Chapter 11
Global burden of disease
Terminology
In this final section of the book we describe the epidemiology of diseases in the world. We look at the burden of non-communicable and communicable disease at the global, European, and UK level. These estimates are limited by measurement difficulties, but we present both mortality and a composite measure of morbidity and mortality, the disability-adjusted life year (DALY).
The DALY is a measure combining years of life lost due to premature mortality with years of life lost due to time lived in poor health. It was developed for the World Bank and is now widely used by WHO and other global institutions to compare the health burdens of different diseases across the world:
(where YLL is years of life lost, YLD is years lived with disability).
1 DALY is a year of perfect health lost. Diseases that cause long-term disability, such as mental health problems, may lead to a large proportion of DALYs without being major causes of mortality.
Further reading
Murray CJL, Lopez AD (eds) The Global Burden of Disease. Cambridge, MA: Harvard University Press on behalf of the World Health Organization and the World Bank; 1996.
WHO. The Global Burden of Disease: 2004 Update. Geneva: WHO; 2008.  http://www.who.int/healthinfo/global_burden_disease
http://www.who.int/healthinfo/global_burden_disease
Global burden of non-communicable disease
Non-communicable disease is the major cause of mortality in high-income countries, and its importance is growing in middle- and low-income countries as the control and treatment of infectious disease improves. This shift from a predominant infectious disease burden to non-infectious conditions is known as the ‘epidemiological transition’.
Mortality
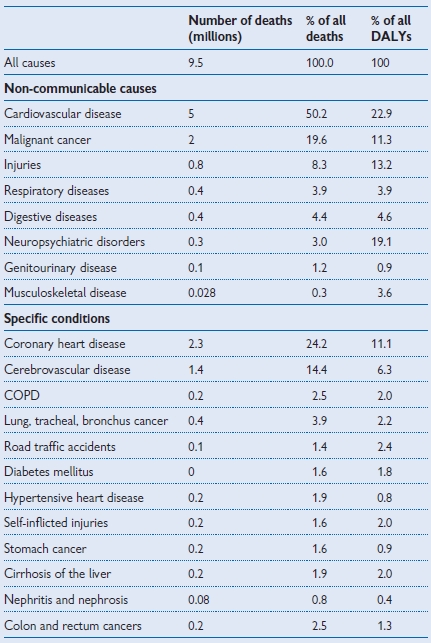
Globally non-communicable diseases are responsible for 59.6% of deaths. Cardiovascular disease is the leading cause of death, responsible for 17.1 million deaths a year1 (Table 11.1); the distribution of chronic disease deaths in Europe is shown in Table 11.2.
Morbidity
The burden of chronic disease morbidity is also high and people are often affected for many years. However, many conditions can be prevented or ameliorated by lifestyle changes including smoking cessation, weight loss, and physical activity (see pp.60–63).
Although low- and middle-income countries experience most of the global burden of infectious disease, almost half of their burden of disease is caused by non-communicable conditions. The burden of non-communicable disease in middle- and low-income countries is increasing as the prevalence of high BP, high serum cholesterol, smoking, and obesity increases.
Overall burden
When DALYs are used to estimate the overall burden of disease, a number of conditions that are rarely fatal become much more important. For example, mental health problems represent a huge burden of disease while not contributing much to overall mortality.
Inequality
The risk of developing a non-communicable condition often increases with age. Therefore the prevalence of these conditions tends to be higher in the high-income countries due to their older population.
Morbidity and mortality can often be improved with healthcare. Therefore the burden of disease can disproportionately affect lower-income countries where resource scarcity can limit healthcare provision, and they suffer under the dual burden of communicable and non-communicable disease.
As knowledge about the causes of non-communicable conditions continues to grow, richer countries are often able to take action to protect their population. For example, they may introduce stricter controls over occupational chemical exposure, tobacco control interventions, and healthy eating initiatives.
Table 11.1 Global burden of non-communicable diseases, 20041

Burden of non-communicable disease in the UK
Mortality
In 2005 there were 580,000 deaths in the UK.1 The top categories of causes of death were:
Infectious and parasitic diseases only accounted for 1.2% of deaths.
Overall burden
In 2004 the UK was assessed as having 7.5 million DALYs overall, of which 87.5% were due to non-communicable diseases.1 The top 4 global burden of disease categories in the UK account for 68% of total UK DALYs:
Demands on healthcare
Healthcare costs
Inequality
Global burden of communicable disease
Overall, infectious and parasitic diseases cause just under 20% of the global burden of disease (see Table 11.3).
Mortality
The proportion of deaths due to communicable diseases declined in rich countries in the 20th century, but they remain important causes of morbidity and continue to present new challenges such as HIV/AIDS and other emerging infections. Globally infectious and parasitic diseases are responsible for 16.2% of deaths, a large number of which are preventable. HIV/AIDS, for example, is the leading cause of adult deaths in sub-Saharan Africa. More than 90% of deaths from communicable diseases are caused by a handful of diseases: lower respiratory infections, HIV/AIDS, diarrhoeal diseases, TB, malaria, and measles.
Morbidity
The burden of communicable disease morbidity is also high. Infectious diseases in childhood, whilst not always associated with high mortality, can lead to poor development and educational achievement for millions of children in low- and middle-income countries, and to loss of productivity and opportunity for adults. In the UK, communicable diseases place a high level of demand on health services and burden of disease and loss of work for individuals.
Inequality
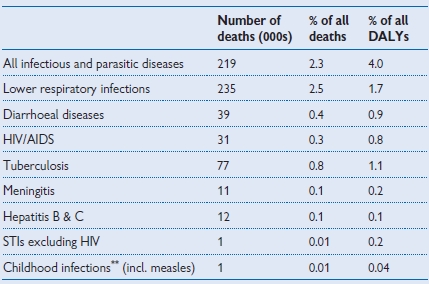
The burden is unevenly distributed between regions of the world, with a much higher proportion of mortality, ill health, and disability attributable to communicable diseases in poorer regions and countries. Major causes of death and disability in the world, such as diarrhoeal disease, measles, and malaria, are far less important in areas such as Europe, as shown by comparing Tables 11.3 and 11.4. However, inequalities also exist within regions and countries, with the burden of disease falling disproportionately on poorer sections of the population. Within Europe, for example, communicable disease causes 1.5% of deaths in high-income areas compared with 2.9% in low- and middle-income areas. In the poorest regions there is an additional burden from neglected tropical diseases (see pp.356–357) which are estimated to affect >1 billion people.
Table 11.3 Global burden of communicable diseases, 20041
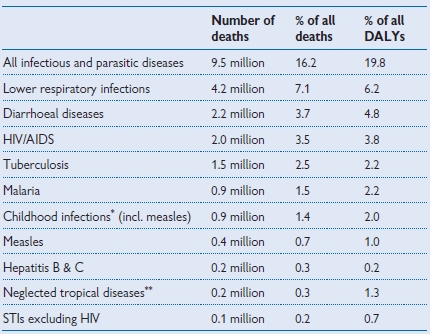
* Childhood infections includes pertussis, polio, diphtheria, measles, tetanus;
** See Neglected tropical diseases, p.356 for definitions.
Table 11.4 European burden of communicable diseases, 20041
Burden of communicable disease in the UK
Mortality from infectious disease declined over the last century from 20% of deaths in 1911 to around 6.6% today. This includes 1% from infections and parasitic diseases such as TB, HIV, meningitis, and 5.5% from influenza and pneumonia1. However, infections are still responsible for a significant amount of illness placing a strain on individuals, health services, and the economy.
Demands on healthcare
Healthcare costs
Mortality
1.2% of all deaths in England and Wales are due to infectious and parasitic diseases (ICD-10 A00-B99, 2005 data);1 including 3% of deaths in children under 16.
Inequality
Gastrointestinal infection leading to hospital admission was 2.4× higher in the poorest fifth of the population than in the most affluent quintile.