on stomach, lift head up 90 degrees1
on stomach, lift head up 90 degrees1Someone’s all smiles this month—and as a result, chances are you’ll be, too. Your infant is just entering what might be considered the golden age of babyhood—a period of several enchanted months when good humor reigns during the day, more sleep is happening at night, and independent mobility has yet to be achieved (which means your baby will continue to stay pretty much where you put him or her, limiting mischief and mayhem; enjoy this while it lasts). Sociable and interested, eager to strike up a cooing conversation, to watch the world go by, and to charm anyone within a ten-foot radius, babies this age are an undeniable delight to be around.
All babies reach milestones on their own developmental time line. If your baby seems not to have reached one or more of these milestones, rest assured, he or she probably will very soon. Your baby’s rate of development is normal for your baby. Keep in mind, too, that skills babies perform from the tummy position can be mastered only if there’s an opportunity to practice. So make sure your baby spends supervised playtime on his or her belly. If you have concerns about your baby’s development (because you’ve noticed a missed milestone or what you think might be a developmental delay), don’t hesitate to check it out with the doctor at the next well-baby visit—even if he or she doesn’t bring it up. Parents often notice nuances in a baby’s development that doctors don’t. Premature infants generally reach milestones later than others of the same birth age, often achieving them closer to their adjusted age (the age they would be if they had been born at term), and sometimes later.
By four months, your baby … should be able to:
on stomach, lift head up 90 degrees1
laugh out loud
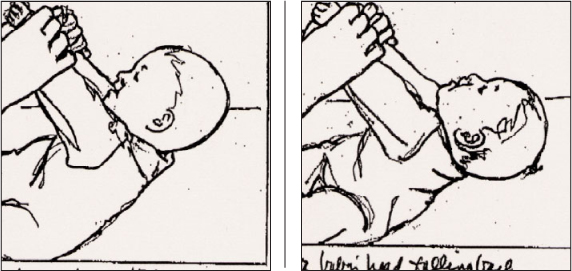
At the beginning of the fourth month, most babies still cannot keep their head level with their body when they are pulled to a sitting position (left). Their heads usually fall backward (right).
follow an object in an arc about 6 inches above the face for 180 degrees (from one side to the other)
… will probably be able to:
hold head steady when upright
on stomach, raise chest, supported by arms
grasp a rattle held to backs or tips of fingers
pay attention to an object as small as a raisin (but keep such objects out of baby’s reach)
reach for an object
squeal in delight
… may possibly be able to:
keep head level with body when pulled to sitting
roll over (one way)
turn in the direction of a voice, particularly mommy’s
say “ah-goo” or similar vowel-consonant combinations
razz (make a wet razzing sound)
… may even be able to:
bear some weight on legs when held upright
sit without support
object if you try to take a toy away
turn in the direction of a voice
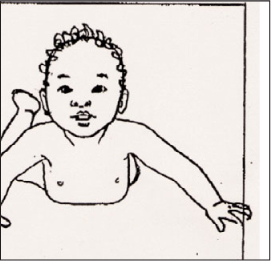
Many, but not all, four-month-olds can raise up on their arms.
Baby probably wasn’t scheduled for a checkup last month, so you’ve probably stored up a lot of questions in the meantime. Here’s your opportunity to ask them all. Since immunizations are also on the agenda at this visit, try (if possible) to get your questions answered before the shots are administered, so that baby will still be calm, and preferably dressed.
Each practitioner will have a personal approach to well-baby checkups. The overall organization of the physical exam, as well as the number and type of assessment techniques used and procedures performed, will also vary with the individual needs of the child. But, in general, you can expect the following at a checkup when your baby is about four months old:
Questions about how you and baby and the rest of the family are doing at home, and about baby’s eating, sleeping, and general progress, as well as child care if you are working out of the house.
Measurement of baby’s weight, length, and head circumference, and plotting of progress since birth.
Physical exam, including a recheck of any previous problems.
Developmental assessment. The examiner may actually put baby through a series of tests to evaluate head control, hand use, vision, hearing, and social interaction, or may simply rely on observation plus your reports on what baby is doing.
Second round of immunizations, if baby is in good health and there are no other contraindications. See the recommended schedule on page 231. Be sure to discuss any reactions to the first round of immunizations beforehand.
Guidance about what to expect in the next month in relation to such topics as feeding, sleeping, development, and infant safety.
Questions you may want to ask, if the doctor hasn’t already answered them:
What reactions can you expect baby to have to the second round of immunizations? How should you treat them? Which reactions should you call about?
When is a good time to start solids?
Also raise concerns that have arisen over the past month. Mention any developmental delays or missed milestones you may have noticed. Jot down information and instructions from the doctor. Record all pertinent information (baby’s weight, length, head circumference, birthmarks, immunizations, illnesses, medications given, test results, and so on) in a permanent health record.
The messages that a new parent receives about when to start feeding solids are many, and often confusing. Baby’s grandmother: “I started you before you were four months. What are you waiting for?” To back up her argument, she points to the obvious: “You’re healthy, aren’t you?” A well-meaning friend insists that starting solids earlier will help any baby sleep through the night. Her proof positive: a baby who’s slept through since his first spoonful of cereal. The pediatrician issues instructions to wait until baby is six months, citing the most recent recommendations and research.
Whom do you listen to? Does mother know best? Or friends? Or the doctor? Actually, your baby does—nobody can tell you when to start giving solids better than he or she can. Though the guidelines offered up by the medical community are certainly valid (probably more so than those offered up by grandma and friends), and should be used to set parameters—an infant’s individual development should be at least one of the deciding factors in promoting a baby to a more varied diet.
Very early introduction to solids isn’t believed to be physically harmful in most cases, though it can occasionally trigger allergies. But it isn’t wise, for a number of reasons. First, a young baby’s digestive system—from a tongue that pushes out any foreign substance placed on it, to intestines lacking many digestive enzymes—is developmentally unready for solids. Second, solids aren’t necessary early on—babies can fill all their nutritional needs for the first six months of life from breast milk or formula alone. Bringing on the solids too soon can also undermine future eating habits (baby may reject the cereal initially simply because he or she isn’t ready, then may reject it later because of prior parental pushing).
On the other hand, waiting too long—until late into the second half of the first year—can also lead to potential pitfalls. An older baby may resist being taught the new (and challenging) tricks of chewing and swallowing solids, preferring to cling to the tried-and-true (and easy) methods of tummy satisfaction: nursing or bottle feeding. And, like habits, tastes may be tougher to change at this point; unlike the more malleable six-month-old, the ten- or eleven-month-old may not be as open to opening wide for solids when he or she is so used to liquids.
To decide if your baby is ready for the big step into the world of solid foods (most will be between four and six months), look for the following clues, then consult the doctor:
Your baby can hold his or her head up well. Even strained baby foods should not be offered until a baby holds his head up well when propped to sit; chunkier foods should wait until a baby can sit well alone, usually not until seven months.
The tongue thrust reflex has disappeared. This is a reflex that causes young infants to push foreign matter out of their mouths (an inborn mechanism that protects them from choking on foreign bodies). Try this test: Place a tiny bit of infant rice cereal thinned with breast milk or formula in your baby’s mouth from the tip of a demitasse or baby spoon, or your finger. If the food comes right back out again with the tongue, and continues to after several tries, the thrust is still present and baby isn’t ready for spoon feeding.
Baby reaches for and otherwise shows an interest in table foods. The baby who grabs the fork out of your hand or snares the bread from your plate, who watches intently and exhibits excitement with every bite you take, is telling you he or she’s eager to sample more grownup fare.
The ability to execute back-and-forth movements with the tongue, as well as up-and-down ones, is present. You can discover this by observation.
Baby is able to open his or her mouth so that food can be taken from a spoon.
There are instances, however, when even a baby who seems developmentally ready for solids may have to wait—most often because there is a strong history of allergy in the family. Until more is known about the development of allergies, it is generally recommended that children in such families be breastfed for most of the first year, with solids added very cautiously, starting at six months. For more on starting solids, see page 312.
“My baby was doing very well at the breast—now, suddenly, he’s refused to nurse for the past eight hours. Could something be wrong with my milk?”
Something is probably wrong—though not necessarily with your milk. Temporary rejection of the breast, also called a nursing strike (even in nonunion babies), is not unusual and almost always has a specific cause, the most common of which are:
Mother’s diet. Have you been indulging in pasta al pesto or another dish redolent with garlic? Feasting your chops and chopsticks on General Tso’s chicken? Honoring Saint Patrick with corned beef and cabbage? If so, your baby may simply be protesting the spicy and/or strong flavors your diet is imparting to his milk. If you figure out what turns your baby off, avoid eating it until after you’ve weaned him. Many babies, on the other hand, don’t mind the strong spices in their mother’s milk, especially if they became accustomed to those flavors in utero through highly seasoned amniotic fluid; some especially relish the taste of spicy breast milk.
A cold. Babies who can’t breathe through stuffy noses can’t nurse and breathe through their mouths at the same time; understandably, they opt for breathing. Gently suction baby’s nostrils with an infant nasal aspirator, or ask your baby’s doctor about nose drops.
Teething. Though most babies don’t begin the struggle with teeth until at least five or six months, a few begin teething much earlier, and a very occasional baby actually sprouts a tooth or two in the first four months. Nursing often puts pressure on swollen gums, making suckling painful. When budding teeth are the cause of breast rejection, a baby usually starts nursing eagerly, only to pull away in pain.
An earache. Because ear pain can radiate to the jaw, the sucking motions of nursing can make discomfort worse. See page 553 for other clues to ear infection.
Thrush. If your baby has this fungal infection in his mouth, nursing may be painful. Be sure the condition is treated so that the infection isn’t passed on to you through cracked nipples, or spread elsewhere on the baby (see page 128).
Slow let-down. A very hungry baby may grow impatient when milk doesn’t flow immediately (in some women let-down may take as long as five minutes to occur), and may push away the nipple in a fury before let-down begins. To avoid this problem, express a little milk before you pick him up, so that he’ll get something for his efforts the moment he starts to suck.
A hormonal change in you. A new pregnancy (unlikely now if you’re nursing exclusively, more possible if you’ve started your baby on supplemental formula feedings) can produce hormones that change the taste of the breast milk, causing baby to reject the breast. So can the return of menstruation, which again isn’t usually an issue until partial weaning begins.
Tension in you. Maybe you’re stressed because you’ve recently returned to work. Maybe it’s because it’s bill-paying time, or because the dishwasher just broke—again. Maybe it’s just because you’ve had a really bad day. Whatever the reason, if you’re worried or upset you may be communicating your tension to your baby, making him too agitated to nurse. Try to relax yourself before offering the breast.
Readiness for weaning. This couldn’t be the case yet—though in a baby approaching his first birthday, breast rejection might be his way of saying, “Mommy, I’ve had it with nursing. I’m ready to move on.” Ironically, babies seem to do this when their mothers are not the least bit interested in weaning, rather than when mom’s ready to quit nursing.
Once in a while, there appears to be no obvious explanation for a baby’s turning down the breast. Like an adult, a baby can be “off his feed” for a meal or two. Fortunately, this kind of hiatus is usually temporary. In the meantime, these suggestions may help you ride out the nursing strike:
Don’t try substitutes. Offering a bottle of formula when your baby balks at the breast could exacerbate the problem by decreasing your milk supply. Most nursing strikes, even “long-term” ones, last only a day or two.
Try some breast in a bottle. Express some milk and give it to your baby in a bottle if he continuously rejects the breast (though this won’t work if it’s something in the milk that’s bothering him). Again, the strike’s likely to last only a day or two, after which your baby will be ready to take milk from the source again.
Try, try again. Even if he rejects it for a few feedings, chances are he’ll surprise you and start right back where he left off.
Slow down on solids. If you’ve started your baby on solid food, he may be eating too much, curbing his appetite for breast milk. At this age, breast milk is still more important than any solids, so cut down on the amount of solids you’re feeding and always offer the breast first.
If rejection of nursing continues, or if it occurs in connection with other signs of illness, speak to his doctor.
“My daughter won’t lie still when I’m changing her—she’s always trying to turn over. How can I get her to cooperate?”
As far as cooperation during diaper changes is concerned, you can expect to receive less and less as the months go by. The indignity of diapering, teamed with the turtle-on-its-back frustration of being temporarily immobilized, may set off a battle with each change. The trick: Be quick (have all the diapering paraphernalia ready and waiting before you lay baby on the table), and provide distractions (a mobile above the changing table, a music box, preferably one that’s also visually tempting, a rattle or other toy to occupy her hands and, hopefully, her interest). Engaging your baby in a song or a cooing conversation may also divert her long enough to get the job done.
“I had my baby propped up in his stroller, and I was scolded by two older women who insisted he was too young to sit up.”
If your baby wasn’t old enough to sit up, he’d tell you so. Not in so many words, of course, but by slumping down or sliding off to one side when you tried to prop him. Though you shouldn’t attempt to prop a younger infant whose neck and back need more support than he would get with propping, a three- or four-month-old who holds his head up well and doesn’t crumble when propped up is ready (and often very eager) for such a position. (Specially designed head supports are available to keep babies’ heads upright when propped.) Babies will usually signal when they’ve had enough of sitting by complaining or beginning to slump.
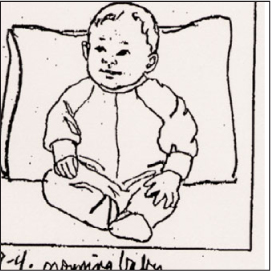
Propping baby up to a sitting position will offer him or her a welcome change of perspective, and it will also help build the muscles and experience needed for unassisted sitting.
Besides providing a welcome change of position, sitting allows a baby an expanded view of the world. Instead of just the sky or the inside of the stroller, an upright baby can see passersby (including those who are sure to chew you out), stores and homes, trees, dogs, other babies in strollers, children walking home from school, buses, cars—and all the other amazing things that inhabit his growing universe. He’s also likely to stay happy longer than he would lying down, which will make outings more pleasant for both of you.
“My baby likes to ‘stand’ on my lap. She cries if I make her sit down. But I’ve heard that standing so early can make her bowlegged.”
Babies usually know what they’re ready for better than anyone else. And many babies of your daughter’s age are ready, and eager, for supported lap “standing.” It’s fun, it’s good muscle-building exercise, it’s an exciting change from lying on her back or slumping in an infant seat—and it certainly does not cause bowleggedness.
On the other hand, any baby who doesn’t seem to want to stand shouldn’t be pushed into doing so until she’s ready. A baby who’s allowed to set her own developmental pace will be happier and healthier than one whose parents try to set it for her.
“I really need to keep my baby in the infant seat once in a while so I can get things done. But she fusses as soon as I put her in.”
Some babies are perfectly content to sit in an infant seat and watch the world (and their parents) go by; others—usually those born with more get up and go than they are able to get up and go with yet are bored and frustrated by stints in the seat. Your baby may be among those who resent and resist such confinement—in which case, keeping her content in infant seats (and car seats, and other places of enforced confinement) may be ever-challenging. To give yourself a fighting chance:
Limit the captivity. Reserve the infant seat for times when you absolutely need your baby safely confined and near your side (as when you’re cooking).
Try a change of scenery. An infant seat with a view is less likely to provoke instant rejection. Place the seat on the floor in front of a mirror (baby may enjoy interacting with her reflection), or in a safe spot next to you (there’s nothing more fascinating than a parent in action).
Add some entertainment. A toy bar can turn an ordinary infant seat into a personal entertainment center, particularly if toys are rotated to keep interest up and boredom from setting in. If toys seem to make baby fussier, it may be because she’s overtired or overstimulated, in which case removing the entertainment may calm her.
Make a motion. Turning on the rocking motion may soothe your baby while she’s in the seat (though some babies are actually upset by the movement; as always, take your cues from her reaction).
Let her loose. While younger infants are often satisfied to sit, older ones begin craving some freedom of movement. So instead of plunking her in the infant seat, try placing her on a blanket—tummy down—on the middle of the floor. This may not only placate her, but give her a chance to practice such skills as rolling over and creeping. The downside to this option while you’re trying to get things done: For safety’s sake, you’ll have to stay close by to supervise her efforts—which will limit the chores you can tackle.
Consider a different approach to confinement. It’s possible your baby has outgrown the infant seat, both physically and developmentally. If you need to keep her in one place sometimes, try a well-stocked play yard or an ExerSaucer instead (but limit use of both; see pages 398 and 333).
“My son cries every time I strap him into the car seat, making driving miserable for both of us.”
Though the purr of the car’s engine and the motion of driving are both soothing and sleep-inducing to many infants (some of whom will drop off to dreamland the moment the key’s in the ignition), not all babies (or their parents) agree that getting there is half the fun—especially when getting there means being strapped into a car seat. Rest assured that your son’s not the only confinement-phobic baby on the block staging his own version of Mutiny on the Highway. Fussing in the car seat is common behavior, particularly once children start becoming older and more active, and especially while they’re still forced to face the rear of the car. Of course, since riding unconfined is not only unsafe but illegal, letting him loose on the open road isn’t an option. Instead, try these suggestions for subduing the car seat rebellion:
Create a diversion. If your baby tends to wail the moment he spies the car seat, keep him busy while you’re buckling him up. Start singing a favorite song or holding up a favorite toy for him to look at as you attempt the dreaded procedure. With any luck, he won’t notice what you’re doing until the dirty work’s done.
Make him comfortable. Harness straps should be tight enough to ensure safety (you shouldn’t be able to fit more than two fingers between baby and harness), but not so tight that they pinch or dig into baby’s skin. Straps that are too loose, in addition to being unsafe, may also allow your son to slide around, which may add to his discomfort. And if he still doesn’t fill up the whole car seat, use inserts specially designed for smaller babies to make him more comfortable and less apt to flop from side to side. Also check the temperature in the back to make sure it’s not too hot or too cold (a blast of air-conditioning blowing on his face may upset him, for instance; if so, repositioning the vent may do the trick).
Block the sun. Many babies are unsettled by having the sun in their eyes; you may have it made if baby’s in the shade. So pull up the canopy on the seat, or invest in a window shade, available at baby stores.
Drive him with distraction. Put on some soothing music or a CD of lively children’s songs for you to sing along with. Equip the seat with car-safe toys that can’t be dropped (and rotate these often so baby won’t get bored). Place a specially designed mirror on the seat back in front of him (the view from a rear-facing car seat would bore anyone to tears); not only will the reflection entertain him, but if you position the mirror in the right way, you’ll be able to see his face in your rearview mirror.
Let him know you’re there. It’s lonely sitting in the backseat, especially while baby’s still in a rear-facing position. So do a lot of talking and singing (yes, even over the crying); the sound of your voice may eventually calm him down.
Try a little companionship. When two adults are in the car, one can buckle in next to baby and offer some live entertainment and reassurance. Older siblings can do the same (all children under the age of thirteen should ride in the backseat, anyway).
Bring the car seat home. You may be able to desensitize your son to the car seat by strapping him in at home for short periods of time, while lavishing him with toys and attention (to ensure a positive experience).
Give it time, but don’t ever give in. Eventually, your baby will come to accept the car seat (though he may never actually enjoy the ride in it). But giving in to his protests—even once, even just for a short ride—is not only incredibly dangerous (it takes only a moment for a crash to occur and for an unrestrained child to be injured or killed) but a strategic error, since it opens the door to future concessions.
“My son has taken to sucking his thumb. At first I was happy because it was helping him sleep better, but now I’m afraid it’s going to become a habit I won’t be able to break him of later on.”
It isn’t easy being a baby. Every time you latch on to something that gives you the comfort and satisfaction you’re searching for, somebody wants to take it away from you—sometimes without good reason.
Virtually all babies suck on their fingers at some time during the first year of life; many even begin the habit in the uterus. That’s not surprising. An infant’s mouth is an important organ, not just for eating but for exploration and pleasure, too (as you will soon discover, to your dismay, when everything baby picks up goes into his mouth, whether it’s a rattle or a long-deceased insect he’s unearthed at the bottom of a closet). But even before a baby can reach for objects, he discovers his hands—and how natural to put the newly discovered hands into that wonderful sensory cavity, the mouth. The first time, the hands may make it to the mouth by random chance, but the baby quickly learns that a mouthful of fingers provides a pleasurable sensation. Soon he’s mouthing his fingers regularly. Eventually, many babies decide that the thumb is the most efficient and satisfying finger to suck on (maybe it’s the most succulent) and switch from finger mouthing to thumb sucking. Some stick with one or two fingers, or even a whole fist.
At first you may think the habit is cute, or even be grateful that your baby has found a way to pacify himself without your help. Then, as the weeks pass and the habit intensifies, you begin to worry, envisioning your little boy trooping off to school with his thumb firmly implanted in his mouth, ridiculed by his classmates, reprimanded by his teachers. Will you have to make monthly trips to the orthodontist for the work necessary to straighten the bite deformed by thumb sucking, or, worse, weekly trips to the therapist to try to uncover the underlying emotional problems that made him suck on his thumb in the first place?
Well, stop worrying and start letting your baby indulge himself. There is no evidence that thumb sucking is in itself a sign of emotional neediness. Nor—if it ceases by age five—does it appear to do damage to the alignment of permanent teeth; any distortion of the mouth that does occur before that time returns to normal when the habit is ended. Since most children generally put the habit aside by age four to six, many experts say attempts to wean a child from the thumb don’t need to begin before then.
Some studies show that nearly half of all children do some thumb or finger sucking past infancy. The behavior peaks on average between eighteen and twenty-one months, though some have already abandoned the habit by then. Nearly 80 percent give it up by age five, and 95 percent by age six, usually on their own. Those who use it to help themselves get off to sleep or to comfort themselves in times of stress hang on to the habit longer than those to whom it is simply a form of oral gratification.
In the meantime, let your baby suck away. Be sure, however, that if he is breastfed, he isn’t sucking his thumb to compensate for suckling he isn’t getting at the breast; if he seems to want to nurse a little longer at each feeding, let him. And if thumb sucking seems to become the focus of his daily activities, preventing him from using his hands for other explorations, occasionally remove his finger from its station long enough to distract him with toys, with finger or hand games (“this little piggy,” “patty-cake,” or “so big,” for instance), or by holding his hands and letting him stand, if he likes that.
“Everybody admires my chubby little daughter. But I am secretly afraid she’s getting too fat. She’s so round, she can hardly move.”
With dimples on her knees and her elbows, a belly to rival any Buddha’s, an extra chin to chuck, and an endearing amount of pinchable flesh on her cheeks, she’s the picture of baby cuteness from head to chubby toes. Yet is the plump baby also the picture of health? Or is she on her way to becoming a fat child and an obese adult? With obesity tripling in the last three decades among American children ages six to eleven, that question has generated a great deal of interest among parents, doctors, and researchers.
One study has already found that babies who put on weight speedily in their first four months may be at an increased risk of obesity later on in life. But even without the benefit of research, there are clearly disadvantages to extreme chubbiness early on. The baby who is too plump to budge may become a victim to a vicious cycle of inactivity and overweight. The less she moves, the fatter she gets; the fatter she gets, the less she can move. Her inability to move makes her frustrated and fussy, which may lead her parent to overfeed her to keep her happy. If she stays overweight through age four, a problem that is becoming more and more common among American children, the odds that she will be an overweight adult grow greatly.
Before you make a reservation at the fat farm for your baby, however, be certain she is indeed overweight and not just nicely rounded (remember, since babies haven’t yet developed much in the way of muscle, even a slim one will sport soft padding; all babies need a certain amount of “baby fat”). Some parents, fearful that obesity will creep up on their offspring, misguidedly attempt to keep their perfectly normal babies thin by underfeeding them—which can be even more dangerous than overfeeding, leading to a failure to thrive, and possibly, to future eating disorders. Before you jump to any conclusions or take any action, compare her growth with the curve on the height-weight chart on page 782. If her weight seems consistently to be moving upward faster than her height (if they’re both moving up quickly, you probably just have a bigger-than-average baby on your hands), discuss this with her doctor.
Unlike the prescription for a chubby adult, the prescription for a chubby baby is not usually a diet. Instead of trying to get an overweight baby to lose weight, the goal is to slow down the rate of gain. Then as she grows taller, she will slim down—something many babies do without intervention as they become more active. Some of the following tips may help not only if your baby is already overweight, but also if you have good reason to believe she’s on her way:
Use feeding only to assuage hunger, not to meet other needs. A baby who’s fed for all the wrong reasons (when she’s hurt or unhappy, when her parent is too busy to play with her, when she’s bored in the stroller) will continue to demand food for the wrong reasons, and as an adult may eat for the same wrong reasons. Instead of feeding her every time she cries, comfort her with a hug or a soothing song. Instead of propping her up with a bottle, prop her in front of a mobile or a music box when you’re too busy to play with her; wear her in a baby carrier while you go about your routine; or let her watch what you’re doing from her infant seat. Instead of always plying her with teething biscuits to quiet her in the supermarket, attach a toy to her stroller to keep her occupied while you shop. In spite of what your mother may have believed, constantly pushing food on your baby is not a positive way to express love.
There’s nothing more wholesome for a baby than a bottle of juice, right? Actually, that’s wrong. Studies show that infants who drink too much juice—particularly apple juice—may become malnourished. That’s because juice (which isn’t very nutritious to begin with) can drown tender appetites for the breast milk or formula that should be the mainstay of a baby’s diet in the first year of life. Excessive juice consumption can also lead to diarrhea and other chronic tummy troubles, as well as tooth decay (a problem that’s especially common among babies who take bottles or sippy cups of juice to bed or suck on them all day long).
The American Academy of Pediatrics recommends that fruit juice not be given at all to infants under six months. After six months, parents should avoid giving any juice at bedtime, and only small amounts during the day (no more than 4 to 6 ounces total daily for children up to the age of six). Mixing the juice at least half-and-half with water will help ensure that your child won’t take in too much of the stuff, while minimizing the effects on tummy and teeth. (Get your baby used to such a mixture from the start, and the watered-down taste won’t be an issue later on.)
Your choice of juice matters, too. White grape, studies show, is less likely to cause stomach upset than that baby-standard apple, especially for babies who suffered from colic. Later on, look for juices that have something to offer besides calories—added calcium and vitamin C, for instance.
Make dietary adjustments, if necessary. One reason that breastfed babies are less likely to become overweight is that breast milk automatically adjusts to a baby’s needs. The lower-fat, lower-calorie foremilk, which comes at the beginning of a feeding, encourages the hungry baby to suckle. The higher-fat, higher-calorie hindmilk, which comes at the end of a feeding, tends to dampen the appetite, sending the message, “You’re feeling full.” If that isn’t discouragement enough, and baby continues to nurse away, the breast slows down the amount of milk produced toward the end of the feeding. Suckling for suckling’s sake can go on without an excess of calories being consumed. Though baby formulas aren’t customized in the same way, if your baby is gaining weight too quickly and is extremely overweight, her doctor may recommend switching to a lower-calorie formula. Before you make such a switch, however, be certain you are not underdiluting the ready-to-mix formula you are presently using—which could increase its calorie count per ounce considerably. Don’t decide to overdilute it, either, without the doctor’s okay. Or to switch to skim or low-fat milk. Babies, even overweight ones, need the cholesterol and fat in breast milk and formula until they’re a year old, and the same from whole cow’s milk between their first and second birthdays.
Try water, the ultimate calorie-free beverage. Most of us tend to drink too little water. Infant diets (because they are entirely, or almost entirely, liquid) don’t require supplementation with water. But water can be very useful for the overweight older baby who wants to keep sucking after her hunger is satisfied, or who is thirsty rather than hungry in hot weather. Instead of breast or formula, offer a bottle or cup of plain water (with no sugar or other sweetening added) when your baby seems to be looking for a nibble between meals—that is, within an hour or two of a previous feeding. (Getting your baby used to the taste, or rather the nontaste, of water early on will make it more likely that she’ll have the healthy habit of drinking water later.)
Don’t give solids prematurely as a way to encourage sleeping through the night—it doesn’t work and may lead to overweight. (Instead, try the tips for helping baby to sleep through the night on page 258.)
Evaluate your baby’s diet. If you’ve already started your baby on solids (on your own, or as recommended by her doctor) and she’s taking more than just a few spoonfuls of cereal, check to see if she seems to be drinking as much breast milk or formula as before. If she is, this is probably the reason for excessive weight gain. Cut back on solids if you’ve started them prematurely, or cut them out entirely for a month or two (most experts recommend not beginning solids until closer to six months anyway). Later, as more solids are added, the amount of breast milk or formula should usually be reduced gradually and the emphasis placed on solids such as vegetables, yogurt, fruits, cereals, and breads. If baby is taking juices (which she shouldn’t be before the age of six months, and which can lead to weighty problems at any age; see box, opposite page), dilute them, half-and-half with water. And don’t put thin cereal or other solids in a bottle for feeding—babies take too much that way.
Get your baby moving. If your baby can “hardly move,” encourage activity. When you change her diaper, touch her right knee to her left elbow several times, then the reverse. With her grasping your thumbs and your other fingers holding her forearms, let her “pull up” to a sitting position. Let her “stand” on your lap—and bounce, if she likes. (See page 305 for other tips on getting your baby moving.)
“All the other babies I see are all rolypoly; mine is long and thin—the 75th percentile in height and the 25th in weight. The doctor says he’s doing just fine and I shouldn’t worry, but I do.”
Thin continues to be in—everywhere but in the nursery. While the lean look is favored on adults, plumpness is what many look for and love in babies. And, yet, though they might not win as many diaper commercial roles as their roly-poly peers, slender babies are usually as healthy, sometimes more.
In general, if your baby is alert, active, and basically content, is gaining weight steadily, and if his weight, though on the low side of average, continues to keep pace with his height, there is, as the doctor has pointed out, no cause for concern. There are often factors that affect a baby’s size about which you can do very little. Genetic factors, for example—if you and/or your spouse are thin and small-boned, your baby is likely to be, too. And activity factors—the baby-on-the-go is usually leaner than the inactive one.
How does a baby grow? Quite contrary to the fears of nervous parents who scan weight and height charts for signs that all is well, usually in a pattern that’s normal for him or her.
A baby’s future height and weight are to a great extent preprogrammed at conception. And assuming prenatal conditions are adequate, and neither love nor nutrition is lacking after birth, most babies will eventually realize that genetic potential.
The programming for height is based primarily on the midpoint between the father’s height and the mother’s. Studies show that, in general, boys seem to grow up to be somewhat taller than this midpoint, girls somewhat shorter.
Weight also seems to be preprogrammed, to a certain extent. A baby is usually born with the genes to be slim, stocky, or a happy medium. But the eating habits learned in infancy and fostered throughout childhood can help to fulfill this destiny or defeat it.
Growth charts, like the one in the Ready Reference section in the back of this book, shouldn’t become a source of anxiety for parents—it’s too easy to misread or misinterpret them. But they are useful in telling parents and doctors when a baby’s growth is departing from the norm, and when an evaluation, taking into account parental size, nutritional status, and general health, is necessary. Since growth often comes in spurts during the first year, one measurement that seems to show too little growth or too much may not be significant. It should, however, be viewed as a red flag. A two-month halt to weight gain may indicate only that baby is slowing down because he or she is genetically destined to be small (particularly if growth in the height department is also easing off), but it can also indicate that baby is being underfed or is ill. A weight gain that is double what is normal during the same two months (if it is not accompanied by a similar jump in height) may just be baby’s way of catching up if birth-weight was low or weight gain has been slow so far, but it can also be a sign that baby is just plain eating too much.
There are, however, a few reasons for thinness that do need remedying. A major one is underfeeding. If a baby’s weight curve keeps dropping off for a couple of months, and if the loss isn’t compensated for by a jump the following month, the doctor often will consider the possibility that the child is not getting enough to eat. If you’re breastfeeding and this is the case, the tips on page 165 should help get baby gaining again. If you’re bottle feeding, you can try, with the doctor’s approval, diluting the formula a little less. Either way, supplementing with solids once the doctor green-lights them can help fill baby out.
Don’t underfeed intentionally. Some parents, eager to get their babies started on the path toward a future of slimness and good health, limit calories and fat in infancy. This is a very dangerous practice, since infants need both for normal growth and development. You can start them on the road to good eating habits without depriving them of the nourishment they need now.
Be sure, too, that your baby isn’t one who is either so sleepy or so busy that he forgets to demand his meals regularly. Between three and four months old, an infant should be eating at least every four hours during the day (usually at least five feedings), though he may sleep through the night without waking to eat. Some breastfed babies may still be taking more feedings, but fewer feedings could mean your baby isn’t eating enough. If your baby’s the kind who doesn’t make a fuss when he’s not fed, take the initiative yourself and offer meals to him more often—even if it means cutting short a daytime nap or interrupting a fascinating encounter with his crib gym.
Rarely, a baby’s poor weight gain is related to the inability to absorb certain nutrients, a metabolic rate that is out of kilter, or an infectious or chronic disease (in which case you would probably notice other symptoms). Such illness, of course, requires prompt medical attention.
“The doctor says my baby has a heart murmur but that it doesn’t mean anything. Still, it’s scary.”
Any time the word heart is part of a diagnosis, it’s scary. After all, the heart is the organ that sustains life; any possibility of a defect is frightening, particularly to the parents of an infant whose life is just beginning. But in the case of a heart murmur, there is, in the vast majority of cases, really nothing to worry about.
When the doctor tells you your baby has a heart murmur, it means that on examination, abnormal heart sounds, caused by the turbulence of the flow of blood through the heart, are heard. The doctor can often tell just what kind of abnormality is responsible for the murmur by the loudness of the sounds (from barely audible to almost loud enough to drown out normal heart sounds), by their location, and by the type of sound—blowing or rumble, musical or vibratory—for example.
Most of the time, as is likely in your baby’s case, the murmur is the result of irregularities in the shape of the heart as it grows. This kind of murmur is called “innocent” or “functional,” and can usually be diagnosed by the baby’s doctor by simple office examination with a stethoscope. No further tests or treatments or limitations of activities are necessary. More than half of all children have an innocent murmur sometime during their lives, and it is likely to come and go throughout childhood. But the existence of the murmur will be noted on your baby’s record so other doctors who examine him at a later date will know it has always existed. Very often, when the heart is fully grown (or sometimes earlier), the murmur will disappear.
If you’re worried no matter what anyone says, you can ask your baby’s doctor to tell you exactly what type of murmur your baby has and whether or not it can be expected to cause any problems, now or in the future, and to explain just why you have nothing to worry about. If the answers aren’t reassuring enough, ask for a referral to a pediatric cardiologist for consultation.
“My daughter’s last diaper was filled with a black stool. Could she be having a digestive problem?”
More likely she’s been having an iron supplement. In some children, the reaction between the normal bacteria of the gastrointestinal tract and the iron sulfate in a supplement causes the stool to turn dark brown, greenish, or black. There’s no medical significance in this change, and no need to be concerned by it since studies show that small amounts of iron don’t increase digestive discomfort or fussiness. On the other hand, for most babies an iron supplement isn’t recommended (breastfed infants get enough iron from breast milk; bottle-fed babies get enough from iron-fortified formula; fortified cereal provides iron later). So unless your baby’s doctor has prescribed one, you should discontinue dosing baby. If your baby has black stools and isn’t taking a supplement, check with her doctor.
“I’ve heard that massage is good for babies. Should I massage my son?”
Massage is no longer for adults only. For some years it’s been known that premature newborns do better with therapeutic massage—they grow faster, sleep and breathe better, and are more alert. Now it appears that massage also benefits healthy infants—and healthy children, as well.
There are a number of reasons why you should consider laying the hands on your baby. We know that being held, hugged, and kissed by a parent helps a baby thrive and enhances parent-child bonding. But the therapeutic touch of massage may do that and even more, possibly strengthening the immune system; improving muscle development; stimulating growth; easing colic, teething pain, and tummy troubles; promoting better sleep patterns; stimulating the circulatory and respiratory systems; and decreasing stress hormones (yes, babies have those too). And a loving touch (whether in the form of massage or just a lot of hugging and holding) has also been shown to decrease aggressive tendencies in children. What’s more, baby’s not the only one who stands to benefit; massaging an infant is actually relaxing for parents, too—and has been found to relieve symptoms of postpartum depression.
If you’d like to learn how to rub your baby, get a book or video, or take a class with a massage therapist familiar with baby massage. Or try these tips:
Pick a time that’s relaxing for you. The massage won’t have the desired effect if the phone’s ringing, dinner’s burning on the stove, and you have two loads of laundry going. Choose a time when you’re unhurried and unlikely to be interrupted, and take the phone off the hook or turn off the ringer and let voice mail take a message (a ringing phone—even one answered by machine—is distracting).
Pick a time that’s relaxing for baby. Don’t massage baby when he’s hungry or full. Right after a bath is a perfect time, when baby has already started to relax (unless he hates the bath and it leaves him riled). Before playtime is another possibility, since babies have been shown to be more focused and attentive after a massage.
Set a relaxing scene. The room you select for the massage should be quiet and warm, at least 75°F (since baby will be undressed except for a diaper). Dim the lights to reduce stimulation and enhance relaxation, and add soft music if you like. You can sit on the floor or bed, and lay baby on your lap or between your open legs; use a towel, blanket, or a pillow covered by a towel or blanket under baby.
Lubricate, if you like. You can give your baby a dry rub, or use a little baby oil, vegetable oil, or baby lotion (but not on baby’s head). Warm the oil or lotion a little between your hands before you start rubbing.
Experiment with techniques. In general, babies prefer a gentle touch—but not so light that it’s ticklish. Here are a few ideas to get you started:
Gently place both of your hands on either side of your baby’s head and hold for a few seconds. Then stroke the sides of his face, continuing down the sides of his body to his toes.
Make tiny circles on baby’s head with your fingers. Smooth baby’s forehead by gently pressing both hands from center outward.
Stroke baby’s chest from center outward.
Stroke baby’s tummy from top to bottom using the outer edge of one hand, then the other, in a circular motion. Then, let your fingers do the walking across your baby’s tummy.
Gently roll baby’s arms and legs between your hands or use firmer, deep strokes to “milk” baby’s arms and legs. Open those curled-up hands and massage those little fingers.
Rub baby’s legs up and down, alternating hands. When you get down to the feet, massage them, uncurling and stroking baby’s toes.
Turn baby on his tummy, and stroke his back from side to side, then up and down.
While you work, talk or sing softly. Always keep one hand on baby.
Take your cues from baby. He will tell you whether you’re rubbing him the right way or not. He’ll also tell you when to keep rubbing, and when it’s time to end the massage session.
“I’ve heard a lot about the importance of exercising your baby. Is it really necessary for me to take my little girl to an exercise class?”
Americans tend to be extremists. Either they’re totally sedentary, getting all their exercise by turning on the TV and reaching for a beer, or they embark on an overly rigorous jogging program that lands them injured in the sports specialist’s office within a week. And either they confine their babies to a stationary life in high chairs, strollers, and play yards, or they rush out and enroll them in exercise classes the moment they can lift their heads, in hopes of creating a fit-for-life infant athlete.
But extremism in the pursuit of good health tends to be ineffective, and is usually doomed to failure. Moderation is a much better goal to aim for, in your lifestyle and your baby’s. So instead of ignoring your baby’s physical development or pushing her beyond her abilities, take the following steps to start her on the road to fitness:
Stimulate body as well as mind. Many parents make an effort to teach their children intellectual matter from the cradle but figure the physical will take care of itself. And, for the most part, it will—but paying a little extra attention to it will remind both you and your baby of its importance. Try to spend some part of your playtime with your baby in physical activity. At this stage, it may be nothing more than pulling her to a sitting position (or a standing one, when she’s ready), gently raising her hands over her head, “bicycling” her legs by bending her knees up to meet her elbows in a rhythmic way, or holding her up in the air with your hands around her middle, making her flex her arms and legs.
Make the physical fun. You want her to feel good about her body and about physical activity, so be sure she enjoys these little sessions—and certainly don’t be serious about them yourself. Talk or sing to her and tell her what you’re doing. She’ll come to identify little rhythmic ditties (such as “Exercise, exercise, how I love my exercise”) with the fun of physical activity.
Don’t fence her in. A baby who’s always strapped safely into a stroller or an infant seat or snuggled into a baby carrier, without opportunity for physical explorations, is well on her way to becoming a sedentary—and a physically unfit—child. Even an infant who’s too little to crawl can benefit from the freedom to move that a blanket on the floor or the center of a large bed (with constant supervision, of course) can offer. On their backs in such a position, many three- and four-month-olds will spend great stretches of time attempting to turn over (help them practice by slowly turning them over and back again). On their bellies, many will inch around, exploring with their hands and mouths, pushing their bottoms up in the air, raising their heads and shoulders. All of this activity naturally exercises tiny arms and legs—and is impossible to duplicate in a confined space.
Keep it informal. Exercise classes or taped programs for infants are not necessary for good physical development, and if they’re the wrong kind or are used in the wrong way, they can be detrimental. Babies, given the opportunity, naturally get all the exercise they need. That said, such activities can be fun for both of you—an opportunity to play and interact with other parents and other babies, and to try things you might not be able to try at home. If you do choose to take your baby to an exercise program, check the program first for the following:
Do teachers have good credentials? Is it safe? Ask your baby’s doctor for an evaluation before you sign up. Also observe. Any program that encourages exercises that jostle or shake babies is a dangerous one (see page 272). Beware, too, of classes that are high-pressure, rather than fun, encouraging competition instead of individual growth.
Do babies seem to be having fun? If an infant isn’t smiling or laughing while exercising, she isn’t enjoying it. Beware especially if the babies seem confused or frightened, or pressured to do things that make them uncomfortable.
Is there plenty of age-appropriate equipment for your baby to play with—for instance, at this age, brightly colored mats, inclines to creep up, balls to roll, toys to shake?
Are babies given plenty of opportunity for free play—explorations made on their own and with you? Most of the class should be devoted to this, rather than structured group activities.
Is music an integral part of the program? Babies like music and rhythmic activities, such as rocking and singing, and the two go together well in an exercise program.
Let baby set her pace. Pushing a baby to exercise, or to do anything else she isn’t ready for or in the mood for, can set up very negative attitudes. Begin exercise with your baby only when she seems receptive, and stop when she tells you, by her indifference or fussiness, that she’s had enough.
Keep her energized. Good nutrition is as important to your baby’s good physical development as exercise. Once solids are introduced (with the doctor’s permission, of course), start her on the First-Year Diet (see page 316) so that she has the energy needed for fun and games and the nutrients for optimal development.
Don’t be an unfit parent. Teach by example; the family that exercises together stays fit together. If your child grows up watching you walking half a mile to the market instead of driving, doing daily aerobics in front of the TV instead of munching chips, swimming laps in the pool instead of sunbathing alongside it, she’s more likely to enter adulthood with good feelings about fitness that she can pass on to her own offspring.
Walking into a toy store is like walking into a carnival in full swing. With every aisle vying for attention with its selection of eye-catching wares, bombarding the senses and sensibilities with an endless array of colorful boxes and displays, it’s hard to know where to start. And though such trips can bring out the child in any adult, for parents several responsibilities come along with the joys of choosing toys.
To make sure you don’t succumb to the prettiest packages and the most alluring gimmicks the toy industry has to offer, and end up with a vast collection of the wrong toys for your baby, consider these questions when contemplating a purchase—or when deciding whether to keep out, shelve, or return to the store playthings that have come as gifts:
Is it age-appropriate? The most obvious reason for making sure a toy you purchase is age-appropriate is so that your baby will appreciate it and enjoy it fully now. A less apparent reason, though, is just as important. Even an advanced baby who might be interested in a toy that’s classified as appropriate for older children, and who might even manage to play with it on a primitive level, could be harmed by it, since age-appropriateness also takes safety into consideration. Giving your baby toys before he or she is ready for them has another disadvantage, as well; it’s possible that by the time baby is ready for them, he or she will also be bored by them.
How can you tell if a toy is appropriate for your baby? One way is the age range listed on the packaging, though your baby may be able to appreciate a particular toy a little earlier or a little later than average. Another is to observe your child with the toy—if you have the toy already or can try it out at a friend’s house or the store. Is he or she interested in it? Does he or she play with it the way it’s meant to be played with? The right toy will help your baby to perfect skills already learned or promote the development of new ones just about to be tackled. It will be neither too easy (which encourages boredom) nor too difficult (which promotes frustration).

For a baby, playtime is learning time. A game of peekaboo will elicit delighted giggles from a three- or four-month-old, and it will help teach the important lesson of object permanence: When mommy hides her face behind her hands, she’s still there.
Nearly every stuffed animal your baby will encounter will be lovable and huggable. Here’s how to make sure those teddies, giraffes, bunnies, and doggies are as safe as they are cute:
Eyes and noses on animals should not be made of buttons or other small objects that could fall off (or be pried or chewed off) and pose a choking hazard. Screen for buttons elsewhere, too (such as on a teddy bear’s suspenders).
No wire should be used to attach parts (such as ears). Even if the wire is covered by fabric, it could be chewed off or worn off and pose a puncture hazard.
No strings should be attached—that goes for bows around the bunny’s neck, a leash on the dog, and so on—longer than 6 inches.
Look for sturdy construction; seams and connections that are tightly sewn. Check periodically for wear that could allow stuffing to come out (which would pose a choking hazard).
All stuffed animals should be washable, and should be washed periodically so germs don’t collect on them.
Never place stuffed animals in baby’s crib; they can pose a suffocation hazard.
Is it stimulating? Every toy doesn’t have to bring your baby one step closer to that college acceptance letter; babyhood (and childhood) are times for just plain fun, too. But your baby will have more fun with a toy if it’s stimulating to the sense of sight (a mirror or a mobile), hearing (a music box or a clown with a bell in his belly), touch (a cradle gym or activity board), or taste (a teething ring, or anything else that’s mouthable) than if it’s merely cute. As your baby grows, you will want toys that help a child learn hand-eye coordination, large and small motor control, the concept of cause and effect, color and shape identification and matching, auditory discrimination, spatial relationships, and those that stimulate social and language development, imagination, and creativity.
Is it safe? This is perhaps the most significant question of all, since toys (not including bikes, sleds, Rollerblades, scooters, and skateboards, which cause hundreds of thousands of injuries of their own) are responsible for over 100,000 injuries a year. In selecting playthings for your baby, look for the following:
Sturdiness. Toys that will break or fall apart easily can often cause injury to a young child.
Safe finish. Be sure that the paint or other finish isn’t toxic.
Safe construction. Toys with sharp edges or breakable parts are unsafe.
Washability. Toys that can’t be washed can become breeding places for bacteria—a problem for infants, who put everything in their mouths.
Safe size. Toys that are small enough to pass through a small-parts tester or a toilet paper tube or have small removable parts or parts that can be broken off, present a serious choking hazard. Ditto toys that pieces can be chewed off of once teeth have emerged.
Safe weight. Toys that can harm your baby if they fall on him or her are unsafe.
No strings attached. Toys (or anything else) with strings, cords, or ribbons longer than 6 inches should never be left anywhere near a baby because of the strangulation risk. Toys can be attached to cribs, playpens, and elsewhere with plastic links that are not only safe, but bright and attractive playthings in themselves.
Safe sound. Loud sounds—for example, from toy guns, model planes, or motorized vehicles—can damage baby’s hearing, so look for toys that have musical or gentle sounds rather than sharp, loud, or squeaky ones.
Do you approve of it philosophically? This is less of a problem in infant toys than it will be later, but it’s not too early to think about the subliminal message a toy is sending, and to consider whether that message agrees with your values. Don’t let society—at least the part of society that creates some of the TV-generated toy mayhem for children—decide what you want your baby to play with.

1. Babies who spend little time on their stomachs during playtime may reach this milestone later, and that’s not cause for concern (see page 210).