II. CONFIGURATIONS IN PLAY AND DREAMS
Configurations in Play—Clinical Notes (1937)
Introduction
Listening to an adult’s description of his life, we find that a clear vista into his past is limited by horizons: one is the onset of puberty, with its nebulous “screen memories;” another the onset of the so-called latency period through which, in retrospect, memories appear inaccurate and obscure, if at all. In our work with children we meet another horizon, the period of language development. “The material which the child furnishes us,” says Anna Freud in her Introduction to the Technic of Child Analysis, “supplies us with many welcome confirmations of facts which up to the present moment we have only been able to maintain by reference to adult analysis. But . . . it does not lead us beyond the boundary where the child becomes capable of speech; in short, that time from whence on its thinking becomes analogous to ours.”1
Associations, fantasies, dreams lead in the analysis of the adult mind to the land beyond the mountains; in child analysis these roads lose their reliability and have to be supplemented by others, especially the sequences which occur spontaneously in the child’s play.
It seems to me, however, that when substituting play for other associative material we are inclined to apply to its observation and interpretation methods which do not quite do justice to its nature. We tend to neglect the characteristic which most clearly differentiates play from the world of psychological data communicated to us by means of language, namely, the manifestation of an experience in actual space, in the dynamic relationship of shapes, sizes, distances—in what we may call spatial configurations.
In the following notes it is hoped to draw attention to this spatial aspect of play as the element which is of dominant importance in the specificity of “Spiel-Arbeit.” These notes are based on observations made for the most part in the twilight of clinical experience, and must be supplemented by systematic work with normal or only slightly disturbed children. For although the adult who is not an artist must undergo the specific psychoanalytic procedure in order to reveal his unconscious in the play of ideas (a procedure which cannot easily be replaced for “scientific purposes” by less intimate and more systematic arrangements), the child in his play continuously and naturally “weaves fantasies around real objects.2”
I. “Houses”
An anxious and inhibited four-year-old boy, A, comes for observation. The worried mother has told us: (1) that he is afraid to climb stairs or to cross open spaces; (2) that as a baby he had eczema and that for eight months his arms were often tied in order to prevent his scratching; and (3) that until recently he continued to wet himself, with a climax at the time of a younger sister’s arrival.
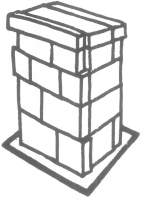
Let us see what he shows in the first minutes of play. Taking a toy house he places three bears close together in one corner. The father bear is lying in the bathtub, the mother bear is washing at the sink, while the baby bear is drinking water. The emphasis on water reminds us of the boy’s urinary difficulty. It also must mean something that the family is placed so close together, for he then arranges a group of animals outside the house equally close to one another. “Can you build a cage around these animals?” he asks me. Provided with blocks, he builds the “cage” shown in Figure 1 beside them—a house-form which on a normative scale of infantile house-building would belong to a much younger age. At five one knows that a house is “around something”; but A has forgotten the animals. He seems to use the blocks in order to express the feeling of being caged; he even places a small picture frame which he finds among the toys around the cage itself. Thus he is indicating in the content of his play what is libidinally the most important function of his body (urination) and in the spatial arrangement of the toys he expresses narrowness and the feeling of being caged, which we are inclined to trace to the early traumatic experience of being tied and to connect with his present fears of open spaces.
Figure 1
The boy then begins to ask persistently for many details about things in my room. When asked, “What is it you really want to know?,” he quiets down quickly and in a dreamy way turns a shallow bowl upside down and puts many marbles into the cavity of its hollow base. This he repeats several times, then takes one toy car after the other, turns it upside down and examines it.
Here, finally, we have behavior which belongs to the “putting-into” and “taking-out” type of play. By his persistent questions, and his silent examination of the toy cars, he seems to express an intellectual problem: “What is the nature of the underside of things?” This question arises because of the real conflict with the objective world which began when his mother gave birth to his sister, and represents the material most accessible for future psychoanalytic interpretation.
Beneath this level we see that two aspects of his “physical” experiences are expressed in his play. The one indicating strong interest in a pregenital (urethral) function will, during treatment, offer material for interpretation and will at the same time necessitate retraining. The earlier experience, the feeling of being caged, seems to be connected deeply with the impression which a seemingly hostile world has made on this child when he was still so young that his only method of defense was a general withdrawal. This must have so influenced his whole mode of existence as to create severe resistances to the analytical or educational approach.
The crux of this resistance is shown in the fact that for an abnormally long time A wanted to walk only in a walker. To be tied, once distasteful, proved in this instance to be a protection. We may assume that it is this double aspect of physical restriction, what it once did to his ego and how his ego is now using it which A expressed in his very first play constructions when he was brought to me, because of his fear of openness and height.
In stating that A expressed some quality of his experience of body and environment in the form of a cage-house, we imply not only that alloplastic behavior may reproduce the pattern of a traumatic impression and an autoplastic change imposed by it, but also that in play a house-form in particular may represent the body as a whole. And indeed, we read of dreams that: “The only typical, that is to say, regularly occurring representation of the human form as a whole is that of a house, as was recognized by Schemer.”3 As is well known, the same representation of the body by the image of a house is found throughout the gamut of human imagination and expression, in poetic fantasy, in slang, wit and burlesque, and in primitive language.
It would not, therefore, be important to lay much stress on the fact that in play, as well, a house-form can mean the body were it not that it is simple to ask a child to build a house, which often reveals the child’s specific conception of and feeling for his own body and certain other bodies. We seem to have here a direct approach through play to the traces of those early experiences which formed his body-ego.
This assumption led to interesting results when older children and even adults were given the task of constructing a house. Two extreme examples may suffice here.
A girl of twelve, B, had, at the age of five, developed a severe neurosis following the departure of her first nurse, who had been in the house from the time of the child’s birth. The nurse had spoiled B; for example, by allowing her to suck her thumb behind her mother’s back, and to eat freely between meals. During the mother’s frequent absences, B and her nurse lived in a world of their own standards; the nurse shared the secret of the girl’s first sex play with a little boy, while the girl was the first person to hear of it when the nurse became pregnant. B had just begun to puzzle about this fact when the parents discovered it and peremptorily discharged the nurse. Knowing nothing of the shared secrets, they were unaware that in so doing they were suddenly depriving the girl of a queer and asocial intimacy for which she was unable to find a substitute, especially since the mother set out to break, in the shortest possible time, all of the bad habits left from the nurse’s era. The result was a severe neurosis. When I saw the child for the time with no knowledge of the psychogenesis of her neurosis, I noted a protruding abdomen, and my first impression was, “She walks like a pregnant woman.” The secrets she had shared with her nurse and their pathogenic importance became apparent only later, however, when she confided that sometimes she heard voices within herelf. One voice repeated: “Don’t say anything, don’t say anything,” while others in a foreign language seemed to object to this command. She could save herself from the anxiety and the voices only by going into the kitchen and staying with the cook, obviously the person best fitted to represent the former nurse.
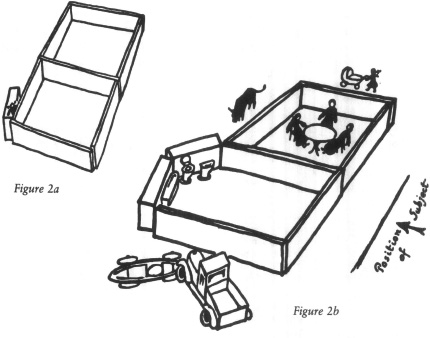
B first built a house without doors with a kind of annex containing a little girl doll (Figure 2a). Then she changed the house and built form 2b with many significant objects placed in and around it. In a vertical position we can see that the house-form could represent not only her own unusual posture but also the unconscious determinants for it, especially her identification with the pregnant nurse. The following superficial parallels (and I assume that deeper investigation of similar cases would reveal these as typical spatial elaborations of infantile body feelings) may be drawn:
CONSTRUCTION |
HOUSE |
BODY |
1 A little girl with a baby carriage goes to the country (to the cow). |
Outside the House: Where there is freedom. |
Head: Where she thinks she would like to go away: to the nurse who gave her everything to eat. |
2 A family around a table. |
In the Dining Room: Where the child has conflicts with the parents about eating. Where she is present when the parents (immigrants) talk about her in a foreign language. |
Inside the Body: Where one feels conflicts. Where she hears foreign voices quarrel. |
3 A cow in the country. |
Outside the House. |
In Front of the Chest: Where women (nurses) have breasts which give milk. |
4 Bathroom furniture behind thick protruding walls. |
In the Bathroom (thick walls): Where the secret is (the closed doors); the forbidden (nakedness, masturbation); the dangers (threats concerning masturbation); the bloody things (menstruation); the dirty (toilet activities). |
In the Protruded Abdomen: Where the secret is (the baby and it origin); that which is forbidden (the baby); the dangers (the growing baby); dirt (feces). |
5 A red racer and a truck in collision. |
Outside the House: Where the dangerous but fascinating life is, from which the parents try to protect the child. The accident. |
Under the Abdomen: Where it seems a girl can lose something, since boys have something there and girls do not. Where people say girls will bleed. Where men do something to women. Where babies come out, hurt women and sometimes kill them (the nurse died shortly after childbirth). |
The doorless house not only pictures the child’s posture, and shows the unconscious idea of having incorporated the lost nurse, it seems also to indicate that part of her body which is firmly entrenched within the fortress of ego-feelings, as distinguished from what are only thoughts and fears concerning the body, felt as “outside”: the expectation of breasts and the fear of menstruation, of which she had been warned.
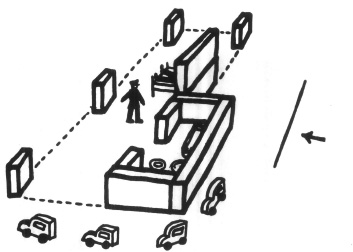
Figure 3
As a further example justifying our looking at the house from different positions and our assumption that the walls reveal something of the builder’s body-ego, the following is of interest: A young schizophrenic man, C, a patient in the Worcester State Hospital, built the house shown in Figure 3.
He said it was a screen house all around, except for the back part. This patient complains of having no feeling in the front of his body. Ever since he was the “victim” of a spinal injection, he claimed that he suffered from a certain electric feeling drawing down from his spine to the rectum, and from difficulties in urination. He walked in a feminine manner with protruding buttocks. One may recognize this posture in the house-form. C strengthened that part of his house which corresponded to the spine of his body by placing two blocks on top of one another, and he furthermore placed walls around one room only (the bathroom) which in position corresponded to his buttocks. The cars are again put at the place corresponding to that of the urethrogenital region on the body and their arrangements suggested a symbolizing of the patient’s urethral symptoms (he could urinate only “in bits”).
In children without marked orality and adults without psychotic symptomatology, I have not found such detailed parallels between posture and house-forms as those of cases B and C. In laying out the play of their houses, they stood over it in such a way that the house, as compared with a body, was “dorsal recumbent,” and therefore might be said to represent more a baby’s than an adult’s body-ego. By rotating the diagrams, we recognized in the same constructions the subject’s posture which could be interpreted as expressing an identification with a mother image. It seems that the phenomenon of most striking similarity between house-forms and posture is based on the introjective and projective mechanisms of orality, which must be assumed to be active in the establishment of the body-ego in earliest childhood.

Figure 4
In attempting to find similar relationships between the growing organism and the typical block-building of normal children, one will have to be prepared for a much less striking and more sophisticated spatial language in which more emphasis is laid on structural principles than on similarity of shape. Interestingly enough, from Ruth Washburn’s nonclinical material, only children with strongly emphasized orality produced parallels between body and house at all similar to B’s and C’s constructions. The house-form shown in Figure 4 was built by D, who was a fat, egoistic boy of five, a heavy eater. He explained that room 1 is the entrance, room 2 the living room. About room 3 he said: “This is where the water goes through; it is not going through now, though.” He added, “There is a drawbridge; when boats come, you pull it up.” D’s eagerness to “take in” and his reluctance “to give away” are well illustrated by the large opening of the entrance and the complicated closing arrangements at the other end, where water and boats go through the house.
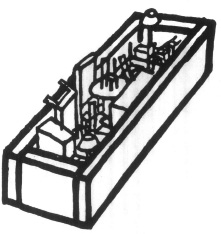
Figure 5
Returning to analytical material from children, we select a house-form of a boy of eight, E, which, in its primitiveness reminds us of A’s construction. Upon my advice, E had been brought home from a special school where, diagnosed as defective, he had spent half his life. The problem was to find out whether with psychoanalytic help he could resume ordinary home and school life. When he came to his first hour, tense and hyperactive, he remained in my office just long enough to build a house with the blocks he found there (Figure 5). This house, primitive and without doors (like A’s house), was filled chaotically with furniture. When, after a few minutes, he ran away shouting that he never would come back, he left behind him nothing but this doorless wall, dividing an outside from a chaotic inside.
I accepted this theme of a closed room and devoted the next few appointments to a short discussion of whether he had to stay and for how long, and whether or not the door of my room would remain open. On the second day he did not want to stay, although the door was not closed. He was immediately dismissed, sooner in fact than he really wanted to go. On the third day he stayed for a few minutes; on the fourth, he asked whether he could stay the whole hour; but when the door was closed, he was driven at once to manifestations of anxiety. He had to touch all the little buttons or protrusions in the room. I made the remark that it seemed as though he had to touch everything, and that he gave me somewhat the impression that for touching something (I did not know what) he expected to be put in jail. His blushing showed that he understood. Like most children who do not quite understand why they are detained with problem children, he had associated the sexual acts of some of them with his own sins and with “being a problem” in general. What he did not remember was that in his infancy, he, like A, had been tied when he rocked his bed (muscular masturbation with genital and anal elements).
The next day he asked questions, all of which began with, “Who has the power to . . .” and since I had heard from his mother that at home he was greatly worried because she wanted to get rid of a soiling cat, I told him that his mother had asked me about the cat and that I had told her she had no right to send the cat away. One should give cats and children a chance before one tries to get rid of them. He sat down and asked softly, “Why do I get so furious?”—and after a long silence, “Why do boys get so furious?” To every reader of Anna Freud’s Introduction to Child Analysis it is obvious that this question shows a concern which is important for the therapeutic situation. While his defiant behavior at first had announced that he did not wish to be sent away or kept anywhere because of his violent aggression, his question showed insight, confidence, and a readiness for conversation. I asked him why he thought boys were “furious.” “Maybe because they are hunters . . . ,” he suggested.
Then we began to compare what boys wanted to be with what girls wanted to be, and to make out a written list containing on the one side the toys which boys liked: (streamline train, speedboat, gun, bow and arrow); and on the other those preferred by girls: (doll, doll’s house, doll clothes, carriage, basket). The one group could be summed up under the symbol of an arrow and the other under that of a circle. I asked him whether this did not remind him of a certain detail in the difference between a boy’s body and a girl’s body. “That is why,” he said thoughtfully, “I call my streamline train Johnny Jump-up.’ ” So we talked about the psychobiological implications of having a penis, the fear of the impulses connected with its possession and the fear of the possibility of not having one. He seemed somewhat relieved.
The next day the cat interfered again. Her regression as to toilet habits had, to say the least, been overdetermined: she was, as everybody at home now agreed, pregnant. But no one could tell just when the kittens would arrive. The questions when do the kittens want to come out and when will they be allowed to come out, became the patient’s main interest in life. Unfortunately, his unlucky father and his even more unlucky analyst happened to tell him different periods for the duration of a cat’s pregnancy. He wondered seriously if God himself was sure when the kittens should come out.

Figure 6
One day, having left the office for a moment, I returned to find E all rolled up in the cover of the couch. He remained there half an hour. Finally, he crawled out and sat beside me. I began to talk about the kittens kept in the cat, children kept in special schools, babies tied in their beds and stillborn babies kept in glass jars. (I knew that not long ago he had seen such an exhibit, and that someone had jokingly told him it was actually a stillborn brother of his.) He probably could not remember, so I added that when he was a baby his father had tied him to his bed because he had rocked so loudly during the night. He blushed and when he got up from the sofa I noticed that he had tied his hands and feet before rolling himself up in the cover.
The toy which he subsequently chose for his first concentrated play in my office was a bowl (Figure 6), a piece of which was broken off. (It will be mentioned here in connection with several cases.) He turned it around to “shoot” marbles into it. For a while we competed at this game, until another cloud came up over the horizon.
As to Figure 5, one can see now how many different phenomena it “meant,” all of them similar only in the possession of strong walls, no doors and chaos within—attributes at one and the same time of his tension of mind and body; his experience of being tied in bed; his concept of the female body as a claustrum; his experience and expectation of being kept at a place far from his family; and last, but not least, my office. In beginning our relationship with the “spatial” discussion of this last mentioned “cage” (office), we succeeded in lining up all his cage-conceptions before an interpretation which included them all was given. The play with the marbles, then, was the first free, though not yet quite uncompulsive, expression of that phallic tendency which, in its unsublimated form, had given him the impulse “to do something to women”—and the fear of “being put in jail.” Soon afterwards his intrusive tendencies began to possess him entirely in the sublimated form of “scientific” curiosity. Appealing for comradely help from his father, and equipped with an extensible telescope, he entered Mother Nature’s secluded areas and investigated birds’ nests and other secrets.
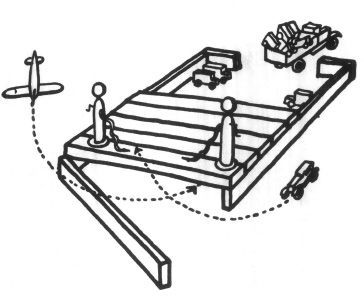
Figure 7
In analyzing the full significance of a certain house-form in play, as in the evaluation of a well-known dream symbol, we need the aid of biographical material. On the other hand, the form of the house itself and the play activity provoked by it will sometimes tell at once where on the scale of object-relationships our small patient can be assumed to be; whether absorbed in narcissistic orality like B, C and D, or restricted by an early psychophysiological experience like A and E, or whether he has achieved a fearless, clear object-relationship, expressed in unrestricted functional play as in the case of F, which follows.
F, a boy of five, was not a patient—he was occasionally brought into the office to play for an hour (a pleasant procedure of regular, preventive observation). At the time of the visit to which I am referring, F talked at home in a rather unrepressed way about impulses towards his mother’s body. She would, he hoped, let him put the next baby into her.
In my office he built a house (Figure 7), and played contentedly, without showing compulsion or anxiety, for a whole hour. Trucks drove into the backyard to unload dozens of little cars which were lined up. A little silver airplane and a red car were the favorites, and had individual rights: when the airplane majestically neared the house, the front door was opened to permit it to glide right in. The red car sometimes jumped on to the roof, to be fed by one of the two gasoline tanks stationed there. His remarks at home and his interest in his parents’ bodies (so usual for this inquisitive age) justify the interpretation that F played with the house as his fantasies played around his mother’s body. The little red car is fed by the two tanks just as F’s sister drinks from the mother’s breasts. The airplane enters the house from the front as his father’s erect penis enters the mother’s body. And his loading and unloading of trucks that like most children he has concluded that there are innumerable babies in the mother’s body and that they are born through the rectum, the orifice through which the contents of his own body pass.
One was reminded of Santayana’s recent description:
A boy at the age of five has a twentieth century mind; he wants something with springs and stops to be controlled by his little master-ego, so that the immense foreign force may seem all his own, and may carry him sky-high. For such a child, or such an adventurous mechanic, a mere shape or material fetish, like a doll, will never do; his pets and toys must be living things, obedient, responsive forces to be coaxed and led, and to offer a constant challenge to a constant victory. His instinct is masculine, perhaps a premonition of woman: yet he is not thinking of woman. Indeed, his women may refuse to satisfy his instinct for domination, because they share it; machines can be more exactly and more prodiciously obedient.4
II. Psychoanalysis Without Words
(ABSTRACT OF A CASE-HISTORY)
A little girl, G, two and one-half years old, had stopped looking and smiling at people and had ceased developing in her play. She had not learned to say a word or to communicate in any way with other children. Only occasionally, and then in connection with some tense, compulsively repeated play, did her pretty face lose its monotonous and melancholy expression. At such moments her excited sounds were strangely gutteral and were produced by noisy inhalations. No diagnosis meant much at this stage. The question was: Could one make contact with her at all? Could one reawaken her interest in this world?
Upon my first visit to her, one single fact induced me to make the trial. As she approached me slowly, coming down a stairway, she did not look at me directly but around me in concentric circles. She did not fail to see me, as had been supposed, but definitely avoided doing so.
My first subsequent observations revealed that her spells of excitement showed a mixture of pleasure and anxiety. I noticed this first during a spell which took place as she was banging a door, which in opening and closing touched a small chain that hung from an electric light. However, such “spells” could also occur when she was quiet. She would suddenly look out of the corners of her eyes at an extreme angle, focusing them far away, usually at the brightest point in the surroundings; then she would twist her hands almost convulsively and produce gutteral sounds, half like crying, half laughing.
She seemed never to have made any of the usual pre-language sounds; nor had she ever licked things as other children do, nor bitten anything. She would urinate only once in twelve or twenty-four hours, and often had bowel movements only once in forty-eight hours. Her room was overclean and her nurse seemed not without anxiety in regard to these matters.
When I heard this, and saw her exhibit the same excitement while simply throwing a ball again and again between a piano stool and a piano, I concluded that she had experienced training as a trauma, which in turn has been connected somehow with unknown traumata of her earlier life. I first tried to approach this symptom by suggestive play. Disregarding her, since she avoided looking at me, I threw stones into some old “potties” for almost an hour. When I then left, and observed her from a place where she could not see me, she played around these potties in concentric circles which grew narrower and narrower. Finally she dropped a stone in a potty, laughed heartily and loudly, and said clearly, “a-ba-ba-ba-ba.” During the succeeding days her toilet habits changed completely, whether as a result of this simple suggestion I do not know, but an immediate relief of general tension was obvious.
We then tried by mild suggestion to influence her playing and her playful movements in space. Not only had she fortified her position against the outer world by not looking at people, not listening, not eating unfamiliar food, and by holding back urine and feces, but she behaved on the whole as if something actually inhibited the movements of her body in space. Her legs and arms were tense and stiff, so much so that a neurological disturbance was suspected and she was examined, with no findings to indicate disease. Even when ample space was at her disposal, she seemed to imagine limits and boundaries where she stopped suddenly, as if confronted with a fence or an abyss. It was an imaginary noise at a certain distance upon which she then focused her attention with an expression half anxious, half delighted. I was interested to see at what limit freer play and freer physical movement would be stopped by a real anxiety or end in the manifest excitement described above. If she threw things, I would try to induce her to throw them further; I would take her hand to run with her, to jump down or to climb steps—always somewhat more quickly or extensively than she would dare to do alone.
While I attempted to help her expand the limits of her expression, it became obvious that there was a correlation between the functions of focusing on objects, grasping objects, aiming at things, biting into things, forming sounds, having sufficiently large bowel movements, and touching her genitals. The manifestation of increasing aggressiveness in one of these functions was accompanied by similar improvements in the others; but when a certain limit was reached, anxiety inhibited all of them. A sudden large defecation on the porch was followed by severe constipation and regression in all functions, and a “talking” spell of four hours one night, in which she seemed to be able to talk all the languages of Babel, but unable to single out English from the confusion, had the same effect.
The first word she suddenly used—pronouncing it quite clearly—showed that it had been right to assume an early traumatic experience. While banging a door she looked far away into the sky and exclaimed (obviously imitating an anxious adult, quite in the fashion of a parrot), “Oh dear, oh dear, oh dear.” On another occasion, she said clearly several times, “My goodness.” A few days later I saw her pick out of a potty numerous stones and blocks which smelled of paint, and lick them. When I softly said, “Oh dear, oh dear,” she vigorously threw the potty away, as if remembering a prohibition.
On the other hand, nothing could excite her more than having a bright, shining pinwheel moved quickly toward her face. I cannot report here all of the details of her play, which finally pointed to the following elements as possible aspects of a traumatic situation in her past: looking through bars (like those of a crib?); a light moving quickly toward her face; a light seen at a certain angle; a light seen far away; traumatic interference with licking and with play somehow connected with defecation. These corresponded to two of the definite
fears she had occasionally manifested, i.e., of a light in the bathroom and of a traffic light blinking some hundred feet away from her window. She had also been terrified by the fringes of the covers on her parents’ beds, a fear which seemed unconnected with this, until the chains of the lights which fascinated or frightened her proved to play an important role.
I then visited the hospital where she had been born. The most critical period of her short life had been its first few weeks, during which her mother had been too ill to nurse her for more than two days. The baby developed an almost fatal diarrhea. Not much was known about this period and her special nurse had left the country.
Another nurse, helping me to study the lights in the hospital, suddenly said, “And then we have another lamp which we only use with babies who have severe diarrhea.” She demonstrated the following procedure with its clear parallels to the child’s play behavior. The baby is laid on its side so that the lamp, which is put as near as possible to the baby’s sore buttocks, can shine directly on them. The baby then must see the lamp from approximately the angle which this child’s eyes always assume when she is preoccupied with her typical day-dream. The lamp has a holder which can be bent and the full light could then shine on the baby’s face for a moment as the lamp is being adjusted. When this has been done, the lamp is covered so that it is, so to speak, in the bed. For the baby, then, the light is where the pain is.
The discovery of this traumatic event from the second week of her life helped us to meet a situation which arose when the child suddenly became frightened of a lamp in my office, stopped drinking milk at home and began, wherever she was, to play at being in bed. She would build a kind of cave out of the cover of my couch, crawl into it, and, terrified but fascinated, would look towards the dangerous light. We began to play with lights. Since at the time she liked all things which could be spun around quickly, I would put a light underneath the cover, presumably where the hospital lamp had been, and would spin it around. She began to love lights, and when she smiled for the first time at the light that she had been afraid of, she said, “ma-ma-ma-ma.” At the same time her motor coordination improved so much that when the lamp above her bed had to be unscrewed because she played with it too much she could rock her bed across the room in the dark to pull another lamp chain.
At this point in the treatment the mother remembered another important part of the child’s earliest history. In the third month of the child’s life, when she had left the girl to take a trip, she had given instructions that an electric heater be turned on while diapers were being changed. After her return she was told that all through this month, dynamite had been used to blast rocks in the vicinity and had terrified the whole neighborhood. The baby, being upset already by the nervousness of the adults, had been further terrified when one day the electric heater suddenly exploded beside her. Here we have the connection between the light where the pain is and the light where the noise is. The flashing traffic light several hundred feet away, of which she consequently was afraid, apparently was a “condensation” of the exploding light near at hand and the terrifying noises at a distance.
After she had learned to play with lights without fear, we attempted to extend further the radius of her activities, and gave her hard toast in order to induce her to bite. She refused—and presently reacted with a show of fear on seeing a tassel hanging from the girdle of her mother’s dress. At the same time, she began to bite into wooden objects. Having observed in her a similar fear of a lamp chain (usually, as I pointed out, the object of traumatic play) directly after she had first seen two little boys naked, I inquired whether, and how much, she could have seen of her father’s and mother’s bodies. Her fear spread to all objects which had tassels or fringes or were furry or hairy, when they were worn by a person. When offered her mother’s belt to play with, she touched and finally took it between thumb and forefinger as if she were taking a living and detestable thing, and threw it away (with an expression much like that occasionally shown by women when they report a snake dream). When by playing with the fringe repeatedly, she had overcome her fear of it, she began staring down into the neck of her mother’s nightgown, focusing her fascinated attention on her breasts. When we add to these observations the recollection of how she had formerly looked in a concentric circle around people, supposedly not seeing anybody at all, we may reconstruct one more of the traumatic impressions which were probably factors in arresting her development. We may assume that as a small child when seeing her parents undressing on a beach, she had experienced a biting impulse toward the mother’s breasts and (a not uncommon displacement) the father’s penis.5 What this meant to her becomes clear when we remember the first two traumatic events we were able to uncover. The first had been the experience of intestinal and anal pain in association with light during the frustrated sucking period. The second was the experience of noise (the blasting) and exclaiming women (“Oh dear,” “My goodness”) in connection with the electric heater during the onset of the biting period. (Other material suggested that the nurse had exclaimed in a similar way when she once found the child playing with feces which she was about to put into her mouth.)
No doubt from the very outset this child had not been ready to master stimulations above a certain intensity. On the other hand, some meaning could be detected in her strange behavior and under the influence of our play and of simultaneous change of atmosphere in a now more enlightened environment, the child’s vocalizations approached more nearly the babble of a normal child before it speaks. She began to play happily and untiringly with her parents and to enjoy the presence of other children. She had fewer fears, and she developed skills. This newly acquired relationship to the object world, though a precondition of any reorientation, was, of course, only a beginning.
III. Pregenitality and Play
A. CLINICAL OBSERVATIONS
1.
In her article Ein Fall von Ebstörung6 [A Case of an Eating Disorder] Edith Sterba reports the case of a little girl who began to hold food in her mouth, after having been trained to release the feces which for an annoyingly long period she had preferred to retain in her rectum. This food she would turn around and around until it formed a ball, whereupon she would spit it out, thus using or rather misusing, the mouth to execute an act which had been inhibited at the anus.
A zone of the body with a specific muscular and nervous structure, the typical function of which is to accept, examine and prepare an incoming object for delivery to the inside of the body, is here used instead to hold for a while in a playful manner, and then return the object to the outside. This act resembles the anal act which it replaces only as a “gesture,” but without any functional logic. Such as “unnatural” use of a substituted zone is one form of what is called displacement. In this case it implies a partial regression, since the mouth precedes the anus in the erogenous zones sequence, and offers the specific tactual pleasure sought after at an earlier period. It is hard to understand psycho-physiologically that a zone can replace another zone of different neurological quality and location, and serve dramatically to represent its function. Psychoanalysts have accepted the interrelationship of these interchangeable zone-phenomena as being libido economical. Physiologists and psychologists in general are for the most part not even aware of the phenomena as a problem.
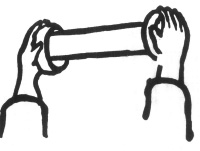
Figure 8
What interests us most in this connection is the relationship to play of such displacements from one organ to another. Most children, instead of displacing from one section of their own body to another, find objects in the toy world for their extrabodily displacements. If, in a moment of deep concentration in play, the dynamics of which are yet to be described, a child is not disturbed from within or without, he may use a cavity in a toy as a representative of a cavity in his own body, thus externalizing the entire dynamic relationship between the zone and its object.
Between displacements within the body (habits, symptoms) and the free external displacement in play, we find various arresting combinations. A little boy, H, two-and-one-half years of age, who struggled rather belatedly against enuresis, began to take to bed with him little boxes, which he held closed with both hands. When a box would open during the night, sometimes apparently with his unconscious help, he would cry out in his sleep, or awaken and call for someone to help him close the box. Then he would sleep peacefully, though not necessarily dry. But he continued to experiment. During the day he looked around for suitable boxes—obviously driven by an urge to materialize an image of “closedness.” Finally he found what seemed to fit the image: it was a cardboard cylinder which had been the center of a roll of toilet paper, and two cardboard caps from milk bottles, which he put over the openings of the roll. (See Figure 8.) All through the night he would try to hold this arrangement firmly together with both hands—as an animistic guardian of the retentive mode. But no sooner had his training achieved a relative success in closing his body during sleep, then he began, before going to sleep, to throw all available objects out of the window. When this was made impossible, he stole into other rooms and spilled the contents of boxes and bottles on the floor.
Clearly, the first act, namely, holding a closed box as a necessary condition for sleep, resembles a compulsive act originating in the child’s fear of being overpowered by his weakness to retain or his wish to expel. Emptying objects, on the other hand, or throwing them out of the window is “delinquent” and the result of the fear of being overpowered by the claims of society to which he surrenders the zone but not the impulse. The impulse begins an independent existence.
To prevent the little boy from throwing things out of the window, it was opened from the top. Thereupon he was found riding on it, leaning out into the night. I do not think he would have fallen out; he wanted only to show himself “master of openings,” as compensation for the surrender of the free use of his excretory openings to society. When, in consequence, his mother kept his window closed until he was asleep, he insisted that the door should be ajar. At an earlier stage, the same boy, as he was learning to control his bowel movements, had gone through a short period of excessive running away. Thus not only sections of one’s body and toys, but also the body as a whole in its spatial relationship to the whole room or to the whole house may serve the displaced impulse in various degrees of compulsive, naughty, or playful acts.
I may refer again to the wooden bowl which I mentioned on page 87 (see Figure 6). After a piece had been broken off, this bowl proved to be of manifold use to various children. They used it with deep concentration and with endless repetitions. As noted in page 79, A, curious and much restricted, turned it upside down to fill its hollow base and look at it; F, reassured about his phallic aggressiveness, used the opening, as thousands of boys at certain ages do, as a goal for his marbles; G, over-retentive, did not “retain” marbles in the bowl, but filled it again and again in order to spill them excitedly all over the floor. Similarly, a girl of three, who was fighting desperately against soiling herself, did not spill, but asked for the broken-off piece to close the bowl tightly, reminding us of the boy H with his animistic retention boxes. Thus we see the impulses appearing in play as the advance guard or rear guard of new sublimations.
It is conceivable that a form such as this bowl, as it is used by children of various age groups, could also prove of experimental value. We must keep in mind, however, that units of play behavior, like parts of dreams or single associations, seldom have independent meaning value. To know what a certain configuration in a child’s play means, we should know the contemporaneous changes in his growth, his habits, his character and his concepts of others.

Figure 9
2.
Let us look at an individual who showed pathological oscillation in the pregenital sphere, and let us place a specific bit of play in the center of our observational field.
At a certain period in his treatment, J, a boy of eight, untiringly repeated the following play: A caterpillar tractor slowly approached the rear end of a truck, the door of which had been opened. A dog had been placed on the tractor’s chain wheels in such a way that he was hurled into the truck at the moment the tractor bumped into it. (Figure 9.)
Symptom. In a very specific way, J had failed to respond to toilet training. Dry and clean when he wished to be, he had nevertheless continued to express resistance against his mother by frequent soiling (as much as three times a day), an act which became a perverted expression of his highly ambivalent feelings about the other sex. In school, when angered by certain girls by whom he would feel seduced, he would take their berets to the toilet and defecate into them. His masturbatory habit consisted in rubbing the lower part of his abdomen, which caused genital excitement at first, but ended in defecation.
First treatment. The psychiatrist who first treated the boy was amazed to find that he offered “unconscious” material of a sexual and anal nature in a never ending stream. As the naïve preconception in some child guidance clinics would express it, the boy was a real “Freudian” patient. But the psychiatrist was well aware of the fact that the patient did not really respond to the explanations for which he seemed to ask. This was probably due to the fact that in being voluble he did not communicate with the therapeutic agency in order to get cured, but cleverly “backed out” by regressing to a new kind of oral perversion in “talking about dirty things.”
Second treatment. When the boy’s masturbation increased, it had been thought necessary to circumcise him, under the assumption that it was a slight phimosis which, though stimulating him genitally, did not allow him to have a full erection and led his excitement into anal-erotic channels. Simultaneously, he was subjected to an encephalogram. Following this, the boy had stopped soiling entirely; but he also underwent a complete character change. He talked little, looked pale, and his intelligence seemed to regress—symptoms which are apt to be overlooked for some time because of the specific improvement in regard to a socially more annoying symptom. In this case, the closing up was nothing but a further regression, an outwardly more convenient but in fact more dangerous retreat into orality (as was also shown by his excessive eating) and into a generalization of the retentive impulse. In consequence, his behavior soon gave rise to grave concern, and when he was first referred to me, I was doubtful as to the therapeutic reliability of his ego, which either seemed to be no longer or perhaps never to have been secure.
Psychoanalytic treatment. The first barrier which psychoanalysis was forced to attack was the castration fear, which, after the circumcision, had suppressed his soiling without ridding him of the impulse. Expecting new physical deprivations, the boy would appear equipped with two pairs of eyeglasses on his nose, three knives on a chain hanging out of his trousers, and a half dozen pencils sticking out of his vest pocket. Alternately he was a “bad guy” or a cross policeman. He would settle down to quiet play only for a few moments, during which he would choose little objects (houses, trees and people) no larger than two or three inches high, and make covers for them out of red Plasticine. Suddenly he would get very pale and ask for permission to go to the bathroom. When consequently the circumcision was talked over and reassurances given for the more important remainder of his genitals, his play and cooperation became more steady.
His first drawing pictured a woman with some forms enlarged so as to represent large buttocks. In violent streaks he covered her with brown paint. It was not, however, until his castration fear had been traced to earlier experiences that he began to look better and to play with real contentment.
J had witnessed an automobile accident in which the chief damage was a flat tire. In describing this and similar incidents to me he almost fainted, as he had also done merely while enlarging and protecting the little toys with covers of Plasticine. In view of his anxiety, I pressed this point. He felt equally sick when I asked him about certain sleeping arrangements. It appeared that he had seen (in crowded quarters) a man perform intercourse with a woman who sat on him, and he had observed that the man’s penis looked shorter afterwards. His first impression had been that the woman, whose face seemed flushed, had defecated into the man’s umbilicus and had done some harm to his genitals. On second thought, however, he associated what he had seen with his observations on dogs, concluding that the man had, as it were, eliminated a part of his penis into the woman’s rectum out of which she later would deliver, i.e., again eliminate, the baby. His castration fear was traced to this experience, and the enlightenment given that semen and not a part of the penis remained in the woman.
First play. His first concentrated skillful and sustained play was with the tractor and the truck. At that moment I made no interpretation of it to him, but to me it indicated that he wanted to make sure by experimenting with his toys that the pleasant idea of something being thrown into another body without hurting either the giver or the receiver was sensible and workable. At the same time, his eliminative as well as his intrusive impulses helped him in arranging the experiment. Finally he showed that his unresolved anal fixation (no doubt in cooperation with certain common “animalistic” tendencies and observations) did not allow him to conceive of intrusion in any other way than from behind. From his smearing of the woman’s picture with brown paint to this game, he had advanced one step: it was not as before brown stuff or mud which was thrown into the truck, it was something living.
Technical consideration. Melanie Klein, in her arresting and disturbing book The Psychoanalysis of Children has given the significance of an independent, symbolical unit to the fact that in a child’s play motor cars may represent human bodies doing something to one another. Whether or not this is unreservedly true in its exclusively sexual interpretation has become a matter of controversy. Probably the question cannot be given any stereotyped answer. Symbolism is dangerous because it distracts attention from the imponderables of interpretation. No doubt, any group of mechanical objects, such as radiators, elevators, toilet and water systems, motor cars, and so on, which are inanimate but make strange noises, have openings to incorporate, to retain, and to eliminate, and finally are able to move rapidly and recklessly, constitutes a world well suited to symbolize one of the early concepts which the child has of his body as he develops the agencies of self-observation and self-criticism. Encountering in himself a system of incalculable and truly “unspeakable” forces, the child seeks a counterpart for his inner experience in the unverbalized world of mechanisms and mute organisms. As projections of a being which is absorbed in the experiences of growth, differentiation, and objectivation, they are not as yet systematically described. Their psychological importance certainly goes beyond sexual symbolism in its narrower sense.
Likewise, play is much too basic a function in human and animal life to be regarded merely as an infantile substitute for the verbal manifestations of an adult. Therefore one cannot offer any stereotyped advice as to the form or time when interpretations of play are to be given to a child. This will depend entirely on the role of play at the specific age and in the specific stage of each child patient. In general, a child who is playing with concentration should be left undisturbed as long as his own anxiety allows him to develop his ideas—but no longer. On the other hand, some children, becoming aware of our interest in play, use this to lead us astray and away from quite conscious realities which should be verbalized. We are not in possession of a theory embracing the dynamics of play and verbalization for different ages in childhood. We do not want to make the child conscious of the fact that play as such means something, but only that his fears, his inability to play playfully, may mean something. In order to do this, it is almost never advisable to show to the child that any one element in his play “means” a certain factor in his life. It is enough after one has drawn one’s own conclusions from the observation of play, to begin to talk with the child about the critical point in his life situation—in a language the sense of which is concrete to a child at a specific age. If one is on the right track, the child’s behavior (through certain positive and negative attitudes not discussed here) will lead the way as far as it is safe. No stereotyped imagery should lure us beyond this point.
Return of the impulse. Outside the play hours, the eliminative impulse typically made its reappearance in J’s life in macrocosmic7 fashion and at the periphery of the life space: the whole house, the whole body, the whole world were used for the representation of an impulse which did not yet dare to return to its zone of origin. In his sleep, he would start to throw the belongings of other people, and only theirs, out of the window. Then, in the daytime, he threw stones into neighbors’ houses and mud against passing cars. Soon he deposited feces, well wrapped, on the porch of a hated woman neighbor. When these acts were punished, he turned violently against himself. For days he would run away, coming back covered with dirt, oblivious of time and space. He still did not soil, but desperation and the need for elimination became so all powerful that he seemed to eliminate himself by wild walks without any goal, coming back so covered with mud that it was clear he must have undressed and rolled in it. Another time he rolled in poison ivy and became covered with the rash.
Resistance. When he noticed that, by a slowly narrowing network of interpretations, I wanted to put into words those of his impulses which he feared most, namely, elimination and intrusion in their relationship to his mother, he grew pale and resistive. The day I told him that I had the impression there was much to say about his training at home, he began a four-day period of fecal retention, stopped talking and playing, and stole excessively, hiding the objects. As all patients do, he felt rightly that verbalization means detachment and resignation: He did not dare to do the manifest, but he did not want to give up the latent.
Return of symptom. He did not live at home at this time. After many weeks, he received the first letter from his mother. Retiring to his room, he shrank physically and mentally, and soiled himself. For a while he did this regularly whenever his mother communicated with him.8 It was then possible to interpret to him his ambivalent love for his mother, the problems of his bowel training, and his theories concerning his parents’ bodies. It was here also that his first free flow of memories and associations appeared, allowing us to verbalize much that had been dangerous only because it had been amorphous. Interestingly enough, after the patient understood the whole significance of the eliminative problem in his life, the eliminative impulse, in returning to its zone did not flood, as it were, the other zones. Verbalization did not degenerate to “elimination of dirt” this time, as in the previous psychiatric treatment.
Sublimation. One day he suddenly expressed the wish to make a poem. If there ever was a child who, in his make-up and behavior, did not lead one to expect an aesthetic impulse, it was J.9 Nevertheless, in a flood of words, produced during an excitement similar to that which had been noticeable when he had talked about dirt to the psychiatrist, he now began to dictate song after song about beautiful things. Then he proposed the idea, which he almost shrieked, of sending these poems to his mother. The act of producing and writing these poems, of putting them into envelopes and into the mailbox, fascinated him for weeks. He gave something to his mother and it was beautiful! The intense emotional interest in this new medium of expression and the general change in habits accompanying it indicate that by means of this act of sending something beautiful to his mother, part of that libido which had participated in the acts of retaining feces from women and eliminating dirt to punish them had achieved sublimation. The impulse had found a higher level of expression: the zone submitted to training.
3.
In part 1 page 94, I gave an example of what different children may do with one toy; in part 2, an example of the therapeutic significance of one play-event in a child’s life. I would like to add a word about a child’s behavior with different play-media:
A child playing by himself may find amusement in the play world of his own body—his fingers, his toes, his voice, constituting the periphery of a world which is self-sufficient in the mutual enchantment of its parts. Let us call this most primitive form of play auto-cosmic. Gradually objects which are close at hand are included, and their laws taken into account.
If, at another stage, the child weaves fantasies around the reality of objects, he may construct a small toy world which is dominated by the laws of his own growing body and mind. Thus, he makes blocks “grow” by placing them on top of one another; and, with obvious pleasurable excitement in repetition he knocks them down, thus externalizing the trauma of his own falls. Later the blocks may serve as the building stones for a miniature world in which an ever increasing number of bodily, mental and social experiences are externalized and dramatized. This manifestation we may call microcosmic play.
We can term macrocosmic that form of play in which the child moves as in a kind of trance among life-sized objects, pretending that they are whatever background he needs for his imagination. Thus he manifests his need for omnipotence in a material which all too often is rudely claimed by adults, because it has other, “grown-up” purposes.
These are a few of the more basic types of play which the child offers to us for comparison—each with its special kind of infantile fascination—developing one after the other as he grows and then shifting more or less freely from one to the other at certain stages.
Following an exceptional sequence of disappointments and frustrations, a girl of eight, K, a patient of Dr. Florence Clothier of Boston, made a veritable fortress of herself. Stubborn, stiff, uncommunicative, she would occasionally open all the orifices of her body, and annoy her environment by spitting, wetting, soiling, and passing flatus. One received the impression that these symptoms were not only animistic acts by which she eliminated hated intruders (her stepmother and her stepbrother) but also “shooting” with all available ammunition. While polymorphous in their zonal expression, these acts were clearly dominated by a combination of the eliminative and intrusive impulses. As the main object of the destructive part of this impulse, one could recognize the stepmother’s body, in which the child suspected that more rival stepbrothers were growing. Naturally, this wild little girl was at the same time most anxious to find for herself a good mother’s body in which to hide, to cry, and to sleep. Someone had told her that her own mother had died while giving birth to her; and one can imagine what conflicts arose when she first met the psychiatrist and saw that this potentially new and better mother was actually pregnant.
These biographic data are enough to explain the play which I am going to describe. Nevertheless, there is nothing essentially atypical in this play. This girl’s constitution and experience simply made dominant the problem of intrusion which every child faces at least in one period of his life, namely, in the phallic period.
The phallic phase, last of the ambivalent stages, leads the child into a maze of “claustrum” fantasies, in which some children—for a longer or shorter time—get hopelessly lost.10 They want to touch, enter and know the secrets of all interiors but are frightened of dark rooms and dreams of jails and tombs. As they flee the claustrum they would like to hide in mother’s arms; fleeing their own disturbing impulses toward the mother’s body they escape into willful acts of displaced violence, only to be restricted and “jailed” again. The mother’s body, into which the baby wanted to retreat in order to find food, rest, sleep, and protection from the dangerous world, becomes in the phallic phase the dangerous world, the very object and symbol of aggressive conquest. Further obstructing this conquest are the father’s rights (because of his strength) and the younger siblings’ rights (because of their weakness); and thus the mother, a heaven and hell at the same time, becomes the center of a hopeless rivalry. Whether to go forward or backward, to be hero or baby—that is the question. It is in this phase that the boy, knowing there is no way back, sets his face towards the future (where all those ideals are waiting for him, which we symbolize by superhuman mother figures); while to the girl, her own body’s claustrum offers a vague promise and new dangers.
In his play, the boy at this stage prefers games of war and crime, and expresses most emphatically the intrusive mode; the girl, by contrast, in caring for dolls, in building a small house with a toy baby or a toy animal in it or in other protective configurations expresses the procreative-protective tendency which will remain the point of reference for whatever course she may take in her future.
Dr. Clothier’s patient, in her play during a period of transition from eliminative-intrusive to female tendencies, showed many distorted manifestations of these problems:
In cutting her own hair and eyelashes, and threatening to cut her eyes and teeth, she approximated a return into the autocosmic sphere of play.
Microcosmic: (1) Dramatic: Five dolls, named after father, stepmother, stepbrother, sister and herself are approached from behind by a snake who eats everybody except herself and her pet animal.
(2) Pictorial: Drawings with long rows of houses which are being approached, entered, and left by a stealing cat: The house more and more assumed the appearance of the human body, with the two sides of the walk leading to it representing the legs between which the door was entered by the cat. The girl noticed this resemblance herself and made the giggling remark, “Do you think that a house can stand on the walk?”
Macrocosmic: (1) For several days she built “houses.” The entrance had two round portal forms represented by a dish on each side. The patient began going in and out of the house on all fours, always entering the house backwards. When inside, she picked up one of the dishes and pretended to drink from it; then she curled up in a fetal position. Crawling backwards over and over again, she said to the psychiatrist, “You watch and tell me so I won’t hit the back of the house.” The psychiatrist told her when to stop, but each time she gave a vicious lunge backwards, breaking through the wall.
(2) Where her macrocosmic play expanded beyond the sphere of toys, i.e., became naughty, she climbed on tables, desks and shelves, invaded drawers, and tore papers. Often only bursting in and out of the room was an act big enough to express her intrusive rage.
(3) At a decisive point in her treatment, the girl was especially fascinated by a rubber syringe with which she squirted water everywhere. “Now I’m a wild Indian, so look out!” On a certain day, during a period of a general change in attitude, the girl squirted on the floor a big circle with one line representing a radius  ; then she angrily made a puddle out of her design. The next day she repeated the same configuration, but added a small circle in the center of the big one:
; then she angrily made a puddle out of her design. The next day she repeated the same configuration, but added a small circle in the center of the big one:  On the third day, she again drew a larger circle and, without the connecting radius, a smaller circle in the center, saying, “This is a baby circle.”
On the third day, she again drew a larger circle and, without the connecting radius, a smaller circle in the center, saying, “This is a baby circle.”  This time she did not destroy the figure, but said giggling, “There are no cats here” (to enter the circle and steal the baby). The change of configurations in this play from phallic (syringe) to female-protective is obvious. Moreover the little girl created a symbol and in doing so seemed to have a moment of clarity and pacification.
This time she did not destroy the figure, but said giggling, “There are no cats here” (to enter the circle and steal the baby). The change of configurations in this play from phallic (syringe) to female-protective is obvious. Moreover the little girl created a symbol and in doing so seemed to have a moment of clarity and pacification.
(4) Around the same time she dictated the following story to a teacher. She said she had heard it somewhere. We add it as an association which in a narrative and quite humorous form seemed to express symbolically an acceptance of the difference between boys and girls:
The Pumpkin and the Cat: The farmer put the pumpkin in the barn, and the cat came, and the cat said to the pumpkin, “Do you want to stay here? Let’s go away.” And the pumpkin rolled and tumbled, and the cat walked and walked, until it began to rain. The cat lifted up his wet paw. A woodcutter came by. The pumpkin said, “Mister, will you please cut my top off, and scrape all the seeds out, so the cat can come in?” The woodcutter cut off the top of the pumpkin and scraped all the seeds out.
They went on tumbling and rolling until morning. They started off again, tumbling and rolling. Then pretty soon it was night. And it began to rain harder, and the cat lifted up his wet paw, and the pumpkin said, “You’d better get inside.” “Yes, but we haven’t got any two windows and a nose and a mouth.” The pumpkin said, “You get out and I’ll go to the carpenter.” He went to the carpenter and said, “Mr. Carpenter, will you please cut two windows and a nose and mouth?”
The cat came in the pumpkin and the pumpkin and the cat laughed. Then they rolled and tumbled, until they came to a little house. They heard a boy whistling and then a girl came out of the house and said, “What do you wish you had most for Halloween?” The boy said: “I wish I had a nice round pumpkin,” and the girl said, “I wish I had a nice little black cat.”
Up rolled the pumpkin to the little boy, and the girl said, “Look what the fairy brought us, and I think it’s a cat inside!”
And off jumped the cover, and out jumped the little black cat, and right into the little girl’s arms.
And they lighted the pumpkin, and put it on the table, and put the kitty next to it, until the mother came home.
B. ZONES, IMPULSES, MODES
It is not only in pathological cases that children’s acts impress us as being unexpected and apparently incoherent. The observer of any child’s life feels at moments that an essential factor is eluding him, as the loon in the lake eludes the hunter by sudden turns under the surface. Whether the child is playful, naughty or compulsive; whether his acts involve bodily functions or toys, person or abstracts, only analytic comparison reveals that what so suddenly appears in one category is essentially related to that which disappeared in another. Sometimes it is the mere replacement in time which makes the analyst become aware of the inner connection of two acts; sometimes it is a quality of an emotion or a tendency of a drive common to both. Often, however, (and this is especially true for the period of pregenitality on which we focus our attention here) the only observational link between two acts is what we wish to describe as the organmode.11
To clear the way for more systematic observations of the interrelationship between the intrabodily and extrabodily aspects of pre-genitality, it seems best to reduce the displaced impulses to the simplest spatial terms, i.e., to signs which represent the dynamic principle of the body apertures in which the impulses are first centered. I propose that we accept the sign  as representing the incorporation of an object by means of sucking.
as representing the incorporation of an object by means of sucking.  may represent the incorporation by means of biting;
may represent the incorporation by means of biting;  the retaining of or closing up against an object;
the retaining of or closing up against an object;  expelling and
expelling and  intruding.
intruding.
The organ-modes, then, are common spatial modalities peculiar to the appearance of pregenital impulses throughout their range of manifestation; whether gratification is experienced in the elimination of waste product by a body aperture, by the spilling of a bottle’s content, by throwing objects out of a window, or pushing a person out of one’s physical sphere, we recognize the mode of elimination as the common descriptive characterization of all these acts, and conclude that we are confronted with interchangeable manifestations of what was originally the impulse of elimination.
Surveying the field of these manifestations, one finds that what Freud has described as pregenitality is the development through a succession of narcissistic organ cathexes of impulses which represent all the possible relationships of a body and an object. Pregenitality not only teaches all the patterns of emotional relationship but also offers all the spatial modalities of experience. Led by pregenital impulses (or confused by them as the case may be) children experiment more or less playfully in space with all the possible relationships of one object to another one and of the body as a whole to space.
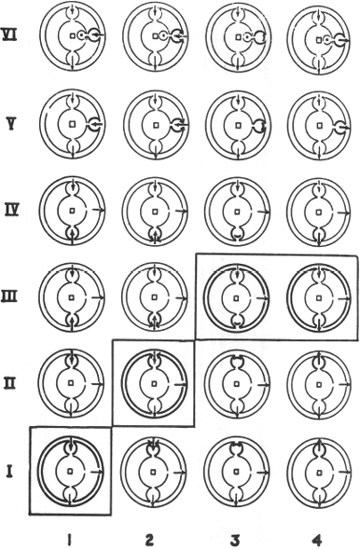
For didactic purposes, I have arranged the modes in a chart of pregenitality which (in formulation without words) indicates the network of original interrelationships of zones and impulses. This chart has been helpful in observation and teaching when used as a shortcut, leading to but by no means avoiding the knowledge of the other components of pregenitality.
Nobody who works in the field of human behavior can be unaware of the dangers of or blind to the necessity for such tentative systematization.

The chart is composed of single diagrams which represent the human organism in the successive stages of emphasis on certain erotogenic zones in pregenitality. I 1, for example, like all the other diagrams, consists of three concentric circles which represent three primitive aspects of the life of any organism: a the inner surface, b the outer surface, and c the sphere of outward behavior. The bodily impulses are represented in the diagram where certain organs connect the outer world with the inner surface of the body, respectively, 1 the oral-facial, 2 anal-urethral, and 3 genitalurethral zones.12
In each diagram one impulse is represented as being dominant by means of a heavier line; in I 1 it is the first (“sucking”) mode in the oral system. Thus we indicate that we are concerned with that stage of development in which the libido is concentrated mainly in the oral system and serves normally to develop this impulse. Also the circle which represents the surface of the body is more heavily outlined, as is true for all corresponding circles in the diagrams which lie on the diagonal. This indicates that the principle of receptive incorporation legitimately dominates the whole “surface of the body” during the first oral stage. Skin and senses are ready to “drink in” all kinds of perceptual sensations as brought to them by the environment and to enjoy libidinally all kinds of touching, stroking, rocking sensations if they are only kept below the threshold at which motor response would be provoked. The heavy outlining of the outer circle indicates that at this stage social behavior also expresses expectant readiness to receive, as is obvious in the rhythm of waiting, crying, drinking, sleeping. Reactions to stimuli which require more than the holding on with mouth and hands to what has been offered by the environment remain diffuse and uncoordinated. All of this—degree of coordination, muscle and sense development, libido distribution and spontaneous behavior—will have to be represented in a final formulation of the first bodily manifestation of our impulse.
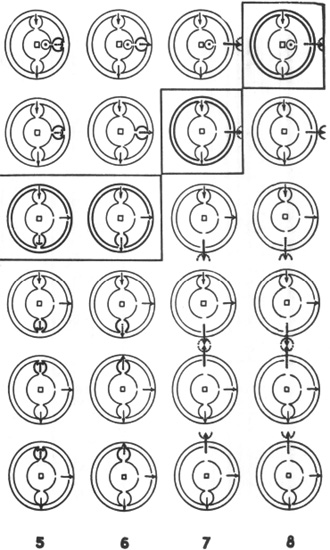

In II 2, the dominating impulse is  The biting system (gums, jaws, neck, etc.) is in the possession of a relatively high amount of libido and of muscle energy which, at the same time, is manifest throughout the spheres of perception and action; the eyes learn to focus, the ears to locate, the hands to reach out, and the arms to hold. The coordination of the system necessary for reaching out to an object and the “plucking” of it for oral incorporation is established. Simultaneously, a change in the concept of the outer world probably occurs. This is represented by the dotted arrow, which indicates that the incoming object is conceived of in a somewhat different way from formerly. The object of libidinal interest and of psychobiological training is now the food. Later it will be feces and then the genitals. Presumably each is first conceived of by the infant as belonging inherently to his own body and subject to his own will, during the first stages of the development of each zone (I 1, III 3, 4, V 6). It is only through a sum of psycho-biological and cultural experiences that the child learns that these objects belong to the environment—an expulsion from the paradise of omnipotence which takes place in the transition from the first (I, III, V) to the second (II, IV, VI) part of each stage. If we say psychobiological and cultural influences, we mean for orality that the changing conditions of the gums and the irresistible biting impulse, no less than the changing character of the food and of its delivery, participate in this expulsion into a world where “in the sweat of thy face thou shalt eat bread till thou return under the ground.”
The biting system (gums, jaws, neck, etc.) is in the possession of a relatively high amount of libido and of muscle energy which, at the same time, is manifest throughout the spheres of perception and action; the eyes learn to focus, the ears to locate, the hands to reach out, and the arms to hold. The coordination of the system necessary for reaching out to an object and the “plucking” of it for oral incorporation is established. Simultaneously, a change in the concept of the outer world probably occurs. This is represented by the dotted arrow, which indicates that the incoming object is conceived of in a somewhat different way from formerly. The object of libidinal interest and of psychobiological training is now the food. Later it will be feces and then the genitals. Presumably each is first conceived of by the infant as belonging inherently to his own body and subject to his own will, during the first stages of the development of each zone (I 1, III 3, 4, V 6). It is only through a sum of psycho-biological and cultural experiences that the child learns that these objects belong to the environment—an expulsion from the paradise of omnipotence which takes place in the transition from the first (I, III, V) to the second (II, IV, VI) part of each stage. If we say psychobiological and cultural influences, we mean for orality that the changing conditions of the gums and the irresistible biting impulse, no less than the changing character of the food and of its delivery, participate in this expulsion into a world where “in the sweat of thy face thou shalt eat bread till thou return under the ground.”
It is to be regretted that for the sake of orderly procedure we have to begin with the lower left corner of our chart which justly should be kept as vague as our knowledge of these stages of development is dark. But a principle of description to be used throughout the chart may be explained here: The normal succession of stages is represented in the diagrams on the diagonal. It is in these stages that impulse and zone find the full training of their function within the framework of growth and maturation. A deviation from the normal diagonal development can be horizontal, i.e., progressing to the impulse of the next stage before the whole organism has integrated the first stage; or, it can be vertical i.e., insisting on the impulse of the first stage when the organism as a whole would be ready for the training and integration of the dynamic principle of the next stage. Thus, a differentiation of zones and impulses is introduced which gives our chart its two dimensions: in the horizontal we have different impulses connected with one and the same zone; in the vertical we see one and the same impulse connected with different zones.
The stages, as well as their functional characteristics, are, of course, overlapping. The libido, during and after the stages of concentration shown in 11, and II 2, becomes concentrated in the excretory system, can be pleasurably gratified by the retention and expulsion of the (now more solid) feces, while, or perhaps just because, the general impulses dominating the rapidly developing sensory and muscular behavior are retaining and expelling. Unlike the previous stages, when incorporation at any cost seemed the rule of behavior, now strong, sometimes “unreasonable,” discrimination takes place: sensations are in rapid succession accepted, rejected; objects are clung to stubbornly or thrown away violently; or persons are obstinately demanded or pushed away angrily—tendencies which under the influence of educational factors easily develop into temporary or lasting extremes of self-insistent behavior, maintaining a narcissistic paradise of self-assertive discriminations. The sad truth to be learned in the anal stage and added to the experience of oral phase (which was: “You shall not find pleasure in incorporation except under certain conditions”) is: “In your body, your self, your mind, your room, you shall find pleasure in retaining or expelling only under certain conditions.”
Thus, the diagonal of the chart indicates and draws up for formulation some normal stages of development, in which certain zones are normally libidinized, certain impulses normally generalized. Where the outer circles are not heavily outlined (in the non-diagonal remainder of the chart) those configurations of impulses can be found which at the particular stage become dominant and generalized only when an abnormal situation arises; though as integrated part tendencies all the impulses are essential for all the zones of a living organism at all times. Wherever a specific case suggests it, the chart might be used to illustrate abnormal correlations by interchanging impulses and by outlining more heavily any untimely generalization of an impulse.
To use the example with which we started: Dr. Sterba’s little patient having learned to exchange IV 5, 6 (anal retaining and releasing in accordance with the wishes of the environment) for III 3, 4 (insistence on her own jurisdiction in matters of elimination) managed to keep impulse 3 by partial regression to II 3 and 4 (oral retaining and expelling)—impulses which, of course, are normally developed during the oral phase (closing up against, spitting out of food) but become dominant later only through regression as in this case, or as a result of fixation and retardation—as for example in Case F, where a traumatic combination of constitutional and environmental circumstances had brought about a general “closing up” of body and mind.
In the case of J, we saw the pathological oscillation of the untrained impulses of an eight-year-old boy in the maze of channels which once and for all are established by the experiences of pregenitality: Trained to the toilet without, however, having allowed this training ever to dominate his psychobiological development and add to his character the traits which are the outcome of having passed through this stage (as would be indicated by IV 5 and IV 6), he used defecation as a means of expression of an asocial, omnipotent attitude (III 3—III 4). His fantasy of intruding by means of defecating into an object belonging to an ambivalently loved person would be represented by III 7. When talking about dirty things to the psychiatrist, he expanded impulse 4 over to the oral sphere (II 4) only to refuse all communication (II 3) as soon as the treatment appeared to him to be a punishment. We saw how under treatment the impulse of elimination returned to its original zone and was subliminated. Case K prepared us for a consideration of the phallic phase.

The last two diagrams at the upper end of the diagonal are characterized by the dominance of the tendency to intrude. The general impulse to enter and to do something to another body or to another body’s sphere of influence, although existing since earliest orality, is now emphasized and made into a social problem by the rapid development of sense-curiosity and motor-development and the phallic-clitoric erogeneity with its dangerous adherence to incestuous atavisms. Psychobiological emphasis and the forces of education work together at this stage to add another set of sad truths, again leaving it to the child’s ego organization to make the best of it: “Not only the inner and outer surface of one’s body and the zones connecting inside and outside are under foreign jurisdiction, but also those forces and organs which single out and seek fascinating objects in the environment in an ecstasy of action.” “You may have the pleasure of touching and entering and finding out only under certain conditions.”

Girls, as we know, have a shorter or longer period of phallic tendencies (with clitoral erogeneity and the fantasy of having or achieving a penis) corresponding to the general development of the intrusive impulse. The question of when and in what way this phase is passed through and overcome, has aroused much controversy in psychoanalysis. Here, too, direct observation of play might prove a via regia. It seems certain that the penis-wish is absorbed more or less completely by the wish for a baby. The girl, following her destiny, which is to libidinize, develop and train a second organ system of incorporation with her procreative organs as its center, can be said to undergo a partial regression to the generalized sensitivity and receptive behavior first manifested during the oral stages. Thus in the last line of the chart we tentatively characterize female destiny by adding a procreative-protective impulse to the impulse of self-preservation “inside the body.” Whenever the chart is used for a female subject or patient, this impulse should be outlined more heavily and generalized in order to give zones and impulses, as well as the surface of the body and the motor sphere, a new specifically female-procreative correlation.13 It is this correlation which differentiates the female tendency to incorporate from sexual passivity in men.
The integration of all the vital impulses is essential and indispensible to physical, psychic and mental self-preservation and for social and sexual intercourse. Whatever one does, it is essential that one be able to accept, to keep, to digest and to eliminate; to give and to receive; to take and to be taken in fair ratio. We find that the under-or over-development of one impulse decisively changes the organization of all the others and creates a more or less pathological “type of personality.” There are “suckers,” “biters,” “retainers,” “expellers,” and “intruders” in all fields of human life. One could say that without them there would not be so many various “fields” in life. And there are types of personality which suffer from impotence in one or more of these impulses. As the Arapesh says: “There are those whose ears are open and whose throats are open; those whose ears are open and whose throats are shut; those whose ears are shut and whose throats are open; and those whose ears and throats are both shut.”14
The schematization of which we have been guilty might find an excuse in the fact that its aim is to help organize not only very simple infantile acts, but also the most primitive concepts the child has of his own organism, and the theories and expectations he develops in projecting his concepts onto others. Here, as we know, the origin of some typical dreams and fears may be found, such as being swallowed or robbed (by “suckers” and “biters”), being jailed and bound (by “retainers”), driven away and banished (by “expellers”), stabbed and raped (by “intruders”).
This, then, is the system of zones and impulses which form the organic basis for the normal or irregular appearance of configurations such as those described in connection with G’s, J’s and K’s auto-cosmic, microcosmic and macrocosmic behavior. The impulses are developed and, as it were, trained at their zones of origin during the (overlapping) stages of child development characterized by the general tendency to incorporation (oral-respiratory, nutritional, sensory-tactual), retentive-eliminative discrimination (muscular, anal-urethal), and intrusion (motor, phallic-urethral). In the course of phylogenetic and ontogenetic development the organ-modes are estranged (because overdue or precocious) from their original zones and can be observed as seeking new manifestations: the organism offers a limited range of safe displacements in habits and minor symptoms; reality allows for certain systems of projections; society accepts the expression through action of a number of character traits. The world of play affords opportunity to experiment with organ-modes in extra-bodily arrangements which are physiologically safe, socially permissible, physically workable and psychologically satisfying.
IV. Play Constructions of College Students*
Interest in the psychology of play ranges from the first playful movements of the baby to the various manifestations of the need for play in adults. Taking the most fascinating extremes of “play,” that of the child on the one hand and the productions of the artist on the other, we find that in spite of the testimony of language popular opinion tends to evaluate them as antithetical phenomena, finding no “sense” in children’s play, while looking at the artist’s play as a phenomenon burdened—and in modern times, overburdened—with conscious problems and meanings.
When the writer undertook to participate in the studies of the Harvard Psychological Clinic on the development and character-formation of a group of average young college men his interest in the psychology of play led him to place these subjects in a play situation in order to observe what their late adolescent imaginations would do with it.
DESCRIPTION OF THE PROCEDURE
Each subject was brought into a room in which there was a table covered with small toys. He was told that the observer (who was unknown to him) was interested in ideas for movie plays, and wished him to use these toys to construct on a second table a dramatic scene. After answering a few typical questions (i.e., “Do I have to use all the toys?”), the observer left the room for fifteen minutes, but watched the behavior of the subject through a one-way mirror. In the following pages these first observations, made while the subject believed that he was unobserved, are referred to as the Preparatory Period. After fifteen minutes the observer reentered the room, wrote down the subject’s explanations and sketched the scene (referred to as the Dramatic Scene).
Some of the toys were provided in large numbers, e.g., farmers, animals, furniture, automobiles, and blocks. To most of the subjects the principal toys suggested a family, consisting of father, mother, son, daughter, and a little girl. In addition, there was a maid and a policeman. It may be added that these toys were chosen without deliberate purpose according to what was available at the nearest toy store.
RESULTS
Five out of 22 subjects ignored the instructions and on the observer’s return greeted him in a friendly way with some such remark as, “Everything quiet! Just a nice, harmonious, country scene!” Of the remaining seventeen subjects, only 4 constructed dramatic scenes which were not automobile accidents, while 13 subjects put in the center either an automobile accident or an arrangement which prevented one. Nine times in these scenes the little girl was the object of danger or the victim of an accident, other female toys twice. In other parts of these same scenes 7 female toys died, fainted, were kidnapped or were bitten by a dog. In all, 18 female toys (the little girl 10 times) and no male figures were in danger or perished, a theme which can be called the typical fantasy of the average member of the group. On the other hand, in the construction of the subject who could be classified as the most masculine and socially best adapted member, a dog was the victim of an accident. The red racer with its not specifically named driver came to grief in the constructions of the two subjects who respectively came nearest to manifest homosexuality and to manifest psychosis.
INTERPRETATION OF RESULTS
The examples to be given in this report will illustrate a few hypotheses which follow from the analysis of the results.
They suggest first that the five friendly subjects had not failed to understand the instructions but that they could not construct a dramatic scene, because they had to suppress their first (most probably unconscious) response which corresponded to some traumatic childhood event (or to a screen memory which embraced a number of traumatic childhood experiences).
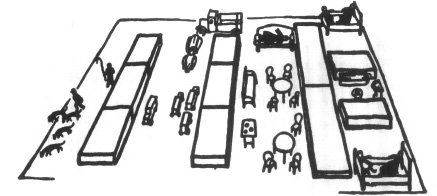
Figure 10
On the other hand, in most of the scenes which dared to be dramatic, traumatic childhood memories appeared either in the Preparation Time or in the Dramatic Scene—in the form of some characteristic symbolic fantasy, usually of an accident in which the little girl, rarely one of the other female figures, was the victim.
The constructed scenes will, of course, be the central object of our analytic efforts. We use as associative material whatever the subject said or did before or just after the construction of his scene, which seemed to be related in content or form specifically to what he did or said in other interviews and experiments.15 This specificity was taken as the basis for interpretation only after it had been established in conference with other observers.16
I. M: Zeeno
1. Preparatory Period. The first toy that Zeeno touched was one of the twin beds. He set it at the extreme edge of the table beyond the edge of the sheet of paper. He did the same with the other twin bed on the opposite edge so that they were as far away as possible from each other. (Figure 10.) Next he placed a wall which separated a couch from the beds. Then the bathroom was constructed and separated; the kitchen followed but was given no wall; neither had the house as such any surrounding walls.
Next he took, as the first toy person, the maid. Here, Zeeno was doubtful for a time—put the toy back and in a nervous manner touched the region of his penis. He looked around the room with a worried expression, then shifted to a street scene. First he placed the cars (the red racer and the green truck) and then outlined the street (just as in the house scene he had first placed the furniture and then built the walls of the rooms). Now he seemed able suddenly to continue more rapidly, obviously lost in that concentration characteristic of undisturbed play. He placed other cars in more rapid succession, then put people quickly and decisively at certain places, keeping males separate from females, and the daughter from the rest of the family.
2. The Dramatic Scene. When the observer entered the room, Zeeno exclaimed, “There is not enough space in this house,” and added quickly and anxiously, as if he did not believe himself, “Shall I tell you why the son and the father sleep in one bed? Because the mother, of course, has to be near the kitchen, and the daughter sleeps in the dining room because the maid has to be near the kitchen, too. The green truck drives on the highway and the red racer has to stop suddenly. Here [pointing to the extreme left of the scene] is a fisherman. He is disturbed by a man with his four dogs who is looking for a lost lamb.”
3. The manifest content of this use of the play material raises several analytic questions: Where is the dramatic scene which the subject was asked to construct? In the house everybody is asleep. Furthermore only those walls are built which separate people—not the outer walls which make a house and a home. The need to keep things separate is paramount: bed, wall, couch, wall; men, women, their positions only weakly rationalized. In the street a collision is prevented—a dubious dramatic element. Likewise the scene at the left at most only implies a drama, i.e., a lamb has been lost—an accident in the past, not a dramatic scene in the present. What is it that has to be separated and why? What does the subject’s childhood memories suggest in regard to these ideas?
The biography calls our attention to the following event: “Zeeno used to sleep in the same room with a sister who died. . . . She died about three o’clock in the morning before the doctor arrived.” He remembers “lying in bed not particularly concerned about this.” Nevertheless the examiner to whom the subject tells this story reports that: “He has a little anxiety about this. He was silent for some time afterwards.”
From dream interpretations we know that the dream often disguises the sleeper’s deep inner participation in a scene by having him see himself as a “not particularly concerned” onlooker. The psychoanalyst of children can add to this well-confirmed interpretation the actual experience of having seen children accept a traumatic experience, especially the death of a relative, with complete calm, although every detail of a later neurosis may indicate the pathogenic importance of this same event. It is possible that a feeling of guilt may torment Zeeno in connection with this death, about which he denies any natural anxiety. Children who mourn in this “invisible” way are often deeply concerned with the idea that some aggressive or sexual act or wish of their own might have been the cause of the death of the ambivalently loved person.
Several times during the various interviews Zeeno voiced thoughts of death. When, in the conference, he was asked of what he was most afraid, Zeno answered, “That I am not going to live terribly long.” To one of the ink blots he said, “I immediately think of a skeleton and ribs, and on each side above I see two faces looking at each other, guarding these ribs with an austere expression, like twins”—a detail which may be significant in considering the role which certain twins played in his life as can be read in his biography. He had shared the bedroom with his second sister after the first had died. At the very time of his sister’s illness Zeeno remembers having had “mimic intercourse” with an older girl several times, either one of his sisters, or more probably one of their friends. Experiences with girls, however, and punishments connected with them seem to have come into associative connection with his sister’s death. It may have been some such anxiety which he was trying to overcome by the repeated self-assurance: “I know a lot of people older than myself who have actually asked me to advise them on certain [sexual] subjects. This always made me think that my advice was pretty good.”
When he talked about his actual sexual experiences, Zeeno’s language became especially queer and detached: “I never mingle in intimate relations.” . . . “I have never desired to indulge with a virgin.” . . . “I decided I might indulge in sexual congress.” . . . “Having found a suitable person, I took part in coitus on various occasions.” In such carefully chosen expressions we see an effort to separate the experience from its affect, a tendency which is obvious both in Zeeno’s thinking and living and in the formal elements of his play construction.
As for the search for the lost lamb, the part of the scene, which in spite of its inconspicuous position at the edge of the table, approached a dramatic content more nearly than any other part: I assume that it represented the unanswered question in the subject’s mind, as to “what happened to the lamb,” the little sister. Other details of this scene which could confirm our interpretation reveal more about the actual family constellation of the subject’s childhood than is permissible to quote.
4. General remarks. In selecting and comparing certain elements of the subject’s memories and of his play, we point to the probable importance of a certain event in his life. As a psychic reality, we assume, the theme of that traumatic event still imposes both its content, and certain structural elements as well, on the subject’s autoplastic and alloplastic behavior, i.e., it imposes certain configurations upon an arrangement of toys on a table.17 In Zeeno’s case we suggest the interpretation that in his life as well as in his play construction he has to separate certain elements because their connection arouses anxiety in him, and that these elements correspond to the details of his experiences with his sister. In this short account we are forced to neglect the fact that in the formulation of every psychic theme it is possible to interchange active and passive, subject and object, without having the theme lose either its importance or its inner truth; that is to say, we may assume that Zeeno is afraid to die young (like his sister) according to the primitive notion of “an eye for an eye,” or that he, the younger, felt himself to have been seduced by his sister, or shared some kind of guilt with her and was afraid of having to die as she did.
Other interpretations may suggest themselves to the careful reader of the subject’s biography. Our conclusion is that he was unable to construct a dramatic situation but revealed only at the very edge the traumatic situation in his memory which struggled for expression when, at our authoritative suggestion “to play,” a safety valve was opened and quickly closed again.
N: Berry
1. Preparatory Period. Without any hesitation Berry builds the form shown in Figure 11a. Then he changes the form and constructs a scene (playing with, contemplating, and at first rejecting the maid as did more than half of the group): The father and mother discover the son with the maid in the kitchen (Figure 11b). But he does not like this scene. He builds another house, without doors, in which the kitchen is separated from the living room and the son and maid from the parents, who, in addition, are completely shut in by a ceiling—the only one to be found in these constructions.
2. The Dramatic Scene. (Figure 11c) He explains the scene more impersonally than the other subjects do. “The owner of the house and his wife, a visitor in the kitchen.” Behind the house in the garden sits “a member of the family,” and on the street the policeman stops traffic in order to let the little girl pass safely.
3. Comments. Again where we vainly awaited a dramatic situation, we find only the indirect suggestion of drama which is implicit in the effort to avoid discovery and accident.
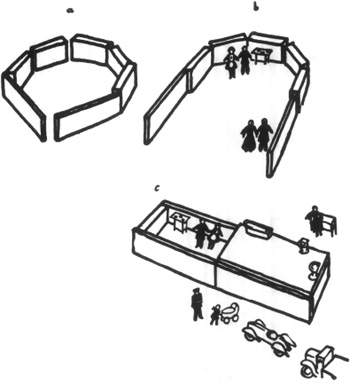
Figure 11
Among the subject’s memories occurs the following scene: At the age of six—a garden behind the house, a little girl with whom he eats onions. He kisses the girl. One day the girl doesn’t come back. She is not allowed to come any more. “Is this because of me?” he asks his mother. “I doubt it,” is the answer. In this moment he says he learned what it meant to doubt—a statement which justifies our taking this scene seriously. An event recurring in his later childhood awoke in him this bitter feeling of doubt again and again, doubt of the justice of his parents. If he had a quarrel with his sister, the parents usually intervened in her favor.
Discovery, intervention, punishment appear in a rather decisive way in the material of the Clinic: For example, the subject relates that Hawthorne’s vicar wears the black veil because he has discovered his brother with a woman. The vicar thus in wearing the veil punishes himself for what he has seen. In the autobiography we find the statement “I had an exceptionally curious mind regarding sex matters and read a great variety of medical books from the age of ten to fifteen.” This may throw light on a neurotic difficulty in reading. This inhibition however had a prior history, Berry having developed first an inhibition against play with girls or touching them at all, especially his sister. Later this inhibition extended to reading, in which his curiosity obviously had found refuge. Visions of the past, so he says, came between him and the reading matter; and it tormented him that there should be so little personal feeling in these visions—a subjective account of that separation of experience and affect which we found in Zeeno.
His first house-form (Figure 11a) suggests a diagrammatic cross-section of a female pelvis. Here he himself has formed that which he perceives in the ink blot test: “Cross-section through a female body, as one sees it in medical books.” Other blots remind him of embryos or portions of a miscarriage; others of ulcers and decomposed animals. Thus the house seems first to represent the (female) body, which contains what he wants to know. It then takes the form of a real house which contains the body which one wants to know about: hence, man, maid, and intervention. But Berry remembers that if one tries to enter and discover the secret, one is discovered oneself and separated from the object of one’s curiosity. Therefore, it seems better to avoid discovery by separating all dangerous elements right at the beginning. Thus, in his play construction, parents are enclosed so that they are unable to discover the son (nor can he, we may add, see what they are doing). This avoidance again (as in Zeeno’s case) has its parallel in a precaution on the street: the traffic is stopped in order to let the little girl pass safely. In this way a traumatic outcome is avoided, but at the same time a dramatic situation has become impossible.
Separated and alone, “a member of the family” sits behind the house in the special arrangement similar to Zeeno’s “sister.” She may well be the girl in the garden behind the house of his childhood, the girl whose disappearance caused or was caused by guilt. Certainly it must be significant that through all of these constructions wherever we are able to sense the persistence of concern for a person who disappeared during childhood, this person is represented by a toy which is placed outside of a closed house or room and always to the right of the subject. In one case, the “best boy” of the group, a dead rival-cousin, was even placed on another table where he “walked in safety.” One cannot help comparing this with the custom of some primitive peoples who make a hole in their houses through which they push the corpses of their dead, only to close it again so that the dead cannot come back into the house. Neither Zeeno’s nor Berry’s house had doors and we find a house without doors in the constructions of the subjects in whose mind the idea of death and sex are closely linked: the dark room whence we come (the womb, the inside of the female body) and the one where we go (the tomb, the beyond). Symbolically these are one idea in primitive thought and may become permanently associated by a traumatic experience occurring at that age and stage of childhood for which this association, in an abortive form, is typical (the phallic-sadistic stage of libido-organization).
Here we might make another suggestion. So far as the first house-form represented a cross-section through a female body it contained a secret with which Berry was much concerned, as is suggested by his history as well as his ink blot fantasies of embryos and miscarriages. In his childhood he had heard that before he was born his mother had given birth to a girl who died—a fact which had strengthened his sexual and medical curiosity and influenced his mental development.
O: Asper
Because of its extreme emphasis on separation a construction which showed the most psychotic elements is of special clinical interest.
1 and 2. Preparatory Period and Dramatic Scene. (Figure 12) Asper places six peasants near one another like soldiers. Then he stares at them for several minutes, looking very unhappy, almost as if paralyzed. Thereupon he arranges some cars: In the green truck he puts a policeman; smaller cars and a man are approaching with a dog. Again follows a long, paralyzed hesitation, as if a single movement would bring about a catastrophe. Suddenly he crashes the red racer into a block so that it overturns. Immediately after this the subject seems freer, as if a magic word had been spoken, and completes the scene quickly. He puts the little girl into a corner and surrounds her by animals. He surrounds the policeman’s car with peasants and turns the peasant with the dog so that he “leaves the field” (as Kurt Lewin would put it).
3. Comments. When the observer enters the room the subject says, “The imagination does not have enough to work on. Everything here is symbolical.” About the little girl he adds: “She does not understand what it is all about. The animals are her pets.” About the green truck: “An army truck. These men could easily be taken into the truck.” (He puts them in.). . . About the peasant: “He is immune to all of us, he lives in the woods, he is outside, he can’t be touched.”
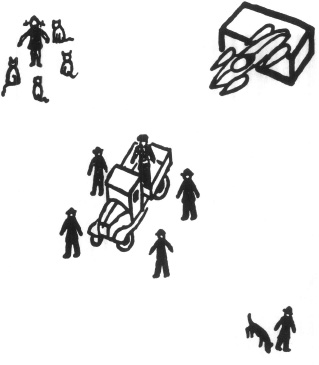
Figure 12
The subject in his nearness to mental disintegration (elsewhere he says that even the word “ ‘incongruous’ becomes meaningless after a while”) was the only subject who felt that his play construction was symbolic; while at the same time, paradoxically but significantly enough, he was the one who of the whole group felt most keenly that the dangers of playing were real. Nearer to “catastrophe” than any of the other subjects, he scarcely dared to move. He maintained a careful organization of cars and soldiers, gradually placed the soldiers closer and closer to the policeman, and felt easier only after he had rendered the red racer innocuous. The peasant with his dog goes silently away: “He is outside, he can’t be touched.”
Much could be said about the psychotic characteristics of this play construction:18 how the danger of symbolic expression in infantile material is feared as if it were a real danger, how the plot shrinks to a mere spatial arrangement whose function it is to make everything, “right in time, right in space, not too late, not too soon, just right,” as one of the inmates of the Worcester State Hospital remarked when he showed me his construction.
It is because of this need to maintain psychic barriers to protect themselves from infantile chaos that out of 40 normal, neurotic and psychotic adults and children the only person to protest against the test as “childish” was an inmate of the Worcester State Hospital. He had said that he could build an accident, but refrained from it. Instead, he merely placed the furniture, people, cars and animals in curved rows. At one point he started to put the little girl into a bed, but smiled thoughtfully and gave it up to arrange another long row of toys. Reminded by the observer that he wanted to build an accident, he said: “Well, well, well, a child might do that, if it cared to.” Then for a moment he threw the cars around furiously, as if illustrating what a child would do. Thereupon he began setting the blocks two and two together, and said, “Some people forget their childhood, others go back to it.” Then, as he built a solid square of block he said, “This could be the foundation for a house—or wharf. And this”—putting two blocks together—“is a breakwater. It is supposed to turn waves backwards.” After a thoughtful moment he began to whirl the breakwater around as if it were helpless against the waves, and said slowly, “Do you think—a wave—can flow—backwards?”
II
“Let nothing happen to the girls and let nothing happen anyway” seemed to be the slogan of the small group of cautious subjects represented by Zeeno and Berry, who by the separation of dangerous play elements demonstrated to us the compulsive character’s technique of prevention. “Let something happen but let it happen to the girl” is the slogan of the majority, whose spokesman we shall describe next.
P: Oriol
1. Preparatory Period. After receiving his instructions the subject jokes. He takes the toy toilet between his fingers and smiles broadly at the observer. Left to himself he grows serious: Let’s see. Little girl? No. Maid? No. Baby carriage? No. (Highly dissatisfied.) Suddenly, with sweeping movements, he makes three piles—people, cars, blocks. He then finds excited satisfaction in taking single objects out of the piles and constructing his scene.
In the center of his construction he first puts a policeman standing on a block with four cars pointing straight at him from four directions. If real, this scene could represent only a suicidal demonstration against the authority of the state. And, although in the final scene he had turned the cars so that they were not pointing at the policeman, his first remark when the observer entered the room continued the theme of revolt.
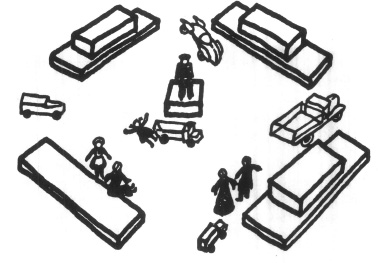
Figure 13
2. The Dramatic Scene. (Figure 13) “This is like the Place de la Concorde, where the riots were.” Of the policeman, “He stands in his box higher than the other people” (suggesting probably something like the Napoleon column in the Place Vendôme). The little girl is run over—thus suffering the fate for which at first the policeman was destined—“because the maid chats with an old friend of her mother and does not watch the girl.” The parents, by coincidence, arrive at this moment and are witnesses to their daughter’s death.
On leaving, the subject again takes the toilet, laughs and says, “I suppose some people use this to express their ideas. I haven’t come to that stage.”
3. Comments: Though the subject jokes twice about the toy toilet, he assures us, without being asked, that he does not use this medium through which he supposes “some people” express their ideas. This and his strange pleasure in piling the toys and in taking single pieces out of the piles, arouses a suspicion as to the psychic reality of a painful element in the subject’s memories. At the age of eight (an unusually advanced age for the breaking through of aggression in this direction) Oriol was found smearing feces. This story is often repeated at home to family intimates, much to his discomfort, and is advanced by his family as a reason for wondering how he ever got into college.
In addition to the riot topic and the hints regarding the anal riot of his childhood, there are in his construction spatial arrangements which indicate what may be the main psychic and physiological quandary of his life, i.e., to retain or release. First he builds one street, then a square with four entrances, and finally points out explicitly that the square has many exits. We may add that no one who had heard the subject talk would fail to remark his speech, which often approaches an oral riot—a flow of intellectually defiant words which he releases continuously. He is said to have learned to talk very late.
Oriol likes to play with the idea of running away from home; but he has decided to run away only intellectually. He keeps silent when with his father, but remains intellectually his own boss, and says so to whoever wants or does not want to listen. While his memories are full of humiliating experiences, his confessions express the wish to overcome humiliation through greatness, and to overcome unclean tendencies by producing beauty. “If I could remodel the world I would like to be the greatest writer.” But, “I am afraid of life and afraid of death.” Sure to be humiliated whenever he expresses his immature and unconsolidated impulses, he must choose masochistic wish fulfillments in order to gain satisfaction. He wants to be a poet—but he wants to be a martyr poet. “I want to expose myself and suffer.” Here, even were it not suggested by other constructions as well, one would suspect that the girl in the accident represents the subject himself whose parents thus witness his suffering.
Of his construction, Oriol is right in saying, “I haven’t come to the stage where I would use the toilet to express my ideas,” for he obviously prefers a suicidal accident to a riot, after the fecal riot of his past (playing with feces) is suggested to him by the stimulus situation of being asked to play. But in spite of his objection, he must repeat the event he wants to avoid in the formal elements of his construction (piling: playing).
4. Second Construction. A year later Oriol was asked to construct another dramatic scene. In evaluating such a repetition we must remember that the earlier construction had taken 20 minutes, had not been understood by the subject as “meaning” anything, and had not been mentioned to him by anybody afterwards. Again Oriol piles the blocks before he starts. This time his square is first round with one exit leading to the water. A truck coming from the direction of the water is headed straight for the policeman. There is a dog in front of the truck. “It will not be run over,” the rebellious subject says, a fact which we shall recall later when, in reviewing the construction of the well-educated and pious Mauve, a dog is run over. In changing the square, all form is abandoned, the blocks and furniture appear in piles. Again the memorial for a revolutionist takes the center and this time it is a communist worker. Quite independent of this scene, another part of the table is supposed to be the inside of a house. Here a little girl stands in front of a mirror “admiring herself and stubborn.” “She is defiant. She does not like people. Later, she will go to the maid, who cannot tell her to ‘shut up!’ ” This parallel to the communistic orator on the memorial characterizes well the state of continuous, narcissistic, and oral revolt in which our subject lives.
When the observer reenters the room, Oriol has the red racer in his hand. After having given his other explanations, he adds it to the scene, remarking as if excusing himself, “This one does not mean anything.” Then, in going out, he says: “I left the bathroom empty. I would be embarrassed—” Thus he seems to follow the pattern of his first construction which he had left with the words, “I suppose some people use this [the toilet] to express their ideas. I haven’t come to that stage.” We have seen how far this last negation really was a double affirmation; we may assume the same about the protested unimportance of the red racer.
5. Remarks. Oriol’s construction shows the confusion which can extend to the adolescent mind from childhood experiences in an almost tragicomic way. Only with weak negations does he separate himself from the most embarrassing childhood situations. A need to expose himself must have been decisive in this construction.
Oriol did not talk when he was expected to; he still soiled when he was no longer expected to do so—and this “stubbornness” (which might well be based on a constitutional or early traumatic factor) still pervades everything he says and does with typical pregenital ambivalence. Not independent enough to do without love and protection, he still is not able to return love because this would have meant in childhood the unconditional surrender of the jurisdiction over parts of his body and now would mean the final socialization of modes of behavior which are derived from those organic functions. Oriol does not soil, because he is neither child nor psychotic; nevertheless, elimination and retention in their characterological and mental aspects are his problem. What is presented here by Oriol, in his chaotic way in regard to anal-sadistic characteristics, differs only quantitatively, not qualitatively, from the general problems facing our whole group of late adolescents. Did their genitality make itself independent of regressive association with the psychobiologically significant drives of childhood? We know that the absence of genital consolidation necessitates a continuous state of defense against the guerilla warfare of infantile impulses which still resist “don’ts” which have long since become senseless, infantile impulses, which promise nonexistent paradises, and which urge the individual to subdue love objects or to surrender to them—in an oscillation between love and hate.
Since we may be criticized for the clinical predilections in our observation of a group of individuals who did not come as patients, it might be of special interest to compare with the illustration of Oriol’s fixation on oral and anal-sadistic autoerotism the construction of Mauve, who was perhaps the best organized personality in the group. His construction shows a typical attempt to overcome the pregenital ambivalence menacing the best organized young men in their relationships with the other sex. Between Oriol and Mauve lies the problem of the whole group: how, in a society, which with moral and economic means discourages unbroken psychosexual progress, can one adapt without sacrificing one’s genital masculinity; how develop without rebellion; how wait without regression; how love without suspicion, fear and hate; in a word, how overcome ambivalence, the counterpart of obedience? This is the moral problem of adolescence which various cultures deal with in various ways.
Q: Mauve
1. Preparatory Period. Mauve took off his coat and, obviously pleased with himself and ready to serve scientific purposes, began his construction like a good organizer, quickly and without interruption. A growing excitement was evident—he got caught by his ideas.
2. The Dramatic Scene. (Figure 14) Mauve explains: “The green truck is running over a dog—it is the little girl’s dog.” A’car coming after it bumps into the truck, a second one is just turning over, a third one tries to avoid the crash. In the kitchen “the maid is fainting; she has a little dog herself and this is the reason why she feels like that.” In the living room we see “a young lady on the couch in the first stage of pneumonia. Something very emotional in this scene. Her fiancé and her doctor are looking down on her. The mother does not feel well and has gone to bed.”
3. Comments: This is the only time a dog is run over instead of a woman; we are therefore interested to hear Mauve in another interview say: “Women are faithful, they are dogs. They have been dogs for so many centuries.” In his outlook on life, as well as in his conception of himself, we see him separate himself from the “animal in us.” “My standards are high and I intend to keep them.” Woman and drives belong to another, an animalistic world which is separated from the young man’s world of clear standards.
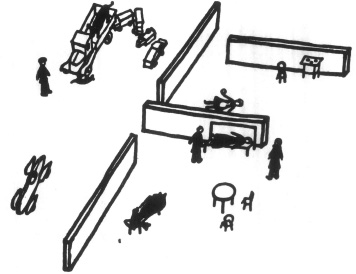
Figure 14
On the other hand, standards are derived from his education by his mother and other women. Many years younger than the father, the mother is deeply attached to the son and he accounts for their emotional relationship in the most explicit œedipus fantasy offered by any of the group.19 Over-obedient to her wishes, he says, he “almost dedicated his life to the avoidance of drinking, smoking and swearing.” And yet certain circumstances in his relationship to his mother seem to draw him deeply into ambivalence towards the weaker sex.
His mother is “handicapped by a disease which periodically disables her completely” and she always tried to keep the healthy, active boy close to home, of which he complains, though taking care of his mother in a most touching manner. If, in the “dog running on the street,” we want to see a symbolic rebellion of the son against all the careful obedience which a physically weakened authority is imposing on him, we may understand that it is his drive, the “animal in us,” which is punished by being run over. On the other hand—the dog represents the group of human beings to whom something happens: i.e., women.
If we confront this subject’s outbreak with his remarks about women on the one side and his educational indebtedness to his mother and other women on the other, a conscious or unconscious duality of attitude towards women, quite common in our civilization, is represented: men easily identify women with the wishes which they stimulate. If they learn to have contempt for “lower” drives (and their pregenital components) they may also have contempt for women so far as they are the objects of their wishes. As beings, however, held in high esteem (“mother, aunt, teacher”) women are also identified with the strictest and most idealistic concepts of conscience. “Angels” or “dogs”—women awaken uncomfortable ambivalent feelings, feelings which spoil the perspective of sex life. A not unusual type of rather well adapted young men (whom Mauve seems to represent) learns to live and to care for a world of achievements which have “nothing to do with women”; it is characteristic of this type that in order to satisfy his conscious and potent genital wishes he goes “to Paris”—as Mauve says he plans to do. There, then, women are neither angels nor dogs; they are French. The girl who does not belong to one’s own culture or class (in other constructions often the girl who does not belong to the family, namely, the maid) is the object of more conscious fantasies.
4. General remarks. We may ask, however, what the little girl, to whom the subjects pay so much damaging attention, might represent. It is hard to give the reader an impression of the uncanny regularity with which these young men whether normal, neurotic or psychotic examined the little girl and, as if they were following a ritualistic duty, seriously put her under the green or red car, or placed a policeman in the center of the scene to protect her. The majority of the subjects who failed to have this theme in their final scene at least considered it and rehearsed it during the preparatory period. A great number of problems must be evoked by this little girl and the crux of the problem must be symbolized by the accidents which happen to her.
Some of the possible explanations, all suggested by material which cannot be quoted here in full are:
a.) The little girl may represent a little girl of importance (i.e., a sister) in the subject’s childhood. The uniform and typical handling of this toy suggests, however, that she represents rather a symbol than an historical individual.
b.) The little girl, as the youngest among the toys, might appear to be the representative of “the child,” the most endangered and therefore the most protected human being in traffic. Can we assume that in spite of the abundance of dramatic moments in life and literature, movies and newspapers, accidents resulting in the deaths of children are emotionally important enough to be the dramatic scene par excellence for the majority of twenty Harvard students? In that case, our psychoanalytic explanations are less valuable, though not entirely worthless since they show the unconscious meaning of this accident in its relationship to other unconscious concepts of “what happens to children.”
c.) The emphasis may lie on girl. Since, according to common infantile theories, girls are made into girls, not born as such, some violence is assumed to exist in sexual matters. The accident, then, which belongs to the “complex” of related symbols dominating our construction, may represent the act of violence of which girls are the victims.
d.) Since, beside the little girl, the victims in these accidents are always and only female toys, the little girl may represent a pars pro toto, namely, the female world, in which case it might have been selected because it provokes the least conscious aggressive fantasies and allows the subject to feel himself consciously free of any participation in the committed violence. We shall presently come back to this point.
e.) The little girl may represent a totum pro parte. Freud, in the Interpretation of Dreams (p. 338), remarks that in dreams “children often signify the genitals since men and women are in the habit of referring to their genital organs as ‘little man,’ ‘little woman,’ ‘little thing.’ To play with or to beat a little child is often the dream’s representation of masturbation.” It is a big step from our first tentative explanation to this interpretation; but the reader will have to decide to make this step with us tentatively—or to leave the question open. Psychoanalytic method, waiting for the most part for associative material in order to interpret any product of the mind, uses only a few “established” symbols, uniform “translation” of which has proved to be necessary and suitable in long and exhaustive studies.
Two of these symbols with which we are concerned here are put together by Freud in a title to the interpretation of a woman’s dream which states bluntly: “The ‘little one’ as the genital organ. Being run over as a symbol of sexual intercourse.” (Op. cit., p. 342.) Dream interpretation thus suggests that what the subjects do with the little girl corresponds in their unconscious with ideas of autoerotic and alloerotic sexual acts, in which something happens to the partner’s or the subject’s own sexual organs. There is nothing in their strange behavior which a priori could devaluate such a strange notion.
f.) We cannot avoid pointing to a sociological factor, namely, the sexual life typical for such a group of biologically mature individuals as our subjects. Their sexual activities are autoerotic, or else consist of a kind of mutual (heterosexual) autoerotism, more or less sanctioned by society. The danger of this form of gratification is the conditioning of masculine impulses by the repetition of a situation with infantile characteristics. Whenever the mature drive is aroused, the impulse of masculine intrusion and certain related sadistic tendencies are mobilized with all the other impulses which participate in the pattern of complete sexual satisfaction. In mere sex play they fail to be satisfied and—as it were—to be disarmed. It is, I think, this frustrated intrusive component of masculinity, which, though continuously stimulated in our subjects, has not yet found its wholesome amalgamation with the other factors of heterosexual partnership, and which therefore in their secret fantasies appears in a certain homicidal and suicidal rudeness—which, we may add here, has an important sociological counterpart in certain adolescent and cruel forms of public sensationalism not dissimilar in content to our constructions.
g.) Female subjects who constructed scenes with the same toys showed as a common factor the criminal man (father). The five college girls among them (the same age as our subjects) constructed the following scenes:
R: A father, who was a deserter in war and lives in shameful exile, picks up on the street a little girl who has been run over by a truck. She is his daughter.
S: A selfish father, who has neglected his wife and children for years, comes home and finds everything destroyed and everybody killed by a flood.
T: A father, supposedly away in an insane asylum, comes home to murder his family.
U: A landowner strangles his wife. His servant’s daughter, to whom he has made advances, testifies against him at the trial.
V: Robbers steal a table out of a house in the middle of the night.
It would be interesting if further studies would substantiate that to the main theme of our male subjects (“Something happens or is prevented from happening to a girl”), there corresponds a female one: “A man is (or is prevented from being) criminally aggressive.” The fact that—with a few exceptions—both sexes place a member of the opposite sex in the center of the construction, points clearly to a sexual component in scenes which on the conscious level refer to danger and death.
W: Krumb
1. Preparatory Period and Dramatic Scene. Krumb considers for a while the problem of whether to use one or two tables. He decides on one. With two blocks he builds a wall, puts the red racer at an angle of 45° toward it and then makes a small opening in it. Then he puts the father into the house so that the red racer, if driven, would run through the hole in the house and hit the father in the back. (Figure 15.) After this his doubts disappear. He obviously gets a funny idea and, laughing, puts the son and the maid together into a bed. The scene is completed quickly as seen in Figure 15. The father finds the son in bed with the maid and forbids intercourse. “Nothing homosexual is going on in the other room,” adds the subject. The little girl is caught between two cars and the red racer speeding dangerously around the corner means one more danger for her. He seems not quite sure about which is the front and which the back of the racer, so that in reality it would, if “speeding dangerously,” hit door and father.
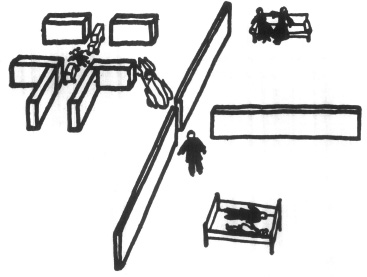
Figure 15
2. Comments: This subject, the only one to put a boy and girl in a bed together, is a manifest homosexual—a fact which without any help from the rich but disorganized and complicated material of his life history, makes it possible for us to understand the meaning of the almost topological description of his inner conflicts in his scene; the living between two alternatives, both dangerous.
“Last year I had affairs with about three women and some fifteen men. Now it is only with men that I can find happiness. Being homosexual makes it possible for me to repress sexual impulses (?). I wish I could repress my feelings of guilt also.”
It seems that Krumb tries to appease his growing feeling of guilt by the following arrangement: the father, between two rooms with a couple of the same sex in one and a couple of heterosexual lovers in the other, turns to the latter and forbids what they are doing. Thus the father himself decides against heterosexuality. The subject assures us that “nothing homosexual” happens in the other room, without our asking. In fact, he did not even know whether or not we were informed of his sexual predilections. Neither did he know that he had given himself away in his very first move: the arrangement of the racer, the door and the father. [Because we know] how often a house symbolizes a body and a car the genitals, this first construction represents the form and mode of a homosexual act: intercourse per anum. (See Oriol’s second construction.) His indecision, then, as to which direction the car is going (whether crashing into the father or into the already mutilated girl) represents the alternative to the homosexual choice: to be the aggressive or the passive, the sadistic or the masochistic, partner. Here again is a choice, in which guilt doubtless drives him into the masochistic part, as many of his remarks in other interviews indicate, i.e., “The moving picture Death Takes a Holiday made me in love with death.”
We have to leave it to the reports on their biographies to emphasize the complicated psychological aspects of the struggle of conscience in the individual subjects. If we could report more examples it would be worthwhile to define and to compare the different ways in which a conflict of conscience appears in the preparatory period, with the outcome as represented in the final scene. In the succession of toys which the subjects take and refuse at the beginning, one notices a peculiar alternation of symbols of repressed (maid, etc.) and repressing forces (policeman, etc.). The street seems always to offer a welcome opportunity for shifting the problem to the impersonal. The subjects show all varieties of guilt-feelings from the anxiety of losing love and protection (i.e., in building harmonious scenes with the mother at the table and the maid at the stove—entirely forgetful of the instructions) to the fear of catastrophe (policeman regulating traffic and preventing accidents as the only “dramatic” element) to various forms of self-punishment. It is as if these subjects, in the slow tortuous process of civilized maturation, had to find a painfully individual substitute for that sacrifice of a tooth or other symbol which “cruel” primitives in their puberty rites inflict uniformly and once and for all on the boys of their community.
Second Construction. One year after this construction (it might be well to state here again that not one word of interpretation was given to the subjects) Krumb was again asked to construct a scene. He immediately asked: “May two things happen?,” thus taking up again the dualism of the first construction. He builds first two houses, then one house with two parts, two rooms in each part. Again males and females are separated. The father, he says, has a homosexual crush on a severely wounded soldier and is in the bathroom—while in the street the red racer is wrecked by the green truck. “I have a feeling,” the subject remarks, “that I have repeated my last construction. I struggled for three minutes to overcome the feeling that I did the same thing. Then I did—and found that I had expressed homosexuality this time, which it seems I could avoid last time.” Finally, Krumb gives a confirmation of our first assumption, which no doubt to many readers seemed hazardous, namely, that the small hole in the house of the first construction symbolized the homosexually attacked rectum; the house of the second construction, again, and at the same place, has a small hole. Krumb remarks about it: “The house is badly built, bad odors come out of here.”
III. X: Vulner
This is the construction of the only subject to whom the suggestion “dramatic scene” implied a scene on a stage.
During the Preparatory Period Vulner is very hesitant. He takes the son first, then the father, but puts them back and seems to think seriously. He accidentally drops the son, plays with the policeman, in serious thought, head dropped forward. Should he take the cow? No. Then he takes the son again and acts quickly.
The Dramatic Scene represents the corner of a room. The mother is sitting in a chair, the father stands in front of her. In a doorway stand son and daughter.
“The head minister is handing in his resignation. The day before he had talked with the queen about the question of the crown prince’s marriage to a commoner. He had decided against it. In the meantime he has learned that it is his daughter whom the prince wishes to marry.” Asked what the outcome will be, the subject replies, as if he were finishing a fairy tale told to a child, “He will probably marry her.”
Analytic Remark: The most interesting aspect of this “really dramatic” construction is that there is very little to say about it. The scene possibly contains some hints in regard to the subject’s family situation; he has one sister, no brother. But essentially the scene is a dramatic cliché and does not suggest any detail of the subject’s biography, except that his mother is a writer and that as a boy he had often participated in dramatic plays.
IV. (Final Remarks)
Having asked out subjects for a dramatic scene, we find a product of traumatic tension; instead of tragedy we find accident.
Dramatic and traumatic moments have one psychological element in common. Both are events which transgress the boundaries of the human ego, the first in widening it beyond individuation, the second in nearly extinguishing it. In other words, in a truly dramatic moment the individual is confronted with a choice which may make him the heroic or tragic master of human fate in its eternal aspects; he is allowed one chance to overcome the bondage of gravity and repetition. The traumatic moment destroys individuation, chance and choice, and makes the individual the helpless victim of repetition compulsion.
To be sure, in offering the little toys for a dramatic task we probably asked our subjects to take a too difficult step from the ridiculous to the sublime. In offering play material we ourselves have provoked the spirit of infantile conflict, since play “presupposes a psychic substance which is not quite structuralized yet.”20 The specific conflicts appearing in the constructions indicate that the subjects when confronted with toys, continued where they had left off in their childhood play with the attempt to overcome traumatic experience by active repetition in play.
In describing these results we naturally do not characterize individuals in their conscious and rational individuation. The psychoanalytic microscope first focuses on neurotic material in its specific psychosexual characteristics. It shows us the inner frontier where the rational human mind—whether in the state of infancy, savagery or civilization—is constantly faced by the wilderness of the irrational.
The set-up of this particular study is not of any general value and is not recommended as a psychological experiment. But the results of this accidental undertaking may be of some interest in regard to the psychology and the psychopathology of play (important for the treatment of patients who cannot or do not want to speak): we can observe directly the structuralization of a given space in accordance with the qualities of a traumatic configuration, which imposes on the subjects’ autoplastic and alloplastic behavior spatial elements of a past event or of the way in which the subject has armed himself against the (irrational) danger of its recurrence.
Further deciphering of play hieroglyphs—especially in the legitimate sphere of childhood—may offer valuable keys for the understanding of the prelinguistic and alinguistic strata of the human mind.
Notes
1 Anna Freud. Introduction to the Technic of Child Analysis. Nervous and Mental Disease Monograph Series 40, (1928), 43.
2 Robert Wälder, “The Psychoanalytic Theory of Play.” Psychoanalytic Quarterly, 2 (1933), 208–24.
According to the current theories of play, either the past, “a pressure exerted by unfinished processes,” leads the playing child’s mind to the mastery through repetition of traumatic experiences: “adding an active counterpart to the passive experience” (Freud); or the present is in the lead insisting on the discharge of surplus energy, on the fulfillment of wishes here and now, or on functional pleasure (Buehler, in Wälder’s formulation: “pleasure experienced in pure performance without regard to the success of activity”); finally, it may be the future and its tasks for which the child may be training himself in the trials, errors and victories of his play experimentation (Groos).
3 Sigmund Freud, Introductory Lectures on Psychoanalysis (London, Allen & Unwin, 1922), 128.
4 George Santayana, The Last Puritan (New York: Charles Scribner’s Sons, 1936), 98–99.
5 As to the development relationship of biting and focusing, see Chapter III, B, page 105.
6 Zeitschrift für psychoanalytische Pädagogik, IX (1935).
7 See part 3 of this note page 102.
8 In concluding a letter to his mother, J wrote instead of “Love, J,” “Left, J.”
9 See, however, case P (Oriol) in Chapter IV, page 124.
10 See case E, page 85.
11 When the author first used the scheme to be presented on the following pages in order to explain certain play phenomena in a seminar in Boston, in 1934, he did not know of F. Alexander’s “vector analysis.” (See the publications of the Chicago Psychoanalytic Institute.) For the limited purpose of these notes, it seems better not to discuss Alexander’s conclusions.
12 A sixth mode,  digestive-assimilative “building-up” is vaguely put “inside the body.” It will have to be replaced by whatever may in the future best represent the knowledge of the complicated relationships and connections (4, 5, 6) of the inner organs to the social organs, which will prove to be of some importance in regard to connection of body-ego and play structurization.
digestive-assimilative “building-up” is vaguely put “inside the body.” It will have to be replaced by whatever may in the future best represent the knowledge of the complicated relationships and connections (4, 5, 6) of the inner organs to the social organs, which will prove to be of some importance in regard to connection of body-ego and play structurization.
13 A later, mature level of this correlation, characterologically and pathologically not independent from this first pregenital level, may be seen in the circle of conception (more or less active incorporation) pregnancy and parturition (more or less retentive or eliminative) and lactation (in which the woman accomplishes more or less the long desired equivalent of intrusive generosity). Men find a fulfillment of this correlation in the sublimation of creative work.
14 Margaret Mead, Sex and Temperament (New York: William Morrow & Co., 1935), 27.
15 The experimental or interview procedures of the Harvard Psychological Clinic mentioned in this report are:
1. Conference. (Dr. Henry A. Murray) The first session for the subject was the Conference. The subject sat down at a table with the 5 members of the Diagnostic Council. He was asked questions and given certain tests to perform in their presence.
2. Autobiography. (Dr. Henry A. Murray) The subject was asked to write for 2 hours about his early life and development. He was presented with an outline to guide him.
3. Childhood Memories. (H. Scudder Mekeel) The subject was given a questionnaire pertaining to family relations, and he was interviewed twice (each session one hour) and asked to give as many memories as possible of his childhood and adolescence.
4. Sexual Development. (Dr. William G. Barrett) The subject was asked to lie on a couch and say what came to his mind. Later, he was asked various questions about his sexual development.
5. Hypnotic Test. (Robert W. White) In two sessions, an attempt was made to hypnotize the subjects and a numerical score assigned representing his susceptibility to hypnosis. On a later day, a different interviewer encouraged him to discuss the test at length.
6. Thematic Apperception Test. (Christiana D. Morgan) The subject was shown a series of dramatic pictures. He was asked to make up a story for which each picture might be used as an illustration.
7. Imaginai Productivity Test. (David R. Wheeler) (a) Beta Ink Blot test. The subject was asked to tell what forms he could make out in the ink blots, (b) Similes test. The subject was asked to make up similes for certain words (presented to him in succession by the E). (c) Minister’s Black Veil test. The subject was asked to spend an hour writing a story using as a theme the appearance of a minister in the pulpit with a black veil over his eyes. (Hawthorne).
16 Unfortunately such a partial report as this one cannot convincingly demonstrate this specificity. The skeptical reader is referred to the Clinic’s forthcoming publication which, in addition to further reports of procedures with the same subjects, contains detailed biographical studies. (The names used in this report are those used in the Clinic’s material.)
17 In Kurt Lewin’s terms: A “structuralization of the life-space” represented in play, a material which is less “refractory” than actual life.
18 See also Saul Rosenzweig and David Shakow, “Play Technique in Schizophrenia and Other Psychoses, II. An Experimental Study of Schizophrenic Constructions with Play Materials.” American Journal of Orthopsychiatry, VII (1937), 36.
19 See the Clinic’s publication [page 749, item 6].
20 Wälder, op. cit.
I. Orientation
The purpose of this monograph is a modest and elementary one. Specimens of a psychotherapist’s experience, namely, the observation of the first play enacted by young patients in his office, are reviewed, as it were, in slow motion. Two aspects are isolated as far as clinical material permits: What, to this psychotherapist, are the outstanding attributes of a play observation? What conscious considerations lead him to the “meaning” on which he bases his first diagnostic decisions?
This primitive inquiry marked the initial phase of a study of neurotic episodes and incipient neuroses in the pre-school child.1 Unfortunately, however, simple purpose does not necessarily make for simple reading; and the concentration on small specimens in a field with such vast connotations and (recently) such general appeal necessitates a rather general introduction.
The problem of play lies at the intersection of a variety of educational and clinical interests. In reaction to an era which hoped to develop virtues in children by clipping the wings of their spontaneity, modern education wishes to develop and to preserve, modern psychotherapy to utilize the benevolent powers which are said to emanate from the child’s “creative” activities.
The contribution of psychoanalysis to this development is a singular one. It not only assumes, with others, a vague—self-teaching, self-healing—function in play but also detects a detailed correspondence between central personality problems and both the content and the form of individual play creations.
The clinical psychoanalysis of play, however, has shared the methodological limits of other psychoanalytic media with which Freud did not concern himself in detail (as he did with dreams, slips, witticisms, etc.). Their discernible phantasy content is welcome as something vaguely similar to and therefore useful substitutions for memories, dreams, and other media which are not plentiful in contacts with a small child; their specific variables, however (such as, in play, the variables of extension in actual space), have not been considered worth any special methodological consideration. Responsibility for this neglect seems to lie in the same general attitude among psychoanalysts which induced Freud to complain in regard to the interpretation of dreams, the oldest via regia to the human mind: “Die Analytiker benehmen sich als wäre die Traumlehre abgeschlossen.” (7)
Tenaciously as the clinical worker may cling to standardized habits of interpretations and may try to see by means of a new medium only that which he had learned to see through older ones, his experience is never the same; new variables of changed experience constantly force him to imply new concepts or a different use of old ones. The clinical observer not only shares a particularly elusive personal equation with all those who observe with the naked eye and ear. His work also underlies the practical equation derived from the necessity to influence sooner or later the very material under observation. Finally, something like a cultural equation expresses the influence on his work and thought of his constantly changing function in science and society. Whatever scientific ore, therefore, may be present in the clinical experience (made elusive by technical, personal, practical, and cultural changes) comes to light mainly through the therapist’s constant efforts at making explicit some of the implicit (preconscious) steps of selecting, associating, and reasoning which constitute his clinical “intuition” at a given time and in a given technique.
This being our object, we shall be forced to risk tiring the reader with details, details which will seem superfluous to the play technician
whose optimism is satisfied with shortcuts, and senseless to the psychoanalyst who has learned to view pessimistically any attempts at demonstrating psychoanalytic experience to the “outer world.”
In adult life (10) “talking it out” is the simplest autotherapeutic measure employed during tense periods by individuals who are not too asocial. Religious and psychiatric sects ritualize it in varying degrees by providing at regular intervals an authoritatively sanctioned listener who gives undivided attention and, sworn to neither censure nor betray, bestows absolution by explaining the individual’s problem as belonging in a greater religious, ethical, sociological, medical context. The method finds its limitations where the clinical situation loses the detachment in which life can mirror itself and becomes the center of a passionate conflict as expressed in a too dependent (if not sexual) or too hostile attitude toward the therapist. In psychoanalytic terms: the limitation is set by the tendency (especially strong in neurotics) to superimpose one’s basic conflicts on every new situation, even the therapeutic one. This leads to a transference which temporarily makes the therapeutic situation a disturbing factor in the patient’s life. The patient is in resistance; in a war to end all wars, he becomes more deeply embroiled than ever. At this point non-psychoanalytic efforts are given up; the patient, it is said, does not want to get well or is too inferior to comprehend his obligations in treatment. Therapeutic psychoanalysis at this point systematically begins to make use of the knowledge that no neurotic is undivided in his wish to get well and by necessity transfers his dependencies and hostilities to the treatment and the person of the therapist; in revealing these “resistances” he points the way to his treatment.
“To play it out” is the most natural autotherapeutic measure childhood affords. Whatever other role play may have in the child’s development (and I do not think that these roles are adequately known), the child also uses it to make up for defeats, sufferings, and frustrations, especially those resulting from a technically and culturally limited use of language. This, the “cathartic” theory of play, is one of the many play theories, all of which agree only in assuming an untimely tension. If not a catharsis for excessive (traumatic) stimulation in the past, play is considered the expression of a surplus energy for which there is no more “practical” use at the moment; with untimeliness projected into phylogenetic dimensions, play becomes a recapitulation of (now useless) phylogenetic leftovers or the preparatory expression of what in the future will be useful activity.
In Spencer’s classic words, wherever circumstances allow or suggest play, those tendencies are “simulated” which are “unusually ready to act, unusually ready to have their correlative feelings aroused” (14) (but at the same time are not any more or not as yet practicable in connection with their real goal).
Of all organisms the human child is probably the one who has to learn to postpone temporarily and permanently the most formidable array of tendencies which because of his slow maturation and his higher aspirations are precocious or definitely out of place. Some of them (as Freud has recognized in neurotics) remain “unusually ready to have their correlative feelings aroused” throughout life. Our new knowledge of such unconscious and subverbal “readinesses” gives the previous theories of play a new and specifically human meaning. In all its slow maturation and long defenselessness, the human child, so we learn, lives through periods of diffuse, culturally and biologically impracticable impulses of a sensual and aggressive nature, which he cannot help attaching to the narrow circle of his very originators, protectors, and educators—his family. The task of maturation, then, is to outgrow in the most constructive manner these premature emotional and instinctual attachments while outgrowing the need for protection. But this is a slow and partly indefinite process; and the human animal not only plays most and longest but also remains ready to become deadly serious in the most irrational contexts.
Modern play therapy is based on the observation that a child made ambivalent and insecure by a secret hate against or fear of the natural protectors of his play (family, neighborhood) seems able to use the protective sanction of an understanding adult, in professional elaboration the play therapist, to regain some play peace. The most obvious reason is that the child has the toys and the adult for himself, sibling rivalry, parental nagging, and routine interruptions do not disturb the unfolding of his play intentions, whatever they may be.
The observing adult’s “understanding” of such play, then, is a beneficial factor even where it finds only an intangible minimum of expression in the child’s presence, while its value for an indirect use in advice and guidance can hardly be over-estimated. The peace provided by solitary play or by play in the presence of a sympathetic adult often radiates for some time, often long and intensively enough to meet the radiation of recognition and love from some source in the environment, a necessary factor in all psychological cures. The chances therefore seem better where the mother too has an opportunity to relieve in conversations her ambivalence toward the child and is prepared to respond to his improvement.
As we shall demonstrate, however, the phenomenon of transference in the work with the playing child, as well as with the verbalizing adult, marks the point where simple measures fail, namely, when an emotion of such intensity as to defeat playfulness forces an immediate and only thinly-veiled discharge into the play and into the relationship to the play observer. The failure is characterized by what is to be described in this monograph as play disruption, i.e., the sudden and complete or diffused and slowly spreading inability to play.
Recent work in this country has emphasized the alternatives of “passivity” or “activity” on the part of the play observer, the extreme passive attitude representing a certain seductive lifelessness, a kind of play hostess attitude, the extreme active one an animated encouragement of the child to “release aggression” against toys named after members of the child’s family. Where a child can follow this latter suggestion without immediate or delayed play disruption we have no reason to be worried about the child, although the “release” theory implied in such procedures seems tenable only in clearly “traumatic” cases and there only theoretically, as the thorough analysis of such cases shows. The clinical problem seems to be solved only be the establishment of permanent and sufficient everyday release channels and not by a momentary release under special conditions. Much of this “release” ideology as well as certain forms of purely symbolic and purely sexual interpretation seems to be a revival of the most primitive techniques of the early psychoanalysis of adults—now transferred to the new field of play therapy.
Those children who transfer not the solution but the insolvability of their problems into the play situation and onto the person of the observer need to be induced by systematic interpretation to reconsider, on a more verbal level, the constellations which have overwhelmed them in the past and are apt to overwhelm them when reoccurring. Where this goal is given, child psychoanalysis begins.
Child analysis proper, in the cases which are its domain, seeks to provide the child with opportunity for catharsis only in the frame of an intimate therapeutic contact in which repeated interpretation furthers the verbal communication of inner dangers and the establishment of a supremacy of conscious judgment over unmanageable or incompletely repressed tendencies. To interpret means to reveal to the patient, at a dynamically specific moment, meanings which he can fully admit to himself only under the guidance of the therapist. Such interpretation is impossible without a technique which systematically and consistently reveals the dynamics of the developing therapeutic situation, especially the forces of transference and resistance. Its application is useless or dangerous where there is not time enough to follow the patient and to give new interpretations until a lasting ability is secured to express in a more conscious and social, more humorous and more useful manner that which he first could only admit to verbalization under the guidance of a therapist. Interpretation waits for a specific moment; it needs preparation and after-treatment; it does not claim success until a general and lasting increase of constructive vitality seems secured.
As the treatment proceeds and as the child’s verbal powers increase, play observation loses much if not most of its exclusive importance. For the age group reported, however, the investigation of the child’s play is a natural first step which coincides with the first step of a variety of treatments; while it can be abandoned or deferred without damage, it can also be pursued and developed without break.
As stated above, this monograph demonstrates the analytic method merely in so far as it permits one to locate through play observation the approximate “seat” and extent of an emotional disturbance before definite clinical procedure is decided upon. This procedure may or may not be child psychoanalysis. Only in the last case to be reported will an effort be made to demonstrate the function of therapeutic interpretations. I should like, however, at least in the introduction, to transgress the scope of this monograph and to indicate briefly some views in regard to the wider problem of psychoanalysis.
Psychoanalysis, besides being a psychotherapeutic method, is a method of research, a system of psychological and “metapsychological” concepts and a social phenomenon. It rests on observation, on speculation, and on professional organization.
Freud’s unconventional eye gave clinical observation a new focus and a new scope. The new focus was neurotic man at the intersection of nature and culture, the scope so vast that the neurologist Freud, in conceptualizing the peculiar logic of a neurosis, found himself referring to such seemingly and academically remote phenomena as the primitive’s superstition, the child’s wishes, the artist’s imagination. However, in doing so Freud painstakingly emphasized the fact that the everyday basis of his expanding system was and remained the observation of the forces most clearly operating in the clinical situation; namely, tranference, resistance, repression, regression, etc. The clinical observer of a verbalizing adult sees his personality outlined in the way in which his feelings, memories, hopes, etc., do or do not cross the threshold of verbalization, once this threshold is emphasized by the suggestion to associate freely. He has to evaluate a dynamic scale of representations, on which a single idea or complex of ideas alternately appears remembered, re-enacted, dreamt, avoided, projected on others, repudiated, joked about, etc., each time with specific disguises and omissions and accompanied by a specific quantity and quality of awareness.
Psychoanalysis emphasizes the fact that the non-clinical fields such as psychology, anthropology, child development, etc., overlap one another precisely in as far as they are psychological. This could be demonstrated either by a changing of focus of their own methods, which would make it possible to find in their material the facts which Freud found in his neurotics, or by an adaptation of the psychoanalytic method to their material, i.e., through methods which use in these non-clinical situations whatever forces in them correspond to the clinical forces of resistance, regression, and transference.2
Thus one will see how individuals and groups defend themselves against ideas and needs which are considered dangerous to the commanding ideas and needs of their reality, and how the suppressed, the expressed, and the aspired to are interwoven.
In the application of psychoanalysis to the study of children, the variations in the individual’s quantity and quality of verbalized awareness obviously cannot provide the proper dynamic scale because children, on the whole, cannot obey the rule of free association. Of the scales to be applied instead, two will be elaborated in this monograph, namely, the correlation of the individual’s verbal behavior with his spatial expression and his recognizable changes of affect.3
There are a number of facts which, for better or worse, are constantly re-established by daily psychoanalytic experience; the discrepancy between the representation in verbalized consciousness and the motivating power of certain ideas (repression); the priority among these ideas of those concerning the child’s first bodily (sexual) orientation in the world of physical and social facts; their disguised expression in various metaphoric ways; the sexual deficiencies and the defensive personality changes resulting from them, etc. All these facts are taken for granted here although they are, of course, considered subject to further scientific observation. The observation of these facts, however, and the theory of transference, resistance, and repression imply and have led to many concepts of what Freud calls “metapsychological” nature.
Freud and the first psychoanalysts were faced with the task of conceptualizing a field which had almost no tradition. They were erudite men who had at their disposal modes of thought from a variety of the scientific and extrascientific fields which in the past had monopolized man’s conduct, such as theology, philosophy, and art. In the psychoanalytic system not only the superficial evidence of an occasional term such as Oedipus Complex points into the past, but, more important, such sweeping conceptual configurations as the free floating in the body of a libido with its cathexis and catharsis; in the mind, the struggle of an ego between an id and a superego: and in the world at large, a gigantic melting of life and death instincts.
The libido concept, for example, might be suspected of having fallen heir to the Greek interpretation of hysteria; there the uterus wandered about in the body, selecting its organ for interference. In Freud’s system it is not the uterus but the libidinal cathexis of the psychic representation of the genitals which is displaced to the representation of other parts of the body which then show conversion symptoms. The same libido, if cathexing the therapist’s representation in the patient’s mind (and reinforced by the transference of the cathexis of the father image to that of the therapist’s), creates the favorable condition for the influence of the therapist on the patient as the animal spirits of the last century did while still actually crossing the space between patient and therapist.
In spite of his antiphilosophic sentiments, Freud on occasion referred, not without sovereign pleasure, to such similarities between his concepts and those of prepsychological thinkers, the last example being the identity of the life and death instincts with Empedocles’ philia and veikos. (7) His “id” he early recognized as a kin of Schopenhauer’s will. Both id and will, several steps further back in the history of conceptual configurations, take on personal shape, appear as the devil.
Freud has traced these and many other ancient images from their projection onto the periphery of man’s world back to where they originated, in man’s mind, where observed with dynamic tools they become a subject of psychology. He draws these images closer to the scientific thinking of his day (and nearer to observation and, ultimately, experiment) by making them quantitative and genetic. Thus, the libido theory on the one hand becomes something like a theory-of preservation of psychic energy, on the other hand, the theory of the fate of the libido directly contacts the theory of evolution.
Freud’s historical habit of weighting a particular observation with whatever standard of conceptualization seemed adequate to further its clarification has led to the use in psychoanalytic literature of a disturbing variety of, as it were, terminological currencies which alternately represent human data in terms of the mythology of millennia, the philosophy of centuries, and the scientific methods of decades. Freud implies that in time all these currencies will be exchanged, at their face value, into one based on the clinical and experimental standard of the day.
The real danger, however, of the pre-scientific ancestry of revolutionary thought in psychology has proved to be and will, at least for a while, be a group-psychological one. A certain idea, by fitting into an ancient, possibly long-suppressed mode of thought, to some appears immediately convincing and pertaining to the nature of the experience: “this I have always known.” The same mode of thought being alien (perhaps repressed) to others may deter them from consideration of the same idea even if it is already well on its way to substantiation: “this I have always avoided.” In such development observation is often little consulted; group identification replaces scientific method; and a regression takes place to conflicts in ancestral thinking and to spiritual and philosophic leftovers and leftouts.
This third influence in the formation of a system, namely, the group psychological meaning derived from the organization of its adherents, has been especially powerful in the history of psychoanalysis for another reason intrinsic in its nature.
When Freud, in the good faith of scientific ethos, first revealed the hitherto undescribed manifestation on which he focused his attention, and the unheard of selections and associations of his mind which made him focus on them, he was met with an overwhelmingly ugly response from the scientists of his day. Partially understandable as a Victorian reaction against a bold mind and his sovereign habits of deduction, this response nevertheless had certain qualities in common with the behavior and the argumentation of a cornered patient: it forced Freud to realize that his era was going to resist as one patient the Freudian kind of enlightenment. He proceeded, however, to recognize and to conceptualize this “resistance” as an attribute of living psychological matter. Freud’s observations had struck at the specific illusion which had reached its climax in his era, namely, that there was no psychological limit to the subordination of sex and aggression to will, belief, and reason. Resistance, in the larger sense, is human inability to accept any theory which makes the current conception of “free will” relative.
The ever-renewed detection and therapeutic utilization of the selective, repressive, projective mechanisms in the human mind are the tools which Freud gave to psychotherapy and psychology; they point beyond systems and schools, for they insist on pursuing resistance wherever it chooses to hide in the evolution of human consciousness, and no school can avoid for long becoming a hiding place for collective regressions—not even the psychoanalytic one from which groups of adherents necessarily aim to derive a secondary gain by ascribing to themselves more than a relative freedom from resistance and privileges such as methodological isolation.
But there is no reason to doubt that all these phenomena will gradually and permanently become subject to the developing psychoanalytic method itself. Always proceeding along the line of most resistance, it will stimulate clinical observation and its application, and will make it possible to understand conceptual and group psychological process such as marked the beginning of its own history.
Freud has not analyzed children himself. He based the reconstruction of psychosexual development in childhood on the systematic analysis of the verbalizations of adult neurotics and on a wealth of corroboratory, although unsystematic, observations of childhood. When it became apparent that clinical contact with small children was possible, Freud left this field to others (and expressly to his women pupils). The few references to direct child observation to be found in his work (8) make apparent the loss which this Victorian fact implies for child psychology.
Anna Freud’s cautious and clear Introduction to the Technique of Child Analysis (5) still seems to be the only safe technical statement in regard to the application of psychoanalysis to clinical work with children. However, detailed discussions of her Vienna seminar, which represented the most significant expansion of her basic technical ideas, have not been published. The field has thus been left to clinical abstracts and to one most ambitious systematic attempt, namely, Melanie Klein’s The Psychoanalysis of Children (11).
Mrs. Klein has enriched our thinking by concentrating on some neglected features of infantile, and especially female, phantasy life, such as the preoccupation with the body interior. Her book, however, abounds in methodologically irresponsible statements referring to what its author is supposed to have “shown” in regard to the psychology of normal childhood. From these “demonstrations” she and her followers derive the license not only to reconstruct earliest psychic development where it is least approachable, but also to convey such reconstructions to child patients. Their interpretations, fairy tales stripped of all artistry, seem to fascinate children and are said to cure them. The author of this paper cannot, at the present time, overcome a suspicion as to the final adaptation of the child cured by this method to any environment, except that which cultivates a special type of psychoanalytic outlook.4
In some of the contributions to the child analysis number of the Psychoanalytic Quarterly (1), a new living relationship between disturbed child and understanding adult (a kind of doctor-aunt who helps the child to find words for unspeakable experiences) is lucidly described.5 As far as smaller children are concerned, such descriptions seem most convincing where the historical tool of psychoanalysis, namely, “making conscious,” is not assumed a priori to have been applied. While the concepts of resistance and transference when applied to smaller children lose little of their value as tools of investigation, repression, because of the lack of dependable verbal contact between therapist and child, becomes a somewhat meaningless concept; by inferring it, one often misses the opportunity to observe stages in which what is later to be called repression is just about to happen, and by treatment seems prevented rather than made retroactive. It is exactly this prevention of a disastrous gap between verbal and subverbal experiences in childhood which promises to become the most useful contribution of psychoanalysis to a future era (and promises to have been the most poignant criticism of the passing one).
However, we have not always been conscious enough of the fact that in the humanities premature reconstruction has to resort to medieval images. In some of our writings Freud’s tentative abstractions of a topology, a genetics, and a mechanics of psychic life are inadvertently colored by visions and clothed in moods. What the child’s ego is said to experience and to do often goes even beyond the concept of a persona in a person; it implies an organism with a sensory and motor system of its own within the organism—indeed, a human-like being between a devil-and a god-like one. Like diaboli of old, these parts of the psyche reflect and act, avoid effort and gain satisfaction with sly and dialectic skill. Similarly, in the conceptualization of inaccessible parts of childhood there occur homunculi of synthetic babies who are complete miniature editions of adult cannibals or psychotics; or reconstructed newborns laden with primordial images of sin and guilt. Thus residues of the intellectual past and by-products of extra-scientific ideologies of today are used to draw prematurely into a developmental synthesis of “the child,” striking observations as well as moods, beliefs, and divinations from many planes.
Any description of a prolonged period of child psychoanalytic treatment seems to find a powerful obstacle in the fact that the child, relatively more than the adult, is constantly changing under the influence of extratherapeutic factors. Therapeutic influences act at best as accelerators and inhibitors on a continuum of maturational processes which, in their normal or, let us say, extra-clinical manifestations, for the most part have never been properly studied and described. The intimate changes observed during a child’s treatment therefore are too easily explained as a function of the treatment; while the danger implied in attempts to influence by means derived from clinical work the as yet unknown factors in the maturation of the child must be obvious. Thus the early possibility of basing a reconstruction of the child’s normal inner development on present clinical data and applying such premature syntheses to the philosophy and practice of education seems doubtful. But it will be as rewarding as it is time-consuming to apply child-psychopathological knowledge to research in “normal” childhood, i.e., the development and inner life of children whom neurosis has not isolated from the supporting field of group values.
II. The Initial Situation and Its Alternatives
Every psychotherapist has certain vague expectations in regard to what a disturbed child entering his room for the first time may be expecting of him and may do. Against this generalized picture the behavior of a single child stands out in its dramatic individuality.
Our young patient usually arrives hand in hand with his mother. He can be expected to have made a mental note of the fact that our office is in a “hospital-like” institution. On entering the waiting room he finds a friendly secretary and is then invited into an inner room about half of which (signified by “adult furniture”) is set aside for the therapist’s plainly non-medical business, the other half (signified by floor space and an array of ordinary toys) for a child’s play. He is told sooner or later that he is expected to let his mother withdraw to the waiting room and to allow the connecting door to be closed; the therapist and the toys are then to be at his disposal.
This situation confronts the young patient with a maze of conflicting possibilities. We would like to describe it as consisting of several overlapping fields of ambiguity which are created by the child’s relation to mother, therapist, toys, and inner conflict.
There is first of all his mother. He may hold on to her hand or body, insist on staying with her in the waiting room, demand that the door remain open, or stubbornly remain near the door which has closed between her and him. If he does this, the situation is for him still related mainly to one goal, his mother, and through her the way home from a vague danger. This idea, however, is rarely unequivocally pleasant. Our small patient usually has reached a deadlock with his mother, who cannot understand why he does not “simply drop” his problem; while the home atmosphere, in which he, in most cases, has been subjected to varying educational methods, has become charged with unsolved conflicts. Thus, frightened as he may be, he feels attracted by the doctor possibilities, the second field, and one which offers possible escape from the unbearable pressure of the domestic situation. Something which the mother or somebody else has said usually has created a slight hope in the child that the therapist may be a person who understands the conditions and the tempo in which a symptom of fear can be gradually abandoned without giving place to chaos within or more trouble without. Many a child has learned also to expect that he will be able to play for time by repeating to this new therapist what has satisfied the old ones. On the other hand the therapist has been called a “doctor” and the medical implications of the surroundings add to the mere strangeness of the situation and create the expectation in the child that some kind of surprise attack is to be made on his physical or moral inviolacy. The mother, with the best intentions, often transfers the negative aspects of the “mother field” into the field of doctor possibilities; she insists, for example, on reporting in the child’s presence latest developments, on admonishing, or even threatening him, or on trying to secure the therapist’s promise of diagnosis and advice. Literally and psychologically, therefore, the mother has to be referred to the waiting room; the child must feel that time has another quality in the doctor sphere, in which paradoxically, there is no hurry about getting well.
In the meantime, a third ambiguous field6 has competed with mother and therapist in dominating the child’s expectancies, namely the toys.7 For the child they open another haven, in which space too has another quality, and the therapist usually is quite glad to resign for a while in favor of this quasi-free sphere. Indeed, “what would we do without toys,” has become a common exclamation now that we have relaxed our efforts to ignore this most natural tool. The toys evoke in the child that remainder of playful explorativeness which his neurosis and the present doctor situation [have] not been able to submerge; and once he has started to select and manipulate, we can be sure that the temptation to play and to be the unquestioned and inviolable master in a microcosmic sphere will be great. However, we again see the child manifest hesitation. He has experienced too often the fact that the imagined omnipotence in the toy world only makes him feel his impotence the more keenly when he is suddenly interrupted. Playfulness does not rule until (and then only as long as) pressing purposes and fears have lost their compelling power. Thus the child often begins to play with hesitation, with selection, with one eye on the therapist or the door—but he begins to play.
Peace seems to reign. The mother is comfortably seated in the waiting room and has promised “not to go away”; the doctor has been diagnosed as a person who will not make surprise attacks on one’s bodily or moral reserve; the toys, sure not to question or to admonish, promise a time of “unpurposeful” play.
However, it is at this point that the most dangerous field of ambiguity—namely, the child’s reluctance to confess and his need to communicate his conflict—takes possession of the peaceful situation. Whatever it is that drives the child—an urge to get rid of some past or to prepare himself for some future, or both—the ever-present gestalt of the life task which has proved too much for him appears in the metaphoric representation of the microsphere. It is here that our “sign-reading” sets in, and that the tools which Freud gave us become indispensable; for they make us realize that in the playful arrangement which the child is driven to superimpose on the inventory of toys we offer him, he offers us an outline of the “inner maze” in which he is caught. Our small patients either show an anxious care in excluding this or that toy from their play or they work themselves toward a borderline where they themselves suddenly find their own doings unsafe, not permissible, unworkable, or unsatisfactory to the point of extreme discomfort. They cannot go on playing in peace—a phenomenon which we shall call play disruption.
I shall give a brief example of the place of such a play disruption in the four fields of ambiguity, governed as they are by the changing valences of the parent who is present, the therapist, the toys, and the shadow of inner conflict.
A girl of four still withstands toilet training. When put on the toilet, she seems unable to “let go”; later she soils her bed. Recently she was knocked down by an automobile; this has increased her inaccessiblity and her pale stubbornness. (As is obvious from her utterances at home, a small neighborhood dog is, at the moment, important in her phantasy life. It is female like herself, and not house-broken, and recently was knocked down by an automobile too; but unlike herself, it is frequently beaten for soiling, was badly hurt in the accident [it lost a leg]. This little dog apparently represents to her all that “is coming to her.”)
Very pale, the little girl has finally left her mother in the waiting room. She stands near the door of my room, sucking her finger, neither willing to play nor wanting to go back to her mother. I try to help her by outlining with some blocks a few rooms on the floor (an approach I use only on rare occasions). A little girl lies in a bed and a woman stands in the middle of the bedroom from which a door leads into a bathroom. There is a garage with a car and a man. After a while the little girl suddenly warms up, approaches with flushed cheeks and kicks the woman doll so that it falls over, closes the bathroom door and goes to the toy shelf to get three shiny red cars for the man in the garage. May we say she expresses a dislike for what must mean to her a mother in front of the little girl’s bed and for the demand of the open bathroom door; and that she shows a readiness to give whatever the cars mean to the man (father). At this point, however, she bursts into tears and anxiously asks, “Where is my mummy?” In panicky haste she takes three red pencils from my desk and runs out of the room to present them to her mother. Then she sits down beside her, pale and rigid, determined not to return to me. (The mother wants to give back the pencils, but she is told that the child is free to return them another time.)
The patient has scarcely reached home when she seems to feel guilty about having taken my pencils and shows signs of despair at not being able to bring them back until the next day. However, when the time for her next hour has arrived, she sits in the waiting room clutching the pencils in one hand, some unknown object in the other. She refuses to come with me. After a while it becomes noticeable that she has soiled herelf. When she is picked up to be led to the bathroom, the pencils fall to the floor and with them a little toy dog, one of whose legs has been broken off.
If we undertake to interpret this example properly, we would be led to consider in detail the patterns of guilt-feeling in this child: Having manifested aggression toward the woman in the play setup, she experienced the fear of the possible loss of her mother’s love; in hurrying to bring her an equivalent of what she had given to the man in the play, she happened to snatch objects which belonged to me, thus provoking a situation which would again ask for acts of rectification and which would imply an element of desire for punishment. (As if under compulsion to do or to allude to that which brings punishments, she held on to my property, brought the toy dog with a damage identical with her dog friend’s injury, and soiled in my room—transferring a “symptom” for which she had never been punished in a way either quantitatively or qualitatively equal to the hostility it expressed, as subsequently became apparent.)
What interests us here first of all is the traffic between the fields outlined above and the play disruption’s place in them. The little girl, moderately sure that her mother would not leave and somewhat loosened by the playful way in which the therapist approached her problem, got as far as to say in the language of play signs that she did not like the idea of the lady standing there near the open bathroom door but was willing to give the reddest cars to the man, when she must have experienced what Adam did when he heard God’s voice: “Adam, where art thou?” Her play suddenly seemed all-visible in the mother-field and she went to atone for her deed not, however, without stealing my pencils and thus innocently establishing a new goal in the doctor sphere. The trip home again increased the stubbornness against mother and bathroom demands and, consequently, the importance of the goal she had established in my sphere. The next day, back in my office and faced with the necessity and possibility of making everything come out even, she is caught by emotional paralysis, and her symptom expresses for her what she did not dare to express in her play; namely, the inability “to give” to an ambivalently loved person.
It is this very inability which in this case called for analysis and re-education. However, we shall have to resist the temptation to describe the little girl’s treatment at this point. Instead we concentrate on some further aspects of the described play situation.
We may call the toy scene on the floor microcosmic, i.e., an arrangement of small objects in such a way that their configuration signifies a configuration of conflicting forces in the child’s life, in this case the child’s retentive attitude toward her mother and her generous attitude toward the father. That the woman in the play really signified her mother (and that the man, perhaps, already indicated a father transference on the therapist) became plain when the microcosmic play was disrupted and she tried to rearrange another sphere in such a way that it represented a reversal of the “guilty” microcosmic configuration: she gave to her mother—and robbed me. Such rearrangements of the child’s relationship to the real persons or the life-sized objects present in the therapeutic situation we shall designate as macrocosmic. In this case the traffic from what we shall call, for short, the microsphere to the macrosphere implied a play disruption which, of course, is not always necessarily the case. Such a shift can take place as a playful expansion, perhaps with a transition from solitary play to a game, especially if another person is induced to play a role in the desired macrocosmic arrangement. (Using, for example, with an omnipotent gesture, a chair for a horse to ride on and to order about would be the macrocosmic play equivalent to the microcosmic form of making a toy rider hop along the floor.)
Beside the microcosmic and macrocosmic “spheres” of representation we can discern an autocosmic one: the sphere of dramatization by means of an interplay of body parts and organ systems. The little girl’s soiling belongs here: it was a symptom in the autosphere. There is also autocosmic play, i.e., the original play in the growing world of the child’s expanding body consciousness and the mutual enchantment of its parts.
The antithesis of play disruption is a phenomenon which we shall call “play situation.” If play “succeeds,” i.e., if it is not disrupted from within or interrupted from without, it has an effect on the child comparable to a few hours of good, long-needed sleep—everything “looks different.” I do not doubt that it is this autotherapeutic function of play which we are restoring in many cases by creating for a child regular and undisturbed periods of play, no matter how we rationalize what is happening during such a “cure.” In contrast to the little girl’s macrocosmic outbreak after the microcosmic disruption we sometimes see microcosmic play satiation lead directly into a macrocosmic play or game in which the rearrangement achieved in small dimensions is tried out (and this often too courageously for the child’s own anxiety) on big objects and people. I shall give here a non-psychiatric example of this normal phenomenon.
I once visited a boy of four a few hours after he had undergone an ear operation. He was, of course, most uncomfortable, insisted that many parts of his body hurt and that he wanted to urinate and defecate but was unable to do so. Three questions were most apparent in his complaints: first, whether or not the doctors were going to stick more instruments into him; second, why it was that only the doctor could remove the bandage around his head; third, whether his ear was still under the bandage.8
An understanding doctor had given him a roll of adhesive tape shortly before and he had held it, clutched in his hand, ever since. The tape was wound on a tin spool which fitted into a tin cylinder. Only one end of the spool could be inserted into the cylinder because the rim on the other end extended beyond the cylinder and served to fasten the two pieces together. The boy removed the spool from its container and suggested the following play: “You try to put this (A) into that (B)” (Figure 1). Accidentally I tried it the wrong way,9 whereupon he said with startlingly emphasis, “It’s much too big!” Since he kept repeating these words with a vague expression of pleasure, I cooperated by not accomplishing the deed, and by repeating my mistake over and over again, giving him the repeated opportunity to pronounce the magic phrase, “It’s much too big.” Each time I had failed to fit the spool and cylinder into one another, he took the two objects and, fitting them correctly, said with much emphasis, “Now it’s closed.” The repetition of this ritual of pretending that only he could stick A into B already seemed to influence his general condition considerably.
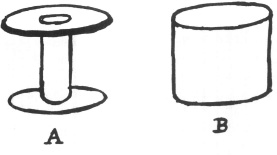
Figure 1
Suddenly he said, “Let’s pretend this is a leg and it’s sore.” He attempted to unwind the roll of adhesive tape, but found he could not separate the layers. Disappointed, he asked me to unwind it. I played that it was very difficult to unwind, whereupon he said with glee, “We need a giant for that.” I pretended to phone the nurse to send up a giant, then left the room and reappeared as the giant. However, I had a white coat on which made the play situation resemble too much the actuality (he was a patient expecting a doctor). He asked anxiously why the giant had an apron on. He quickly recovered, however, and, after the giant’s initial help, began to remove the tape from the spool (to which task, as had now been proved, only a giant’s strength was equal). Pieces of it were placed around the cylinder, which was now serving as the “leg.”
There was much joyful concentration on the completion of the “bandage.” But a few tiny spots of red inscription were not covered by the tape and he now concentrated on them. “Look! There’s a toe sticking out. And here is another toe, and another toe.” I asked, “Shall we put the bandages around the toes, too?” He replied enthusiastically, “Yes,” and put the tiny bandages over the toes. While doing so he began to sing and already felt quite cool. It was evident that he felt no pain.
When the entire surface of the cylinder was fully bandaged, the patient inserted the spool into it and taped over the whole configuration. “Nobody can take this off.” He asked his mother and me to remove the bandage, but, of course, “we couldn’t.” Whereupon he proudly repeated that, first, nobody but he could remove the bandage or the spool; that, second, he was not going to do it. Our “requests” were of no avail.
It will already have become evident to the reader that the patient arranged the play objects in such a way that they expressed in sign magic his active mastery over the situation victimizing him at the time. That only he could stick Object A into Object B, a pleasure provided by the nature of the toy (which, as we shall see, was subsequently bandaged), may have had a quite general meaning of mastery, although it may have already implied the more specifically satisfying idea that nobody (i.e., the physicians) could stick more objects into his head. The fact that he was obliged to wait until the physician was willing to remove his bandage was reversed by the game wherein only a giant could remove the adhesive tape from the spool and only the child remove the bandage from the cylinder (but would not do it). Finally, since he himself had covered the “toes” so carefully, he knew that these “extremities” were there and that he himself had covered them—an arrangement which might have been reversing the actual situation wherein the physician had covered his ears and would not allow him to see whether or not they were still there.
After approximately half an hour of such play the patient was smiling and singing. He fell asleep after I left. When he woke up again, he smiled mischievously and said to his mother, who was sitting beside his bed, “Let’s put some bandage over the doctor’s eyes when he comes in; let’s put it all over him. The big bad wolf—only then we wouldn’t have enough bandage left if Charlie10 hurts his leg.”
Leaving aside the last “altruistic” remark in which the patient already visualized a time when he might be providing bandages for his brother (who had by then become the medical victim), we see in the remark about the doctor being covered all over by the bandage a typical omnipotent rearrangement in phantasy of the macrosphere in accordance with a previous microcosmic rearrangement. First, only the patient could make and remove bandages, and now the doctor himself becomes the victim of bandaging to a degree (“all over him”) surpassing the discomfort he had created for the child.
This wishful and wileful restructuralization in play of the child’s most immediate sphere of discomfort uses, of course, all the mechanisms which Freud showed were governing factors in play, in his classical example of a boy who had to adapt to his mother’s absence:11 the working over of an experience in which one had been a passive victim by its representation in such a way that one becomes the active aggressor against a toy or a partner. As for microcosmic play, the traumatic experience is caught in a small and simple configurational frame (an accessible Beutefeld), and is to be reprojected in its all-too-simple formulation into the bigger world, which consequently becomes a macrocosmic play-and-error field for microcosmic theories.
In the little girl’s case the microsphere represented “a family”; in the case of the hospital patient, endangered parts of the body, ear, head, etc. Thus a variety of segments of the pressingly immediate life situation may be projected into this least refractory of all spheres of representation. A child concerned about “the body as a whole” or even about “life as a whole” may build corresponding configurations both as wishful arrangements and as traumatic repetitions. Illustrations of this will follow.
Of special interest is one of the intermediate steps between the spheres of representation, namely, behavior with extensions of the autosphere. Play belongs in this category wherever it is clear that an isolated object is used as a means to extend or intensify the mode of expression of an organ or an organ-system and does not become a part of an extrabodily microcosmic arrangement. Let us say a block, if replacing the finger as an object of licking, is a part of an autocosmic extension; it would still be one if rhythmically banged against another block, while it would become a part of a microcosmic arrangement when, with consideration for its physical laws and its usual connotation, it is placed on another block so that together they may form a building.12
These spheres of representation and dramatization can help us where it is advisable to neglect social connotations, such as what is considered to be a play act, a serious deed, a habit, a symptom, etc., and to find instead in corresponding configurational properties the common denominator for the various parts within the complicated unit of a clinical contact. Our girl patient, for example, manifested the quandary of cooperative retention and elimination on the one side and hateful retention and ejection on the other (plus their relationship to mother and father) in all the three spheres mentioned.
As for the traffic between these spheres of representation we observe that just as an organ, the whole body, a family constellation, or a conception of life as a whole can be represented by a microcosm, so sucking, banging, defecating, etc., when they are prolonged habits, can often be understood as dramatizing social situations and attitudes.
We will readily see that especially for the disturbed child from three to six years old (the age range in our study) autocosmic manifestation leads back easily into the sphere of regressive habits, while macrocosmic expansions make the child try out the environment in a manner both surprising and displeasing to attending adults. There remains then, by force of age preference and expediency, the microsphere as a haven for overhauling the boats before taking further trips into the unknown. Our disturbed children approach this sphere, break down or hesitate before they reach it, experience a disruption in it, or suffer a belated disruption after having over-estimated the omnipotence provided by it. The “sign-magic” used during such behavior seems to us to outline where in the child’s life the sphere of relative tolerance borders on the danger sphere of unbearable pressures.
Among such manifestations, that of extrabodily representation of organ modes, which is the subject of early and special environmental interference, is of outstanding importance for the understanding of preschool play and also for that of all emotionally disturbed older children.
As diagrammatically developed in a previous article (2), the orificial organ-modes incorporation, elimination, retention, and intrusion and the body apertures which are their “models” par excellence—namely, mouth, sphincters, and genitals—are combined to normal mutual emphasis in successive stages, namely, the stages described by Freud as pre-genital. In each of these stages there is an interrelation between the sensitization and training of a vital orifice and the growing periphery of mastery (a) oral-(respiratory)-sensory-tactual, (b) anal-(urethral)-muscular, (c) genital-(urethral)-motor. This interrelation can express itself in mode-behavior both centrifugally as generalization of the mode, i.e., the mode of the dominant zone becomes the dominant mode of behavior in general, or centripetally as a specialization of the zone (i.e., a general tendency can express itself in the habits of one zone). For example, the retentive mode may first find emphasis in sphincter-habits and then appear as a general retentive tendency in many aspects of behavior; or it may become noticeable in other habits (such as keeping food in the mouth and neither swallowing nor returning it) and then find its most intensive expression in sphincter-habits. We thus can speak of mode-fixations and of zone-fixations, the first being a carrying over of one mode from its model-zone to other zones where it is as it were a gesture without functional logic or in the use of one zone for several untimely and displaced modes. Some of these generalizations and specializations are only observable in a limited number of temporarily or permanently fixated children.
“Surveying the field of zone experience and mode manifestation, one finds that what Freud had described as pre-genitality is the development through a succession of narcissistic organ cathexes of impulses and modes of behavior the final integration of which implies all the possible relationships of a body and an object and thus the basic spatial modalities of experience. Led (or confused) by zone experience as well as growing capacity children experiment more or less playfully in space with all the possible relationships of one object to another one and of the body as a whole to space.” To modes which in their bodily, spatial, or social expression are curtailed by inhibiting experiences “the organism offers a limited range of safe displacements in habits and minor symptoms. Reality allows for certain systems of subjectified perception; society permits a number of odd social habits and, more or less queer traits. To the child especially the world of play affords opportunity to experiment with organ-modes in extrabodily arrangements which are physiologically safe, socially permissable, physically workable and psychologically satisfying.”
Between displacements within the body (habits, symptoms) and the free external displacement in play, we find various arresting combinations. The following example, a previously published (2) nonpsychiatric observation, illustrates the way in which the dominance of simple organ-modes during training may for a while govern a child’s spheres of behavior. A little boy, H, two and one-half years of age, who struggled rather belatedly against enuresis, began to take to bed with him little boxes, which he held closed with both hands. When a box opened during the night, sometimes apparently with his unconscious help, he would cry out in his sleep or awaken and call for someone to help him close it. He would then sleep peacefully, even though not necessarily dry. But he continued to experiment.
During the day he looked around for suitable boxes—obviously driven by an urge to materialize an image of “closedness.” Finally he found what seemed to fit the image, a cardboard cylinder which had been the center of a roll of toilet paper. He put two cardboard caps from milk bottles over the openings of the roll. All through the night he would try to hold this arrangement firmly together with both hands—as an animistic guardian of the retentive mode. But no sooner had his training achieved a relative success in closing his body during sleep than he began, before going to sleep, to throw all available objects out of the window. When this was made impossible, he stole into other rooms and spilled the contents of boxes and bottles on the floor.
Clearly, the first act, namely holding a closed box as a necessary condition for sleep, resembles a compulsive act originating in the child’s fear of failing to retain because of his weakness or because of his wish to expel. Emptying objects, on the other hand, or throwing them out of the window is “delinquent” and the result of the fear of being overpowered by the claims of society to which he surrenders the zone but not the impulse. The impulse appears on other levels of representation, where it betrays itself through configurations representing the retentive and eliminative modes.
To prevent the little boy from throwing things out of the window, it was opened from the top. Thereupon he was found riding on it, leaning out into the night. I do not think he would have fallen out; he probably wanted only to show himself “master of openings,” as compensation for the surrender of the free use of his excretory openings to society. When, in consequence, his mother kept his window closed until he was asleep, he insisted that the door be left ajar.
Thus not only sections of one’s body and toys, but also the body as a whole in its spatial relationship to the whole room or to the whole house, may serve the displaced expression of the impulse in various degrees of compulsive, naughty, or playful acts.
The animal psychologist, having seen rats (whom he had made hungry) learn to run mazes (which he had built) toward food (which he had put there) comes to the conclusion that “the environment takes on for the physiologically aroused organism, by dint of his innate endowment and past experiences, the character of a hierarchy of to-be-sought and to-be-avoided superordinate and subordinate objects” (15).
Essentially, our diagnostic confidence is based on the same expectation, which, however, is derived from the repeated clinical experience that the hierarchy of actually sought-after and avoided toys (offered as stimuli and supports) allow us to draw conclusions in regard to what has aroused or is arousing the playing organism physiologically and what has happened to it environmentally. That we cannot consider play an intermission or a vacation from urgent life but rather a continuation of it on a sign level is only our serious adaptation to the serious way in which (given our therapeutic setup) the child behaves with strict selectivity, creates meaningful sign coherence, and by his emotions betrays a “purpose” where “play” has been suggested.
In describing to the reader, by way of introduction, some of the significant alternatives with which the child is faced on entering the therapeutic situation, and some of the therapist’s useful expectancies, we by no means hope to induce him to share what may seem a radical determination. Illustrations can only convince him who already believes that those selected are representative. Therefore I can close this introduction only with the rather inhuman suggestion that a publication like the present one should be read at least twice. Only after the comparison of several cases has made the reader more familiar with the nature of the inventory of possible kinds of behavior from which the individual child makes his choices will he begin to believe that even if presented with different supporting objects the individual child patient could not have produced configurations essentially dissimilar to those which are described in the following pages.
III. Studies in Play Interpretation
A. METHOD OF REPRESENTATION
Our material is divided into contacts (visits), which in turn consist of behavior items. These items are described and discussed in five categories, A, B, C, D, E, which indicate the shifting foci of the analytic attention; their peripheries overlap.
A gives a commonsense description of what happens before the observer’s eyes; B and C demonstrate (in slow motion, as it were) two concurrent tendencies in the observer’s mental activity: B is directed toward a future exact description in areas which can also be explored and measured under other than psychiatric conditions; C toward the clinician’s age-old right and duty to allow himself to be led by subjective factors. The reader should visualize the relationship of B and C and their intervention between A and D in the following manner (Figure 2).
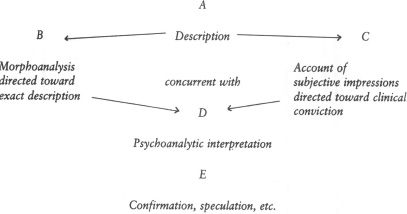
Figure 2
“A”
The “behavior item to be analyzed” represents as nearly as possible the span between the moment when we observe that the child has turned his attention to a toy, a person, or a conversational manner and the moment when we notice that he turns to the next one. This is, of course, a crude concept of an “observational unit”; however, it is the one naturally used in a therapeutic situation in which the task is to infer from the selective attractions and aversions created by a standard environment what the patient’s relationship may be to certain classes of ideas and thus to discover the pathogenic associations of his mind—which he may keep hidden, which may be unconscious to him, or whose reference and importance may not be understood by him.
“B”
Morphoanalytic description emphasizing the configurations manifested in four areas of behavior:
1. Affective: The patient’s manifested emotional interest in and withdrawal from the object of the behavior item.
2. Ideational: Verbalized content, acted out themes, etc.
3. Spatial: Configurations and modes in the three spheres of representation.
4. Verbal: Mode of expression; speech, voice.
“C”
Observer’s Impressions, Associations, and Reflections. While in B the therapist attempts an approximation of objective configurational analysis of what he sees and hears in the currently manifest, in C he gives impressions (“it was as if . . .”) and associates past impressions—previous observation on the child in question or on other children, data communicated to him by the parents, etc.—and he reflects on latent possibilities, i.e., the possibility that his associations may correspond to a genetic or associative connection in the child’s mind between what he is doing under the observer’s eyes and what he is said to have done in other situations.
“D”
Psychoanalytic Interpretation.
1. His observational and reflective reactions lead the observer to various interpretational hints. A symbolic equation or metaphor may make it possible to recognize a play act as alluding to and standing for an otherwise manifestly avoided item (person, object, or idea); or a play arrangement may prove to represent a specific effort on the part of the child to rearrange “in effigy” his psychological position in an experienced or expected danger situation. Such an arrangement usually corresponds to the child’s defense mechanisms (6).
2. If these first hints survive the sifting processes of further observation and investigation, they will sooner or later grow together and create a conviction and an image in the observer’s mind in the form of the reconstruction of a genetic sequence or of a dynamic configuration pertaining to the patient’s inner or outer history.
3. The observer may proceed to convey parts of these reconstructions to the child whenever he feels the time has come to do so. This, then, is the therapeutic interpretation.
“E”
Confirmation of interpretation gained after the contact, and further speculation reaching out beyond the evidence offered by the behavior item.
B. A SIX-YEAR-OLD BOY’S SECRET: JOHN
The observation of the first of our “specimens” led to the discovery of a later verifiable fact, namely, a conscious secret kept hidden from the therapist (and his predecessors) by both the child patient and his mother.
John is six years old and a sailor’s child. Years of psychiatric investigation have failed to throw light on his impulse to soil himself when overcome by a strange state of rage and sexual excitement. This infantile habit in its importance for the environment has remained the center of a general emotional arrest and of a system of petty delinquency. The mental test shows traces of disintegration and extreme fatigue rather than retardation in his only slightly subnormal intelligence. When he is brought to my attention John is at a hospital where he has undergone (with negative results) an examination of his eliminative organs and an encephalogram; he has also been circumcised. Thus unlike all the other patients to be presented here, John is not brought by his mother. On the contrary (and this is a variation of our model “field situation”), the way back to his mother leads through a successful relationship with me, knowing, as he does, that I will have a word in the final decisions as to his placement, further treatment, etc.
The day before the first regular contact, John had been casually introduced to Ps.13 He had a toy gun in his hand and a dagger at his side and had exclaimed, “I am a cop.” When asked, “Who are you going to shoot?” he had replied, “The bad guy.” “Who is the bad guy?” “Me.”
Today Ps brings him some Plasticine because he was told that John had been sad about the fact that none of the hospital toys were “his own.” Ps therefore expected John to spend valuable time on the question of which of Ps’s toys he would be allowed to take to his room, a common technical problem which can be solved only from case to case and often is of diagnostic value in itself. However, Ps did not want to lose any time in this instance and assumed that once the ownership of the play medium was settled Pt would concentrate more quickly on whatever he needed to express. Ps also considered Plasticine to be a fitting “support” for the phantasies of a child who soiled and played with feces.
1. First Contact
John appears, armed again and looking pale, forlorn, and somewhat scared; he accepts the Plasticine with surprised eagerness but without thanks, and immediately concentrates on making an “aeroplane,” which, as he says with a shy smile, “brings people from across the ocean.” This smile quickly gives way to serious concentration, during which he ignores Ps for a while.
“A”
BEHAVIOR ITEM TO BE ANALYZED
Plasticine: Balls
John makes small balls of Plasticine.
With three blocks he builds a grocery store.
“You are the grocery man; I am a truck driver.” John fills the truck with the balls and then, elaborately and with a “motor noise” approaches the store, finally dumping the truck’s contents into a corner. When asked, “How much does the grocery man owe you?” John refuses payment (as if the delivery represented a present to the grocery man). This is repeated.
Suddenly he calls one Plasticine ball mother nut. Then he takes a smaller ball of the same color and calls it baby nut. He then makes of another color Plasticine a long row of balls equal in size to the first one and calls them brother nuts. “Whose brothers are they? “My mother’s brothers.” “You mean uncles?” John becomes very pale, sways as if he were going to faint, and leaves the room hurriedly.
After a while he comes back, obviously from the toilet for he refers to his general state with the words “This is the way I feel when I soil.” Ps asks once more, “Now tell me, who are your mother’s brothers?” John, with a desperate look, “Me.”
“B”
MORPHOANALYSIS OF MANIFESTED CONFIGURATIONS
1. Affect as manifested in interest and withdrawal: The interest in the Plasticine is first one of hungry taking into possession. Then follows a short period of quiet play concentration out of which suddenly emerges the idea for a game. The expression increasingly becomes one of eagerness to play in cooperation with Ps and to play at giving him something. At the height of this contact-seeking the phantasy of the nut family appears. Some implication of this phantasy then brings about a sudden and vehement play disruption; an anxiety attack and the symptom of sudden defecation make an end to play and game. (What is the dangerous implication of the nut family phantasy?)
2. Ideational content: (a) Balls are being made; (b) groceries are delivered without pay; (c) a nut family is represented which consists of a mother, a baby, and many “brothers.” (What relation is there between balls, delivery, and the members of a family?)
3. Spatial expression: After having put aside his weapons and prepared the balls, Pt seeks intimate spatial contact with Ps, trying to win him for a game in which they concentrate together on the microcosmic elaboration of Pt’s phantasies. This game is dominated by the configuration of delivering and dumping. After the disruption the autocosmic sphere takes the lead and the patient defecates.
It will be seen that the microcosmic play and the autocosmic symptom have in common the eliminative mode, the difference being that the balls are dumped as presents in the context of a general contact seeking, the feces eliminated in anxiety, followed by a general closing up. (What is to be delivered in friendliness, what retained in anxiety?)
4. Verbal expression: (a) There is probably more than one meaning in the “nuts” which he delivers, the most obvious being that the family he has in mind is “nuts”; (b) the “me” the day before manifestly expressed the “turning against himself” of the weapons originally intended for “bad guys.” Today it turns my questions in regard to the uncles back to him. (Bad uncles in a crazy family? Who are they?)
“C”
IMPRESSIONS, ASSOCIATIONS, REFLECTIONS
John, apparently too starved for gifts to smile or express thanks, accepts the Plasticine the way a hungry man reaches for food. (This “aeroplane bringing people from across the ocean” could be equally well associated with either John’s absent sailor father or Ps, whose accent indicated he had come from far away. Is this the beginning of a transference, i.e., does this express the need for a father?)
John had been described to Ps as a very friendly, accessible, and even voluble boy who craved for a good contact, especially with men. However, at a certain point he would always close up without any real understanding having been reached. When would he close up in the game with the balls which seemed to mean more and more to him as he proceeded?
He made balls, then seemed very eager to play in cooperation with Ps and to deliver something to him, a mode underscored by the refusal of payment which would naturally belong to the commercial play content. This “delinquent” boy who steals and hides what belongs to others and does not even give his feces at the requested time wants to deliver something to Ps (a father substitute?).
The nuts turn into a family, a mother, and a baby. Is he homesick? One automatically expects next a father and a brother (to complete approximately the actual family constellation), but John lets about fifteen “brothers” follow who are different in color. The number makes Ps suspicious and asks who they are. The answer, “mother’s brothers,” could still mean, for example, the many brothers which he expects his mother to produce now that she has started on that line. To make sure which kind of brothers he means, Ps gives him the term for a mother’s real brothers.
The word “uncle” seems to hit him like a blow, causes panic with organic symptoms, including the urge to defecate, and ends the game. “Uncles,” of course, is not always a correctly used term, and the “different color” suggests that these uncles may not be real relatives, may be outsiders, strangers—John’s father is a sailor and the mother has many nights without a husband.
After the disruption and John’s return from the toilet, he had answered Ps’s last question with “me”—just as he had done that day before when asked, “Who are you going to shoot?” In other words, when asked about the subject of admitted aggressive tendencies, Pt had evaded the issue by putting himself jokingly into the role of the “guy” whom he wanted to harm. Today, in a much more serious way, he acts as a victim (internalizes somatically) when asked for the identity of somebody who is characterized as “mother’s many brothers” who in the play family appear in the father’s place and cause panic when called “uncles” If our reflections point in the right direction, John has been made the victim (and has gone on making himself a victim) of an unbearable secret which he does not dare convey, namely, his mother’s infidelity or maybe prostitution.
As to our expectation that in John’s handling of the clay we would find expressed something of the retentive-eliminative problem which builds the basis of his main symptom, namely his untimely elimination of feces: We see him all-giving where he plays in delivering the clay balls, apparently unconsciously “giving away” more than he wanted to. Then he tried to close up—and defecates (just as the little girl above had done when deciding to hold on to the pencils). As for the fact that the patient’s eliminative system has become the means of expressing ambivalence, constitutional and historical factors will have to be considered. From the anamnesis one fact suggests itself: John was hard to train and his mother beat him often. When, as we assume, he was a witness to his mother’s infidelity, i.e., saw her do “dirty” secret and sexual things herself, it is conceivable that he was overcome by hate against the deceitful M out of love for whom he had fought himself in an effort to become clean, asexual, and truthful. However, more important at this moment than any reconstruction is the recognition of the conscious factors which block the access to the Pt’s confidence.
“D”
PSYCHOANALYTIC INTERPRETATION
1. Symbols, (a) The balls (dumped in playful cooperation) correspond in consistency and mode of use to feces (which he ejects in anxiety and anger), (b) The balls (“mother nut,” “baby nut” on the one side, many “brother nuts” on the other) correspond in their most obvious differentiations—namely color and number—to a traumatic family constellation (mother and baby on the one side, many strangers on the other).
2. Defensive arrangements: The two sets of symbols correspond to the two main problems (both eliminative-retentive) of the therapeutic situation: (a) to the symptom which is to be removed; namely, the untimely elimination of feces; (b) to the first requirement for its removal, namely, the giving away of the mother’s secret, which John has succeeded in keeping isolated from all therapeutic confessions made during previous treatment. That Ps, instead of asking embarrassing questions, has brought John a present and plays with him probably increases the (conscious) feeling in John that to be fair with Ps he should verbally deliver the secret and thus make the first step toward a new life in which he would learn to retain his feces. For various reasons, some of which will be made apparent only by further analysis, the patient first resists the overwhelming need to deliver his secret. His defenses are: (a) to use the play support offered by Ps for the substitution of the delivery of the secret with a delivery in a game. This defense fails when the patient’s conversation unconsciously gives away a hint by delivering the strange nut family, (b) Noticing this, he uses his second and usual defense; he closes up, as far as the secret behind the hint is concerned, while the eliminative urge expresses itself at its original zone, the eliminative organs. As this happens the conflict between the eliminative and retentive modes and his masochistic tendency to express aroused emotions in a regressive, autocosmic, and punishment-provoking way get the better of him.
3. At the end of this first contact, Ps makes only an intentionally vague statement to Pt, for which the latter thanks him with a smile. More cannot be done, since it remains necessary to disclose what may be proven to be fact in these “communications,” in this case a too delicate investigation with which to burden a child. If the information proves correct, the mother has to be urged to give John permission to talk about all his experiences, including those involving her. Only then can we decide how “deep” we have to go to locate the possible damage to John’s inner defenses.
“E”
CONFIRMATION AND FURTHER SPECULATION
During Ps’s next conversation with the patient’s mother, she confessed that there were certain episodes she had urged John not to tell the doctors about, and had added, “Daddy surely would kill me if he heard about it.” She asked for psychological help for herself and released John from the promise of secrecy which had blocked previous therapeutic efforts.
The following rudely clinical excerpts from a previous publication (2) may serve to characterize John’s further treatment.
The first barrier which psychoanalysis was forced to attack was the castration fear, which, after the circumcision, had suppressed his soiling without sublimating the impulse. Expecting new physical deprivations, the boy would continue to appear equipped with two pairs of eyeglasses on his nose, three knives on a chain hanging out of his trousers and a half dozen pencils sticking out of his vest pocket. Alternately he was a “bad guy” or a cross policeman. He would settle down to quiet play only for a few moments, during which he would choose little objects (houses, trees and people) no larger than two or three inches high, and make covers for them out of red Plasticine. But again and again he would become very pale and ask for permission to go to the bathroom.
In describing an automobile accident he had witnessed, in which the chief damage was a flat tire, John almost fainted. He felt equally sick when I asked him about certain sleeping arrangements. It appeared that he had seen (in crowded quarters) a man perform intercourse with a woman who sat on him, and he had observed that the man’s penis looked shorter afterwards. His interpretation of this had been entirely anal. Maybe the woman, whose face seemed flushed, had defecated into the man’s umbilicus and had done some harm to his genitals. Or the man had, as it were, eliminated a part of his penis into the woman’s rectum out of which she later would deliver, i.e., again eliminate, the baby. In addition to the enlightenment given that semen and not a part of the penis remained in the woman, the circumcision was talked over and reassurances given for the more important remainder of his genitals.
His first concentrated skillful and sustained play was the following: A caterpillar tractor slowly approached the rear end of a truck, the door of which had been opened. A dog had been placed on the tractor’s chain wheels in such a way that he was hurled into the truck at the moment the tractor bumped into it. Obviously he wanted to make sure by experimenting with his toys that the pleasant idea of something being thrown into another body without hurting either the giver or the receiver was sensible and workable, although his unresolved anal fixation (no doubt in cooperation with certain common “animalistic” tendencies and observations) did not allow him to conceive of intrusion in any other way than from behind. But it was not as before brown stuff or mud which was thrown, it was something living (semen).
Outside the play hours, the eliminative impulse made its reappearance in John’s life in macrocosmic fashion. The whole house, the whole body, the whole world was used for the representation of an impulse which did not yet dare to return to its zone of origin. In his sleep, he would start to throw the belongings of other people, and only theirs, out of the window. Then, in the daytime, he threw stones into neighbors’ houses and mud against passing cars. Soon he deposited feces, well wrapped, on the porch of a hated woman neighbor. When these acts were punished, he turned violently against himself. For days he would run away, coming back covered with dirt, oblivious of time and space. He still did not soil, but desperation and the need for elimination became so all powerful that he seemed to eliminate himself by wild walks without any goal, coming back so covered with mud that it was clear he must have undressed and rolled in it. Another time he rolled in poison ivy and became covered with the rash.
When he noticed that, by a slowly narrowing network of interpretations, I wanted to put into words those of his impulses which he feared most—namely, elimination and intrusion in their relationship to his mother—he grew pale and resistive. He began a four-day period of fecal retention, stopped talking and playing, and stole excessively, hiding the objects. As all patients do, he felt rightly that verbalization means detachment and resignation: He did not dare to do the manifest, but he did not want to give up the latent.
He did not live at home at this time. After many weeks, he received the first letter from his mother. Retiring to his room, he shrank, as it were, physically and mentally, and soiled himself. For a while he did this regularly whenever his mother communicated with him. It was then possible to interpret to him his ambivalent love for his mother, the problems of his bowel training, and his theories concerning his parents’ bodies. It was here also that his first free flow of memories and associations appeared, allowing us to verbalize much that had been dangerous only because it had been amorphous.
One day he suddenly expressed the wish to make a poem. If there ever was a child who, in his make-up and behavior, did not lead one to expect an aesthetic impulse, it was John. Nevertheless, in a flood of words, he now began to dictate song after song about beautiful things. Then he proposed the idea, which he almost shrieked, of sending these poems to his mother. The act of producing and writing these poems, of putting them into envelopes and into the mailbox, fascinated him for weeks. He gave something to his mother and it was beautiful! The intense emotional interest in this new medium of expression and the general change in habits accompanying it, indicate that by means of this act of sending something beautiful to his mother the eliminative impulse had found a higher level of expression: the zone submitted to training.
C. A NEUROTIC EPISODE IN A GIRL OF THREE
The second case should bridge to some extent the short and all too “obvious” first and the longer and very complex third examples. Among the writer’s Boston notes, he finds the following encounter with a charming but badly scared little girl who was friendly enough to provide a basis for diagnosis in two contacts. We shall call her Mary.
The complaint was that shortly before her third birthday Mary had developed nightmares during which she struck about wildly; at about the same time, after a dozen visits to a play group organized by a group of mothers in a suburb, she had been overcome by violent anxiety attacks with uncontrollable crying. An attempt had been made to let Mary’s mother stay in or near the nursery, but this arrangement had helped only temporarily. The routine situations of afternoon rest and going to the toilet seemed provocative factors in the outbreaks of anxiety.
It must be noted however, that Mary had no attacks during her first visits to the play group, although she showed some tenseness and some rigidity of posture and behavior. When the attacks began, the play group leader as well as the mother felt that something in the nursery must have frightened her. We shall concentrate on the way this complicated something was revealed during the first two contacts with me.
1. First Contact
Mary, dark-haired, attractive, is slight but well built. Her walk is somewhat stiff and her handshake rigid, but she seems well coordinated.
“A”
MOTHER
Holds mother’s hand as she enters office. When she shakes hands with Ps, she gives him a brief smile, then immediately turns her head away and from then on tries not to look at him. She turns to her mother, puts arms around her, and keeps her near the open door. While M tries to encourage her to look at the toys, she closes her eyes tightly, hides her face in M’s skirt, repeats in a babyish voice, “Mommy, mommy, mommy.”
“B”
I
1. After a short glance into the room and a very short and slightly coquettish contacting of Ps in whom M tries to interest her, Mary withdraws to her mother.
2. Spatially keeping near the open door, she clings babyishly to M’s body (adherence) as if she wanted to hide in it, and excludes Ps to the extent of closing her eyes very tightly so as not to see him (encasement). No selectiveness in regard to the toys is evident.
“C”
I
She first looks at me as if she wanted to see whether or not the new adult is going to understand fun. However, this feeler is quickly withdrawn; her flight to her mother seems somewhat dramatic. I am not sure that she is not hiding a smile. It seems that she did not show any similar reaction either to the secretary or to a lady who spoke to her in the waiting room; the first impression is that she is conscious of my being a man (doctor) and that there is a coquettish element in her behavior.
“A”
II
MOTHER AND DOLL
Pointing to a (girl) doll, Mary asks M several times, “What that, what that?” After M has explained that it is a dolly, Mary repeats in a babyish way, “Dolly, dolly, dolly,” and suggests in words not understandable to Ps that M take off the dolly’s shoes. M tries to induce her to perform this act herself, but Mary simply repeats her demands again and again without listening to M.
“B”
II
1. Her interest in the doll is not able to overcome her reluctance to play; she makes her mother play.
2. The content: Mother dresses, undresses a girl doll’s feet.
3. Thus Mary draws the doll into the mother adherence.
4. Her speech remains babyish, repetitious.
“A”
III
INTERRUPTION
M begins to feel embarrassed since the hour is assuming the character of an observation of her in her play with Mary. She asks, therefore, if it is not time for her to leave the room and to wait outside. Ps approves of her decision. Mary does not show any signs of fear when, the adherence to M being thus broken up, she suddenly finds herself without anybody to lean on.
“C”
III
Mary showed the same initial lack of anxiety when left by M in the nursery school. It seems either that something specific must happen to provoke manifest anxiety or that her anxiety typically remains latent for a while.
“A”
IV
DOLL
M has left the doll in Mary’s hand. Mary grasps it firmly around its legs. Suddenly she smiles mischievously, her face flushes, and she begins to touch various things in the room with the doll’s head. When a toy falls from the shelf, she laughs and begins to push smaller toys, always with the doll’s head, in such a way that they fall too. Her excitement increases, manifested by chuckling and laughter. With special glee she pushes (with the doll’s head) a toy train which is on the floor in the middle of the room. As one car overturns, she overturns them all. But then she suddenly stops and becomes very pale.
She leans with her back against the sofa, holds the doll over her genital region and drops it on the floor. She picks it up again, holds it over the same region, and drops it again. While repeating this from ten to fifteen times, she begins first to whine, then to cry, finally to yell, “Mommy, mommy, mommy.”
(M, sure that the game is up, enters room to take Mary home.)
“B”
IV
1. The sudden hilarity and blushing aggressiveness immediately enter into a dramatic curve of quickly increasing excitement. This likewise suddenly reverts to pale inhibition and overt anxiety. Her blind screaming contacts her mother and restores the mother adherence.
2. The discernible content has been: Pushing and throwing down of things, not with her hand but with an extension of her hand; the dropping from the genital region of a doll (which before, as an extension of the hand, had been, as it were, a pushing tool).
3. Spatially, after the physical adherence to M is made impossible, the child turns in a diffused way to the room at large and to the small toys in it. Her play is of the autocosmic extension type with the doll used as an extension of the pushing hand. Only in pushing the train does she approach a possible microcosmic theme (train accident); whereupon she withdraws to the periphery of the room where she dramatizes the loss from the genital region of the doll which had been an extension of the aggressive hand. Paralysed by anxiety, she then contacts her mother, who leads her out of the conflict situation.
4. Corresponding to this aggressive and regressive behavior, her loud communication changes from coquettish chuckling to excited laughter, to pale silence, to anxious whining, to desperate screaming, “Mommy, mommy, mommy.”
“C”
IV
The doll in Mary’s hand is used in such a way as to appear that she does not dare touch or push the objects with her bare hand. One is reminded that in the play group her strange way of touching and lifting things (“never with the whole hand”) was observed. This and a certain rigidity in the extremities suggest that Mary is (constitutionally or traumatically) disturbed in the manipulative and locomotor sphere.
The way in which she then seems unable to stop her own dramatization of something dropping from the genital region reminds one of the interpretation given to certain hysterical (grand mal) attacks in which the patient is supposed to represent both partners in an imagined scene, namely, the victim and the aggressor in a sexual act. Here it would be the robbed and the robber. Literally, the dropping of a doll from between the legs suggests “birth.” The half-sitting position she assumes when dropping the doll suggests a “toilet situation.” Birth and toilet situation have in common the “dropping” of (valuable) bodily content. While we know nothing about the events of Mary’s toilet training period, it seems that in the nursery the toilet situations were factors in the outbreak of her anxiety. Finally the association with “extension” (and pushing?) suggests that she may be dramatizing the fact that she has no penis. It is most probable that on entering the nursery school Mary was given her first opportunity to go to the toilet in the presence of boys and to see boys’ genitals. Is this the “loss” which she indicates?