From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Test ECG-1
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-2

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-3
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-4
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-7

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-9

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-10
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-12

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-13

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-14

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-15
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-16

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-17

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-18
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-19
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
Test ECG-20

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: |
PR intervals: |
Notes: |
|
Regularity: |
QRS width: |
|
|
P waves: Morphology: Axis: |
Grouping: |
|
|
Dropped beats: |
||
|
P:QRS ratio: |
Rhythm: |
SECTION 5 Self-Test Answers
Test ECG-1

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
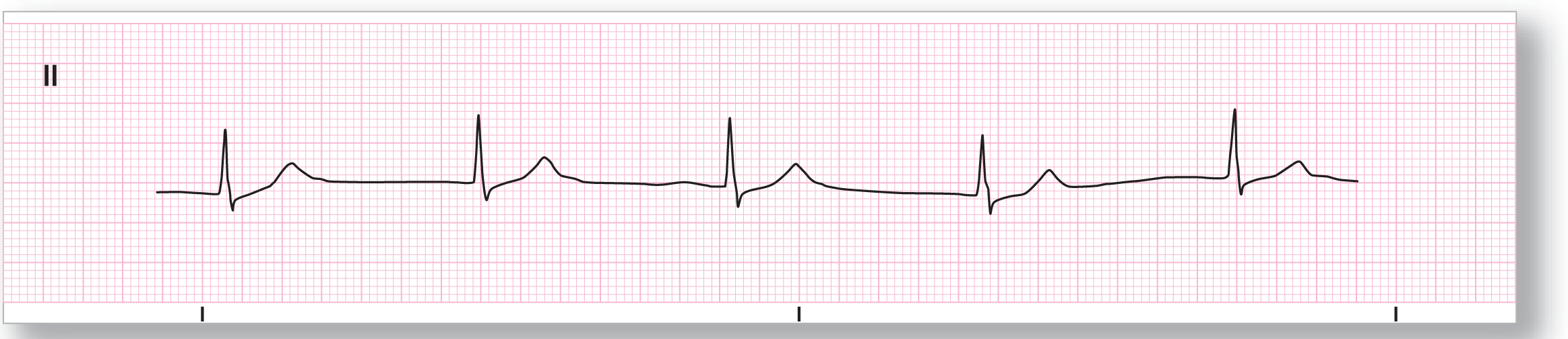
Rate: About 76 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
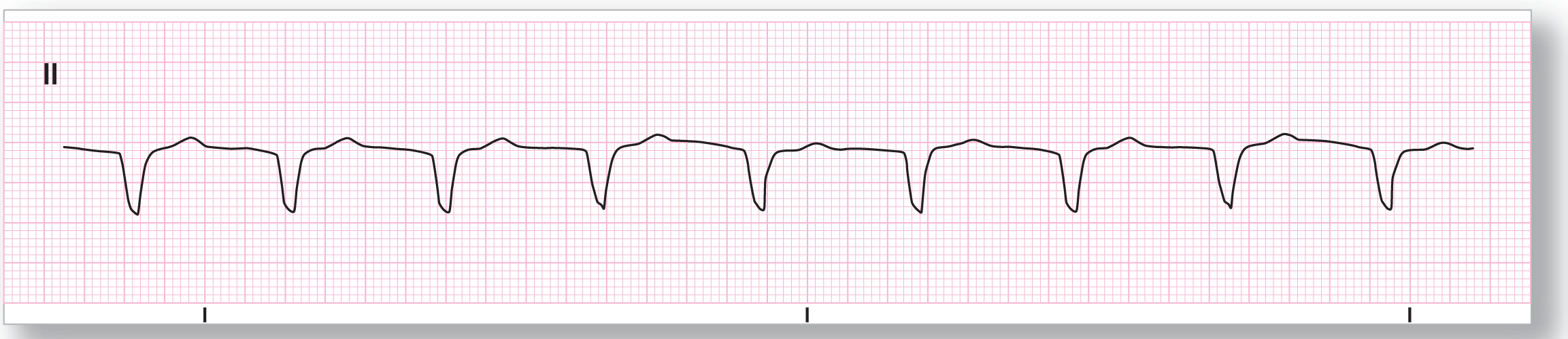
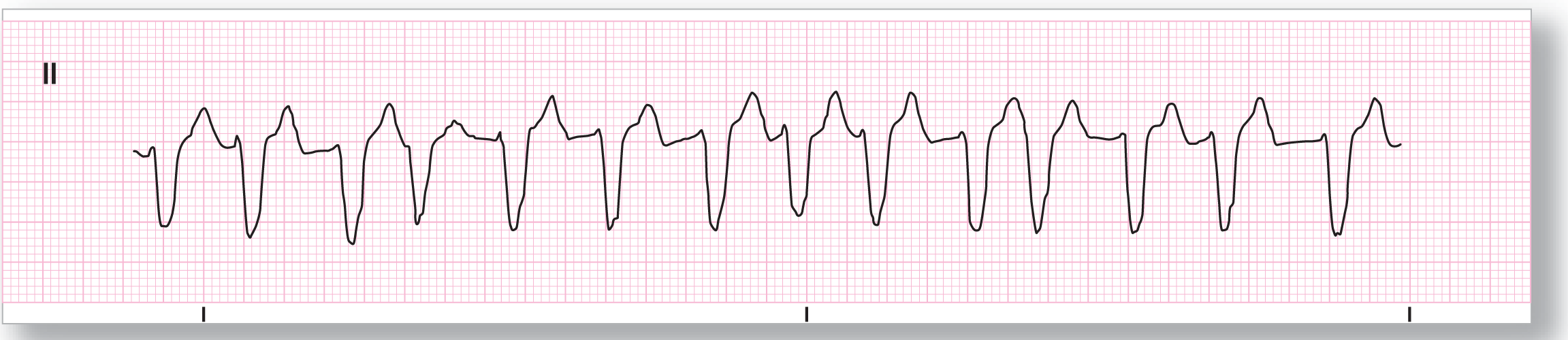
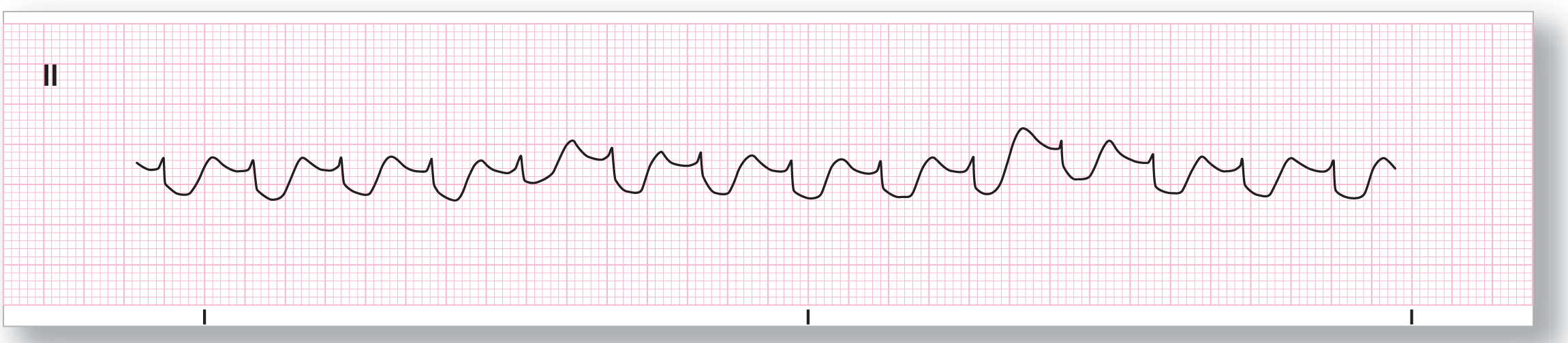
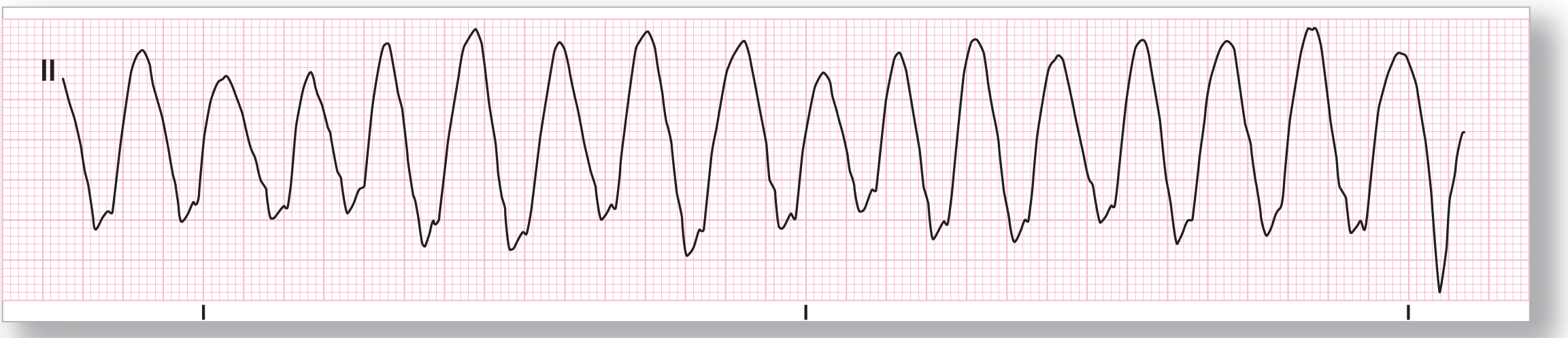
Rhythm: Accelerated idioventricular |
Discussion:
Test ECG-1 shows a wide-complex rhythm at about 76 BPM. The rhythm has no obvious P waves anywhere along the strip. The rate and the ventricular origin for this rhythm make the diagnosis accelerated idioventricular rhythm.
Test ECG-2

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: None |
PR intervals: Not applicable |
|
Regularity: Not applicable |
QRS width: Not applicable |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
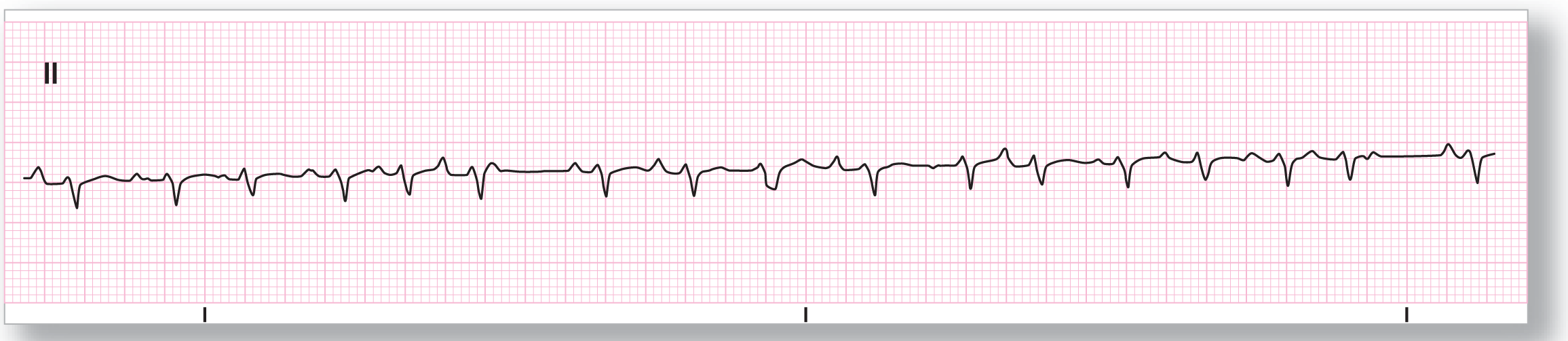
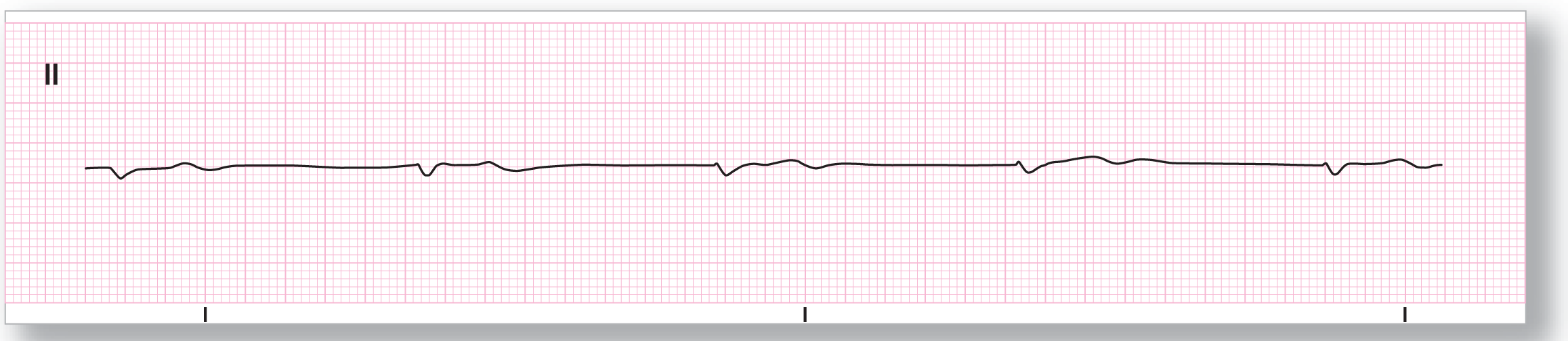
Rhythm: Asystole |
Discussion:
There are no obvious waves anywhere along Test ECG-2. This is an example of asystole. For completeness, remember to try various leads to make sure that you are dealing with asystole and not artifact or a completely isoelectric lead. Remember to always try to interpret any rhythm strip based on information gained from the clinical correlation with the patient.
Test ECG-3
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 115 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: Present, pseudo-R’ Morphology: Not applicable Axis: Not applicable |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: 1:1 |
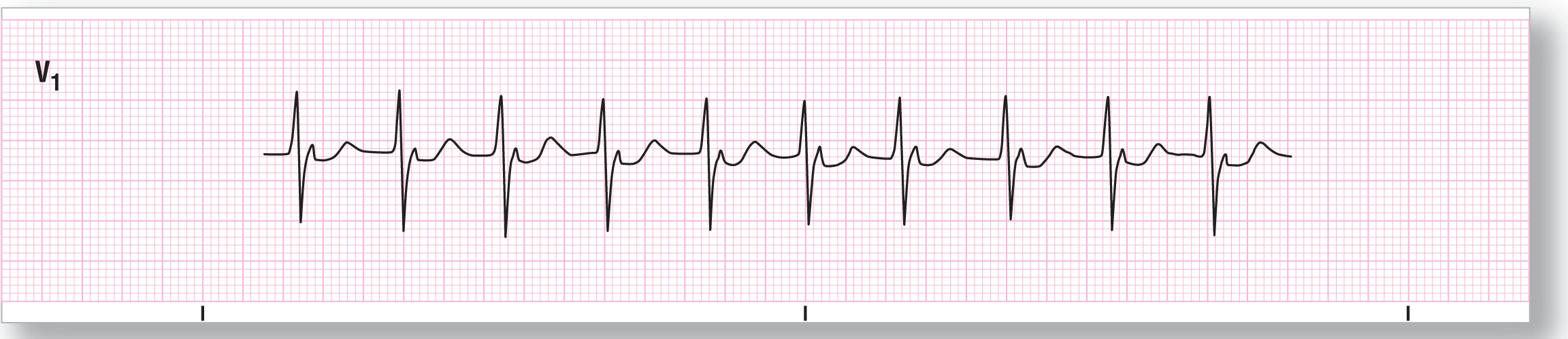
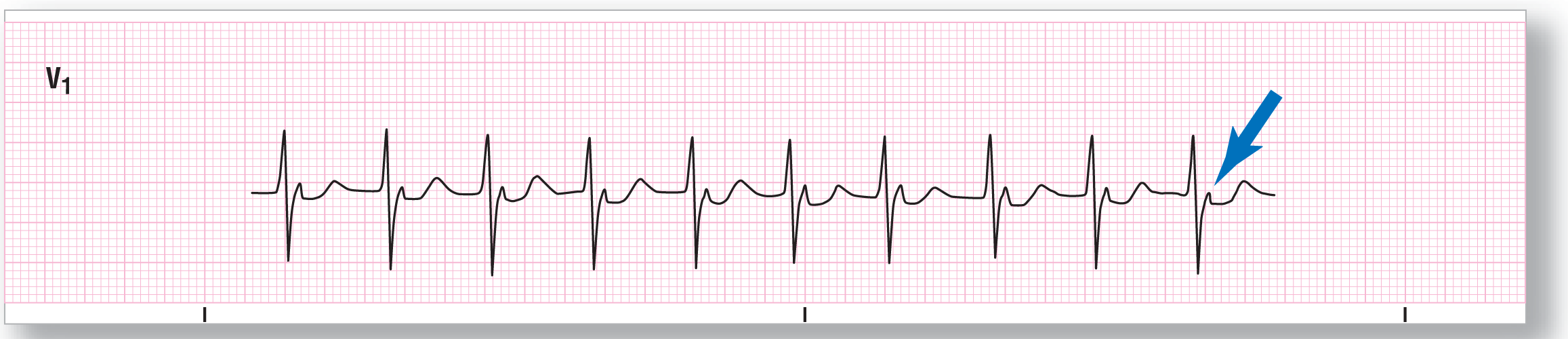
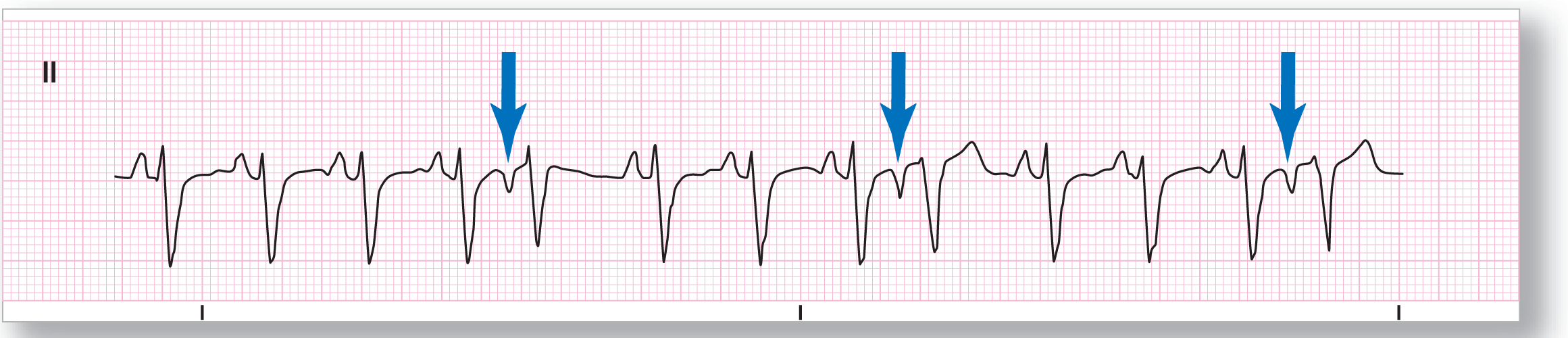
Rhythm: Accelerated junctional |
Discussion:
Test ECG-3 shows a narrow-complex tachycardia at a rate of about 115 BPM. There are no P waves noted before the QRS complexes. The R’, however, is consistent with the presence of a pseudo-R’ wave (see blue arrow). Remember, the pseudo-R’ is caused by an upright P wave buried within the QRS complex in lead V1 that simulates the presence of an R’ or r’ peak. They occur in either junctional, accelerated junctional, or AVNRT rhythms.
Test ECG-4
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 133 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
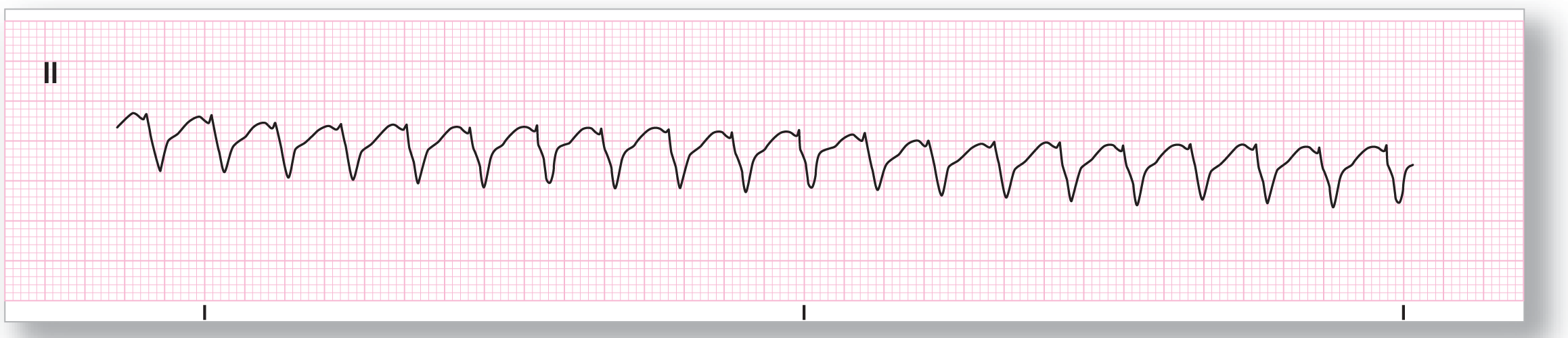
Rhythm: Monomorphic ventricular tachycardia |
Discussion:
Test ECG-4 brings up a typical problem seen when analyzing many patients with ventricular tachycardia: the small voltage of lead II. We are all used to seeing examples of VTach with large QRS complexes that are unmistakably ventricular in nature. The problem comes in when the VTach has a right bundle branch morphology. Typically, lead II shows small voltage, which could be either positive or negative. RBBB is a common morphologic presentation for VTach, so you will see this presentation very frequently. Because it appears benign, clinicians tend to downplay its importance. Be careful! A wide-complex tachycardia with or without AV dissociation should always be considered for VTach. A 12-lead ECG on this patient verified the presence of both VTach and an acute anteroseptal MI with lateral extension. The ST-segment depression present on this ECG was due to the reciprocal changes of the MI.
Test ECG-5

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 98 BPM |
PR intervals: Normal, except in events |
|
Regularity: Regularly irregular |
QRS width: Normal, except in events |
|
P waves: Present Morphology: Normal Axis: Normal |
Grouping: Yes |
|
Dropped beats: Yes |
|
|
P:QRS ratio: 1:1 except in events |
Rhythm: Sinus rhythm with ventricular trigeminy |
Discussion:
Test ECG-5 shows a sinus rhythm with a monomorphic PVC recurring every third beat. This is an example of a ventricular trigeminy. Note on the strip that the second P wave is a slightly different morphology than the others. This is, however, not a PAC because it arrives on schedule and has the same PR intervals as the others. This could be due to the firing of a different pacemaker within the sinus node itself or due to some slight artifactual difference. The pauses associated with the PVCs are fully compensatory, as you would expect.
Test ECG-6

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: Less than 20 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: Agonal rhythm |
Discussion:
Test ECG-6 shows ventricular complexes that are occurring at a very slow rate. It is slower than the lower limit typically seen in idioventricular rhythms. This is an example of an agonal rhythm. Remember, this is usually a terminal rhythm. If your patient has this rhythm, he or she doesn’t have much time. External or transvenous pacing, as well as drugs like atropine, are emergently indicated to try to speed up the rate and maintain a viable cardiac output. Epinephrine may also be helpful in these cases, but its use needs to be considered carefully.
Test ECG-7
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 120 BPM |
PR intervals: Normal, except in event |
|
Regularity: Regularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Normal, except in event Axis: Normal, except in event |
Grouping: None |
|
Dropped beats: See discussion |
|
|
P:QRS ratio: 1:1 |
Rhythm: Sinus tachycardia with frequent PACs |
Discussion:
Test ECG-7 shows an underlying sinus tachycardia at a rate of about 120 BPM. The sinus tachycardia is broken up by occasional PACs (see blue arrows). Notice that these complexes are triggered by inverted P waves with normal PR intervals. These findings indicate that the premature complexes originate in an ectopic atrial site and not in the junctional area. However, the pauses are fully compensatory, which is less typically found in PACs.
Test ECG-8

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: Variable rate |
PR intervals: See discussion below |
|
Regularity: Regularly irregular |
QRS width: See discussion below |
|
P waves: Present later in the strip Morphology: Normal Axis: Normal |
Grouping: None |
|
Dropped beats: Yes |
|
|
P:QRS ratio: See discussion below |
Rhythm: Monomorphic ventricular tachycardia becoming a sinus rhythm with ventricular bigeminy |
Discussion:
Test ECG-8 is an example of the events that occur at the termination of a run of VTach. Notice that at the onset of the strip, there is a monomorphic VTach at a rate of about 125 BPM. Then there is some slight irregularity in the rhythm, which is commonly seen in VTach at the start and the end of runs. The patient then has a sinus rhythm with ventricular bigeminy. Notice that the PVCs have the exact morphology as the complexes in the run of monomorphic VTach. Clinical correlation and a full 12-lead ECG should be considered to further evaluate this patient.
Test ECG-9
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 185 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: Monomorphic ventricular tachycardia |
Discussion:
Test ECG-9 is a tough strip! It is tough because there are a few things that this could be: AVNRT, AVRT, or ventricular tachycardia. There are no P waves or evidence of AV dissociation present. We do see evidence for the presence of Josephson’s and Brugada’s signs, pointing us towards VTach. The one thing that we know for sure is that this is a regular wide-complex tachycardia. So, what do we do now? Well, we treat it as a presumed VTach. A full 12-lead ECG verified the presence of ventricular tachycardia on this patient who was having an acute MI. As we have seen over and over again, clinical correlation and a full 12-lead ECG made the diagnosis clearer.
Test ECG-10
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 275 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
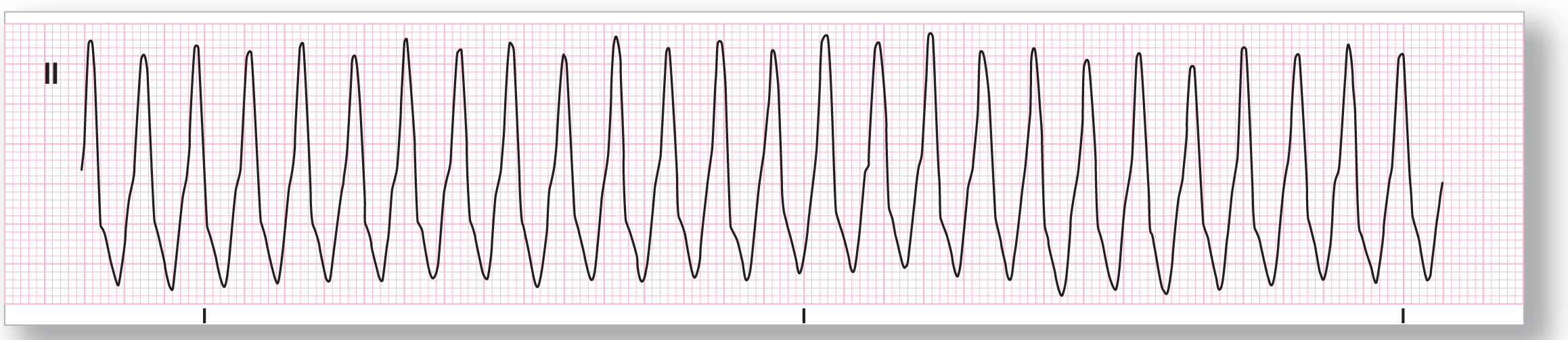
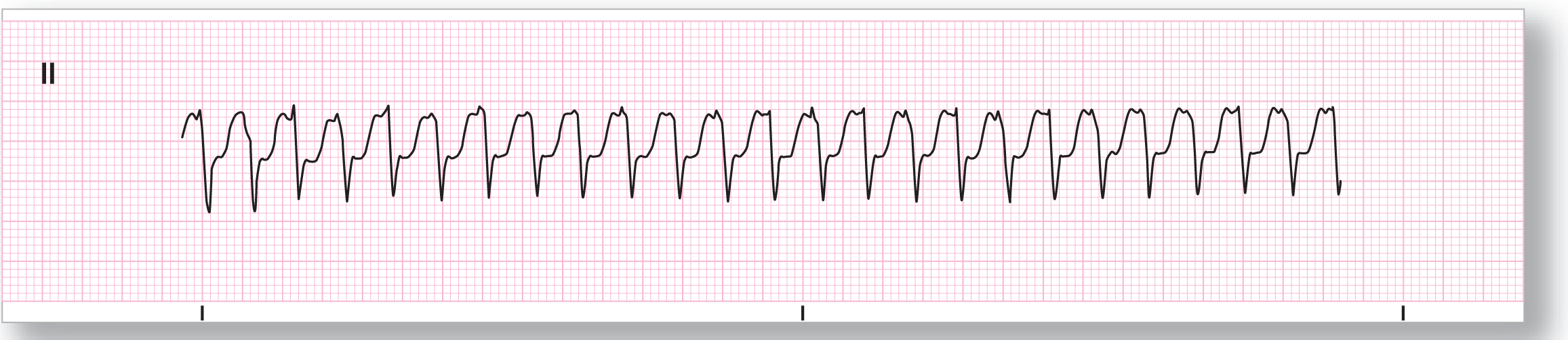
Rhythm: Antidromic AVRT |
Discussion:
Test ECG-10 is another example of small QRS complexes in a patient in VTach? The answer is no. The important diagnostic feature of this strip is the very rapid rate. A rate of about 275 BPM is simply too fast for a ventricular tachycardia. Ventricular flutter at this rate would have to have, by definition, an almost sinusoidal pattern with no discernible QRS or T waves. This strip shows clearly evident and discrete QRS complexes and T waves. Remember, when the rate exceeds 250 BPM, start thinking about rhythms caused by conduction through an accessory pathway. In this case, the wide QRS complexes make this an example of an antidromic AVRT.
Test ECG-11

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 93 BPM |
PR intervals: Normal, until rhythm change |
|
Regularity: See discussion below |
QRS width: Normal, until rhythm change |
|
P waves: Present Morphology: Normal Axis: Normal |
Grouping: None |
|
Dropped beats: Yes |
|
|
P:QRS ratio: 1:1 until rhythm change |
Rhythm: Sinus rhythm changing to torsade de pointes |
Discussion:
Test ECG-11 shows a patient who is in sinus rhythm at a rate of 93 BPM. The patient’s complexes, however, show an obvious QT prolongation, with a QT interval of 0.41 seconds. The QTc is 0.51 (QTc = QT/square root of R-R interval in seconds), which is markedly prolonged. Remember that the QTc is a value that takes into consideration the physiologic changes that occur in the QT interval due to rate. The patient has a PVC that falls on the T wave of the previous complex (R-on-T phenomenon) and triggers an episode of an undulating, irregular, wide-complex rhythm associated with polarity changes. This new rhythm is torsade de pointes.
Test ECG-12
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 47 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Normal |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: Junctional rhythm |
Discussion:
Test ECG-12 shows a slow narrow-complex rhythm that is regular. There are no obvious P waves anywhere along the strip. This is an example of a junctional rhythm.
Test ECG-13
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
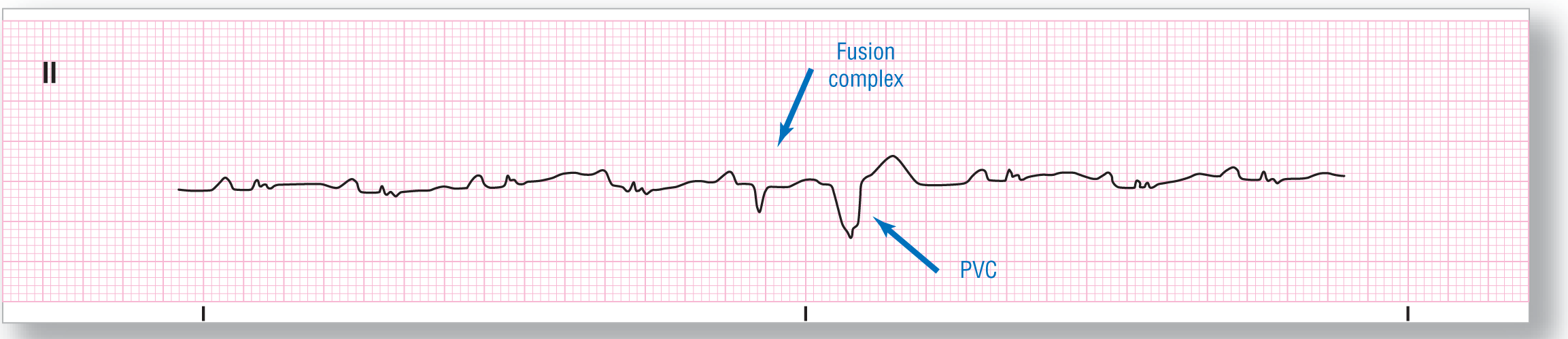
Rate: About 94 BPM |
PR intervals: Normal, except in event |
|
Regularity: Regularly irregular |
QRS width: Normal, except in event |
|
P waves: Present, except in event Morphology: Normal Axis: Normal |
Grouping: None |
|
Dropped beats: Yes |
|
|
P:QRS ratio: 1:1, except in event |
Rhythm: Sinus rhythm with a ventricular couplet |
Discussion:
Test ECG-13 shows a patient with very small voltage on the QRS complexes. The patient has an underlying sinus rhythm. After the fifth P wave, two different QRS complexes are noted. The second of these complexes is a clear PVC. The first of these two complexes, however, is completely different from either the normal QRS complex or the PVC. The PR interval of this complex is different, but the P wave is the same and the cadence is unchanged throughout the strip. This QRS complex is most probably a fusion complex involving the normally conducted supraventricular impulse and the PVC.
Test ECG-14
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
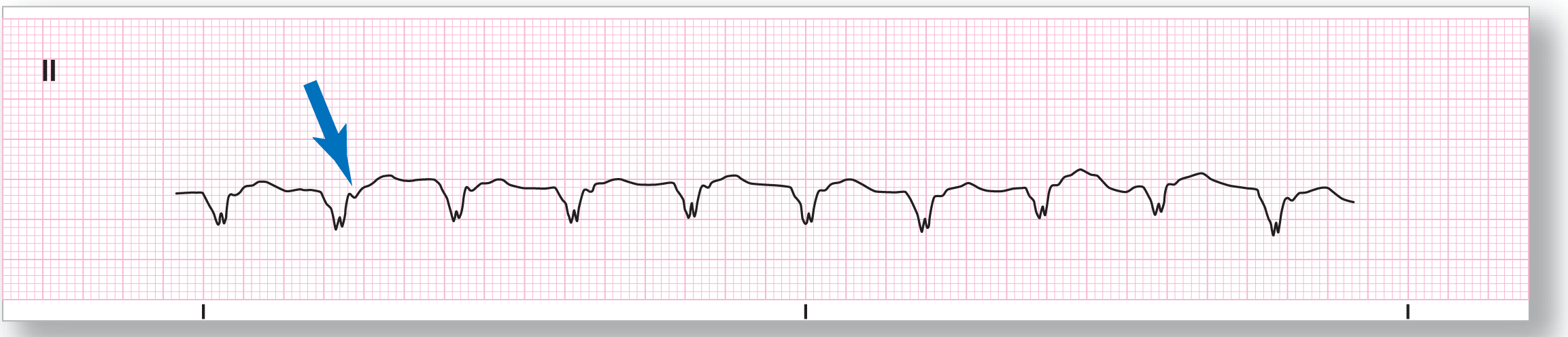
Rate: About 102 BPM |
PR intervals: See discussion below |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: See discussion below Morphology: See discussion below Axis: See discussion below |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: See discussion below |
Rhythm: Accelerated idioventricular |
Discussion:
Test ECG-14 shows a wide-complex tachycardia at a rate of about 102 BPM. The rhythm is regular and monomorphic in appearance. This is an example of an accelerated idioventricular rhythm. As a side point, the blue arrow points to a negative deflection within the ST segment. This is an inverted P wave due to the retrograde conduction of the ventricular impulse into the atria.
Test ECG-15
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 140 BPM |
PR intervals: Not applicable |
|
Regularity: Irregularly irregular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: Atrial fibrillation |
Discussion:
Test ECG-15 brings up a common clinical scenario that often causes patients to be misdiagnosed—the presence of a preexisting condition which causes wide QRS complexes. To start, the rate on this strip is rapid at about 140 BPM. Is this rhythm regular, regularly irregular, or irregularly irregular? The rhythm is irregularly irregular. The three main irregularly irregular rhythms are atrial fibrillation, WAP, and MAT. Are there any P waves anywhere on the strip? Since there are no visible P waves anywhere on this strip, the most probable diagnosis is atrial fibrillation. Why are the complexes wider than 0.12 seconds? The reason for the wide complexes in this patient is that there was a preexisting left bundle branch block. This is an example of an uncontrolled atrial fibrillation in a patient with a preexisting LBBB. The key to making the diagnosis in this patient was to answer the question about the chaotic timing of the complexes and not the presence of the wide complexes themselves.
Test ECG-16
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 100 BPM |
PR intervals: Not applicable |
|
Regularity: See discussion below |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
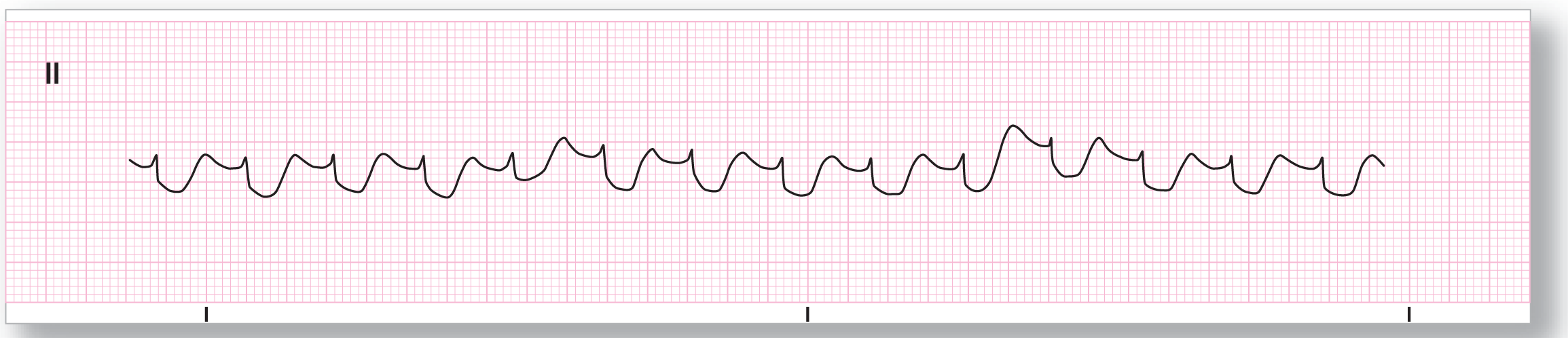
P:QRS ratio: Not applicable |
Rhythm: Polymorphic ventricular tachycardia |
Discussion:
Test ECG-16 is also very irregular. But, compare it to Test ECG-15. You will see that there are no obvious QRS complexes and T waves on this strip. There is also a wave-like undulation in the size of the QRS complexes throughout the strip. In addition, the undulations involve multiple complexes forming small groups. This is an example of a very slow polymorphic ventricular tachycardia. Clinical correlation was consistent with an acute MI in this patient.
Test ECG-17
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 100 BPM |
PR intervals: See discussion below |
|
Regularity: Regularly irregular |
QRS width: Normal, except in events |
|
P waves: Present, except in events Morphology: Normal Axis: Normal |
Grouping: None |
|
Dropped beats: Yes |
|
|
P:QRS ratio: See discussion below |
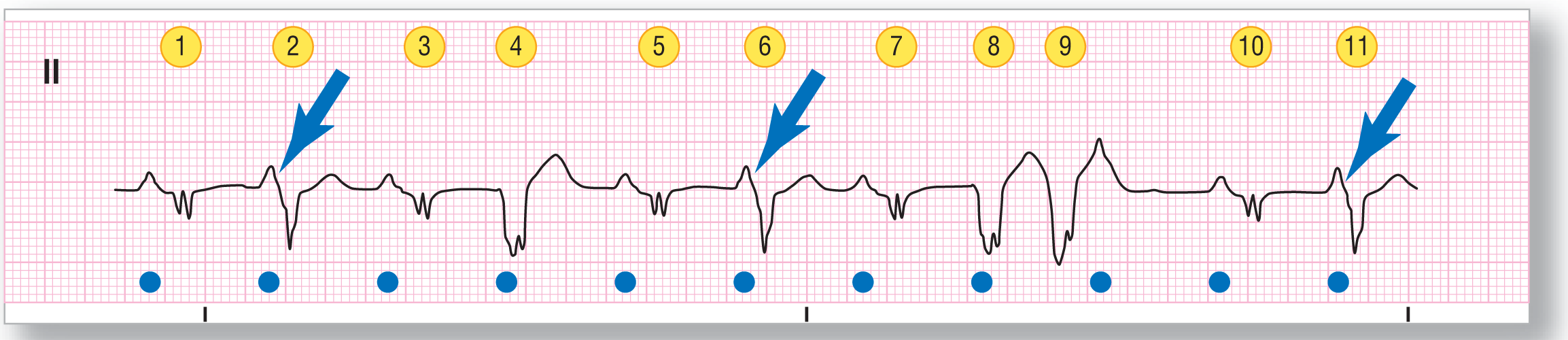
Rhythm: Sinus tachycardia with frequent PVCs and a ventricular couplet |
Discussion:
We figured that you were ready for a challenge by now. In Test ECG-17, we have labeled the ventricular complexes for easier identification and are using the blue circle to signify the atrial complexes. The morphology of the QRS complex labeled 1 is representative of the normally conducted complex. The baseline rhythm on this strip is a sinus tachycardia. Complexes 2, 6, and 11 are fusion complexes formed by the normally transmitted supraventricular complexes and PVCs. Complexes 4, 8, and 9 are PVCs. Note that the supraventricular rhythm marches throughout the strip essentially unchanged and causing a fusion between the P waves and the underlying PVCs and fusion complexes. Finally, the P waves in complex 2, 6, and 11 are themselves fused with the onset of their respective ventricular fusion complexes (see blue arrows). All in all, a very confusing rhythm strip.
Test ECG-18

From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
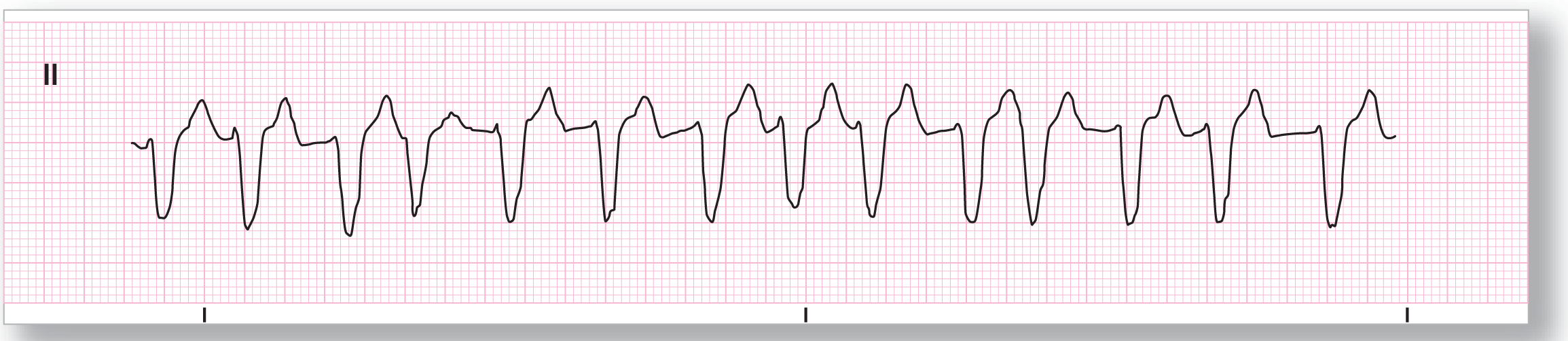
Rate: About 220 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
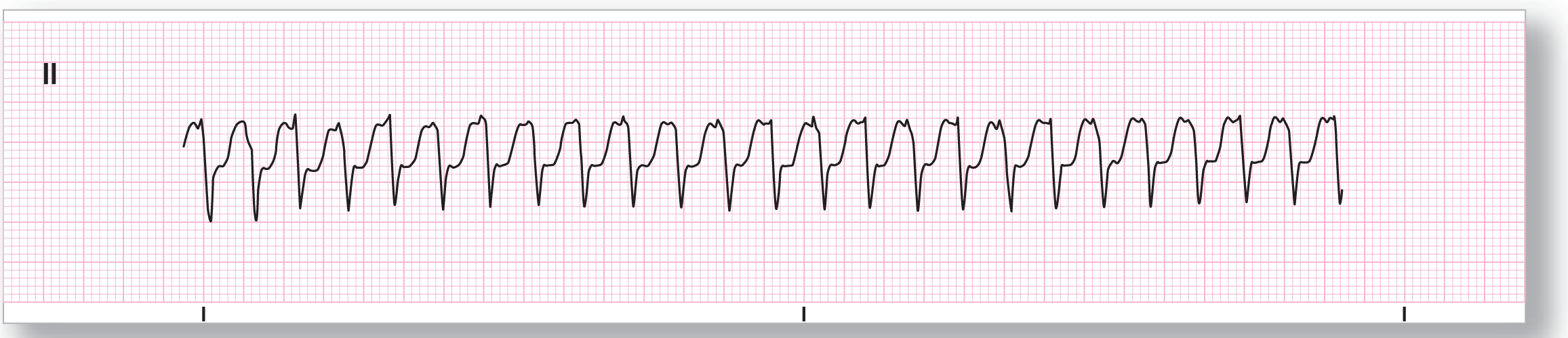
Rhythm: Ventricular flutter |
Discussion:
Test ECG-18 shows a wide-complex tachycardia with an almost constant sinusoidal pattern of the QRS complexes and the T waves. This is an example of ventricular flutter. Note that the polarity of the complexes does not change in this type of rhythm, compared to polymorphic ventricular tachycardia.
Test ECG-19
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
Description|
Rate: About 140 BPM |
PR intervals: Variable |
|
Regularity: Irregularly irregular |
QRS width: Normal |
|
P waves: Present Morphology: Variable Axis: Normal |
Grouping: None |
|
Dropped beats: See discussion below |
|
|
P:QRS ratio: 1:1 |
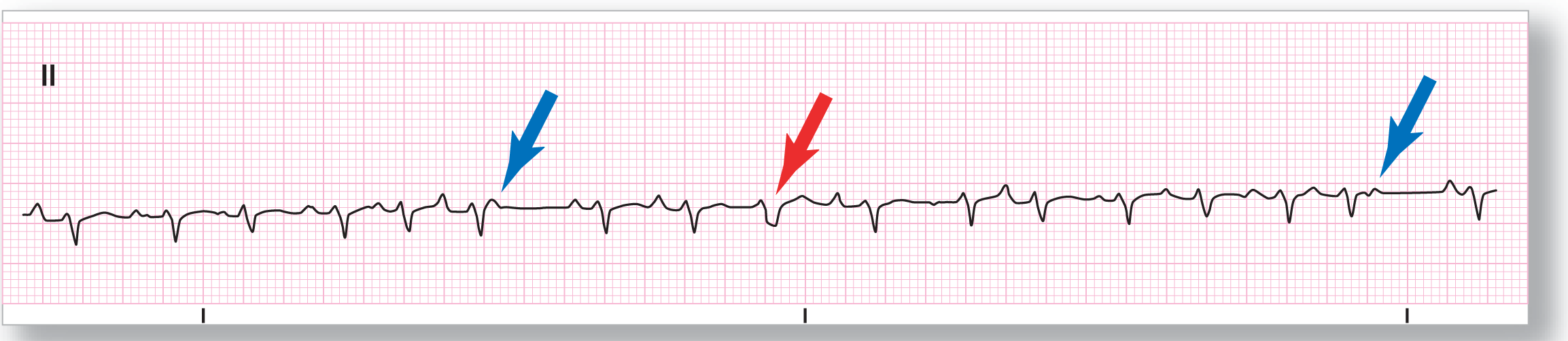
Rhythm: Multifocal atrial tachycardia |
Discussion:
Once again, there are three main irregularly irregular rhythms: atrial fibrillation, WAP, and MAT. Are there any P waves noted on Test ECG-19? Yes. This means that the rhythm, with rare exceptions, is going to be either WAP or MAT. The tachycardia makes MAT the most likely candidate. Now we need to prove our presumptive diagnosis. Do we have at least three different P-wave morphologies? Yes. Are they associated with different PR intervals? Yes. The diagnosis is now definitely MAT.
There are many buried P waves throughout the strip, as would be expected in a rapid MAT. In addition, there are two blocked P waves (see blue arrows). Finally, there is one complex labeled by the red arrow that most likely represents either a PJC with aberrancy or a PAC with aberrancy in a complex with an isoelectric P wave.
Test ECG-20
From Arrhythmia Recognition: The Art of Interpretation, courtesy of Tomas B. Garcia, MD.
|
Rate: About 39 BPM |
PR intervals: Not applicable |
|
Regularity: Regular |
QRS width: Wide |
|
P waves: None Morphology: None Axis: None |
Grouping: None |
|
Dropped beats: None |
|
|
P:QRS ratio: Not applicable |
Rhythm: Idioventricular rhythm |
Discussion:
Test ECG-20 shows a series of wide complexes at a rate of 39 BPM. There are no visible P waves anywhere along the strip. This strip could be due to a junctional rhythm with aberrancy, a preexisting condition leading to wide QRS complexes, or an idioventricular rhythm, the most probable option being an idioventricular rhythm. A full 12-lead ECG and clinical correlation would be needed in this patient to be completely sure of the diagnosis.