![]()
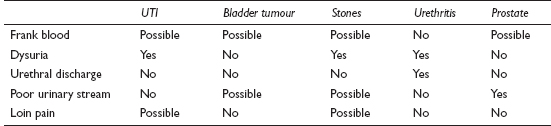
Bright red blood in the urine causes instant alarm in a patient, and usually generates an emergency appointment or an out-of-hours call. Blood may also be picked up by dipstick testing or MSU during the assessment of some other problem or in a routine medical. This is often less frightening even when disclosed to the patient, but should prompt full investigation.
![]()
COMMON
 UTI
UTI
bladder tumour
renal/ureteric stones
urethritis
prostatic hypertrophy/carcinoma of prostate
OCCASIONAL
jogging and hard exercise
renal carcinoma
chronic interstitial cystitis
anticoagulant therapy
nephritis/glomerulonephritis
RARE
renal tuberculosis
polycystic kidney disease
blood dyscrasias: thrombocytopenia, haemophilia, sickle-cell disease
infective endocarditis
schistosomiasis (common abroad)
trauma
![]()
![]()
LIKELY: urinalysis, MSU, FBC, U&E, ACR/PCR.
POSSIBLE: PSA, ultrasound, plain abdominal X-ray, IVU, cystoscopy.
SMALL PRINT: urethral swab, CT scan, urine cytology, renal biopsy, angiography.
Urinalysis: pus cells and nitrite in UTI. Pus cells alone in urethritis, TB and bladder tumour. Presence of protein suggests renal disease.
Urine microscopy and culture to establish pathogen in infection. May show casts in renal disease.
FBC and U&E help establish basic renal function and any associated anaemia or leucocytosis; consider PSA – usually elevated in prostatic carcinoma.
ACR/PCR: to quantify any proteinuria.
Urethral swabs if urethritis (best done at GUM clinic).
If painless haematuria, ultrasound may show renal tumour or polycystic kidneys; CT may be more useful.
IVU is investigation of choice if renal/ureteric stones are suspected (when pain is present); plain abdominal X-ray useful when attack has settled (reveals 90% of stones). IVU also required if ultrasound, abdominal X-ray and cystoscopy are all negative.
Specialist investigations include cystoscopy, urinary cytology, renal biopsy and angiography.
Microscopic haematuria in an asymptomatic menstruating woman can be ignored temporarily; repeat the urinalysis at mid-cycle.
Remember that there are other less common causes of spurious haematuria – sometimes the blood may be coming from the rectum or vagina. Assess each case carefully and be prepared to rethink if symptoms persist but urological investigations prove negative.
Some food pigments, beetroot and certain drugs (e.g. nitrofurantoin) can colour the urine red – confirm haematuria with urinalysis to save the patient unnecessary tests.
Painless frank haematuria is an ominous sign indicating possible malignancy.
Beware of recent onset of recurrent cystitis with haematuria in the elderly. The underlying cause may be a bladder tumour, especially if the haematuria (micro- or macroscopic) does not settle with treatment of the infection.
Renal tumours can sometimes present with renal colic, as blood clots in the ureters mimic the effects of stones. A useful clue is that the bleeding may precede the pain.
Haematuria requires emergency admission if there is significant blood loss or clot retention.
![]()
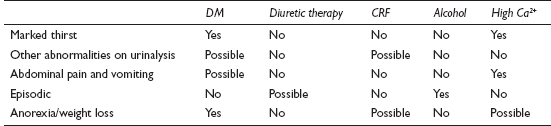
Polyuria is a highly subjective symptom and one which presents rather less often than urinary frequency (which is dealt with separately, see p. 416). Most of the causes of polyuria listed here are also, by implication, causes of polydipsia – the only causes of true polydipsia not included are those due to dehydration.
![]()
COMMON
diabetes mellitus (DM)
diuretic therapy
chronic renal failure (CRF)
hypercalcaemia (e.g. osteoporosis treatment, multiple bony metastases, hyperparathyroidism)
alcohol
OCCASIONAL
potassium depletion: chronic diarrhoea, diuretics, primary hyperaldosteronism
relief of chronic urinary obstruction
drugs: lithium carbonate, demeclocycline, amphotericin B, glibenclamide, gentamicin
cranial diabetes insipidus (hypothalamo-pituitary tumour, skull trauma, sarcoidosis or histiocytosis X)
Cushing’s disease from excessive corticosteroid doses and ACTH-secreting bronchial carcinoma
sickle-cell anaemia
early chronic pyelonephritis
RARE
psychogenic polydipsia (compulsive water drinking)
supraventricular tachycardia
DIDMOAD syndrome (diabetes insipidus, diabetes mellitus, optic atrophy, deafness: autosomal recessive)
familial cranial diabetes insipidus (autosomal dominant inheritance)
familial nephrogenic diabetes insipidus (males only: X-linked recessive)
Fanconi syndrome
![]()
![]()
LIKELY: urinalysis, fasting glucose or HbA1c.
POSSIBLE: FBC, U&E, serum calcium.
SMALL PRINT: blood film, further specialist investigations (see below).
Urinalysis: glucose and possible ketones in diabetes; possible haematuria and proteinuria with renal problems; specific gravity very low in diabetes insipidus and psychogenic polydipsia.
Fasting glucose or HbA1c: to confirm diabetes mellitus.
FBC: normochromic anaemia in CRF; film for sickle-cell anaemia.
U&E: to detect potassium deficiency and abnormalities suggesting CRF.
Serum calcium: elevated in hypercalcaemia.
Further specialist investigations: many of the aforementioned ‘causes’ will need further investigation in secondary care to establish underlying aetiology (e.g. ultrasound and renal biopsy in CRF, water deprivation test for diabetes insipidus, CT scan if possible pituitary lesion, and so on).
Take time to clarify the symptoms. It is essential to differentiate polyuria from frequency, as the causes are very different.
Remember alcohol as a possible cause, especially in young males. Patients can be surprisingly slow to make quite obvious connections.
Refer for more detailed investigation if the symptoms are clear-cut and baseline tests draw a blank.
Diabetes mellitus is not the only cause of polyuria with thirst. If urinalysis is negative for sugar, consider diabetes insipidus or hypercalcaemia.
Weight loss and cough in a smoker with polyuria suggests a possible ACTH-secreting tumour. Arrange an urgent CXR.
If urinalysis reveals glucose and ketones in a known or new diabetic, arrange for urgent assessment with a view to admission for stabilisation.
Renal disease is likely in patients with polydipsia who have blood and protein on urinalysis.
![]()
This means an increased frequency of micturition, and is usually associated with the passage of small amounts of urine. It is not the same as increased production of urine (see Excessive urination, p. 413). It is a commonly presented problem, affecting women far more often than men: the average GP will deal with around 60 cases of cystitis (the main cause) each year. Terminology can be confusing – we now use ‘LUTS’ for what we used to describe as ‘prostatism’.
![]()
COMMON
infective cystitis
anxiety
overactive bladder syndrome
bladder calculus
lower urinary tract symptoms (LUTS) in men
OCCASIONAL
interstitial cystitis (non-infective)
prostatitis
pregnancy
ureteric calculus (in lower third of ureter precipitates reflex frequency)
urethritis, pyelonephritis
iatrogenic (e.g. diuretics)
bladder neck hypertrophy
‘habit frequency’
RARE
pelvic space-occupying lesion, e.g. fibroid, ovarian cyst, carcinoma
secondary to pelvic inflammation: PID, appendicitis, diverticulitis, adjacent tumour
bladder tumour (benign or malignant)
post-radiotherapy fibrosis (testicular, ovarian and prostatic cancer)
tuberculous cystitis/renal TB
fibrosis secondary to chronic sepsis from long-term catheter drainage
![]()

![]()
LIKELY: urinalysis, MSU, urinary frequency volume chart.
POSSIBLE: urethral swab, PSA, uroflowmetry, urodynamic studies, plain abdominal X-ray, IVU, cystoscopy, CA-125.
SMALL PRINT: pelvic ultrasound, U&E, pregnancy test and three EMUs for TB.
Urinalysis: protein, nitrites, leucocytes and possible haematuria in infection; possible stone or tumour if blood alone.
MSU: microscopy may show abnormal epithelial cells, blood, pus and help identify pathogen in infection.
Urinary frequency volume chart – may be useful in men with LUTS.
Swab any urethral discharge present for Chlamydia and gonorrhoea.
CA-125 – may be useful if ovarian cancer suspected.
EMU: for pregnancy test; also three EMUs to check for TB if suspected (e.g. sterile pyuria).
U&E: check if assessment suggests chronic sepsis or outflow obstruction.
PSA: consider this if LUTS in male.
Specialist tests include: uroflowmetry (for LUTS, urodynamic studies (for unstable bladder), IVU and cystoscopy (for stones and tumours) and ultrasound (for pelvic masses or if CA-125 elevated).
Frequency due to anxiety is typically long term, worse with stress and cold weather, and is associated with a normal urinalysis.
It is reasonable to make an empirical diagnosis of overactive bladder syndrome in a non-pregnant female with frequency in whom CA-125, pelvic examination and urinalysis are entirely normal.
An unrecognised pregnancy may present with frequency: ask about periods, and do a pregnancy test if a period has been missed.
In the elderly, a bladder tumour may present as cystitis. If a new, recurring problem, or haematuria attributed to the cystitis does not settle with antibiotics, consider referral.
Do not ignore sterile pyuria on the MSU: possible causes include urethritis and TB.
The adult patient with frequency who has persistent microscopic haematuria but no other abnormalities on urinalysis may have a stone or tumour. Refer.
Appendicitis can cause mild frequency and pyuria. Do not be misled by the urinalysis into an inappropriate diagnosis of UTI: act according to the clinical findings.
UTI in infancy is a major cause of renal failure. Manage according to NICE guidance.
![]()
Incontinence is involuntary micturition. It is not a common presenting symptom, embarrassment tending to inhibit patients, but it is often mentioned as a ‘while I’m here’ or noted by the doctor, typically because of the characteristic odour when visiting an elderly patient. It may present more frequently in the future as the problem receives more publicity and patients realise that help is available. The population prevalence in women is around 10%, but is probably much higher in older age groups.
![]()
COMMON
stress incontinence (with or without prolapse)
infective cystitis
overactive bladder syndrome: idiopathic or secondary to other problems, e.g. CVA, dementia, Parkinson’s disease
chronic outflow obstruction, e.g. prostatic enlargement, bladder neck stenosis, urethral stenosis
after prostatectomy (usually temporary)
OCCASIONAL
chronic UTI
interstitial cystitis
bladder stone or tumour
after abdomino-pelvic surgery and radiotherapy
fistula: vesicovaginal/uterine, ureterovaginal (surgery and malignancy)
polyuria (any cause, e.g. diabetes, diuretics – particularly if compounded by immobility in the elderly)
RARE
after pelvic fracture (direct sphincter damage with or without neurological damage)
congenital abnormalities: short urethra, wide urethra, epispadias, ectopic ureter
sensory neuropathy, e.g. diabetes and syphilis
multiple sclerosis, syringomyelia
paraplegia, cauda equina lesion
psychogenic
![]()

![]()
LIKELY: urinalysis, MSU.
POSSIBLE: PSA, U&E, ultrasound, IVU, urodynamic studies, uroflowmetry.
SMALL PRINT: fasting sugar or HbA1c blood sugar, syphilis serology, cystoscopy, neurological investigations.
Urinalysis: to test for infection and diabetes.
MSU: to confirm infection and guide antibiotic treatment.
Fasting sugar or HbA1c and syphilis serology: if diabetes or syphilis a possible cause of neuropathy.
PSA: consider this if LUTS or prostatic enlargement on examination.
U&E: to assess renal function in chronic outflow obstruction.
Ultrasound good for assessing renal size non-invasively: may suggest outflow obstruction or chronic infection.
IVU best for looking for renal scarring of chronic UTI, structural anomalies and demonstrating residual urine; may also reveal site of outflow obstruction and fistulae.
Specialist investigations may include: urodynamic studies (helpful to distinguish between urge and stress incontinence), uroflowmetry (prostatism), cystoscopy (may reveal cause of outflow obstruction, stone or tumour) and neurological investigations (e.g. imaging of spinal cord).
Incontinence has many causes, but can often be broadly categorised into one of three groups: stress incontinence (e.g. with coughing), urge incontinence (‘when I’ve got to go, I’ve got to go’) and continuous, like water over the edge of a dam (e.g. through a vesicovaginal fistula, or in overflow from a chronically distended bladder).
The aetiology may be multifactorial, particularly in the elderly. Mobility, vision, distance to the toilet and ongoing medication may all be relevant.
Overactive bladder syndrome and stress incontinence can be difficult to distinguish. The latter rarely causes nocturnal incontinence, while it may be a feature of overactive bladder syndrome. If in doubt, refer for urodynamic studies.
Adopt a sympathetic approach. Incontinence can have a devastating impact on self-esteem and seriously affect a patient’s social and sexual functioning.

Incontinence with saddle anaesthesia and leg weakness suggests a cauda equina lesion. This is a neurological emergency: refer urgently.
Continuous incontinence suggests significant pathology, such as a fistula, chronic outflow obstruction or a neurological problem.
Never empty the huge bladder of chronic retention in one go. This can cause bleeding and renal complications. Admit for catheterisation and controlled release.
Adult-onset nocturnal enuresis suggests chronic retention.
![]()
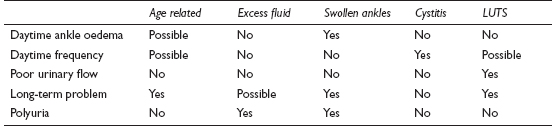
Nocturia may present in isolation or it may be a manifestation of other urinary disturbances such as polyuria or frequency. Surprisingly, in older age groups, it is as common in women as men. Occasional nocturia is, of course, quite normal – the symptom should only be viewed as pathological when it causes disruption or distress.
![]()
COMMON
age related (in part caused by a reduction in bladder capacity)
excess fluid at bed time (especially alcohol)
any cause of swollen ankles (the recumbent posture redistributes the fluid load at night) – see Swollen ankles, p. 312
cystitis
LUTS
OCCASIONAL
overactive bladder syndrome
lower urinary tract obstruction (other than prostate problems)
any other cause of urinary frequency (see Frequency, p. 416)
diabetes mellitus
any other cause of polyuria (see Excessive urination, p. 413)
sleep apnoea (causes overproduction of urine)
RARE
anxiety
drug side effect (rare because drugs likely to cause a diuresis are usually taken in the morning)
diabetes insipidus
![]()
![]()
NOTE: urinary frequency, polyuria, or swollen ankles as ‘causes’ of nocturia will need investigating in their own right – see the relevant sections for more details on each of these topics.
LIKELY: urinalysis, MSU, urinary frequency volume chart.
POSSIBLE: blood sugar, PSA.
SMALL PRINT: cystoscopy, urodynamic studies, IVP/ultrasound, water deprivation test.
Urinalysis: protein, nitrites, leucocytes and possible haematuria in infection; glucose in diabetes; specific gravity very low in diabetes insipidus.
MSU: to confirm infection and identify pathogen.
Urinary frequency volume chart – to help distinguish nocturnal polyuria (increased urine production at night) from reduced bladder storage capacity.
Blood sugar: to confirm diabetes mellitus.
PSA: pros and cons of this test may be discussed if assessment raises the possibility of prostate cancer.
Specialist tests include: cystoscopy and IVU/ultrasound (for lower urinary tract obstruction), urodynamic studies (for unstable bladder) and water deprivation test (for diabetes insipidus).
In the elderly, the cause is often multifactorial.
The effects – such as disturbed sleep, a disrupted household, exhaustion and occasional incontinence – may be more important to the patient than the specific diagnosis.
Swollen ankles – of any aetiology – are frequently overlooked as an underlying cause.
Nocturia may just be a manifestation (albeit the most distressing) of polyuria or urinary frequency. Focus your approach on the underlying problem.
Exclude diabetes – but remember that it is not the only cause of polyuria, nocturia and thirst.
A habitual ‘nightcap’ may be the cause of nocturia – and may be a pointer to an underlying alcohol problem, especially in solitary elderly males.
![]()
Retention is failure to empty the bladder completely. The acute form characteristically affects men, presents urgently and requires immediate catheterisation or hospitalisation. Chronic retention may produce few symptoms and may only be discovered during palpation of the abdomen.
![]()
COMMON
prostatic hypertrophy: benign, rarely carcinoma
anticholinergic drugs: bladder stabilisers and tricyclic antidepressants
constipation
bladder neck obstruction/urethral stricture
UTI (including prostatitis and prostatic abscess)
OCCASIONAL
urethral calculus
‘holding on’ (leads to prostatic congestion)
pelvic mass: retroverted, gravid uterus or fibroid uterus
acute genital herpes (via local inflammation and interference with neurological control of detrusor reflex arc)
clot retention (e.g. after bleed from tumour or post-TURP bleed)
balanoposthitis in children (if very painful)
RARE
neurological: MS, syphilis, spinal cord compression
pedunculated bladder tumour
traumatic rupture of urethra
foreign body inserted into anterior urethra
phimosis
psychological
![]()

![]()
LIKELY: urinalysis, MSU.
POSSIBLE: U&E, PSA, ultrasound, IVU, cystoscopy.
SMALL PRINT: neurological investigations, prostatic biopsy, urethrography (all hospital-based investigations).
Urinalysis of any urine available may confirm a UTI as the cause; may also reveal microscopic haematuria if a stone or bladder tumour.
MSU: will confirm infective agent in UTI.
U&E: renal failure may follow chronic retention.
PSA may be worth considering if preceding symptoms of prostatism or abnormal prostate on examination.
Specialist tests may include: renal ultrasound (reveals obstruction and pelvic masses), IVU (may reveal site of obstruction and will provide information about renal function), cystoscopy (may be diagnostic and therapeutic for stones, stricture, bladder outflow obstruction and bladder tumour), neurological investigations (e.g. spinal cord imaging if cord lesion suspected), prostatic biopsy (if suspicious area of prostate palpable) and urethrography (for stricture).
Do not overlook faecal impaction in the elderly patient as a cause of urinary retention.
‘First-aid’ relief of retention when the cause is a painful perineal condition (e.g. balanoposthitis, herpes simplex or UTI) may be achieved by encouraging the patient to urinate while immersed in a warm bath.
Anuria can be mistaken for retention. A straightforward clinical assessment should differentiate the two conditions.
A history suggesting a disc prolapse with urinary retention indicates possible cord compression – admit immediately.
Sudden stoppage of urine with a pain like a blow to the bladder and passage of a few drops of blood is pathognomic of urethral calculus.
Beware of any drugs with anticholinergic side effects in patients with a history of outflow obstruction – they may precipitate acute retention.
Avoid catheterisation when sepsis is likely (e.g. possible UTI) – instrumentation may result in septicaemia. Instead, admit to hospital for catheterisation under appropriate antibiotic cover.
Do not catheterise the patient with chronic retention; admit for controlled drainage. Sudden decompression can result in haematuria and renal complications.