
• Progressive visual loss due to degeneration of the macula
• Eye exam may reveal spots of pigment near the macula and blurring of the macular borders
The macula is the area of the retina where images are focused. It is the portion of the eye responsible for fine vision. Degeneration of the macula is the leading cause of severe visual loss in the United States and Europe in people 55 or older, and is second to cataracts as the leading cause of decreased vision in people over 65. It is estimated that more than 150,000 Americans are legally blind from age-related macular degeneration, with 20,000 new cases occurring each year.1,2
The major risk factors for macular degeneration are smoking, aging, atherosclerosis (hardening of the arteries), and high blood pressure.1–4 The degeneration appears to be a result of free radical damage, similar to the type of damage that induces cataracts (see the chapter “Cataracts”). However, decreased blood and oxygen supply to the retina is the key factor leading to macular degeneration.
Types of Macular Degeneration
The two most common types of age-related macular degeneration (ARMD) are the atrophic (“dry”) form, by far the more frequent, and the neovascular (“wet”) form.2,3 In either form, patients may experience blurred vision. The patient may note that straight objects appear distorted or bent, that there is a dark spot near or around the center of the visual field, and that, while he or she is reading, parts of words are missing.
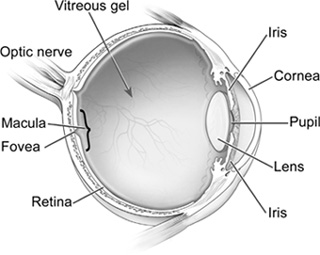
Anatomy of the Eye
Between 80 and 85% of people with ARMD have the dry form of the disease. The primary lesions are atrophic changes in the retinal pigmented epithelium (RPE), which composes the innermost layer of the retina. Beginning in early life and continuing throughout life, cells of the RPE gradually accumulate sacs of cellular debris known as lipofuscin. The lipofuscin sacs are either remnants of incompletely degraded abnormal molecules from damaged RPE cells or derivatives of damaged membranes of nearby cells. Progressive engorgement of the RPE cells with lipofuscin is associated with the leakage (extrusion) of other cell components.1–3 The hallmark feature of macular degeneration is the appearance of this extrusion beneath the RPE. This extrusion, which can be seen with the aid of an ophthalmoscope, is referred to as drusen.
The disease progresses slowly, and only central vision is lost; peripheral vision remains intact. It is rare for anyone to become totally blind from dry ARMD. Currently there is no standard medical treatment for this common form of ARMD, though the use of nutritional supplements designed to address the underlying oxidative damage is becoming the “unofficial” standard of care.
Wet ARMD is also known as the neovascular form or advanced ARMD. It affects 5% to 20% of people with ARMD. Wet ARMD is characterized by the growth of abnormal blood vessels. Because the disease can rapidly progress to a point at which laser surgery cannot be used, treatment should be performed as soon as possible. A common early symptom of wet ARMD is that straight lines appear wavy.
Wet ARMD can be treated quite effectively in the early stages with laser surgery and other medical treatments such as lower-powered laser or low-dose radiation therapy. Drugs known as antiangiogenics or anti-VEGF (anti–vascular endothelial growth factor) agents are also used. These drugs can shrink the abnormal blood vessels and improve vision when injected directly into the vitreous humor of the eye. The injections have to be repeated on a monthly or bimonthly basis. Examples of these agents include ranibizumab (Lucentis), bevacizumab (Avastin), and pegaptanib (Macugen).1,2
Therapeutic Considerations
Treatment of the dry form and prevention of the wet form of ARMD involve the use of antioxidants and natural substances that correct the underlying free radical damage to the macula. Reduce the risk of ARMD by focusing on preventive factors against atherosclerosis, increasing dietary intake of fresh fruits and vegetables, supplementing with nutritional and botanical antioxidants, and not smoking.
In particular, smoking tobacco greatly increases the risk of ARMD.3 Someone who smokes a pack of cigarettes a day for any significant length of time increases the risk of ARMD by two to three times that of someone who has never smoked.3 The risk does not return to the normal level until after someone has stopped smoking for 15 years.
There is also a strong genetic component to consider. While a number of genetic markers have been identified, a family history may be the easiest screening method. The lifetime risk of developing late-stage macular degeneration is 50% for people who have a relative with macular degeneration, vs. 12% for people who do not.5
Interestingly, higher birth weight and a lower ratio of head circumference to birth weight are associated with significantly higher risk for ARMD.6
Not surprisingly, the dietary factors important in the prevention and treatment of ARMD are the same as those that prevent other chronic degenerative diseases including atherosclerosis. A diet rich in fruits and vegetables is associated with a lower risk for ARMD. Presumably this protection is the result of greater intake of antioxidant vitamins and minerals.7–10 However, various nonessential food components such as flavonoids and the carotenes lutein, zeaxanthin, and lycopene are proving to be even more significant in protecting against ARMD than traditional nutritional antioxidants such as vitamin C and E, zinc, and selenium. The macula, especially its central portion, the fovea, owes its yellow color to its high concentration of lutein and zeaxanthin. These yellow carotenoids function in preventing oxidative damage to the area of the retina responsible for fine vision and have a central role in protecting against the development of macular degeneration.9,10
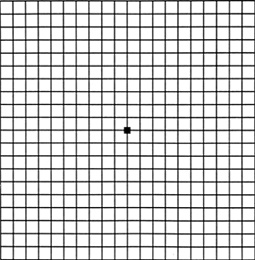
Normal Appearance of Amsler Grid
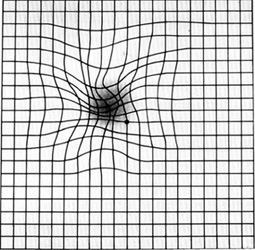
Appearance of Amsler Grid in Macular Degeneration
The carotene lycopene, a component of tomatoes and other red fruit and vegetables, is also protective. In one study, individuals with the lowest levels of lycopene content were twice as likely to have ARMD.11
Moderate wine consumption is also associated with decreased risk of ARMD.12 Red wine contains anthocyanins, powerful antioxidants that are probably responsible for its protective effect. It is important to note that beer consumption increases drusen accumulation and the risk of exudative macular disease and therefore should be avoided.13
Just as in atherosclerosis, types of dietary fat appear to play a role in ARMD. A cohort study of 261 individuals with early or intermediate stages of ARMD revealed a twofold increased risk of progression with a diet high in animal fat and commercial baked goods (sources of sugar and trans-fatty acids). In contrast, higher intakes of fish and nuts are associated with a lower risk of ARMD progression.14 A higher intake of long-chain omega-3 fatty acids was shown to be inversely associated with progression to ARMD over a period of 12 years.15–17
In addition to a diet high in antioxidants, supplementation with nutritional antioxidants such as vitamin C, selenium, beta-carotene, and vitamin E is certainly important in the treatment and prevention of macular degeneration. Studies conducted by the Age-Related Eye Disease Study Research Group (AREDS) confirm that a combination of these nutrients will be likely to produce better results than any single nutrient alone, because other studies have demonstrated that none of these antioxidants alone accounts for the impaired antioxidant status in ARMD.18 Instead, the lower antioxidant status reflects decreases in a combination of nutrients. The specific amounts of antioxidants and zinc used in the study were 500 mg vitamin C, 400 IU vitamin E, 15 mg beta-carotene (often labeled as equivalent to 25,000 IU vitamin A), 80 mg zinc (as zinc oxide), and 2 mg copper (as cupric oxide).
Food Sources of Carotenes Important for the Eyes |
|
CAROTENOID |
FOOD SOURCE |
Lycopene |
Tomatoes, carrots, green peppers, apricots, pink grapefruit |
Zeaxanthin |
Spinach; paprika; corn; richly colored fruit, especially kiwi fruit and grapes |
Lutein |
Corn, potatoes, spinach and other greens, carrots, tomatoes, mangoes |
Several other studies utilizing various commercially available broad-based antioxidant formulas have shown promising results. For example, a 11/2-year study demonstrated that the progression of dry ARMD could be halted (but not reversed) with a broad-spectrum, 14-component antioxidant capsule (Ocuguard).19,20 A retrospective study of a nutritional supplement called ICAPS Plus (which contains beta-carotene, vitamins C and E, zinc, copper, manganese, selenium, and riboflavin) compared 38 patients who used the preparation regularly with 37 patients who used only one bottle and who served as controls. Fifteen of the treated patients showed improvement in their vision by one line or more on a vision acuity chart, compared with only 6 of the control group. In addition, only 3 of the 38 in the treatment group lost one line or more of vision, compared with 13 in the control group.21 In a second blinded clinical trial reported in the same review, after six months, visual acuity was the same or better in 36 of 61 controls compared with 168 of 192 treated patients.
B vitamins are also important. In a randomized, double-blind, placebo-controlled trial, 5,442 female health care professionals 40 years or older with preexisting cardiovascular disease or three or more cardiovascular disease risk factors randomly received a combination of folic acid (2.5 mg per day), vitamin B6 (50 mg per day), and vitamin B12 (1 mg per day) or a placebo. After an average of 7.3 years of treatment and follow-up, there were 55 cases of ARMD in the combination treatment group and 82 in the placebo group. There were 26 cases of more severe ARMD in the combination treatment group and 44 in the placebo group. These results indicate a 34% and 41% reduced relative risk, respectively.22
Lutein
In addition to a high-lutein diet, supplementation with additional lutein is of benefit. One 12-month double-blind study, the Lutein Antioxidant Supplementation Trial (LAST),23 sought to determine whether nutritional supplementation with lutein or lutein together with antioxidants, vitamins, and minerals improves visual function and symptoms in ARMD. Patients receiving lutein (10 mg) alone or in combination with other vitamins and minerals in a broad-spectrum supplementation formula showed improvements in visual function.
In another study, 27 patients with ARMD were randomly divided into two groups: 15 patients took vitamin C (180 mg), vitamin E (30 mg), zinc (22.5 mg), copper (1 mg), lutein (10 mg), zeaxanthin (1 mg), and astaxanthin (4 mg) every day for 12 months, while 12 patients served as controls. Visual acuity assessments indicated quite clearly that early-stage ARMD can respond positively to supplementation with carotenoids and antioxidants.24
Zinc
Zinc plays an essential role in the metabolism of the retina, and the elderly are at high risk for zinc deficiency. In addition to the studies with a combination of nutrients, a two-year, prospective, randomized, double-blind, placebo-controlled trial involving 151 subjects with dry ARMD demonstrated that the group taking 200 mg per day of zinc sulfate (approximately 80 mg elemental zinc) had significantly less visual loss than the placebo group.25
In another study, using a zinc-monocysteine (ZMC) supplement, 40 subjects with ARMD were randomly assigned to either ZMC 25 mg or a placebo twice per day for six months. The ZMC group showed improved visual acuity, contrast sensitivity, and macular light flash recovery time. No improvement occurred in the placebo group. ZMC was well tolerated, with a gastrointestinal irritation rate of under 2%.26
![]()
QUICK REVIEW
• Degeneration of the macula is the leading cause of severe visual loss in the United States.
• The major risk factors for macular degeneration are smoking, aging, atherosclerosis (hardening of the arteries), and high blood pressure.
• The treatment goals in the dry form and prevention of the wet form involve the use of antioxidants and natural substances that protect against free radical damage and improve blood and oxygen supply to the macula.
• A diet rich in fruits and vegetables is associated with a greatly lowered risk for macular degeneration.
• In addition to a high-lutein diet, supplementation with additional lutein is of benefit.
• Antioxidant formulas have been shown to halt and even reverse macular degeneration.
Flavonoid-Rich Extracts
Flavonoid-rich extracts of bilberry (Vaccinium myrtillus), ginkgo biloba, grape seed, or pine bark (e.g., Pycnogenol) offer significant benefits in the prevention and treatment of ARMD. In addition to exerting excellent antioxidant activity, all of these extracts have been shown to have positive effects on retinal blood flow and function. Clinical studies of humans have demonstrated that all three are also capable of halting the progressive visual loss of dry ARMD and possibly even improving visual function.27–30 Of the three, bilberry extracts standardized to contain 25% anthocyanidins appear to be the most useful. The anthocyanosides of bilberry have a very strong affinity for the retinal pigmented epithelium, reinforcing the collagen structures of the retina and preventing free radical damage. Because the RPE is the portion of the eye affected in ARMD, bilberry anthocyanosides appear to be ideal therapeutic agents for the disorder. However, ginkgo biloba extract (24% ginkgo flavonglycoside content) is perhaps a better choice if a person is also showing signs of decreased blood flow to the brain.
![]()
TREATMENT SUMMARY
As with most diseases, prevention or treatment of ARMD at an early stage is most effective. The treatment of the wet form is clearly laser therapy, used as soon as possible. Because free radical damage and lack of blood and oxygen supply to the macula appear to be the primary causes of macular degeneration, consumption of antioxidant supplements and promotion of retinal blood flow are the keys to effective treatment.
The use of nutritional supplementation in ARMD has undergone extensive cost-benefit analysis. Compared with no therapy, antioxidant therapy yielded a cost-effective improvement in quality of life and lowered the percentage of patients with ARMD who ever developed visual impairment in the better-seeing eye from 7.0 to 5.6%.31
Follow the guidelines given in the chapter “A Health-Promoting Diet.” Foods to avoid in cases of ARMD are:
• Fried and grilled foods, and other sources of free radicals
• Animal fat
• Processed baked goods
• Beer
Important foods to emphasize are:
• Yellow vegetables, green vegetables, tomato products
• Flavonoid-rich berries (blueberries, blackberries, cherries, etc.)
• Other fresh fruits and vegetables, nuts, and fish
• Moderate amounts of red wine
• A high-potency multiple vitamin and mineral formula as described in the chapter “Supplementary Measures”
• Key individual nutrients:
![]() Vitamin B6: 25 to 50 mg per day
Vitamin B6: 25 to 50 mg per day
![]() Folic acid: 800 to 2,000 mg per day
Folic acid: 800 to 2,000 mg per day
![]() Vitamin B12: 800 mcg per day
Vitamin B12: 800 mcg per day
![]() Vitamin C: 500 to 1,000 mg per day
Vitamin C: 500 to 1,000 mg per day
![]() Vitamin E (mixed tocopherols): 100 to 200 IU per day
Vitamin E (mixed tocopherols): 100 to 200 IU per day
![]() Magnesium (bound to aspartate, citrate, fumarate, malate, glycinate, or succinate): 200 to 300 mg three times per day
Magnesium (bound to aspartate, citrate, fumarate, malate, glycinate, or succinate): 200 to 300 mg three times per day
![]() Selenium: 100 to 200 mcg per day
Selenium: 100 to 200 mcg per day
![]() Zinc: 30 to 45 mg per day
Zinc: 30 to 45 mg per day
![]() Vitamin D3: 2,000 to 4,000 IU per day (ideally, measure blood levels and adjust dosage accordingly)
Vitamin D3: 2,000 to 4,000 IU per day (ideally, measure blood levels and adjust dosage accordingly)
• Fish oils: 1,000 mg EPA + DHA per day
• Zeaxanthin: 1 to 2 mg per day
• Astaxanthin: 4 to 6 mg per day
One of the following:
• Ginkgo biloba extract (24% ginkgo flavonglycosides): 120 to 240 mg per day
• Bilberry extract (25% anthocyanidin content): 120 to 240 mg per day
• Grape seed or pine bark extract (95% procyanidolic content): 150 to 300 mg per day