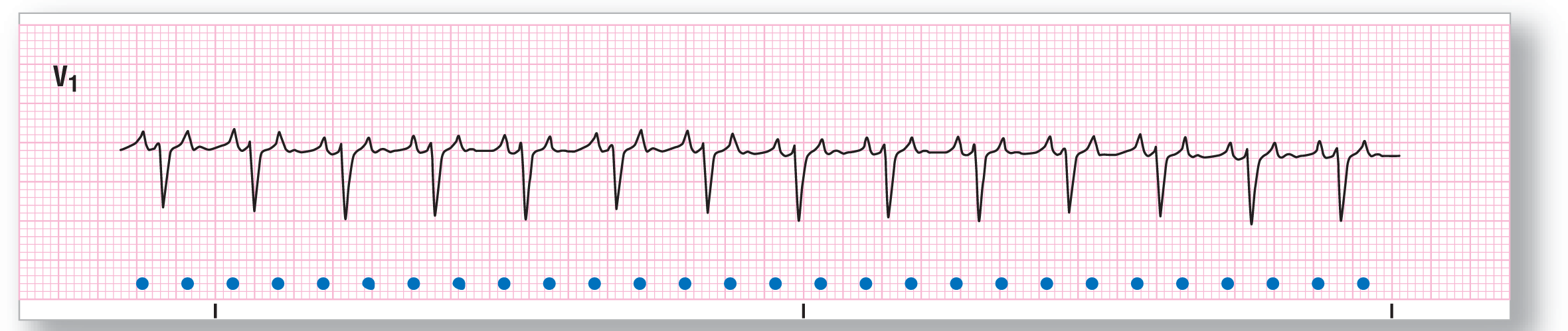
Discussion:
Test ECG-20 is similar to Test ECG-16 that we saw a few strips back. There is an F wave right before the QRS complex and one buried in the ST segment. The key to diagnosis is to realize that the ventricular rate is 150 BPM. Once you hear that number, you should instantly think of atrial flutter with 2:1 conduction and begin looking for the F waves. Remember, if you can’t see them in lead II, get another lead, preferably lead V1 because it will show positive F waves and they will be much easier to pick out. Once again, vagal maneuvers and IV adenosine may unmask the F waves in questionable cases and should be attempted if no contraindications to using them exist.