One of the most important goals for parents starting the ketogenic diet is to reduce their child’s medications. Parents are surprised when they start the diet that we write more prescriptions than when they came in! Nevertheless, most of these supplements are essential for maintaining the diet and are vitamins and minerals to keep their child safe.
A child on a regular diet should be able to meet all of their vitamin and mineral needs just from eating their foods. However, the ketogenic diet is very high in fat and very low in carbohydrates, essentially eliminating a huge component of a regular diet. Vitamins and minerals are found naturally in fruits, vegetables, and animal proteins. However, in the United States all grains are enriched with vitamins and minerals. Through eliminating pastas, cereals, and bread and limiting fruits and vegetables, you are eliminating essential vitamins and minerals. The Dietary Reference Intakes (DRIs) have been established and provide recommendations for both macro nutrients (carbohydrate, protein, and fat) and micro nutrients (vitamins and minerals). It is provided free of charge for pdf download at this Web site: http://iom.edu/Reports/2006/Dietary-Reference-Intakes-Essential-Guide-Nutrient-Requirements.aspx
It is essential for all children on the ketogenic diet to be supplemented with a complete pediatric multivitamin meeting all of the DRIs for their age. There are a couple of vitamins that are low in carbohydrates that can either be purchased over the counter at a local pharmacy or via the Internet.
Some of the common vitamins that we use are Sugar-free Scooby Doo vitamins® (Bayer), Kirkman’s Children Hypoallergenic Multi Vitamin® (Kirkman), Nano VM® (Solace Nutrition) and Phlexy Vits® (Nutricia). In the United States, other commonly used preparations include Unicap M® (McNeil), Centrum® (Wyeth), and Bugs Bunny Sugar-free® (Bayer). In Europe, Multibionta® (Seven Seas) is also available as a liquid formulation. Most general complete multivitamins are still low in calcium, requiring additional calcium supplementation. Nano VM® and Phlexy Vits® are the only vitamins that usually do not need additional calcium. Nano VM® is typically ordered over the Internet (http://www.solacenutrition.com/products/nanovm/nanovm.html) and is available for ages 1–3 years and 4–6 years. Nano VM® and Phlexy Vits® are powdered supplements that can be mixed in with fluids or small amounts of calculated applesauce or keto yogurt. The other vitamins can be chewed, swallowed, or crushed with water to provide via gastrostomy tube.
Formula-fed babies and older kids getting formula through a gastrostomy tube might not need additional supplementation. Compare the vitamins and minerals in the formula for the amount being provided to the DRIs, and supplement only those vitamins that do not meet 100% of the child’s daily needs.
A lot of epilepsy medications are associated with bone loss and calcium metabolism. Many studies have shown that common medications for epilepsy lead to significant reduction in bone mineral density. However, it is unclear if supplementing more calcium and vitamin D than is required will help with calcium absorption. On the ketogenic diet there are very few calcium sources through foods. The only dairy that is eaten is cheese, and it’s limited. Therefore, adding a calcium and vitamin D supplement will ensure that your child is getting at least the DRIs for their age.
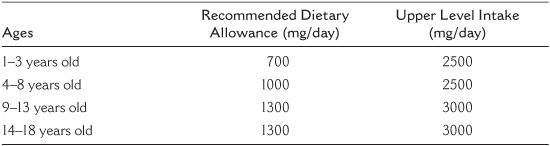
Calcium is essential for the structures of bone and teeth and is also involved in vascular and neuromuscular functions. It is the most abundant mineral found in the body. Calcium is found in dairy products, such as milk, yogurts, cheeses, and ice cream; green leafy vegetables, such as broccoli and kale; and calcium-enriched foods, such as orange juice. Despite dairy products being high in fat they still have protein and some carbohydrates in them, making them difficult to use for the ketogenic diet. Heavy cream, the fat skimmed off of milk, contains minimal calcium. Therefore, calcium supplementation is essential on the ketogenic diet. Recently, the Institute of Medicine came out with new calcium guidelines (see Table 10.1).
Some common calcium supplements that we use are found in most pharmacies or available for purchase on the Internet. For tablets that can be crushed or swallowed, we use Nature Made brand of either 500 or 600 mg calcium plus vitamin D or Caltrate® from Wyeth. There is an oral suspension from Roxanne called Calcium Carbonate 1250 mg for 5 ml oral suspension, and there is a powdered supplement from Now Foods called Calcium Citrate powder that can be mixed into liquids.
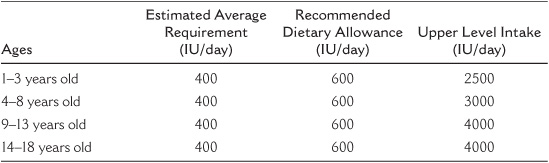
Vitamin D (calciferol) is also involved in bone health and is not found naturally in many foods products. It is synthesized in the skin through sun exposure, and it aids in calcium and phosphorus absorption. Vitamin D can be found in fatty fish, fortified milk, and other fortified foods like breakfast cereals. The Institute of Medicine also came out with new guidelines for vitamin D intake. The range is 400–600 International Units (IU) per day, but a child should not exceed 2500–4000 IU per day (see Table 10.2).
You can purchase vitamin D from Now Foods or Carlson, in doses ranging from 100 IU to 1000–2000 IU per day.
TABLE 10.1
Calcium Guidelines from the Institute of Medicine
Table 10.2
Vitamin D Guidelines from the Institute of Medicine
Due to recent studies based on known side effects on the diet, many centers are providing oral citrate supplements. At Johns Hopkins we prescribe a potassium citrate (Polycitra K®) to all of our patients starting the diet. Since supplementing each patient we have seen a significant reduction in the amount of kidney stones by nearly 7 times, as shown in a study by a Hopkins medical student, Ms. Melanie McNally, in 2009. Oral citrates work to alkalinize the urine and solubilize urine calcium. They increase the pH in the urine, which increases urinary citrate and essentially decreases the amount of kidney stones. Polycitra K® is a powder supplement that can be added to water, and it is recommended to drink a lot of fluid as well to prevent kidney stones. For most children we dose it 2 mEq/kg/day, for a young child we may give 15 mEq twice daily (half of a 30 mEq packet), and for an older child 30 mEq twice daily (a full packet twice daily). Other supplements, like Citra K® and sodium bicitrate are fine and can be substituted if the pharmacy doesn’t have Polycitra K®.
Constipation and gastrointestinal intolerances to the ketogenic diet are both common side effects while on the diet. There have not been any studies looking at beginning antireflux medications when starting the diet, however, a high fat diet can cause gastroesophageal reflux and may be helped by starting an antireflux medication.
Constipation is one of the common side effects of the ketogenic diet. It is a diet very low in fiber, fresh fruits, and vegetables, and sometimes fluids. There are ways to help with constipation through foods using oils, MCT oil, and avocados, adding some prunes to the meals, exercising, and drinking enough fluid. But when that doesn’t work, Miralax® is usually the safest and most effective way to treat constipation. It is another powder that gets added to water, but this one has no flavor! Some families report benefits with using Georges Aloe Vera®, but there are no studies regarding its efficacy, and there it is not approved by the FDA.
Carnitine is a compound synthesized by the amino acids lysine and methionine and required for fatty acid to be transported into the mitochondria during the breakdown of fats for the making of metabolic energy. The active form of carnitine that is needed is called L-carnitine. The body makes enough carnitine on its own to help turn fat into energy; however, some children on a high fat diet can either not make enough carnitine on their own or have issues transporting it across the cell.
There are some clinicians that start all children beginning the ketogenic diet with carnitine and some that test levels and only give carnitine if the levels are low. Symptoms of carnitine deficiency can be fatigue and lethargy. The consensus of multiple centers is to test the carnitine level before the diet is started and then check every 3–6 months while on the diet and only supplement if there is a deficiency. Carnitine is another pill or liquid to take on top of everything else and can be expensive, so we use it at Johns Hopkins only when necessary. Carnitor® is the brand name product, but generic works fine. It comes in 330 mg capsules or 1000 mg/10 ml liquid.
MCT oil is a medium chain triglyceride oil compared to the regular household oils that are long chain triglycerides. In the 1970s MCT oil was introduced as a modification to the classical ketogenic diet. MCT oil was thought to produce higher ketosis; it is absorbed better than long chain fats and is carried directly to the liver. Because MCT oil was thought to be more ketogenic, less fat is used compared to the classical ketogenic diet, allowing for more protein and carbohydrates on the diet. Originally MCT oil would provide 60% of total prescribed calories, but this caused gastrointestinal distress and was reduced to 30% of total energy with long chain fats providing the other 30% of energy. The first double blind study was conducted comparing classical ketogenic diet to the MCT oil diet, and it showed no difference in the two groups attaining 50–90% seizure reduction. There is more information about MCT oil in the MCT diet in Chapter 20.
Because MCT oil is not sold in the supermarket and needs to be obtained from the Internet or specialty health food stores, it is not a supplement that is usually started at the initiation of the diet. It may be started for a variety of reasons such as high cholesterol and triglycerides or to increase ketosis, and it can be started in various doses of 5 gram to 25 gram at each meal or per day.
Coconut oil is one of the only oils available in most supermarkets in the health food section that contains MCT oil; depending on how the oil is extracted it can be 80–100% MCT oil. Many families are choosing to use coconut oil instead of other oils due to the higher MCT content. It still contains saturated fats. Coconut oil can be used in replace of all oils and is very heat stable and good for cooking and frying.
Omega 3 fatty acid (alpha linolenic acid) is an essential fatty acid; the body does not make it by itself, and it has to be consumed through food, but it is still necessary for human health. You can find omega 3 in fish, such as sardines, tuna, and salmon; some plants; and nut oils. Omega 3 is a poly unsaturated fatty acid, and plays a vital role in brain function and normal growth and development, may reduce the risk of cardiac diseases, and is anti-inflammatory. The highest concentration of Omega 3 is found in the brain and is important for cognition, behavioral functions, and performance.
For children, the recommended range of Omega 3 is to have 0.6–1.2% of total fat intake be from polyunsaturated sources. Due to the fact that the ketogenic diet is very high in fats, making the right choices for foods and fat sources should provide more than adequate amount of Omega 3. There is no established amount of Omega 3 that is too much to consume in one day, but the FDA recommends that total dietary intake of Omega 3 fatty acids from fish not exceed 3 grams per day for adults. Therefore, there is no reason to supplement with Omega 3 or assume that your child is deficient in Omega 3 fatty acid. However, one of the forms of Omega 3 is an oil and can easily be added into the diet.
Selenium is an antioxidant nutrient that is involved in the body’s defense against oxidative stress. One of the side effects of not eating enough selenium is cardiomyopathy, which is a weakening of the heart muscle or a change in the structure of the heart muscle. Regular diets provide adequate selenium through foods; however, because the ketogenic diet is restrictive it might not provide enough. Foods that contain selenium are Brazil nuts, tuna, beef, chicken, turkey, and enriched grains. Because we supplement every child with a multivitamin on the ketogenic diet we rarely see a selenium deficiency; however, the clinician must look at the vitamin that is chosen to determine if there is enough selenium for that child, and if not, then an additional selenium supplement is added.
To make the ketogenic diet work for your child it is imperative that you provide your child with all of the prescribed supplements. Sometimes it’s very difficult to force your child to take another pill or drink the flavored water, or even use a syringe to get in all of these supplements. Your keto team will work with you to find a supplement that works best for your child, such as a crushed pill versus a powder, but sometimes there are no other forms and that extra supplement is what is preventing your child from kidney stones or another side effect of the diet. There are many Web sites and chat rooms that talk about additional supplementation for children with all types of chronic illness. Do not start anything new unless you speak to your keto team and discuss the pros and cons of that supplement.