Your baby has been delivered. You have a new person in your life who needs your care and attention. But you also need care and attention as well as time to tend to your own needs. Soon after birth, you may start thinking about how to feel your best again. Keep in mind your body can’t recover overnight from 9 months of pregnancy, so don’t expect it to. Relax and take your time!
The recovery period following your baby’s birth (the first 6 weeks) is called the postpartum period. Your body rapidly downsizes as it begins to recover after pregnancy. During this time, you go through many physical and emotional adjustments.
Because older women have a higher chance of having complications during pregnancy and delivery, you may not bounce back as quickly as a younger woman. This may make postpartum recovery a slower process. But take heart—you will return to normal! But it may be a new “normal” now.
You can help yourself during the postpartum period in many ways. Eat nutritiously, allow others to help you and accept the fact that you may have to take it easy for a while. Another way you can help yourself is to learn as much as you can about what may happen after delivery.
When your baby is delivered, the healthcare provider clamps and cuts the umbilical cord, and the baby’s mouth and throat are suctioned out. Then baby is usually passed to a nurse or pediatrician for initial evaluation and attention. Apgar scores (see page 314) are recorded at 1 and 5 minutes after birth. An identification band is placed on the baby so there’s no mix-up in the nursery.
It’s important to keep the baby warm; the nurse will dry the baby and wrap him in warm blankets. This is done whether the baby is on your chest or attended by a nurse or healthcare provider.
If your labor is complicated, baby may need to be evaluated more thoroughly in the nursery. The baby’s well-being and health are of primary concern. You’ll be able to hold and to nurse him, but if your child is having trouble breathing or needs special attention, such as monitors, immediate evaluation is the most appropriate procedure at this time.
Your baby will be taken to the nursery where he is weighed, measured and footprinted (in many places). Drops to prevent infection are placed in the eyes. A vitamin-K shot is given to help with blood-clotting factors. Your baby may receive the hepatitis vaccine if you request it. Then he is put in a heated bassinet for 30 minutes to 2 hours.
Your pediatrician is notified immediately if there are problems or concerns. Otherwise, he or she will be notified soon after birth, and a physical exam will be performed within 24 hours.
After I deliver my baby, how long will I stay in the hospital?
After a vaginal delivery, you’ll spend 1 to 2 days in the hospital. After a Cesarean delivery, it’ll probably be 2 to 4 days. This varies, depending on several factors:
•your healthcare-insurance coverage
•problems during pregnancy, labor or delivery
•complications with your baby
A baby is examined and evaluated at 1 minute, 5 minutes and, sometimes, 10 minutes after birth. The system of evaluation is called the Apgar score. This scoring system is a method of evaluating the overall well-being of the newborn infant. In general, the higher the score, the better the infant’s condition. Areas scored include the baby’s heart rate, respiratory effort, muscle tone, reflex irritability and color.
A baby with a low 1-minute Apgar score may need to be resuscitated. This means a pediatrician or nurse must help stimulate the baby to breathe and to recover from the delivery. In most cases, the 5-minute Apgar score is higher than the 1-minute score, as baby becomes more active and more accustomed to being outside the uterus.
Blood is taken from baby’s heel for a blood screen. Tests are done for anemia, sickle-cell disease, hypothyroidism and blood-glucose levels. Results often indicate whether baby needs further evaluation.
The Coombs test is administered if your blood is Rh-negative, type O or if you have not been tested for antibodies. It tests blood taken from the umbilical cord. Test results indicate whether you have formed Rh-antibodies.
The reflex assessment tests for several specific reflexes in baby, including the rooting and grasp reflexes. If a particular reflex is not observed, further evaluation will be done.
In the neonatal maturity assessment, various characteristics of baby are assessed to evaluate her neuromuscular and physical maturity. Each characteristic is assigned a score; the sum indicates baby’s maturity.
The Brazelton neonatal behavioral assessment scale covers a broad range of newborn behavior. An observation test, it provides information about how a newborn responds to her environment. It is usually used when a problem is suspected, but some hospitals test all babies.
All 50 states and the District of Columbia require every newborn be screened for many life-threatening disorders. State laws and rules vary, but all states require screening for 21 or more of 29 serious genetic or functional disorders including:
•biotinidase—to determine if baby is deficient in biotinidase
•congenital adrenal hyperplasia—to learn if adrenal glands are functioning properly
•congenital hypothyroidism—to check thyroid levels
•cystic fibrosis—to determine if baby has cystic fibrosis
•hemoglobinopathies—to check for defects in the hemoglobin
•homocystinuria—to learn if baby has a B12 deficiency and will need a special diet
•galactosemia—to determine if baby can handle galactose efficiently
•maple-syrup urine disease—to determine if some amino acids must be restricted for baby
•PKU—to test for phenylketonuria
The state of New York requires hospitals to check every newborn for HIV. Results are reported to the mother or guardian.
For further information about baby after birth, read our book Your Baby’s First Year Week by Week. It contains a lot of information you may find useful.
You will probably be discharged from the hospital a day or two after your baby is born if labor and delivery were normal and baby is doing well. Some women choose to go home 24 hours after the birth of their baby or even sooner. If you have a Cesarean delivery, you will probably need to stay a few days longer.
Your blood pressure and bleeding are checked regularly in the first hours after the birth. You will be offered medication for pain relief and encouraged to nurse your baby.
Your uterus goes through great changes after baby is born and takes several weeks to return to its original size. The size of your uterus at birth is quite large. Immediately after delivery, you can feel the uterus around your navel; it should feel very hard. You are checked frequently to make sure it remains hard after delivery. If it feels soft, you or a nurse can massage it so it becomes firm.
The uterus shrinks about a finger’s width every day; this is called involution. In the hospital, someone will check you daily; this exam can be a little uncomfortable.
Afterpains are just what they sound like—pains you experience after baby’s birth. They are normal; you’ll probably feel them for several days after birth as your uterus contracts. Contractions occur to prevent heavy bleeding and enable the uterus to return to its normal size. Cramps can be eased by lying on your stomach and by taking mild pain relievers. An empty bladder enables the uterus to work more efficiently, with less pain, so drink lots of fluids and urinate often.
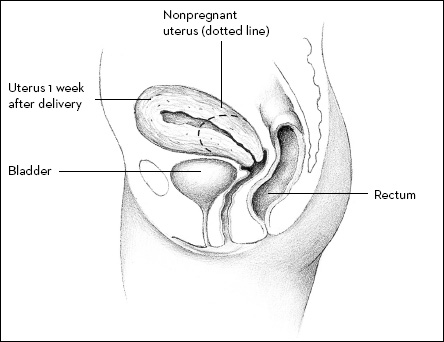
Your uterus shrinks a great deal after delivery. This illustration compares a nonpregnant uterus with a uterus 1 week after birth.
After you deliver your baby, the uterus shrinks from the size of a watermelon to the size of a volleyball. It’s not unusual to lose blood during labor and delivery; however, heavy bleeding after birth can be serious. A loss of more than 17 ounces (500ml) in the first 24 hours after delivery, called postpartum hemorrhage, is significant. Bleeding is controlled by massaging the uterus (called Credé) and with medication. Bleeding lessens gradually over time, then stops.
A number of things may cause heavy bleeding after the birth, including a uterus that won’t contract, lacerations or tearing of the vagina or cervix during birth, a large or bleeding episiotomy, a tear or rupture in the uterus, retained placental tissue, or clotting or coagulation problems. If you experience a significant change in bleeding after you go home, call your healthcare provider. Some bleeding is normal, but it’s best to talk to your healthcare provider about it. He or she may want to see you, prescribe medication or determine if the amount of bleeding is normal.
It’s not unusual to have sluggish bowels for a few days after your baby’s birth. The digestive system slows down during labor, and pregnancy and delivery stress abdominal muscles. You may have had an enema or emptied your bowel during the pushing phase of labor. Pain medication can cause constipation. These all contribute to changing bowel habits. Don’t worry about having a bowel movement for the first 4 or 5 days. Constipation at this time is acceptable.
To help your system work more efficiently, eat a diet high in fiber and drink lots of fluid. You might need a laxative. Prunes, prune juice and apple juice are natural laxatives. Over-the-counter stool softeners also help. If you don’t have a bowel movement within a week after delivery or you become uncomfortable, call your healthcare provider.
An episiotomy or hemorrhoids can make a bowel movement more difficult or make you more apprehensive about having one. If you still have hemorrhoids after delivery, be assured they usually shrink on their own. If you have problems with them, a compress of witch hazel or commercial compresses can offer relief. Ice packs may also help them shrink.
After delivery, breasts may be sore whether you breastfeed or bottlefeed. If you bottlefeed, your milk still comes in; healthcare providers don’t give medication to stop it as they did in the past. Your breasts fill with milk, called engorgement. Engorgement lasts a few days and can be very uncomfortable. You can ease discomfort by wearing a support bra or binding your breasts with a towel or an Ace bandage. Ice packs also help milk dry up.
If you feed baby formula, don’t empty your breasts unless you really have to because of pain—your body will replace the milk with more milk! Avoid nipple stimulation and running warm water over your breasts. These practices stimulate breasts to produce milk.
You may have a mild fever with engorgement. Acetaminophen can help reduce the fever and discomfort. See also the discussion of breastfeeding in Appendix B.
Headaches can be a problem for some women after delivery, and they can make you miserable. A headache can be caused or influenced by many factors, such as a long labor, having to push for a while or not sleeping in 24 to 36 hours.
If you had pre-eclampsia or pregnancy-induced hypertension, either could cause a headache after delivery. An epidural or spinal anesthetic for labor or a Cesarean delivery can result in a headache called a spinal headache. It doesn’t happen often—about once in every 100 deliveries—and is treated with bed rest and fluids.
Tell your healthcare provider if you have a headache that doesn’t go away or doesn’t get better, especially if a headache is severe or accompanied by blurred vision or nausea. He or she can recommend a course of treatment for you. Usually rest, fluids and mild pain medicine help.
It has been commonly believed symptoms associated with hyperemesis gravidarum (severe morning sickness, see Chapter 11) disappear after pregnancy. This is the case for the majority of women, but a few women continue to have problems even after baby’s birth.
Studies show some women with severe hyperemesis gravidarum can experience symptoms well beyond delivery that can take months to overcome. Symptoms include food aversions, gastroesophageal reflux (GERD), digestive problems, nausea, gallbladder issues, fatigue and muscle weakness. Women who received I.V. feedings during pregnancy because they couldn’t eat had the highest rate of symptoms.
Recovery can take a few months to as long as 2 years. Some believe it takes 1 to 2 months of recovery for every month you were ill during pregnancy. Women who have nausea and/or vomiting into late pregnancy usually find it takes several months to regain their energy and to restore nutritional reserves.
Talk to your healthcare provider if hyperemesis gravidarum persists after baby’s birth. You may need to see a nutritionist. It is especially important to seek help before you plan another pregnancy.
You may feel pain in the perineum, the area between the vagina and anus. The area may have been stretched, cut or torn during delivery. Most of the soreness should be gone in 3 to 6 weeks.
Ice packs offer some pain relief in the first 24 hours after delivery. Ice numbs the area and helps reduce swelling. After 24 hours, a warm bath or a soak in a Sitz tub can offer relief. Do this several times a day. Other remedies for perineal pain include numbing sprays, walking (to stimulate circulation), witch-hazel compresses and Kegel exercises (see Chapter 13).
Urination may be painful; acidic urine can sting the cut area. You may want to urinate standing up in the shower with running water washing over the area. The pressure exerted on your urethra during delivery may also make it a bit more difficult to urinate after baby’s birth. This will slowly clear up.
After delivering your baby, you will experience a vaginal discharge similar to a heavy menstrual flow. This discharge, called lochia, lasts from 2 to 4 weeks. The discharge is red for the first 3 or 4 days, then turns pink, then brown and finally white or colorless at around 10 days. You will also have lochia if you have a Cesarean delivery, although it may be less than occurs with a vaginal birth.
If the discharge is foul-smelling, remains heavy or is extremely light the first few days, tell your healthcare provider. He or she may want to examine you.
If you don’t breastfeed, your first menstrual period occurs within 6 to 8 weeks after giving birth. If you breastfeed, you may not have a regular menstrual period until you wean your baby.
If you take care of yourself after delivery, you should not feel ill. Occasionally problems do occur. Refer to the list of symptoms and warning signs below. Call your healthcare provider immediately if you experience any of the following:
•unusually heavy or sudden increase in vaginal bleeding (more than your normal menstrual flow or soaking more than two sanitary pads in 30 minutes)
•vaginal discharge with strong, unpleasant odor
•a temperature of 101F (38.3C) or more, except in the first 24 hours after birth
•chills
•breasts that are painful or red
•loss of appetite for an extended period
•pain, tenderness, redness or swelling in the legs
•pain in the lower abdomen or in the back
•painful urination or an intense need to urinate
•severe pain in the vagina or perineum
Temporary emotional changes are not uncommon during the postpartum period. You may have mood swings, mild distress or bouts of crying. See the discussion of postpartum distress that begins on page 328. Mood changes are often a result of birth-associated hormonal changes in your body.
Lack of sleep may play a part in how you feel. Many women are surprised by how tired they are emotionally and physically in the first few months after baby’s birth. Take time for yourself, and allow yourself a period of adjustment.
Sleep and rest are essential after baby is born. To get the rest you need, go to bed early when possible. Take a nap or rest when your baby sleeps.
Have you heard how important it is to “bond with your baby”? What is bonding? Is it really important in your life with baby? When does it happen? How does it happen?
Bonding is a process that usually takes longer than one instance for it to occur. It’s the process of becoming emotionally attached to your child, and it deepens over time.
We once believed bonding was a purely emotional response, but today we believe there is also a physical aspect to bonding. Some researchers theorize bonding stimulates production of prolactin and oxytocin in you, which causes you to feel more motherly toward your baby.
Carrie was due to deliver soon and wanted to breastfeed, but she was scared she couldn’t do it. She had read books, talked to friends and knew lots of information. I think her biggest fear was she would be left alone with this new baby and wouldn’t know what to do. I told her it didn’t work that way, and there would be lots of help available. One of the best places to learn to breastfeed is in the hospital after baby’s birth. The nurses are experienced in helping new moms learn how to get started, and they’re available to help after you go home. Women have told me after they went home, they called the hospital nursery and even went back for help.
The hour following birth is a prime bonding time for mom, dad and baby. However, you can bond with your baby in the delivery room, your hospital room or at home. Don’t be afraid the bond will be weaker if you and baby cannot “meet in the delivery room.” A mother and her infant are programmed to connect after baby’s birth. Both need each other. The mother needs to see, touch, smell and hold this person she has carried for 9 months. The baby needs the comfort of his mother’s touch after going through the stressful birth process.
Bonding often begins in the delivery room. Ask your healthcare provider if procedures normally done can safely be postponed for a little while so you can share this time together. If you can’t hold your baby, ask your partner or a nurse to hold the baby up to your face, where you can nuzzle him with your cheek.
Bonding can continue in your hospital room if baby’s in your room. You can respond to baby whenever he needs you. Breastfeeding is one of the best ways for a mom to bond with her baby, especially if baby is fed on demand.
If you don’t breastfeed, you can still bond when you bottlefeed. Respond to your baby when he cries. Look at baby, talk to him and hold him close. Create as much skin-to-skin contact as possible.
As your infant begins to mature, the bonding process will be strengthened. Relax and let it happen. Dad also needs to bond with baby. Encourage your partner to hold baby close and make eye contact and skin contact. He can also respond when the baby cries. Let Dad feed him when you begin expressing your breast milk.
The key to bonding is to focus on the baby and the experiences you share. Include baby in your daily activities. For example, if you’re ironing or doing the dishes, put him in his infant carrier and keep him close to you. Talk to him or sing silly songs.
Holding, cuddling and cooing are other great ways to bond. Your baby will connect with you both when he feels the love and security you each offer.
Some women choose to have a form of surgical sterilization performed, called tubal ligation, postpartum tubal ligation or BTL, while they are in the hospital after baby’s birth. Tubal ligation is the number-one birth control method in the United States. About 28% of women who use contraception have chosen tubal ligation—11 million women. Half of all tubal sterilization procedures are performed following delivery of a baby, while the woman is still in the hospital.
The surgery involves blocking a woman’s Fallopian tubes to prevent further pregnancies. If you have decided before baby’s birth to have tubal ligation, doing it after delivery while you’re still in the hospital can make sense. If you received an epidural for your labor and delivery, you’re already anesthetized. If you didn’t have an epidural, the procedure may require general anesthesia.
The failure rate for tubal ligation is 1 to 2 in 1000 procedures. Failure rates are a little higher with tubal ligations performed immediately after delivery than they are when they are performed at other times.
If you have a postpartum tubal ligation, your healthcare provider may want to examine you 10 to 14 days after you leave the hospital. He or she will check the incision to see if it is healing properly and look for signs of infection.
Many women are eager to begin exercising after baby is born. Exercise helps you feel better physically and can lift your spirits. You can start by doing simple isometric exercises the day after delivery. Practice holding in stomach muscles, or start with mild Kegel exercises.
When you’re up and about again, you can do other forms of exercise. Do something you enjoy, and do it on a regular basis. Walking and swimming are excellent exercises to help you get back in shape. Your aerobic capacity can increase as much as 20% in the 6 weeks following baby’s birth. This is good news, especially if you’re overly fatigued. As your hormones return to a normal level, you’ll probably have more energy. Before you start any postpartum exercise program, check with your healthcare provider. He or she may have particular advice for you.
Be careful about beginning an exercise program too soon. Don’t overtire yourself by choosing a program that is too ambitious. Always get enough rest.
After a Cesarean delivery, light activity is important. In the hospital, you may have to practice coughing or deep breathing to keep lungs clear. Wiggle toes to aid circulation. Walking may not be easy, but it helps minimize the chances of developing a blood clot in your lower extremities. Check with your healthcare provider before starting an exercise routine or exercise program of any kind.
A source of discomfort after you deliver will be in the vagina and between the opening of the vagina and the rectum, called the perineum. Pain or discomfort should lessen every day. You will be given a prescription for mild pain medications if necessary. It’s OK to take pain medicine, but it usually isn’t needed as much once you’re home. You may want to continue to take your prenatal vitamins or iron supplements.
It’s normal to bleed after delivery; bleeding continues for several days up to a couple of weeks. In the hospital, nurses will check bleeding to be sure it isn’t excessive. If bleeding after delivery was excessive, you may be prescribed vitamins and iron. When you leave the hospital, you will still be bleeding, but the amount of bloody discharge should be decreasing. Sometimes when you go home and are more active, bleeding may be a little heavier at first, but it shouldn’t last more than a few hours before it slows down again.
If there is concern about infection, you may be given antibiotics. If you’re Rh-negative, you may be given RhoGAM. Laxatives and stool softeners are often prescribed to help you avoid constipation.
When you go home, increase activities gradually. Walk around, eat more normally and become more active each day. You may need to rest frequently—that’s normal. Pay attention to your body. Most healthcare providers recommend you wait until after your 6-week postpartum checkup before you begin any strenuous activity, exercise or become sexually active again.
If you take pain medicines or have problems, such as dizziness, don’t drive. It’s OK to use stairs, but plan ahead so you’re not running up and down stairs all day.
Full recovery is different for every woman. If you had complications or problems, it may take longer. From 2 to 6 weeks, you should be feeling a little better every day. You probably won’t be taking pain medicine any longer, and bleeding will decrease or it will have stopped.
Recovery from a Cesarean delivery is different from recovery from a vaginal birth. You have undergone major abdominal surgery, so be prepared to take it easy for a while. Although you have experienced many of the same situations as someone who had a vaginal birth, you face some additional restrictions.
Get up and out of bed as soon as possible after baby is born. Moving helps prevent blood clots in the legs, lung collapse and pneumonia. Walking helps body functions, such as relieving constipation and abdominal gas.
Be careful not to strain stomach muscles. Avoid lifting anything heavy. Once home, keep your incision clean and dry, and watch for infection. Infection of a Cesarean incision usually occurs 4 to 6 days after surgery. If any of the following signs appear, contact your healthcare provider immediately. Signs of infection include the following:
•redness that spreads from the edges of the incision
•fever
•hardness around the incision
•discharge from the incision site
Although you did not deliver vaginally, you will probably experience painful uterine contractions for several days after delivery. This is a sign your uterus is returning to its prepregnancy size. If you breastfeed, you may notice the pains when your baby nurses.
You will have lochia with a Cesarean delivery. However, your discharge may be lighter than lochia that follows a vaginal birth.
If you’re interested in exercising after a Cesarean, you can usually begin light exercise about 4 weeks after birth. You can probably resume full activity between 4 and 6 weeks postpartum. Your healthcare provider can advise you.
One concern you and your partner may share after delivery is postpartum sex. Getting back into “the swing of things” after your baby is born can be difficult. Stress, hormonal changes, emotions, fatigue and other physical factors, such as bleeding, can affect your sex drive. Pain from an episiotomy or an incision can also be a factor.
We once advised women to wait at least 6 weeks before having intercourse. If you feel no pain or discomfort and your episiotomy has healed, you can resume sexual relations when you feel comfortable. Be sure bleeding has stopped. For most women, this will be at least a few weeks after delivery.
If you decide to have intercourse, you need to take precautions if you don’t want to become pregnant again. You can become pregnant before you have a menstrual period. Discuss birth-control options with your healthcare provider.
Contraception is something you and your partner may want to think about. You will probably begin ovulating 6 to 8 weeks after birth, and you could get pregnant again. If you do not want to have another baby very soon, discuss birth-control options with your healthcare provider in the hospital or at your postpartum checkup.
Breastfeeding protects you against pregnancy to some degree, but breast-feeding is not an effective method of birth control. If you breastfeed, consider birth-control methods if you want to postpone pregnancy.
If you used a diaphragm or cervical cap for birth control in the past, you need to be refitted after delivery. The size of your cervix or vagina may have changed. You may consider condoms or spermicides if you breastfeed. Neither interferes with breastfeeding.
If you bottlefeed, you may decide on a method that can be started immediately after delivery. These methods include hormone implants, Depo-Provera injections, a progestin-only pill or an IUD. If you want to use a combination birth-control pill, which contains estrogen and progestin, wait at least 2 weeks after delivery to begin.
When your older children come to the hospital to see you and meet the new baby, greet them with open arms (that means not holding the baby). If a younger child sees you holding the baby right away, he or she may feel displaced. Give your children, especially toddlers, lots of attention. It’s hard on kids to be displaced by a new baby, so your extra attention is welcome.
When you go home, let your children help with the new baby. Even a young child can get you a diaper or baby wipes.
Remind those who come to visit to recognize your older children before the baby. This helps the older child feel secure and provides him or her the opportunity to “show off” the new baby. If you have to let some household chores go for a while to provide your children with the attention they need, that’s OK.
To help ease the transition, get your partner involved with older children. Try making these changes before the baby is born so they become part of your family routine. A few things dad can do to make older children feel special include the following.
•Take over some chores, such as getting older children ready for bed or reading to them.
•Create some special time together with the kids. Go to the library together on Saturday mornings, or cook dinner together one night a week.
•Spend time together at home. Make one evening a “family” evening when you play games, listen to music or read together. No TV on these special nights!
•Dad can help children learn to do chores. Even young children can help empty the trash or clear the table. When everyone works together, more work gets done faster. And it’s more fun, too!
You must decide if you want to breastfeed or bottlefeed. Even after you choose a method, you may have to make adjustments after your baby is born.
Early in life, most babies eat every 3 to 4 hours, although some babies feed as often as every 2 hours. It may help your baby get on a regular schedule if you time the feedings. Or let baby set the schedule; some babies need to feed more often than others.
Sometimes a baby needs to feed more often than she normally does. See how often your baby wants to feed and whether she is growing properly. A baby usually waits longer between feedings and feeds longer at each feeding as she grows older.
A baby is usually the best judge of how much to take at each feeding. Usually she will turn away from the nipple when she’s full.
At her 37-week visit, Lily wanted to talk about breastfeeding and bottlefeeding. With her first child, she had tried breastfeeding and had a miserable experience, giving up after 2 weeks. This time she planned to bottlefeed from the start and wanted to know if this was OK. Friends and family had been giving her a hard time about it. I reassured her bottlefeeding was fine and not to feel guilty. I told her breastfeeding wasn’t for everyone; it’s an individual decision. Lily left my office feeling better. Giving birth to, caring for and raising a baby requires making a lot of decisions. Some aren’t easy to make.
Breast milk contains all the nutrients a baby needs, and it’s easy for baby to digest. Breastfed babies have lower rates of infection because of the immunological content of breast milk. Breastfeeding can also give baby a sense of security and the mother a sense of self-esteem. However, if there are reasons you cannot or choose not to breastfeed, baby will do well if you bottlefeed her formula.
See the discussion of bottlefeeding and breastfeeding in Appendix B that begins on page 349.
After the birth of your baby, you may notice lots of changes in your body—it’s only natural. You may see changes in your abdominal shape and skin. Breasts may also be affected.
After they give birth, some women find their abdomen returns to normal naturally. For others, it never quite returns to its prepregnancy state. Abdominal skin is not like muscle, so it can’t be strengthened by exercise. Perhaps the most important element affecting your skin’s ability to return to its prepregnancy tightness is connective tissue, which provides suppleness and elasticity. As you get older, your skin loses connective tissue and elasticity. Other factors include your fitness level before pregnancy, heredity and how much your skin stretched during pregnancy.
After giving birth, most women’s breasts return to their prepregnancy size or even decrease a little in size. If you breastfeed, it takes longer for your breasts to return to normal. This is a result of the change in the connective tissue that forms the support system of your breasts. Exercise cannot make breasts firmer, but it can improve the chest area underneath so breasts have better support.
Don’t get anxious about losing pregnancy weight after your baby’s birth. Regaining your prepregnancy figure may take longer if you’re older. It’s normal to lose 10 to 15 pounds immediately after baby is born. An additional 5 pounds of fluid may wash out of your system within a few days.
Extra weight may be harder to lose. Your body stored 7 to 10 pounds of fat as energy for the first few months after birth. If you eat properly and get enough exercise, these pounds will slowly come off.
If you breastfeed, all the nutrients your baby receives depend on the quality of the food you eat. Breastfeeding places more demands on your body than pregnancy. Your body burns up to 1000 calories a day to produce milk. When breastfeeding, you need to eat an extra 500 calories a day. Be sure they are nutritious calories (eat fruits, vegetables and breads—stay away from junk food). And keep up fluid levels.
You may experience many emotional changes after baby is born. Mood swings, mild distress or bouts of crying are not uncommon. Changes in moods are often a result of hormonal changes you experience after birth, just as they were when you were pregnant.
Many women are surprised by how tired they are emotionally and physically in the first few months after baby’s birth. Make sure you take time for yourself. Sleep and rest can help you deal with mood shifts, which seem to occur more often when a woman is exhausted.
After pregnancy, many women experience some degree of depression. This is called postpartum distress syndrome (PPDS). Some experts believe postpartum depression may begin during pregnancy, but symptoms may not appear until several months after delivery. They may occur when a woman starts getting her period again and experiences hormonal changes.
Postpartum distress syndrome can resolve on its own, but it can often take as long as a year. With more severe problems, treatment may relieve symptoms in a matter of weeks, and improvement should be significant within 6 to 8 months. Often medication is necessary for complete recovery.
If your baby blues don’t get better in a few weeks or if you feel extremely depressed, call your healthcare provider. You may need medication to help deal with the problem.
There are different degrees of depression. The mildest form is baby blues. Up to 80% of all women have “baby blues.” They usually appear between 2 days and 2 weeks after the baby is born. They are temporary and usually leave as quickly as they come. This situation lasts only a couple of weeks, and symptoms do not worsen.
A more serious version of postpartum distress is called postpartum depression (PPD). It affects about 10% of all new mothers. The difference between baby blues and postpartum depression lies in the frequency, intensity and duration of symptoms.
PPD can occur from 2 weeks to 1 year after the birth. A mother may have feelings of anger, confusion, panic and hopelessness. She may experience changes in her eating and sleeping patterns. She may fear she will hurt her baby or feel as if she is going crazy. Anxiety is one of the major symptoms of PPD.
The most serious form of postpartum distress is postpartum psychosis (PPP). The woman may have hallucinations, think about suicide or try to harm the baby. Many women who develop postpartum psychosis also exhibit signs of bipolar mood disorder, which is unrelated to childbirth. Discuss this situation with your healthcare provider if you are concerned.
Your Appearance
After your baby’s birth, you may be concerned about your appearance. Although you won’t immediately regain your prepregnancy figure, there are a few things you can do to look and feel better.
•Buy and wear a well-fitting, supportive nursing bra.
•Oversized shirts (your partner’s may do the trick) offer you variety. Stay away from your maternity clothes, which you probably want to burn anyway.
•Wear tops untucked—wait a little while for tummy muscles to tighten up before tucking tops in.
•Wear comfortable drawstring pants, elastic-waist or stretch pants.
•A loose-fitting dress can be flattering because it doesn’t hug your curves.
•Don’t wear sloppy clothes, such as sweatshirts and sweat pants, very often; sometimes when you wear sloppy clothes, you feel sloppy.
After you give birth, if you believe you are suffering from some form of postpartum distress syndrome, contact your healthcare provider. Every postpartum reaction, whether mild or severe, is usually temporary and treatable.
It’s normal to feel extremely tired, especially after the hard work of labor and delivery and adjusting to the demands of being a new mom. However, if after 2 weeks of motherhood you’re just as exhausted as you were shortly after you delivered, you may be at risk of developing postpartum depression.
Researchers aren’t sure what causes postpartum distress; not all women experience it. A woman’s individual sensitivity to hormonal changes may be part of the cause; the drop in estrogen and progesterone after delivery may contribute to PPDS.
A new mother must make many adjustments, and many demands are placed on her; either or both of these situations may cause distress. If you had a Cesarean delivery, you may also be at greater risk for postpartum depression.
Other possible factors include a family history of depression, lack of familial support after the birth, isolation and chronic fatigue. You may also be at higher risk of suffering from PPDS if:
•your mother or sister suffered from the problem—it seems to run in families
•you suffered from PPDS with a previous pregnancy—chances are you’ll have the problem again
•you had fertility treatments to achieve this pregnancy—hormone fluctuations may be more severe, which may cause PPDS
•you suffered extreme PMS before the pregnancy—hormonal imbalances may be greater after the birth
•you have a personal history of depression or you suffered from untreated depression before pregnancy
•you have experienced any major life changes recently—you may experience a hormonal drop as a result
•you are anxious or have low self-esteem
•you have a struggling relationship with baby’s father
•your access to finances and health care is limited
•you experience little social support
•you have a colicky or high-maintenance baby
•you experienced a lack of sleep during pregnancy, you sleep less than 6 hours in a 24-hour period or you wake 3 or more times a night
In addition, if you answer “most of the time” or “some of the time” to any of the following questions, you may be at increased risk.
•I blame myself when things go wrong (even if you have nothing to do with them).
•I often feel scared or panicked without good reason.
•I am anxious or worried without good reason.
One of the most important ways you can help yourself handle baby blues is to have a good support system near at hand. Ask family members and friends to help. Ask your mother or mother-in-law to stay for a while. Ask your partner to take some work leave, or hire someone to come in and help each day.
Rest when your baby sleeps. Find other mothers who are in the same situation; it helps to share your feelings and experiences. Don’t try to be perfect. Pamper yourself.
Do some form of moderate exercise every day, even if it’s just going for a walk. Eat nutritiously, and drink plenty of fluids. Get out of the house every day. Eating more complex carbohydrates may help raise your mood. And giving baby a massage may help you because it helps you connect with your baby.
Talk to your healthcare provider about temporarily using antidepressants if the above steps don’t work for you. Many women who suffer from postpartum depression require medication for up to 1 year.
Beyond the relatively minor symptoms of baby blues, postpartum distress syndrome can appear in two ways. Some women experience acute depression that can last for weeks or months; they cannot sleep or eat, they feel worthless and isolated, they are sad and they cry a great deal. For other women, they are extremely anxious, restless and agitated. Their heart rate increases. Some unfortunate women experience both sets of symptoms at the same time.
If you experience any symptoms, call your healthcare provider immediately. He or she will probably see you in the office, then prescribe a course of treatment. Do it for yourself and your family.
If you experience baby blues or PPD, it can also affect your partner. Prepare him for this situation before baby is born. Explain to him that if it happens to you, it’s only temporary.
There are some things you might suggest to your partner that he can do for himself if you get blue or depressed. Tell him not to take the situation personally. Suggest he talk to friends, family members, other fathers or a professional. He should eat well, get enough rest and exercise. Ask him to be patient with you, and ask him to provide his love and support to you during this difficult time.
Your body changes a lot in the 4 to 6 weeks following delivery. By the time you visit your healthcare provider for your 6-week postpartum checkup, your uterus will be about the size of a grapefruit. That’s an incredible feat, considering it was the size of a small watermelon only a few weeks before!
At your visit, tell your healthcare provider if you have had headaches or experienced increased irritability or fatigue; you may be prescribed an iron supplement. You will have a physical exam, similar to the one at your first prenatal exam. Your healthcare provider will probably check your weight and blood pressure. The average weight loss after giving birth is about 12 pounds.
Your healthcare provider checks any incision you have. Your breasts are examined, and your uterus, ovaries and cervix are checked—yes, that means another pelvic exam. Your healthcare provider may discuss postpartum depression with you; you may undergo screening for the condition.
If you had a vaginal birth, your healthcare provider will examine any tears or incisions. If you had a Cesarean delivery, your incision will be examined. If you developed hemorrhoids or varicose veins during pregnancy, your healthcare provider will also check those.
If you took any medication before or during pregnancy, ask about continuing it or resuming it now. If you have any questions about your recovery, address them at this time. It’s a good time to discuss birth-control options if you don’t want to become pregnant again immediately.
Your 6-week postpartum checkup is also a good time to ask questions about future pregnancies. Discuss concerns about, and complications from, your recent delivery. This information can be helpful if you move or deliver with a different healthcare provider or hospital in the future.