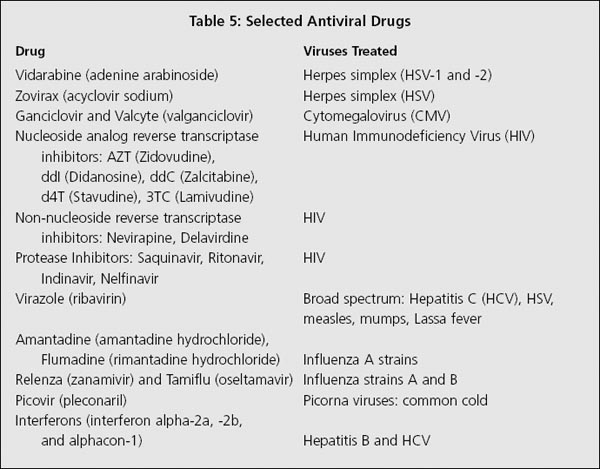
In order to better understand the principles used to renew the immune system and how to use natural antiviral medications effectively, it helps to have some knowledge about the key agents on the viral playing field. In this chapter, I present the most common and most important of current viruses. Some are only mentioned, while those that have more importance in chronic and serious disease, such as hepatitis C and herpes, are discussed in more detail.
Since there are many authoritative books on HIV and AIDS, this subject is covered only briefly; however some important issues surrounding its origin are presented to illustrate how differing opinions of the experts in the field of virology confuse the issues. Many viruses have been omitted here because they are not specifically pertinent to the theme of this book, although that does not make them less serious or dangerous.
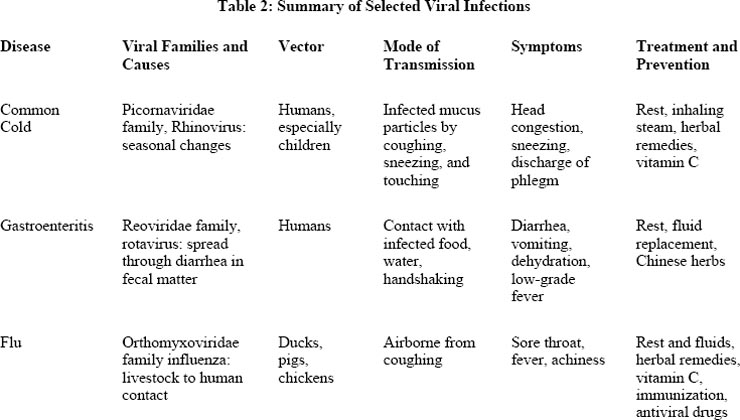
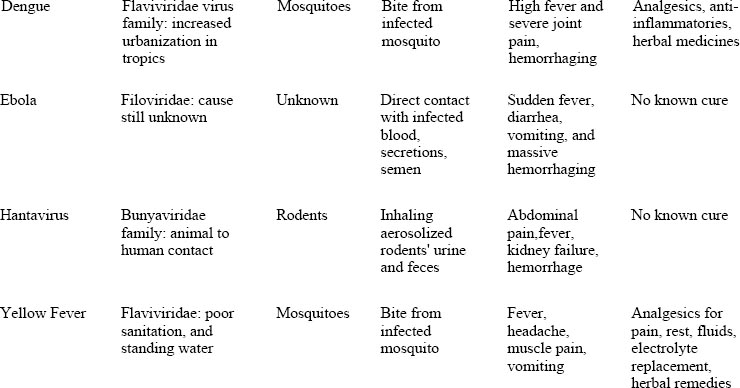
We know so little about viruses and how and when new infections might emerge that the specter of a viral plague looms as a threatening backdrop to modern civilization. Among the viruses presented in this chapter (see table 2), the one most likely to cause a pandemic (a worldwide epidemic) is the flu, perhaps the most common and widely known of all viral diseases. Indeed, it is a real threat, and one that has a high likelihood of occurring within the next decade or so, if microbiologists' predictions are correct.1
From the standpoint of the evolutionary model, we have as much or more to worry about from chronic viruses and depressed immune system states than we do from an influenza pandemic. Prior to the mid-twentieth century, poor sanitation and crowded cities facilitated the transmission of viral infections from person to person. In modern times, chronic viral illnesses occur due to hosts with compromised immunity, and in some parts of the world, nineteenth-century conditions still exist alongside widespread immune system weakness.
The worse case scenario for viral problems is if an outbreak of an extremely lethal, acute viral infection, combined with spreading chronic infections that debilitate and kill slowly were to occur at the same time. In fact, such situations already exist in Africa and parts of India. In these countries, millions are affected by horrible living conditions, and tens of thousands of people die every day from the effects of malnutrition and suppressed immune systems.
While AIDS and common infections take their toll, these unfortunate souls are also under the constant threat of serious viral disease such as yellow fever, dengue fever, and nonviral infectious diseases like malaria and cholera. So far, these conditions have not spread into the developed countries, except in poverty-stricken sections of many of the larger industrial cities, where deepening third-worldlike conditions facilitate the spread of AIDS, tuberculosis, and transplanted infectious disease.
Respiratory tract infections (those that affect the nose, throat, and lungs) are the most common of acute viral illnesses and include the common cold and flu. However, what most people, and even many doctors call “the flu” is actually caused by adenoviruses and paramyxoviruses, and is not “true flu,” which is caused by a different family of viruses (discussed in more detail below).
In the Northern Hemisphere, common respiratory tract infections generally occur seasonally, primarily in the late fall and winter and into the early spring. They can, however, occur at any time of the year in tropical countries, and even in the southern parts of the United States, including Southern California and Florida. Why certain viruses appear at different times of the year is still a mystery, but one explanation may be found in the theory of temperature selectivity of viruses.

Many viruses, such as those that cause the common cold, reproduce better in cooler temperatures and are inhibited by heat. Your immune system exploits this characteristic to your benefit by raising the body's temperature with a fever to control viral spread in the early stages of infection. In the fall and winter, the body's natural immunity is more stressed by inclement weather, exacerbated by radical temperature changes from a warm house to the colder outside, and in summer in moving from air-conditioned buildings to a hot outer environment.
From the viewpoint of Chinese medicine, autumn is the season of the lungs, and a time when the respiratory tract becomes more vulnerable. From an evolutionary point of view, winter is the time when natural selection takes place. Trees are pruned by winter storms and toppled from the wind, wild animals hibernate or die off from starvation, and humans are prone to viral infections that in the past killed the elderly and the very young, allowing only the strongest to survive and mate in the spring.
How Colds Are Spread: Respiratory viruses spread from person to person by sneezing, coughing, or hand contact, and from touching objects like cups, phone handsets, keyboards, and doorknobs contaminated by the person suffering from a cold. As I mentioned in chapter 1, the customary Asian greeting of bowing instead of shaking hands is an excellent means of preventing the spread of viruses. In Asia, people greet each other at arms length and bow to each other without hand contact, or even face-to-face exposure, thereby minimizing the chance that the other person might breathe or sneeze directly into your face.
Viral particles from a human sneeze can travel at 40 mph and reach a distance of 30 feet from the infected person, easily covering a normal-size room. These viral particles then launch their attack on the lining of the nose or throat, or even from direct access to the lung tissue, if they are inhaled directly. Small children are the perfect carriers for colds, flu, and other common viruses. As children play and move around a room, they sneeze and cough without covering their mouths, and they constantly wipe their hands across dripping and draining noses, thereby spreading virus-laden mucus by touching objects and other people.
The Viruses Responsible for Colds: The majority of common colds are caused by a group of viruses called rhinoviruses, of which there are more than 150 types. All rhinoviruses are members of the Picornaviridae family. Two to ten percent of colds are caused by coronaviruses, another common respiratory tract virus. In addition to rhinoviruses and coronaviruses, two other viral groups cause common respiratory tract infections including symptoms identical to the common cold; these involve members of the Adenoviridae and Paramyxoviridae families.
Adenoviruses cause about 5–10 percent of coldlike infections and are one of the most common infections in young children, causing coughs and stuffy or runny noses. Older children and adults infected with adenoviruses mainly experience sore throat (pharyngitis) and mild nasal symptoms. Adenoviruses also cause other infections, such as redness and swelling of the eyes (conjunctivitis), urinary tract infections (cystitis and urethritis), and infections in the intestinal tract (gastroenteritis). In immunosuppressed people, including AIDS patients, adenoviruses can cause life-threatening pneumonia.
The paramyxoviruses cause croup, bronchitis, pneumonia, middle-ear infections (otitis media), and measles and mumps. One member of this family, parainfluenzavirus, causes up to one-half of all respiratory infections in young children. Like other common viruses, there is no pharmaceutical cure, and natural remedies are the best treatment option.
The Course, Symptoms, and Treatment of the Common Cold: After an incubation period of two to three days, typical acute cold symptoms begin. Usually starting with a sore throat, head congestion, stuffiness of the nose, and frontal headache or pain in the back of the neck and upper shoulders, a cold can progress rapidly to coughing and sneezing with copious discharge of mucus from the nose. If a fever is present at all, it is mild and may be accompanied by chills.
As a rule, colds resolve by themselves in a week or two and leave no other diseases in their wake. A common medical school saying wryly illustrates this: “An untreated cold lasts one week, and a treated one lasts seven days.” Interestingly, since I was in medical training, the timing has changed from seven days to twenty-one. Does this mean that colds are stronger than in the past and run a longer course, or that people have weaker immune systems?
Serious secondary infections with colds are rare, but it is not uncommon for a cold to turn into a bacterial sinus infection or bronchitis in the elderly or immune-compromised patients of any age.
Western medical doctors are taught that there is no cure for the common cold. The standard recommended treatment includes bed rest, fluids, and waiting. Symptomatic over-the-counter medicines such as cough suppressants, acetaminophen or aspirin for headache, decongestants, and antihistamines to dry up nasal drainage are recommended. Despite wide use by doctors and as over-the-counter remedies, none of these have any proven effectiveness.
Patients often have their own favorite way of managing colds and most medical doctors tolerate these “folk remedies,” including old-fashioned chicken soup. It turns out this remedy has been shown by research studies to have value in reducing inflammation and the symptoms attributed to the common cold. A vaporizer or the inhalation of steam is also useful in breaking up chest congestion.
In traditional Chinese medicine, the symptoms of common respiratory tract illnesses are classified under the term biao zheng, which denotes an illness of the exterior, as compared to an illness of the organs and interior part of the body, called li zheng. Specifically, viral induced conditions of the upper respiratory tract are called biao han, or “wind-cold” illness, and the common cold is referred to as gan mao.
Despite the difference in terminology, the symptomology of the common cold in Chinese medicine and Western medicine is identical, with the exception that in traditional Chinese medicine, determining a pulse pattern and examining the tongue coating are added as part of the diagnosis. Doctors of traditional Chinese medicine routinely examine the patient's pulse at the radial artery on the wrist of both hands to evaluate the qi. A pulse that is stronger near the surface of the wrist is called a superficial pulse and indicates an active defense response against biao han, or acute illness caused by an attack of wind and cold. There are numerous different pulse qualities that the Chinese doctor uses to determine the state of the patient's health, the location of the illness, the strength of the defensive response, and the quality of yin and yang.
Tongue diagnosis is the other main method of assessment used in Chinese medicine. The body of the tongue is evaluated for color, thinness or thickness, dryness or moisture, and to see if there are ridges, teeth marks, or other geographic abnormalities. The coating is also considered, and is more important than the body of the tongue in assessing acute conditions like the common cold. The tongue of a healthy person is of average size, without teeth marks along the edges, is neither too dry nor too moist, is of a fresh pink color, and has a thin white coat. With a cold, the pulse is superficial and the tongue coating is a thicker white than normal.
In naturopathic medicine, diagnosis for the common cold is exactly the same as that of a conventional medical doctor, though treatment is different. There is a telling joke told by naturopaths about the difference between the two systems of medicine. It goes like this:
Question: “What is the difference between an M.D. and an N.D. (naturopathic doctor)?”
Answer: “When a patient calls in the middle of the night with a runny nose, sore throat, and headache, the M.D. says, ‘Take two aspirin and call me in the morning.’ The N.D. says, ‘Take 20 drops of echinacea and call me in the morning.’”
All three schools of medicine (Western, Chinese, and naturopathic) acknowledge the same symptoms; however, each system has a different perspective concerning the cause.
In Chinese medicine, it is the changing seasons and the colder winds that cause an imbalance in the person's energy state, leading to the activation of defensive mechanisms that attempt to expel the pathogenic influence from the surface of the body. The most common treatment is to cause sweating (diaphoresis), take herbs that expel the pathogenic wind and cold from the surface of the body, and treat accompanying symptoms like headache and cough.
If the body is weak, Chinese doctors also recommend nourishing its intrinsic energy (qi) with chicken soup combined with herbs, or taking tonic herbs like astragalus (Astragalus membranaceus). In fact, there are many excellent traditional Chinese remedies for cold symptoms. One of the most widely used is gan mao ling. It comes in tablets, tea, and instant granules (called ganmao tuire chongji or gan mao char). These remedies can be easily obtained in any Chinese herb store, from most acupuncturists' offices, or by mail from one of the resources listed in appendix E. Their use is explained in detail in part 2.
Naturopaths agree with traditional medical doctors (as do modern Chinese medicine doctors) that the cause of a cold is a virus, and that the symptoms are largely the results of the body's natural defense mechanisms working to neutralize the virus. However, the similarity ends there, as naturopathic philosophy contends that the doctor should assist these natural mechanisms and not suppress symptoms, especially by the use of antihistamines that reduce nasal secretions which are part of the body's mechanical means of expelling virus particles. Naturopathic doctors state it is important to allow the body to discharge the virus, and that suppressing symptoms makes the individual more prone to other illnesses.
Many natural remedies are effective for managing a cold, including high doses of vitamin C. A review of twenty-one placebo-controlled studies on vitamin C indicated that between 1,000 to 8,000 mg daily reduces the duration and severity of symptoms (Hemila, et al. 1995). Zinc lozenges and oral zinc tablets or capsules are also very effective in managing a cold. A number of common herbal teas and tinctures are helpful and include elder flowers, echinacea, yarrow, sage, fresh ginger, and boneset. The therapeutic use of these herbs is explained in part 2.
Many natural remedies are effective for managing a cold, including high doses of vitamin C. A review of twenty-one placebo-controlled studies on vitamin C indicated that between 1,000 to 8,000 mg daily reduces the duration and severity of symptoms.
Viral gastroenteritis, also called the stomach flu, the intestinal flu, or grippe, can be caused by adenoviruses, rotaviruses, caliciviruses, or astroviruses. Symptoms appear suddenly after a very brief incubation period, and include abdominal cramping, mild fever, diarrhea, and vomiting. Because these illnesses are frequently contracted from contaminated food or water, people often think they have food poisoning when in fact they have a case of viral gastroenteritis. However, clinically, both illnesses are often indistinguishable and both resolve in 24–48 hours. In young children or susceptible individuals, dehydration can occur from vomiting and diarrhea, so adequate fluid intake is necessary to prevent dehydration.
Prevention and Treatment of Gastroenteritis: Conventional medical treatment includes mostly supportive care such as bed rest and easy access to a toilet. Typically, fluids like sweetened warm tea, ginger ale, and bland foods like broths or cooked cereal are recommended, since it is difficult to eat without feeling nauseous, vomiting, or having diarrhea. Low blood sugar can occur from lack of food, and drinking fruit juice or fluids sweetened with honey can help prevent hypoglycemic symptoms of weakness and shakiness. Intravenous electrolytes are given if dehydration is severe; however, this is rarely necessary in the average case of gastroenteritis.
Natural medicine views common gastroenteritis similarly as does conventional medicine, but it adds additional remedies like acidophilus to replenish lost “friendly” bacteria and to control unfriendly species in the intestines. High dosages of vitamin C should be avoided since they can cause more diarrhea.2 Although it is generally considered good practice to allow the body to cleanse the offending agent out of the system by not suppressing diarrhea, if the diarrhea is persistent (but not severe enough to require intravenous electrolyte and glucose replacement) mild astringent herbs like blackberry (Rubus fruticosus), blueberry (Vaccinium spp.), or raspberry leaves (Rubus idaeus) can be helpful. You can sweeten herbal teas with honey to keep the blood sugar level normal and prevent fatigue.
Supplements or vegetable broths can provide minerals and electrolytes such as sodium and potassium that are depleted by diarrhea. Chamomile tea (Matricaria recutita) is very useful in reducing cramping and gastrointestinal upset. Berberine,3 a yellow alkaloid and the active ingredient in goldenseal (Hydrastis canadensis), barberry (Berberis vulgaris), and Oregon grape root (Berberis aquifolium) have antimicrobial properties and can help reduce the viral activity in the intestines.
Chinese medicine has several excellent remedies for gastroenteritis. Most contain huang lian (Coptis sinensis), a berberine-containing herb like goldenseal, only stronger. Chinese medicine also recommends not suppressing diarrhea caused by acute mild gastroenteritis, and encourages managing nausea and fever with herbal medicines. Other remedies for diarrhea and gastrointestinal viruses are discussed in detail in part 2.
Influenza is called the “last of the great uncontrolled plagues,” and some epidemiologists believe that we are imminently due for an influenza epidemic of plague proportions like that of 1918. Evolutionary biologists disagree, arguing that conditions for transmission and rapid viral spread are very different now from the Europe during World War I. They also point out that antibiotics are readily available to treat secondary bacterial infections like pneumonia, infections that were fatal in 1918; they contend that reasonably safe and successful vaccines are more widely used now. They also hypothesize that a combination of the two known influenza pandemic strains (hemagglutin type 1 and neuraminidase type 1) does not inevitably lead to a deadly strain similar to that of 1918, as is suggested by conventional virologists (see figure 2-1).
Such discussion seems more like the splitting of hairs because viral reality is completely different from and independent of human opinion. Viruses have their own agenda. Influenza is a potentially fatal disease that is still very much among us. It is just a matter of when, how many people will be infected, and how many deaths will occur. Given the increasing virulence and frequency of other viruses, it seems certain that a more potent influenza virus will appear.
Figure 2-1: Structure of Influenza Virus
This electron micrograph of a cluster of influenza virions shows the typical spherical shape and closely packed spikes that create the characteristic halo around individual influenza virions.
In the temperate regions, like North America and Europe, flu outbreaks occur every winter and epidemics approximately every eight to ten years. Worldwide influenza pandemics occur every ten to forty years, and in the last century the world experienced three: the Spanish flu of 1918; the Asian flu in 1957; and the Hong Kong flu in 1968.
Pandemics occur when there is a major change in the genetic material of the virus, creating an entirely new strain and one against which the world's population has no immunity. Given these parameters, and if the conventional experts are correct in their calculations, we could experience another sweeping influenza outbreak some time in the first decade of the twenty-first century. As one British researcher chillingly remarked, “Put simply, each year brings us closer to the next pandemic” (Shortridge 1995).
The Cause and Types of Influenza: True flu, or influenza virus, is caused by a member of the Orthomyxoviridae family. There are three known types of flu that infect humans: influenza viruses A, B, and C. The most important of these is influenza A, which has over thirty known subtypes. One of the unique characteristics of influenza A is its ability to cause infections in a wide range of animals, including humans, pigs, horses, aquatic mammals like seals, and birds. This ability to infect a broad spectrum of different species effectively ensures its survival.
In humans, influenza virus causes acute outbreaks of severe respiratory tract infection. It has a remarkable ability to evade individual host defenses and to undergo massive genetic changes that prevent human populations from acquiring permanent immunity against it—a trait that contributes to its characteristic rapid spread and ability to cause pandemics.
Influenza A can also change by gene swapping. In an infected cell, different virus particles can share genes. As a shared disease of both humans and livestock, influenza A can rearrange itself in unpredictable intervals, forming new strains in rapid succession. RNA viruses, of which influenza is a member (as is hepatitis C), have extraordinary rates of mutation—estimated at one million times higher than human DNA—producing one mutation for every ten thousand viral replications and taking less than an hour to achieve.
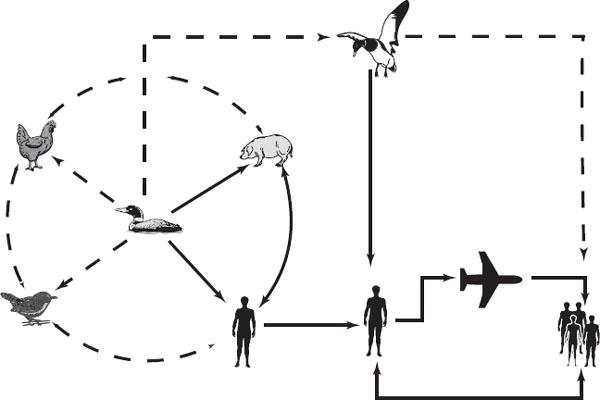
Vectors: Domesticated poultry, primarily ducks and chickens, are the primary vectors for influenza A. From there it spreads to pigs, thereby accounting for the name of one type of influenza A virus, “swine flu.” While rooting around the farmyard, pigs inhale and ingest infected poultry droppings, causing the pigs to catch the flu; from them the virus is passed to humans working and living around the pigs; the virus then travels from human to human.
In a country with very high population density based mostly on rural, self-sufficient farms raising ducks, chickens, and pigs (where the virus keeps continuously circulating), the disease has a chance to jump back and forth between animal species and humans, gene-swapping and mutating to its advantage (see figure 2-2).
Influenza was not known in the New World prior to colonization by Europeans. One explanation is that American indigenous cultures did not have domesticated pigs, cows, or horses, and only in tropical Central and South America were wild birds like parrots, turkeys, and ducks kept as pets, but not in farmyards as they are in Europe or China. Influenza proved to be a particularly severe and mostly fatal disease among American Indians in both North and South America.
Ducks in particular are thought to be the main reservoir of flu viruses. Though not affected themselves, they act as carriers and spread the virus in their droppings. Wild migratory ducks also spread influenza viral particles by dropping feces as they fly, and when they stop over in ponds and lakes they contaminant the water with their feces, which are then taken up by other ducks that fly long distances themselves further spreading the disease.
Origins of Influenza: Historically, southern China is considered the place of origin for most influenza A pandemics. From China they spread through Russia into Europe, and then to the Americas. In centuries past, when land travel was slow, a viral epidemic might run its course, spending itself before spreading too far. However, with the advent of increased world trade and faster means of transportation, a powerful strain of influenza virus could easily reach Europe and America in a matter of days; and with jet travel, and Chinese flying to the West and Westerners traveling to China, viral spread is all the more global and rapid, and could, conceivably, occur in a matter of hours.
Figure 2-2: How the Flu Is Spread
Influenza virus has an animal reservoir and vector, primarily ducks and pigs. Humans inhale viral particles released from the breakdown of fecal matter from ducks or from exposure to pigs. Human-to-human transmission takes place through droplets of air when an infected person coughs or sneezes. A single infected person can carry the flu over thousands of miles in an airplane, and infect an entire population of people.
When I was first in China in the early 1980s, long before most Westerners were allowed to enter this closed society, one expected to catch a severe respiratory infection caused by influenza virus within the first two weeks. Westerners had no immunity to the Chinese influenza strains and became very sick and bedridden for up to three weeks with symptoms of fatigue, headache, coughing, and high fever. As China opened her doors and trade goods flowed in both directions along with businesspeople, students, and tourists, Chinese strains of influenza have spread from country to country with ease. It is conceivable that a potential strong virus could easily arrive in the United States in this fashion.4
Virulence: Virulence refers to the degree of damage an infectious organism can inflict on its host. The amount of damage is influenced by several factors that include the activity of the organism and the strength of the host's immune system. Influenza has a wide range of virulence, and though it can be a fatal disease, it is generally considered a comparatively short-lived infection of the upper respiratory tract, affecting the nose, throat, and lungs.
The severity of a bout of flu is usually related to the immune function of the host, such that those with weakened immune responses, such as older people, the chronically ill, and those with compromised immune systems, suffer the most. It can also be a fatal illness in these groups of people. In the United States alone, influenza kills more then twenty thousand people each year, most of them elderly.
Secondary complications, like bacterial bronchitis and viral pneumonia, are intertwined with severe flu and are considered the probable cause of most of the deaths from the 1918 Spanish flu epidemic, a time when antibiotics were still undiscovered. In the one year that the Spanish flu was at its peak, one in every one hundred people died from influenza or complications. If such an outbreak were to occur today, a one percent death rate would mean that 60 million people, more than the population of France, would die in one year.
Contagion and Symptoms: Infection from influenza virus is simple, extremely effective, and universal. It occurs from breathing contaminated air containing viral particles spread by coughing and sneezing. After an incubation period of two to three days, symptoms start abruptly with shivering, malaise, fatigue, headache, and aching of the limbs and back. Fever is often present and can be as high as 102° to 104° F. When you are sick with the flu you can feel so ill that you have to stay in bed. A typical flu generally runs its course in seven to ten days, but generalized symptoms can linger longer with malaise and fatigue lasting up to three to four weeks.
Pandemic influenza tends to be extremely virulent, much more so then regular flu, and progresses very rapidly. It can cause primary viral pneumonia and death can follow as soon as forty-eight hours or less after primary infection. For the average person and even most doctors, influenza is largely ignored for most of the year, but between December and the end of February large numbers of workers and school children are home sick with the flu. In recent years with the introduction of new strains from China, there have been stronger flu outbreaks, but no major epidemic and as yet no pandemic.
Most medical experts consider influenza, even in its most severe forms, an acute but short-lived infection without any complications or residual effects, however, bacterial secondary infections are common during the course of the illness. Middle ear infection, or otitis media, is a frequent complication of influenza infection in children and causes considerable discomfort for the child and has the potential to cause permanent hearing loss. Influenza virus can also invade the cells of the central nervous system or muscles and cause chronic infections in each called encephalopathy and myositis, respectively.
Fibromyalgia, one of the new diseases and a condition similar to myositis (though more systemic in its effects, including insomnia, fatigue, and irritable bowel complaints) still defies medicine's attempts to assign a definitive cause. There are several theories about the cause of fibromyalgia, including a virally induced cause blamed mostly on herpes viruses. Though little attention is paid to a possible connection between fibromyalgia and influenza A, some experts suggest it is an overlooked syndrome.
In one research paper, Allen Tyler, a medical doctor and naturopathic physician, reports that fibromyalgia was not seen before the 1918 flu pandemic. In his research, he found that 90 percent of fibromyalgia patients tested positive for influenza A antibodies. Tyler postulates that since not all people who contract influenza A come down with fibromyalgia, and though it may be the primary precipitating event, it may be only one factor among many, including stress, altered immunity, and low serotonin levels, that contribute to the full syndrome (Tyler 1997).
Though the conventional medical establishment has not endorsed this theory, Dr. Tyler is not alone in his thinking about chronic influenza infections. German homeopaths have long considered the connection between immune impairment and chronic viral infection to be one of the main causes of modern diseases,5 such as fibromyalgia, and British and Australian physicians are aware of influenza virus-induced myalgias and fatigue.
In these days of complicated viral illnesses, it is prudent to know what flu symptoms are and how to differentiate them from the common cold or other respiratory viral infections. With careful observation you can easily tell the difference between a cold and the flu. At the outset, influenza does not have the characteristic symptoms of a cold like runny nose, sore throat, and sneezing. Flu starts with fever, achy joints, and sore muscles while a cold starts with headache, stuffiness in the head, and congested sinus passages. Fatigue and malaise are present in both the flu and a cold, but with the flu the fatigue is stronger.
German homeopaths have long considered the connection between immune impairment and chronic viral infection to be one of the main causes of modern diseases, such as fibromyalgia, and British and Australian physicians are aware of influenza virus-induced myalgias and fatigue.
Diagnosis and Treatment: There are no commonly used clinical lab tests to diagnose the flu. Rather the diagnosis is based upon the characteristic presentation of symptoms and the knowledge that an outbreak is occurring in the general population. Antibody studies (blood tests that measure levels of immune substances) to influenza virus are available but are used mainly by researchers and not clinically by your typical family physician. A new 30-minute test involving a throat swab, like the ones used to test for strep throat, is available but it does not yet have wide clinical acceptance.
Though there is no medical treatment for the flu, most doctors routinely prescribe antibiotics as prevention or treatment for secondary bacterial infections—a practice that is causing concern over the development of antibiotic-resistant bacterial strains. With the advent of newer antivirals, some experts are suggesting wider use of antiviral drugs to obviate antibiotic use in viral infections, and thus cut down on antibioticresistant bacteria. Such a practice appears to be replacing one problem with a potentially greater one—viruses can develop drug resistance at an alarming rate, one that is often, in fact, faster than bacteria.
Common over-the-counter medicines are sometimes recommended by doctors to treat the symptoms caused by the flu, such as Tylenol (acetaminophen) for fever, Advil (ibuprofen) for joint pain, or nasal decongestants like Sudafed (pseudoephedrine hydrochloride). Sometimes antihistamines are recommended to dry up runny mucus, or a combination of the above is used, such as in commercial flu remedies (for example, TheraFlu).
Even though aspirin is commonly used for the symptoms of flu, in some cases, if taken by children or teenagers, it can cause a rare but potentially fatal complication of influenza called Reye's Syndrome, so it is not routinely recommended for younger patients. However, the aspirin connection is not well understood and since Reye's Syndrome is so rare, there has been no motivation to investigate it further. Until we know more about aspirin-induced syndromes, it is best not to give aspirin to young children when they have the flu.
The “flu shot” is the accepted form of prevention and is mainly taken by high-risk groups such as medical workers, police and fire departments, teachers, and the elderly. The 2001–2002 influenza vaccine guidelines from the Centers for Disease Control and Prevention (CDC) include three categories: those over sixty-five; people fifty to sixty-four years old who have chronic medical conditions (weakening their immune system and making them more susceptible to severe complications); and high-risk people such as health care workers and their families.
Flu vaccines are safer now than in earlier years, but the chances of the vaccine containing the specific antigen, or immune-triggering agent, that matches the current virus is estimated at a success rate of only fifty percent.
Influenza vaccines have a checkered history. In 1976, the swine flu created a national scare as experts predicted an influenza epidemic. Though it never materialized, a mass immunization program was initiated by the federal government under the order of President Gerald Ford. The experts acted aggressively and some forty million Americans were vaccinated. Ironically, the virus, unaffected by the vaccine, ran a benign and short-lived course on its own.
Critics say that the government reacted too strongly and the vaccine, untested at the time, caused about five hundred people to contract Guillain-Barré Syndrome (GBS), a sometimes fatal condition characterized by rapid onset of symptoms with inflammation of the peripheral nerves, those outside the brain and spinal cord, leading to debility and paralysis. About 50 percent of GBS victims report their condition started immediately after a case of influenza. Many recover, but the process can take several years with most patients never returning to normal strength and energy.
Influenza A is inhibited by a class of antiviral drugs called neuraminidase inhibitors, though they are not widely used by doctors because they are relatively new, not well understood, and there is concern about adverse effects. Amantadine hydrochloride and rimantadine hydrochloride are the two most common of these drugs and have been in use for a number of years. Two newer ones, zanamivir and oseltamivir, were approved in 1999 for the treatment of uncomplicated influenza A and B. Amantadine has a high degree of effectiveness in reducing the severity and duration of a flu but all these drugs have side effects that include nervousness, anxiety, lightheadedness, nausea, and vomiting. There is also concern about overuse causing the emergence of drug-resistant viruses that could make the drugs eventually ineffective.
Since vitamin C and other natural remedies also have been shown to reduce the severity and duration of the flu, and do not cause drug-resistance, it seems prudent to try natural medicines first. Natural medicines for the flu include Oscillococcinum, a French homeopathic medication prepared from the livers of Mallard ducks (Anas bar-bariae). Many common herbal remedies are used for influenza including echinacea (Echinacea purpurea and angustifolia); elder flowers (Sambucus nigra); wild indigo (Baptista tinctoria); boneset (Eupatorium perfoliatum); and goldenseal (Hydrastis canadensis). Strengthening the immune system with beta-1,3 glucan; zinc; other antioxidants in addition to vitamin C; and the Chinese herb astragalus (Astragalus mem-branaceus); and other adaptogens, is helpful as a preventive measure. These measures are discussed in part 2.
Since China is the origin of most influenza virus strains, it is not surprising that Chinese doctors have developed many effective herbal medications for the treatment of the flu. Like the common cold, traditional Chinese medicine classifies influenza symptoms in the external disease category of wen bing and biao zheng, as discussed in the previous chapter. However, based upon symptoms, flu has a category of its own called biao re, or “wind-heat.” The Chinese make a distinction between herbs that treat symptoms of the common cold and those that treat influenza and more virulent respiratory tract viral infections.
You may recall that “wind-cold” or gan mao was the Chinese diagnosis of the common cold. You may also remember that one of the distinctions between a cold and the flu is that during a case of the flu, the fever is much higher. The heat generated by the fever and accompanying inflammation is simply called “wind-heat,” or biao re in Chinese, referring to an externally caused illness characterized by fever and inflammation. Herbs that treat wind-heat are febrifuges that help to lower fever and are considered cool in nature. Herbs that treat wind-cold are warming in nature and cause sweating. Many of the herbs used for the flu have been scientifically shown to contain antiviral, anti-inflammatory, and antifebrile properties. Many of these are discussed in part 2.
Individual Chinese herbs used for influenza include isatis (Isatis tinctoria); andrographis (Andrographis paniculata); bupleurum root (Bupleurum falcatum); wild chrysanthemum flowers (Chrysanthemum indicum); honeysuckle flowers (Lonicera japonica); and houttuynia (Houttuynia cordata). Unlike Western herbology, which uses individual herbs or a mixture of herbs with similar functions, in Chinese medicine herbs are combined into formulas that exert synergistic effects.7 Two commonly used formulas for influenza are yin chao san and zhong gan ling (discussed in part 2).
Influenza Summary: Influenza appears to be a disease that will remain with us as long as pigs, ducks, chickens, and humans intermix. However, it is a disease that we can become more familiar with, and against which we can develop better and safer methods of prevention and treatment. As mentioned earlier, there is a high probability that another influenza pandemic will occur within the next ten years. Being prepared, by understanding the way influenza spreads and having a medicine chest of natural flu remedies, is wise. Exercise good judgment when considering use of the flu vaccine, and use antiviral drugs only as the medication of last resort. Prepare for seasonal illnesses and a possible flu pandemic by using natural remedies, especially Chinese medicine, to shorten its duration and intensity.
Human papilloma viruses (HPV) belong to the Papovaviridae family and cause common warts, plantar warts, and genital warts. There are over 80 known different types of HPV, and though most are benign, some types can develop into cancer. The most important of the potentially malignant type are those that occur in the female cervix, especially HPV types 16 and 18. These are found by a physician performing routine pelvic examinations and are often easily seen by eye or with a colposcope. An annual Papanicolaou staining smear (Pap test) is taken and sent to a pathology lab where the pathologist looks at the slide under a microscope to determine if any irregular cells are present. Cervical lesions are treated by freezing or cone biopsy.
Natural remedies for HPV include antioxidants, herbal medicines, homeopathic remedies, and antiviral suppositories that are inserted against the cervix. Though the natural medications used to treat HPV are safe, the proper application and correct dosages, as well as appropriate follow-up Pap smears, require the supervision of a naturopathic physician. Such care is outside the scope of this book, and I suggest you consult with a doctor skilled in natural gynecology.
Herpes viruses cause a variety of infections in humans, including cold sores, sexually transmitted infections, and neurological diseases, and they are also implicated in certain forms of cancer and chronic disease states like chronic fatigue immune deficiency syndrome (CFIDS). What makes herpes viruses such a potential problem is that 95 percent of the world's population harbors some form of herpes virus, and after initial exposure and primary infection, all of these viruses enter a dormant state within different tissues or cells, such as skin or cells of the nervous system. Infection is therefore permanent, and latency of the virus is lifelong.
Under most circumstances, the immune system is able to contain the virus or maintain it in a latent state. However, when the immune system is weakened, the virus may awaken and reactivate, causing disease. This characteristic makes the herpes viral family one of the most insidious of all the viruses, and is the reason some researchers think herpes viruses are responsible for many of the modern chronic ailments, such as CFIDS, multiple sclerosis, and even Alzheimer's.
If the concept that the stress of modern living and the exposure to environmental toxins contribute to immune deficiency is valid, then the potential for herpes viruses to remain latent in infected cells for years and even decades is cause for considerable concern for two reasons. First, because it is so common; and second, because of its effects, such as the central nervous system damage found in multiple sclerosis.
The virus can stay in a dormant state inside the nucleus of a cell without detection from the normal immune system, and because the viral genome is not being expressed the immune system is not even alerted to its presence. When the circumstances are ripe for reactivation—such as the use of immunosuppressive drugs, the development of AIDS or other infections, age-related immune decline, hormonal changes as accompany menstruation, or other causes—the viral genome begins to replicate.
The immune system reacts, but it may not be in time to control the infection caused by the reactivated virus, or it may not be sufficiently effective. Severe, debilitating disease and even death can result from herpes viruses. In addition, since the virus is within the cells that make up body tissue, the immune system can react against itself and inappropriately start attacking the body's joints and muscles, causing a rheumatoid-like autoimmune inflammation.
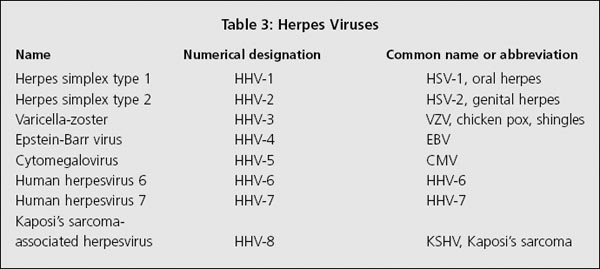
There are eight known types of herpes virus that infect humans and all of them belong to the Herpesviridae family. Herpes viruses have been extensively studied and much is known about their structure. They are large viruses containing up to 150,000 nucleotide molecules, the smallest unit of information stored in the chromosome, in much the same way as data stored on a computer disc. The herpes genome is highly effective, and the viruses have an impressive array of biomolecular techniques to infect a host, invade the immune system, and survive. A numerical system is used to differentiate the types (see table 3).
Herpes Simplex: Herpes simplex (HSV-1 and -2) viruses are similar but cause different infections in humans. HSV-1 affects the upper part of the body, mostly the lips and gums, causing the familiar “cold sore,” whereas HSV-2 primarily affects the lower part of the body, usually in the genital region. Both are spread by human contact: HSV-1 by kissing and HSV-2 by genital sex. Infection is divided into initial and latent infections, and since one person can be infected with both types, the first infection is called the primary infection.
If repeated outbreaks occur, which is common in both types of herpes simplex infections, they are called reactivations of the latent infection. Both types have outbreaks characterized by blisters that occur in the same area each time, and these can be very sore, uncomfortable, and unsightly. Mild systemic symptoms like fatigue and general malaise, or a mild “flu-like” feeling can also occur. The social stigma of genital herpes, though less now than in the 1980s, can still be the cause of considerable emotional stress.
Both HSV types appear on a cyclical basis. They reactivate when the immune system is at a lower ebb or are triggered by a variety of other causes. Many people know what conditions trigger their own outbreaks, such as a cold or flu, stress, or even menstruation. Interestingly, different types of light affect HSV viruses. Ultraviolet light can set off an occurrence in some people, reactivating cold sores from sun exposure. People who are sensitive to sunlight should use sun block or zinc oxide applied to the skin before exposure to the sun. Infrared light has the opposite effect; it can prevent or shorten outbreaks.
HSV-1 infection can also invade the eye (herpetic keratoconjunctivitis) and can lead to permanent damage of the eye and even loss of vision. Other complications of herpes simplex infection include meningitis and fatal encephalitis.
Studies have shown, and patient results have confirmed that supplementing with the amino acid lysine and reducing dietary intake of arginine-containing foods are helpful in preventing and managing outbreaks of herpes simplex. Arginine-containing foods include nuts, peanuts, and chocolate.
Acyclovir (acycloguanosine) is the drug of choice for treatment and prevention of both HSV-1 and -2 by conventional medical doctors. However, to be fully effective it must be given at the early stages of an outbreak. No treatment other than topical acyclovir is generally prescribed for local lesions (or boric acid washes for the eyes).
Physicians practicing natural therapies know from repeated clinical experience that herpes simplex can be controlled, sometimes completely, by enhancing the immune system and using natural antivirals such as olive leaf extract and plant tannins. Immune-enhancing nutrients like vitamin C, vitamin A, zinc, and selenium are also effective. Topical application of lemon balm (Melissa officinalis) extract has been shown to be helpful for cold sores (Wohlbling 1994).
Studies have shown, and patient results have confirmed that supplementing with the amino acid lysine and reducing dietary intake of arginine-containing foods are helpful in preventing and managing outbreaks of herpes simplex (Albert 1987). Arginine-containing foods include nuts, peanuts, and chocolate. Though lysine can be obtained from nonfat dairy products, it is best used as a supplement in dosages between 1,000 to 3,000 mg. (For detailed use of all of these nutrients and antiviral herbs, see part 2.)
Chinese herbal medicines can be very effective in the treatment of severe oral blisters and genital herpes. Formulas containing gentiana (Gentiana macrophylla), such as long dan xia gan tang, are particularly useful. For viral infections in the eye, the coptis-containing formula nu huang jie du pian (Bovine Bezoar Toxin-Resolving Pill) is effective. The use of these medications is discussed in part 2.
Varicella-Zoster Virus: Primary infection with varicella-zoster virus (VZV) causes chickenpox, a common childhood infection with an incubation period of about two weeks and resulting in the characteristic rash on the trunk of the body. Adults with chickenpox may have severe systemic symptoms affecting their whole body along with a widespread rash. Most cases of chickenpox run a benign course and conventional treatment is usually limited to bed rest and applying calamine lotion to control the itching. Natural medicine also recommends resting and application of calamine lotion, baking soda, or oat-meal baths to reduce itching, but also prescribes vitamin C, vitamin A, and echinacea to manage the virus.
Complications are rare in simple cases of chickenpox, but in immune-compromised patients, chickenpox can lead to pneumonia (varicella pneumonitis) and brain infections (post-infection encephalitis). Individuals with cancer, children with leukemia, AIDS patients, and those on immunosuppressing drugs, should be particularly careful if they are exposed to chickenpox.
Generally, after the primary infection, natural immunity takes place and the individual cannot be re-infected; however, like all herpes viruses, this virus goes into hiding. VZV remains latent for life, hiding in the nerve cells in the dorsal root ganglion along the spine. Facial nerves, like the trigeminal nerve, can also be affected. When the immune system is weakened, as when under stress, in older people, or when the immune system is compromised by another disease or drugs, the virus reactivates and causes a new condition called herpes zoster, or shingles, causing the skin to break out in painful blisters.
Shingles usually occur on the trunk of the body, but can also be in the lower back and waist, or on the face and head, including entry into the eye. The infected nerve itself can be damaged by the virus, leading to a condition called post-herpetic neuralgia, one of the most painful conditions known.
In the early 1980s, when I was first practicing, shingles was considered a disease of the elderly. At that time, most of the patients I saw for this condition were well into their eighties, with the youngest around sixty-five. Then, as environmental conditions changed and natural immunity became challenged, people started to have shingles at earlier and earlier ages, including children of five years old. In addition, with the advent of AIDS, shingles became a common secondary illness due to immune deficiency.
One of the most tragic cases of my career was that of a twenty-six-year-old man who developed herpes zoster in his right eye. This very handsome and athletic young man was one of the kindest patients I had met. He was very health-conscious and kept extremely fit with regular exercise as well as maintaining his professional dance career. His diet was largely vegetarian and he took adequate dosages of supplements, including extra antioxidants.
However, he was HIV-positive, and during a drawn-out stressful crisis involving his work, his immune system weakened and the herpes zoster virus reactivated. Due to the severity of the pain, he was admitted to the hospital, and once there declined very rapidly, dying of secondary infections within a month. It happened so fast, there was very little I was able to do for him.
Conventional treatment for shingles is limited to time, application of Zostrix, a cream containing extract of cayenne pepper, and the antiviral drug acylcovir or related drugs like famvir. However, these measures are mostly ineffective and the patients often suffer needlessly when there are good natural remedies available. Surgery is resorted to in severe cases, and I have seen patients with eyes removed in attempts to control herpetic-induced pain.
Luckily, if caught in time, there are alternatives for shingles and post-herpetic neuralgia. Acupuncture is effective in reducing the pain and shortens the duration of the attacks. Vitamin C, vitamin A, selenium, and zinc, along with olive leaf extract, are very helpful.
Two other cases illustrate how natural methods can help. Several years ago, two women, both in their thirties, came to my office in the same week with the same complaint: an itchy painful rash about the size of a half dollar on the cheek. Both had a case of herpes zoster. The first had already been to her conventional medical doctor and the drugs prescribed did not work. When she came to my office, the pain was severe and the woman was in tears because of the unsightliness of the lesion.
I treated her daily with acupuncture and prescribed natural medications. Before the week was over, the pain was gone, she felt normal, and the rash was in retreat. By the end of eight days, it was completely gone. The other woman did not have much pain and was not inclined to use conventional medicine. She came to see me first. I treated her in the same way and the results were just as good as the first patient.
Epstein-Barr Virus: Epstein-Barr virus (EBV) has been called the most sinister of the herpes virus family because of its association with certain forms of cancer and its ability to reappear in chronic and reactivated forms. Remarkably, 80 to 95 percent of all adults worldwide have antibodies to EBV, which means that it is a common—almost ubiquitous—infection.
Primary infection occurs mainly in children or young adults and can cause no symptoms at all, mild flu-like symptoms, or infectious mononucleosis (the “kissing disease”), with symptoms of fever, sore and swollen throat, fatigue, and enlargement of the lymph nodes and spleen. Recovery from mononucleosis takes three to four weeks, but in severe cases, lassitude and fatigue can linger for months. However, complete return to normal is the rule. Like other herpes viruses, it then remains latent for life.
There are two types of EBV, the A and B forms. Type A is the most common form, but in equatorial Africa and with AIDS patients, type B can predominate. Both types can coexist in the same person and according to current knowledge, both types cause similar infections. EBV causes infection of the B-lymphocytes, important cells in second-line defense, and induces more than eighty known virus-specific antigens in the B cells. These antigens are important for the laboratory diagnosis of EBV, from which your doctor can tell if you have an active or chronic infection or if you merely have the immune markers from a previous, normal exposure without evidence of current or chronic infection.
EBV is also implicated in several forms of cancer: Burkitt's lymphoma, nasopharyngeal cancer, and B-cell lymphoma, and it has been linked to T-cell lymphomas and Hodgkin's disease. To date, most of these EBV-induced cancers occur in the Third World. However there is concern that in the developed countries, EBV causes other non-cancerous chronic diseases that may have connections to other cancers.
Epstein-Barr virus is implicated in numerous chronic diseases including fatigue syndromes. In the late 1970s and early 1980s, people started to complain of vague but persistent and often debilitating symptoms of fatigue and flu-like sensations. At first, doctors thought these symptoms were caused by ordinary neuroses or mild depression masquerading as tiredness. Since the victims were mostly women in their late twenties to mid-thirties who were often high achievers and over-worked in professional jobs, the syndrome was dubbed the “yuppie flu.”
However, in 1984 an outbreak of strange symptoms with a common fatigue profile among the patients took place in Incline Village, a small town on the Nevada side of Lake Tahoe. Symptoms included severe and persistent fatigue, “brain fog,” and mildly swollen lymph glands—a condition very much like mononucleosis. However, the symptoms did not go away or resolve over a period of time, as mononucleosis would.
Even more strangely, when the individual started to feel better and exerted any amount of energy, such as trying to exercise, their symptoms worsened for two to three weeks afterwards. These relapses were a complete mystery to medical doctors and a source of considerable anxiety for the patients.
Paul Cheney, a family practice physician in Incline Village, was among the first to suggest that the cause for this pattern was EBV. The syndrome became referred to as chronic Epstein-Barr virus (CEBV). However since then, researchers have failed to conclusively prove that all cases of chronic fatigue, now called Chronic Fatigue Syndrome (CFS) or Chronic Fatigue Immune Deficiency Syndrome (CFIDS), have positive laboratory evidence of active or chronic active EBV infection. Cheney, pursuing the disease further, found that a majority of blood samples of CFIDS patients tested positive for HTLV-1 and HTLV-2, a retrovirus related to HIV, and discussed in the next section. However, he was unable to conclusively prove that this virus was the specific cause rather than EBV.
While more and more patients turned up at doctors' offices with the same pattern of symptoms, the controversy whether chronic fatigue was an organic disease caused by a virus or a stress-related psychological disease akin to depression continues to this day. Most conventional doctors were completely baffled by CFIDS, as they still are, having no training in medical school on how to diagnosis or manage such an illness. Eventually complications to CFIDS started to appear: fibromyalgia, irritable bowel syndrome, leaky gut syndrome, and cognitive disorders like poor memory and reduced ability to concentrate.
For CFIDS, some of the typical presentations are psychological symptoms; it is therefore not surprising that medical doctors, who diagnose largely by the presenting symptoms, would think that the cause was depression. Patients with this condition often feel hopeless and become depressed, and experience mood changes that include irritability and bouts of unexplained anger.
In the early and mid-1980s, I treated scores of such patients. One in particular comes to mind: a medical professional herself and an athlete, this woman suffered from recurrent sore throats, debilitating fatigue, and significant mood changes which included depression, irritability, and hopelessness. For several years she was unable to work at her own clinical practice. She traveled extensively in an unsuccessful search for a definitive diagnosis and effective treatment, including trips to several of the top university research centers in the country. In the end, what seemed to work best was simply time, rest, and vitamins and minerals. She gradually improved enough to return to her work, but never recovered completely and never obtained a definitive diagnosis.
A profound lack of will is an interesting aspect of chronic Epstein-Barr virus infection, but it is distinctively different from common or classical depression. However, many medical doctors, not understanding chronic fatigue or the difference in mood between clinical depression and fatigue states, continue to diagnosis chronic fatigue patients with depression.
When the selective serotonin re-uptake inhibitor (SSRI) antide-pressants (like Prozac) came out, conventional medicine thought these drugs were the solution to the chronic fatigue problem. The reasoning went something like this: if the condition was a biochemically induced depression related to serotonin, this class of drugs should work–another case of the “magic bullet” mentality, and one that completely ignored social, psychological, and environmental conditions.
However, in my clinical experience I have seen patient after patient with fatigue syndromes try Prozac or Paxil and later tell me they had no improvement or that their mood was slightly better but they still were just as fatigued as ever. Though antidepressants can sometimes play a complementary role in the treatment of this condition, SSRIs do not cure chronic fatigue syndrome and are not very effective in the treatment of depression related to EBV infection.
In his groundbreaking book Chronic Fatigue Syndrome: The Hidden Epidemic, Jesse Stoff, M.D., one of the original proponents of the chronic EBV theory,7 stated that EBV can cause a transient state of immune deficiency (different from acquired immune deficiency syndrome, AIDS) leading to chronic disease which is CFIDS in its mild form. In its severe form, EBV can penetrate the nervous system, causing encephalitis, Guillain-Barré syndrome, and a condition called transverse myelitis, a neurological syndrome characterized by the rapid development of leg weakness.
Transverse myelitis is a condition similar to multiple sclerosis (MS), and though little is known about its cause, most evidence indicates that it is triggered by an infection, such as from viruses in the herpes family. This condition is most likely a repercussion of the immune system attacking the whole nervous system trying to get at the virus lodged in the nerve cells. It's like a pack of dogs tearing up your yard to get at a few gophers.
In addition, according to Dr. Stoff, chronic EBV can contribute to numerous other inflammatory conditions like myocarditis, pneumonitis, and pancreatitis, as well as metabolic disorders like diabetes and hypothyroidism.
Besides affecting the nervous system, one of the primary targets of EBV is the liver. A liver chronically affected by a low-grade viral infection may not show signs of cellular damage for twenty or more years, if ever. However, its function will be impaired, consequently affecting metabolism and many other processes in the body, all of which can impair one's health.
Cytomegalovirus and Stealth Viruses: Cytomegalovirus (CMV), another member of the herpes family, can be passed from mother to fetus during pregnancy, while breast-feeding, or from the urine or saliva of other infants if they lay together, such as in child-care. Adolescents and young adults can acquire it from kissing and sex. It can also be contracted from contaminated blood during a transfusion, and from infected donated organs. Like other herpes viruses, once CMV is acquired it lasts for life, lying dormant in the body with the capacity for reactivation. At least 50 percent of Americans over forty years old test positive for exposure to CMV.
Active CMV infection is similar to mononucleosis without the sore throat and swollen lymph glands. AIDS patients are particularly at risk for serious CMV infection, as are those undergoing organ transplant using immune-suppressing drugs.
CMV appears to be the perfect virus. Often first contracted in infancy, its transmission is usually unnoticed. In later years, its transmission is usually through sexual activity, and if any symptoms arise, and often they do not, it only causes an illness similar to mononucleosis. Diagnosis is therefore often missed. Then, undetected by the immune system, it remains latent until the situation is right for reactivation. In an immune-compromised individual, its reactivation can cause severe illness with secondary, and sometimes fatal, infection of the lungs.
CMV is involved in chronic disease and causes a wide range of neurological and autoimmune illnesses while remaining undetected by the immune system and undiagnosed by medical professionals. Therefore, it often goes untreated. Inflammation caused by CMV infection is also thought to contribute to heart disease by exacerbating atherogenic lesions, or plaques, that form in the blood vessels of the heart.8 Perhaps the most devious design of CMV is its possible role in hidden brain infections.
W. John Martin, M.D., Ph.D., director of the Center for Complex Infectious Disease in Rosemead, California, investigates complex neurological disease and CFIDS and believes he has identified a new class of cytopathic (cell killing) viruses, which he calls “stealth viruses” (Martin 1994). In his studies, he has found that there is considerable laboratory and clinical evidence to suggest that patients with CFIDS and neurological diseases like MS and transverse myelitis are suffering from an atypical viral infection, most likely caused by a form of CMV, but he also has found positive evidence for other herpes viruses like EBV, HSV, and HHV-6.
Dr. Martin's clinical research has lead him to hypothesize that a new class of virus, derived from herpes virus and capable of evading detection from the immune system, is a possible cause for the wide range of new complex diseases, including CFIDS, fibromyalgia, the increasing incidences of MS, and some forms of psychosis.
Like Dr. Stoff, Dr. Martin has also found viral evidence in other tissue. Liver, thyroid, muscle, skin, salivary glands, urinary tract, and intestinal tract, and diseases related to these organs and tissues all interplay in his stealth virus paradigm. In this paradigm, he suggests that these viruses use cytokines (immune system proteins that affect the behavior of other cells) as a growth factor.
Dr. Martin's treatment strategies make sense in light of this idea. Primary treatment is aimed at regulating cytokine activity. Suppression of viral activation and replication by antibiotics and antivirals is reserved for severe cases only. Relying mainly on natural medications, primarily quercitin, a flavonoid antioxidant with anti-reverse transcriptase (an enzyme that is an essential component of retroviruses) activity, Dr. Martin employs a wide range of natural substances and practices, dietary recommendations, and nutritional supplements that support cellular metabolism, such as antioxidants, amino acids, and essential fatty acids.
Dr.Martin's clinical research has lead him to hypothesize that a new class of virus, derived from herpes virus and capable of evading detection from the immune system, is a possible cause for the wide range of new complex diseases, including CFIDS, fibromyalgia, the increasing incidences of MS, and some forms of psychosis.
In addition, he suggests stress reduction, behavior modification, and other strategies including antidepressants and nootrophics (brain-enhancing medications) to improve neurological function. Finally, he recommends evaluation and treatment for secondary conditions such as hypothyroidism, correction of bowel ecology, adrenal enhancement, allergy testing, and improvement of blood circulation—treatments that are very much in accordance with the way a naturopathic physician would treat.
Though Dr. Martin's work is not finished, the direction of his research is correct and fits all the criteria that I present in this book. First, it comes out of a thought process that allows for complex disease patterns caused by evolutionarily adapted infectious organisms, in this case, a stealth virus. Second, it does not attempt to eradicate the virus with a treatment that may be worse than the cure; instead it neutralizes its growth factors. Third, he uses supportive natural medications to improve the function of other vital systems of the body, allowing for greater immune strength and organ reserve (the term used to describe the normal tissue health and immune status of an organ). We need more physicians like Dr. Martin.
Human Herpesvirus 6: One of the newest members of the herpes family, human herpesvirus-6 (HHV-6), was discovered by Robert Gallo, M.D., in 1986. Like its cousins EBV and CMV, HHV-6 is usually acquired early in life. In children, it causes roseola, a common childhood infection with symptoms of fever, sometimes convulsions suggesting central nervous system involvement, and a characteristic rash on the trunk of the child's body. When contracted later in life, it may cause a mono-like illness. After the initial infection, which can be silent in both children and adults, the virus goes into latency. Also like the other two herpes viruses, when reactivation of HHV-6 occurs, it can cause CFIDS and other chronic neurological diseases, including MS. Unbelievably, an estimated 90 percent of adult Americans have antibodies to HHV-6, meaning they have been exposed to it.
There are two known variations: HHV-6A and HHV-6B. Another form, HHV-7, has also been identified causing illnesses similar to HHV-6. This virus infects the T lymphocytes, a type of white blood cell, and researchers believe that it is capable of disabling key components of the immune system, especially the CD4+ T lymphocytes. HHV-6 can also destroy natural killer (NK) cells, part of the first line defense against viral infection and cancer.
Coincidentally, NK cells are also disabled in both CFIDS patients and AIDS victims. Donald Carrigan, Ph.D., the foremost American HHV-6 researcher, believes HHV-6 can be a co-infection contributing to the immune deficiency associated problems in both diseases. Carrigan's colleague, Konnie Knox, Ph.D., has conclusively found evidence from autopsy tissue samples that HHV-6 is extremely active at the time of death in AIDS patients, suggestive that it, and not HIV, is the viral killing factor in AIDS. Her doctoral dissertation, “Human Herpesvirus Six (HHV-6): Evidence for Its Role as a Cofactor in the Pathogenesis of AIDS” (Carrigan et al. 1996), further supports Carrigan's theory (Regush 2000).
Herpes Virus Summary: Nearly every adult is infected by one or more members of the herpes virus family. Usually acquired in childhood or infancy, herpes viruses are latent for life. Though they are common in humans and generally are considered to be more inconvenient than life-threatening, in a world of increasing immune incompetence, herpes viruses can become lethal causing severe and debilitating symptoms. At least one member of this family, HHV-6, is linked to AIDS either as a cofactor or as the cause of death. HHV-6 is an extremely potent and dangerous virus, one that most people have been exposed to and now carry in their bodies.
As immune dysfunction is becoming increasingly more common, it seems prudent that more research be focused on it. In the meantime, I suggest doctors familiarize themselves with the consequences of chronic herpes infections and the effective natural ways to treat them.
EBV is one of the most insidious of all the herpes viruses and can cause or participate in a wide range of illnesses. Conventional medical doctors, who diagnose from symptoms and standard blood tests, will most likely miss a diagnosis of CEBV, CMV, or HIV-6. Specialized blood tests are required (see the appendix).
There is no one-shot drug for herpes viruses. Most viral diseases are ineffectively controlled by drugs and only HSV-1 responds well to pharmaceutical antiviral drugs. However, keep in mind that if you have a life-threatening viral infection, drug therapy might save your life, but a better approach is to prevent viral infection and to strengthen the immune system with the natural therapies listed in part 2. Many of these natural medications effectively treat herpes infections.
Though the overwhelming majority of AIDS researchers support the theory that human immunodeficiency virus (HIV) causes AIDS, the HHV-6 controversy of a stealth virus or deadly cofactor and other equally confusing issues continue to overlap with AIDS research, causing considerable concern. This issue of what actually are the real viral dynamics in immunodeficiency states is extremely important for individual and global future health. If the dominant consensus is wrong, then government and research establishments have wasted tens of billions of dollars and years of time going in the wrong direction. Even if they are correct, the final chapter on AIDS is far from being written, and certainly the nineteenth-century infectious model based on Koch's postulate is not working well enough in the twenty-first century. A more comprehensive evolutionary approach would be helpful.
Since 1884, when Robert Koch (1843–1910), a German physician who won the Nobel Prize for medicine in 1905, presented his theory, the idea that infectious microbes like bacteria and viruses cause disease has been one of the cornerstones of Western medicine. However, it has become more accepted that the immune status of the host contributes to resistance to infection and influences virulence.
The evolutionary model suggests that disease is the result of interaction between the host and the microbe, and is not simply based upon the strength of the infectious agent.9 The model of Chinese medicine takes it a step further: the strength of the host's immune system is the primary factor in preventing infectious disease.
A Brief History of HIV: The retrovirus family, of which HIV is a member, is not new to virologists, and was first identified in the early years of virology. In 1910, Peyton Rous, M.D., working with the Rockefeller Institute for Medical Research in New York, discovered a virus (avian sarcoma virus) that caused tumors in chickens; for his research he was awarded a Nobel Prize. In 1930, other tumor-causing retroviruses were discovered in mice and other animals, including feline leukemia virus—a disease that causes immune deficiency and death in cats. In 1978, the first human retrovirus, human T-cell leukemia virus type 1 (HTLV-1), was discovered by Robert Gallo, the same scientist who discovered HHV-6.
During the late 1970s and early 1980s, while laboratory scientists were laboring over individual viruses, clinicians were trying to unravel the causes of a new fatigue syndrome with life-threatening respiratory infectious complications. Paul Cheney, still on the trail of CFIDS, moved on from thinking of EBV as the sole cause and developed a theory, based on the available lab tests of the time, that HTLV was the possible causative agent for CFIDS. Then a new and more severe form of fatigue syndrome developed, casting an even more somber tone on both the clinical and laboratory scene.
Joseph Sonnabend, a New York medical doctor, reported numerous cases of gay men with unusual and complicated illnesses characterized by profound immunodeficiency with a common element, the development of fatal Pneumocystis carinii pneumonia (PCP). In 1981, the condition was named acquired immune deficiency syndrome (AIDS).
A virus was suspected and reactivated CMV was first considered the most likely candidate because it often occurred in the later stages of the illness. In 1983, Luc Montagnier, a cancer researcher at the Pasteur Institute in Paris, uncovered a new retrovirus in the Lentivirus genus: human immunodeficiency virus (HIV). The Latin root, lentus, means “slow.” Gallo and his coworkers later confirmed HIV's involvement by independent research, and eventually two types were identified: HIV-1 and HIV-2. However, Sonnabend and other practicing physicians still argued that AIDS was a syndrome, or constellation of many factors, including various possible viruses, that together contributed to the disease rather than it being caused by only one infectious agent.
In fact, questions still circulate concerning both Montagnier's and Gallo's research about a positively identified, unique HIV genome. Debate continues to this day whether a unique AIDS virus in fact exists, if HIV is the sole cause or an opportunistic virus, and what the role of other immune factors in the progression of the disease is.
Essentially, the confusion arises from a difference of paradigms. The “old school” of medical science still favors the single-agent, or one-cause, theory. Researchers look for one infectious organism and then attempt to develop a vaccine or drug to kill it. Koch's Postulate of 1884 is still used, which states that the infectious organism must be found in all patients with the same disease; that the organism can be isolated and cultivated in the laboratory outside of the infected host; that a similar disease should develop when infecting animals with the laboratory organism; and that the same organism should be recovered from the inoculated experimental animals.
Old-school practitioners do not favor theories based on lifestyle or a broader view of disease, which is the realm of evolutionary thinkers who view AIDS as a product of our times, related to environment, lifestyle, and perhaps reconstituted viruses—but not to a single causative agent.
Further AIDS Controversy: Even though the Durban Declaration, delivered at the Thirteenth International AIDS Conference in Durban, South Africa, in May and June of 2000, tried to put the AIDS controversy to rest by affirming Koch's Postulate stating that all patients with AIDS are infected with HIV and that HIV is the causative agent of AIDS, numerous influential scientists continue to disagree. Among the dissenters are Peter Duesberg, Ph.D., a microbiologist at the University of California at Berkeley, and Eleni Papadopulos-Eleopulos, Ph.D., a researcher from the Royal Perth Hospital in Australia and head of the Perth Group.
Papadopulos-Eleopulos is convinced that the decrease in CD4+ T cells seen in AIDS is not due to destruction by HIV but is caused by lifestyle-induced immune deterioration. In one paper, she proposed that oxidative cellular damage, the negative effects of oxygen activity on cellular molecules, is one of the critical steps in the progression of immune deficiency.
Not ending her case there, she has published numerous other articles defending her group's theory, and has offered an explanation for the African AIDS epidemic. She contends that HIV-positive blood tests do not prove it is the cause of AIDS since the symptoms and diseases African victims experience are identical to tuberculosis, diarrheal diseases, parasitic infections, and other diseases that have existed in Africa since Egyptian times.
Duesberg also questions the proposition that the cause of AIDS is the retrovirus HIV. He has referred to the AIDS virus as a harmless “passenger” virus, just another virus among many living parasitically in the human body, and he claims that a positive HIV test is merely a viral marker (and not indicative of the cause) indicating immune system damage.
In his opinion, based upon exhaustive research, AIDS is an immune deficiency disorder caused by overuse of recreational drugs and a lifestyle that burns the candle at both ends, including promiscuous sex. Eventually, the immune system collapses. Then pre-existing latent viruses reactivate: some cause illness like CMV and others, like HIV, proliferate but are only along for the ride. Finally, other opportunistic infections take over, like candidiasis (Candida albicans) and Pneumocystis pneumonia, which eventually kill the patient.
The debate continues: the majority still favor the one-cause-fits-all theory and the dissidents support an evolutionary theory that makes sense but that cannot yet be conclusively proven. From my clinical perspective, if Duesberg and Papadolpulos-Eleopulos were correct, AIDS patients would recover with rest, change of lifestyle, and nutritional supportive medications. If infectious symptoms are managed with antibiotics, antifungals, and antivirals, patients should improve and recover. But they do not.
Nutritional support and natural therapies do make a substantial difference in how AIDS patients feel by reducing their symptoms, but in themselves they have not been found to be curative. So what is happening with the immune function of these patients?
According to some experts, such as Papadolpulos-Eleopulos, the answer lies not in how the body recovers, but in how gradual, irreparable cellular damage occurs, caused by environmental toxins, drugs, and stress. Like the saying, “You can make a pickle out of a cucumber, but not a cucumber out of a pickle,” once a certain cellular line has been crossed, the tissues are incapable of returning to a completely normal state. However, this is not the end of the story.
To further complicate matters, Howard B. Urnovitz, Ph.D., a microbiologist with Calypte Biomedical in Berkeley, California, has challenged the notions of the monkey origin of AIDS. According to Dr. Urnovitz (elegantly documented in The River [1999] by Edward Hooper), AIDS was caused by oral polio vaccine contaminated with monkey virus causing a recombined hybrid virus, HIV-1. If this is the case, given the right circumstances, then additional millions of people worldwide will start showing symptoms of immune deficiency. Further, in those people who have suffered genetic damage, this damage will be passed on to their children and their children's children.
Hooper's book caused enough controversy to stimulate some researchers into action, and three short papers were published in the journal Nature in 200l exonerating polio vaccines (Weiss 2001). Still, Hooper and others are unsatisfied and continue to press the contamination theory. It may be a long time before we ever know the real origins of human immunodeficiency disease.
An even more sinister scenario was proposed and documented by Leonard Horowitz, a Tufts- and Harvard-educated dentist with a Master's degree in public health, in his controversial book, Emerging Viruses: AIDS & Ebola, Nature, Accident, or Intentional (1996). Horowitz's worst-case scenario, his primary theory, is of a CIA-conducted biological weapons experiment gone wild. His alternative theory is similar to Hooper's: the accidental outbreak from contaminated vaccines. Neither of Horowitz's theories have been conclusively proven, but due to the seriousness of his accusations, both deserve further investigation.
Not only are the causative factors questioned, but the progression of AIDS is also disputed. Louis J. Picker, M.D., associate director of the Vaccine and Gene Therapy Institute at Oregon Health and Sciences University in Portland, Oregon, argues that there is no direct association between levels of HIV-specific CD4+ T cells and disease progression, and suggests that lowered levels of these cells in AIDS patients could be a countermeasure by the immune system to reduce target cell levels so the virus has fewer activated cells to attack.
Not all HIV-positive patients progress to full AIDS. I have encountered many of these individuals in my own practice. By practicing a healthy lifestyle that includes nutritional supplements, antioxidants, antiviral herbal medications, and immune-enhancing substances, they remain active and lead normal lives. Many, like basketball star Magic Johnson, are able to lead high-performance, athletic lifestyles.
A few HIV-positive patients, over time and after up to ten years of treatment with natural therapies and lifestyle changes, have tested negative for the virus. Though very few researchers are investigating the role of natural immunity in minimizing or preventing AIDS, some believe that the immune system has the ability to contain and even eliminate the virus completely.
Urnovitz reports that in a study of seven patients, at least five with confirmed exposure to HIV, none of the seven subjects had any symptoms of AIDS, and two of the patients who previously tested positive for HIV by urine samples later tested negative (Barnum 1993). In an interview with a British medical journal, Urnovitz is quoted as saying, “What this tells me is that there is hope in reversing HIV infection if we pay attention to how to do it” (Stolberg 1993).
This study suggests that immunity may play a larger role in preventing and eventually halting the spread of AIDS. Though documentation for these cases is still lacking and more research and publications are needed, our immune systems may win the race between science and nature.
This study suggests that immunity may play a larger role in preventing and eventually halting the spread of AIDS. Though documentation for these cases is still lacking and more research and publications are needed, our immune systems may win the race between science and nature.
Is There a CFIDS-AIDS Continuum? Though each condition is still looked at as an independent disease, after I carefully sifted through all the differences of opinion, one common thread emerged and one immense question remained unanswered. Are CFIDS (chronic fatigue complicated by immune deficiency)10 and AIDS related conditions on a continuum of immune system breakdown, rather than different conditions with specific viral infections?
As I will describe in a later chapter, though a viral trigger is suspected in about 80 percent of CFIDS cases, the syndrome does not have a single obvious viral cause that can be substantiated by lab tests. Therefore, from the point of view of the conventional biomedical model, both are distinct disease entities: HIV causes AIDS while CFIDS has not been linked to a virus.
Though research has found that both conditions display immune deficiency patterns, to my knowledge, few researchers are pursuing this line of thought. Nancy Klimas, M.D., of the University of Miami School of Medicine in Florida, is one of those investigating the immunological abnormalities in chronic fatigue patients. Her work suggests a gradual progression of the illness, starting with a genetic predisposition and a triggering event or series of events, such as a viral infection complicated by immune system weakening as occurs in stress or from toxic exposure (Klimas 1990).
In a world out of balance with environmental pollution at unprecedented levels, ecological disruption, overwhelming psychological stress, repeated wars and violent civil strife tearing individual lives and entire countries apart, abuse of stimulant drugs, sexual promiscuity, and over-use of pharmaceutical drugs causing microbial drug-resistance, immune system disruption may be the root cause of a variety of apparently different but actually similar diseases.
Treatment Options: Despite the fact that HIV has become the most medicated viral disease in medical history, there still is no cure. In a stunning article published in The Scientist, Myrna Watanabe writes (2001): “Despite billions of dollars spent in research funding and a brief reprieve in Western nations after the introduction of multidrug therapy, AIDS continues to win its battle against humankind.”
In the face of such evidence, the current treatment remains the use of several drugs at the same time—multidrug therapy. Initially heralded as a possible cure because patients showed early improvement, this aggressive “cocktail therapy” appears to cause more harm than good, and creates drug-resistant viral strains at an alarming rate. The side effects are severe, including liver damage.
Even when symptomatically effective, it does not kill all of the virus, which has developed ways of hiding out in the memory cells of the immune system, a strategy similar to latency. In this case, however, the dormancy is a response to pharmaceutical medications. When the drugs are discontinued, the virus emerges from these temporary reservoirs and rebounds, causing renewed infection—the drugs having only masked the symptoms without effectively treating the underlying cause.
Until recently, people with AIDS in Africa, India, and the world's poor countries could not afford drugs. However, pirated patents are now available at a fraction of the cost in the United States and Europe, and some drug companies bowing to international pressure have made generic drugs available. In the next few years, drug treatment for HIV will skyrocket. Even at reduced costs, poorer nations will not be able to afford medications without bankrupting their already strained economies.
In the developed nations, AIDS has become a severe chronic disease that one lives with for years under the management of extensive drugs, before eventually succumbing to an opportunistic infection. Considerable evidence suggests that natural and alternative therapies can have significant influence on managing the infection in the early stages and in slowing progression over the course of the disease. Rather than a single factor, such as a virus, influencing outcome, HIV infection is influenced by many different factors including genetic susceptibility, response to therapy, nutritional status, immune status at the time of infection, metabolic and hormonal changes, and previous infections such as latent CMV.
An AIDS vaccine, if an effective one is found, is still at least another ten years away. Seth Berkley, M.D., an epidemiologist and head of the International AIDS Vaccine Initiative, a global call for action launched at the United Nations General Assembly special session on HIV / AIDS, June 2000, contends that a vaccine is our last and best hope of halting the AIDS epidemic. I agree that searching for a vaccine is important, but without radically altering how we live in this world, deadly viral diseases will continue to defy the notion that we have superiority over nature.
The Perfect Virus: HIV may be nature's perfect virus. It spreads by an act common to almost all humans, sexual activity, and infection progresses slowly, allowing for a host carrier to spread it to other individuals before full symptoms appear. It invades specific cells of the immune system causing increased vulnerability to a wide variety of fatal infections. It has proven impossible to eradicate; mutates rapidly, defying antiviral drugs; and when suppressed by drugs, it is capable of lying latent indefinitely.
It is challenging modern medicine's superiority complex and altering economies and the politics of nations, especially in Africa and Asia. In a matter of two decades it shattered conventional medical opinion from one of arrogance and complacency about infectious diseases to a more realistic awareness that new diseases continuously emerge. The AIDS pandemic has defied our notion of superiority and shocked infectious disease theorists at their roots because HIV infection does not follow Koch's Postulate.
AIDS also forced social changes by opening the closet doors on homosexuality; it altered people's sex lives and birthed a new genre of literature, theatre, film, and painting. It brought increased awareness of the global disparity between the rich and poor, and by entrenching itself in the most vulnerable communities and countries: mostly poor, uneducated, and people of color. It has called our attention to the greatest moral issue of our time. AIDS also served to accelerate the acceptance of alternative medicine and stimulated new research into the areas of nutrition and natural antivirals.
Hepatitis, a general medical term for liver inflammation, is not caused by only one virus. Though many different viruses cause infections in the liver, including Epstein-Barr virus, three main viruses cause damage to human liver cells, the hepatocytes, resulting in true hepatitis (see table 4).
Hepatitis A: Infectious hepatitis, or hepatitis A (HAV), is caused by an RNA virus of the Picornaviridae family, the same group that includes poliovirus and rhinovirus, that causes the common cold, and HAV is contracted through feces containing viral particles that then contaminate water or food consumed by humans. It can also be transmitted through blood transfusions, shared needles, and sexual contact. Minor HAV outbreaks occur regularly in the United States but as it is still a common disease in third world countries, and care should be taken when traveling overseas to have only well-cooked food and bottled water.
After an incubation period of two to six weeks, symptoms of fatigue, vague abdominal discomfort, and fever occur. Jaundice, the classic sign of hepatitis (yellowing of the skin and whites of the eyes), follows. Generally HAV is a short-lived acute infection that passes without complications. However, if the immune system is run down, it can cause severe fatigue and illness enough to make you bedridden for a month. Though prevention is the main way of avoiding infection, there is an effective inactivated vaccine available and human immunoglobulin shots give temporary natural immunity for people traveling in endemic areas, such as India. Herbal remedies are used in India, Nepal, and China to treat HAV.
Hepatitis B: Hepatitis B (HBV), sometimes referred to as serum hepatitis, is a serious blood-borne viral illness that can lead to chronic liver disease, liver cancer, or in the case of severe rapid infection (a condition called fulminate hepatitis) it can cause death. It is a member of the Hepadnaviridae family and is transmitted in blood and other body fluids, like semen and breast milk.
A highly contagious disease, HBV can be contracted through sexual intercourse, the use of contaminated needles (including unsterilized hypodermic and acupuncture needles, tattoo needles, and needles shared by drug addicts), and through blood transfusions. It is endemic in China and other parts of Asia where up to 20 percent of the general population is infected; it is less common in Europe and North America. There are an estimated 350 million HBV carriers worldwide.
HBV has been studied extensively both in the laboratory and clinic, so today there are several accurate laboratory tests to show if you have ever been exposed to HBV and if you have developed effective immunity against it. Despite the extensive knowledge about HBV, there is no effective treatment available in Western medicine. First generation live vaccines, introduced in the late 1900s, caused several deaths and considerable controversy. Though a genetically engineered vaccine has been developed and is reported to be safe (it requires a series of shots with a booster every five years), until the vaccine is proven to be completely safe and effective, caution is strongly advised in its use.
Since the incidence of infection is so high in China, HBV has been recognized for centuries and many traditional herbal medicines are used to treat its acute and chronic states. Several of these herbal formals, such as sho-saiko-to (Japanese for xiao chai hu tang, or minor bupleurum decoction), have also been shown by modern scientific studies to be effective in the management of HBV (see part 2).
Hepatitis C: In the mid-1970s, around the same time AIDS and CFIDS symptoms first appeared, another new infection was emerging. Originally called non-A, non-B hepatitis, it was first found in blood transfusion patients. Named hepatitis C (HCV) in 1989, it was first described as a new virus in Science (Choo et al. 1989) and has since become the most prevalent infectious disease and the most important liver condition in the United States and Canada, with an estimated four million Americans infected. Currently 8,000 to 10,000 deaths occur each year in the United States alone due to HCV. Worldwide, 170 million people are infected—more than four times as many as HIV.
ORIGINS AND TRANSMISSION: Like HIV, the origins of the hepatitis C epidemic remain obscure and speculative. An RNA virus, HCV belongs to the Flaviviridae family, the same group of viruses that includes yellow fever and dengue. There are currently one hundred identified strains of HCV.
HCV is considered a blood-borne virus, but many cases report no contact with any possible source of contaminated blood. This mystery has yet to be solved; however, it appears there are modes of transmission other than blood. Known sources of infection include injection drug use, needle-stick accidents by health workers, contact with infected blood products, sexual contact with menstrual blood in infected persons, infants born to infected women, tattoos, and shared toothbrushes and razors. Though a mosquito vector was ruled out by researchers in the late 1990s, preliminary studies by French scientists at the Hospital Pasteur in Paris strongly suggest that some HCV cases may be mosquito-transmitted.
THE COURSE OF HCV INFECTION: Though acute HCV infection can sometimes lead to death, the majority of cases develop silent and slow-progressing infections, called chronic hepatitis C. In these cases, cirrhosis and hepatocelluar carcinoma are the predominant causes of death. However, at least 15 percent of cases resolve completely without complications, and even many cases of chronic infection remain stable and do not develop into cirrhosis. In the majority of cases, symptoms only appear when advanced liver disease has already developed, although some individuals complain of fatigue, joint pain, and itching during the early course of the disease.
Disease progression appears to be more rapid in elderly and immune-compromised individuals. In addition, slow progressive liver disease causes fibrosis—or hardening of the liver tissue—which greatly impairs liver function. Alcohol consumption and HIV infection accelerate the progression of HCV.
When this impairment is severe enough, even without cirrhosis— the end stage of liver fibrosis—a variety of systemic conditions can develop: ascites (a buildup of fluid in the abdomen); esophageal varices (bleeding from varicose veins); stagnation of blood in the veins of the legs complicated by edema; reduced immune function; fatigue; and mental confusion. Hepatocellular carcinoma, or cancer of the liver cells, is the worst-case scenario and generally leads to death (see figure 2-3).
TREATMENT OPTIONS: Medications of choice include interferon alpha—a chemical messenger produced naturally by the immune system—administered by injection, and the oral antiviral agent Ribavirin, a nucleoside analog. Even so, they are ineffective, cause considerable side effects, and this therapy is very expensive. Meta-analysis has shown that interferon alpha, when given for one year, has an effective rate of only 16–23 percent, and the cost for forty-eight weeks of combined treatment is around $20,000. As in AIDS, combination therapy has become popular, although interferon plus Ribavirin produce a sustained response in only 40 percent of patients. (See table 5 for a summary of drug approaches to viruses.)
However, once the drugs are discontinued, most patients relapse and only 50 percent of patients who relapse and are treated with a second course respond favorably. This is a dismal clinical picture. Liver transplant, a life-saving measure, is reserved for patients with end-stage liver disease, though mild HCV infection to the transplanted liver occurs in most of these patients.
SIDE EFFECTS: Side effects of therapy are common and frequently debilitating, with the majority of patients experiencing severe flu-like symptoms. Tachycardia (rapid heart rate), restlessness, irritability, depression, and insomnia may also occur. Bone marrow suppression and severe neuropsychiatric disorders, including suicidal depression, may occur later in therapy. Conventional treatment of side effects is based on symptoms and includes the use of acetaminophen, electrolyte management, and selective serotonin re-uptake inhibiting anti-depressants. Alternative treatments for side effects, which include acupuncture, herbs, and nutritional supplements, are very effective and safe.
Figure 2-3: Course of Hepatitis C Infection
Approximately 15 percent of people infected with HCV completely clear the virus from their systems. The other 85 percent develop chronic HCV. The majority (80 percent of people with the chronic form) do not develop serious complications, and of the remaining (20 percent) who develop cirrhosis, most (75 percent of those with cirrhosis) slowly progress, and only a minority (25 percent) actually develop hepatocellular cancer or require a liver transplant.
One of my patients, a professional in his late forties, experienced severe and nearly intolerable side effects of combination therapy, including nausea and vomiting, headaches, debilitating fatigue, insomnia, and depression and mood changes. Within two treatments of acupuncture and herbal remedies, the nausea and headaches were completely gone; he was sleeping better and had more energy. By the end of six weeks, the side effects were controlled enough for him to return to work.
This patient continued on the interferon and ribaviran therapy. In fact, he did two complete courses. In the process, his viral count reduced considerably, but once he discontinued the treatments the virus rebounded and his counts went back up to pre-treatment levels. He has now accepted that natural therapies are best, and that through them he can improve his immune status and his body can learn to coexist with the virus without damaging itself.
ALTERNATIVE APPROACHES: A number of alternative therapies have been suggested for the treatment and management of HCV. Alcohol is a well known liver toxin and must be eliminated completely in order to effectively manage liver inflammation and the progression of hepatitis C.
Excess tissue iron can damage the liver and promote the growth of bacteria that cause secondary infections. If you have hepatitis C, avoid taking an iron supplement and use a multivitamin and mineral that is iron-free. Also eliminate red meat and egg yolks, though keep your protein intake adequate by eating fish and poultry. If your blood levels of iron are too high from your blood test, you may benefit from old-fashioned blood-letting by having your physician draw off a small amount of blood in a procedure called venesection, as is used to take blood when you have a blood test.
Bile salts reduce liver injury by lowering bile acid levels in the liver and gallbladder, and they also have immune-enhancing properties and as yet unknown activity that protect the liver cells. Bile salts are often found in digestive enzyme formulas or can be prescribed by your medical doctor or naturopathic physician.
Supplemental use of antioxidants (vitamins C and E, and lipoic acid); oral N-acetyl cysteine (NAC) combined with interferon alpha, aspirin and other nonsteroidal anti-inflammatory drugs; and the use of thymosin with interferon alpha are helpful.11
Schisandrin C, derived from the Chinese herb Schisandra chinensis (wu wei zi), and silymarin (the active flavonoid component of milk thistle, Silybum marianum) have been shown to have liver protective action. Licorice extract (Glycyrrhiza glabra) is effective when combined with interferon alpha. Many of these substances are discussed in part 2.
Due to the high incidence of viral hepatitis B in China, traditional Chinese medicine has had a long history of treating chronic hepatitis utilizing a systematic and comprehensive methodology underlying its principles of treatment. Although hepatitis is not specifically mentioned in The Yellow Emperor's Classic, it did describe syndromes that closely resemble the symptom profile of hepatitis in the acute and chronic stages.
Though most research in China on herbal treatment for hepatitis has been on hepatitis B, recent studies demonstrate equal effectiveness against HCV. One double-blind study in Australia utilizing a new Chinese formula called CH-100 for HCV indicated significant reduction in ALT, an enzyme used to measure liver function and whose elevated levels are not desirable. Another study in Japan on minor bupleurum decoction (sho-saiko-to) showed it to have activity against HCV. This formula is one of the most researched formulas for hepatitis in China and Japan, and is commonly used by North American practitioners for all types of liver disorders.
Though researchers are not entirely clear how this formula works, it is suggested that it may activate macrophages, increase cytokine production, and promote natural killer cell activity.12 A promising preliminary study on a new combination of Chinese herbs named “Eurocel,” containing extracts of Patrinia villosa, was performed at the Institute of Life Sciences at Chungbuk National University in Korea and showed a decrease in viral markers.
The most promising work with Chinese herbs and HCV is by Qingcai Zhang who was trained as a medical doctor in China and who now practices traditional Chinese medicine and acupuncture, along with extensive clinical research, in New York City. Dr. Zhang's work with AIDS and HCV patients over a period of fifteen years clearly indicates that Chinese herbs, if properly prescribed and in concentrated preparations taken over a long period of time, can control viral spread and even reduce the viral load to such a degree that a few cases of his have subsequently tested negative for viral markers (Zhang 2001).
Due to the high incidence of viral hepatitis B in China, traditional Chinese medicine has had a long history of treating chronic hepatitis utilizing a systematic and comprehensive methodology underlying its principles of treatment.
Complications or side effects of these herbs appear to be rare. If they do occur, they are usually minor gastrointestinal upset or diarrhea, which are self-limiting upon reduction of the dose or discontinuance of the medication. There is evidence that minor bupleurum decoction may cause interstitial pneumonitis, a form of pneumonia, when used in combination with interferon alpha.13
Licorice root and glycyrrhizin (licorice extract) are common additions in Chinese herbal formulas. It is generally considered safe to use, however in high dosages or in susceptible individuals, it can cause fluid retention and lower potassium levels causing fatigue and high blood pressure. Considered a harmonizing tonic herb in traditional Chinese pharmacology, it is processed by steaming to remove any toxic effects and when taken in the usual prescribed amounts it generally does not cause any side effects. To be safe, people with hypertension should not use it.
HEPATITIS C SUMMARY: Serious liver disease constitutes a chronic uncontrollable stress resulting in physical, emotional, and immune disruption. Integrated therapy—conventional allopathic methods combined with alternative therapies, lifestyle modification, and psychological counseling—appears to offer great promise.
Though the ultimate therapeutic goal is the eradication of all detectable viruses, in many patients with chronic HCV this outcome is very difficult or impossible to achieve. One of the reasons HCV has become so common is that natural immunity to HCV infection appears to be weak or absent—yet another sign that the increasing incidence of viral diseases is equally a problem due to emerging species, heightened virulence of known viruses, and a possible immune deficiency in the general population.
The viruses in this group include a wide range of viral diseases from several different viral families. Among them are well known diseases like yellow fever and dengue, as well as newly emerging ones like Ebola and hanta viruses. Insects spread most of these viruses—one in particular: the Aedes aegypti mosquito. This species of mosquito is responsible for dengue and yellow fever viruses.
Dengue: Another of the old world diseases brought to the Americas, dengue—also called “break-bone fever”—was once common in North America at least as far north as Philadelphia. It reached a high point after World War II and then declined to a point where it was considered an uncommon and benign disease causing little more than flu-like symptoms. But since 1980, dengue has revived to epidemic proportions, and a newer deadly form, dengue hemorrhagic fever, has emerged.
Though mostly concentrated in Southeast Asia, where thousands of cases are reported annually, dengue hemorrhagic fever shock syndrome (DHFS)—a condition once found only in children—is now also found in the Caribbean and South America. Dengue has also returned to the United States. In the mid-1980s, the Asian tiger mosquito (Aedes albopictus, a close relative of A. aegypti) arrived in a freighter load of tires containing standing water. Worldwide, dengue infects between fifty and a hundred million people each year and is considered the most common mosquito-borne virus.
Dengue belongs to the Flaviviridae family which also includes yellow fever and hepatitis C, and there are four known sub-types: dengues 1–4. Symptoms appear rapidly after an average incubation period of five to eight days and include severe joint and muscle pain—thus the name “break-bone fever” because of the severe bone pain. Alternating severe chills and high fever are common, severe headache, pain behind the eyes, and the patient is so sick he can hardly move.
Though there are few fatalities from typical dengue, the illness can be so severe the patient feels as if he is dying. In severe cases the patient feels exhausted and remains debilitated for weeks or months, or longer. There is no medical treatment other than bed rest, replacement of fluids, and transfusions of whole blood in hemorrhagic cases. Aspirin or Tylenol is recommended to help relieve pain. This is an appalling situation given the frequency of dengue and its increasing severity, and more effort should be given to mosquito control in third world countries in addition to finding better treatments.
In colonial America, the specific herb for break-bone fever was boneset (Eupatorium perfoliatum), a member of the daisy family (Astericae) to which echinacea also belongs. It is prepared as a strong infusion and drunk as a tea; it may also be used as a tincture combined with echinacea, and homeopathic preparations are also available.
Yellow Fever and Other Viral Disasters: Arthropod-borne viruses, diseases caused by “blood-sucking” insects, produce an array of viral illnesses that range from mild flu-like symptoms to death. Of these, yellow fever, carried by the same mosquito as dengue, is the most severe. It arrived in the Americas by slave ships from West Africa and became one of the most feared of diseases up until the early part of the twentieth century. Yellow fever is a hemorrhagic disease that attacks the liver causing jaundice, necrosis (death of cells), and death. It is still common in tropical Africa, Latin America, and Asia. An effective vaccine is available, but there is no specific treatment other than management of symptoms and blood transfusion.
A number of other insect-borne viral illnesses that cause illnesses in America include Venezuelan equine encephalitis, Colorado tick fever, Eastern equine encephalitis, Western equine encephalitis, St. Louis encephalitis, California encephalitis, and West Nile Fever. Most of these viruses cause (or can lead to) inflammation of the central nervous system. Other viruses that also cause central nervous system damage include the herpes viruses, HIV, poliovirus, and the mumps; however, these are not insect-borne illnesses.
Rodents, such as squirrels, mice, and rats, spread viruses in their droppings when they forage for food. The contaminated food is then eaten, or dried fecal matter contaminates the air and is then inhaled. The most notorious of rodent-related viruses is hanta. First identified in 1954 during the Korean War, the virus was isolated from samples found near the Hantaan River in 1978. This disease, originally called Korean Hemorrhagic Fever, belongs to the Bunyavirus family and has a genus of its own, Hantavirus, with three types identified. In 1993, an emerging hantavirus was identified in New Mexico, which caused headline news over an emerging viral threat. It attacks the kidneys and can cause lung inflammation, internal bleeding, and death.
Next to AIDS, Ebola virus—because of its terrifying consequences—has become the virus most imprinted on contemporary consciousness. There are three types of Ebola, which is also a bleeding fever like Hanta and dengue, but only two types affect humans; the other known type infects only monkeys. It is endemic in parts of Africa, but Ebola has “cousins,” all members of the Filovirus family, that occur in other parts of the world including Europe, South America, and Asia. The most notorious of these is the Marburg virus, first identified in South Africa. Other fatal hemorrhagic viral diseases include Lassa, Argentine, and Bolivian fevers.
With increasing human population density, less funding for public health measures in third world countries and Eastern Europe, uncontrolled rodent and insect populations, increasing genetic diversity among viruses, and increasing destruction of natural biodiversity and habitat, it is likely that we will see more incidences of these diseases, especially of dengue fever, in the future.
One of the strangest things about viruses is that they are often described as being both dead and alive—or neither dead nor alive—a paradox that scientists have yet to solve and medical philosophers continue to puzzle over. Looking at the triangular, hexagonal, and spiral structures of viruses, I am amazed at their beauty and symmetry, which more resemble that of minerals and crystals than animal or plant cells.
Prions and the BSE Crisis: A number of diseases have appeared that are not identifiable according to any of the known microbial categories: they are neither a virus, a bacteria, a protozoa, nor a parasite. A new category, proteinaceous infectious particles (PrPs), or prions, the cause of mad cow disease, or bovine spongiform encephalopathy (BSE), are rogue proteins that convert normal protein into misshapen and deadly forms. What makes these diseases threatening is their ability to jump species and easily penetrate brain tissue.
Prion diseases are unique from other infectious illnesses in that they are both an infectious and hereditary disease, and occur in animals and humans. Humans can become infected from contaminated beef, as a result of general surgery, by hormone injections from contaminated products, in corneal transplants in eye surgery, and by genetic transmission. The chief human prion disease is Creutzfeld-Jacob Disease (CJD), a condition that causes loss of motor control, dementia, paralysis, and death. How prion diseases progress is still unknown and there is no effective treatment.
Pleomorphism: The phenomenon of microbial pleomorphism, that infectious agents can have more than one shape, was documented as early as 1881 in Sweden by Ernst Almquist, a student of Robert Koch (of Koch's Postulate). Since then, pleomorphic forms have been identified for fungal and bacterial species and are one of the suspected causes of stealth infections. It would not be surprising if viruses also displayed the ability to “morph.”
The ability of microorganisms to change forms like the shape-shifters of science fiction may eventually add another dimension to our understanding of evolution. Humans, like all vertebrates, require many thousands and even millions of years to evolve even the simplest of changes. Microorganisms, on the other hand, can see generations come and go in a matter of minutes, and they are able to evolve more quickly than we are, as evidenced in drug-resistant forms of bacteria and viruses. Therefore, treatment strategies that work with nature to achieve environmental balance within the body are required to either complement existing or developing pharmaceutical drug treatments, or in some cases to replace them entirely.
Plants have very complex structures and their immune mechanisms work to inhibit viruses from several different avenues at the same time, making it difficult for the viruses to develop resistance to natural compounds. Evidenced by the increased interest by scientist worldwide in antiviral and immunomodulating natural compounds, herbal medication can play a significant role in the treatment of viruses, especially in light of drug-resistant and pleomorphic forms of those viruses.
Extraterrestrial Origins: Sir Fred Hoyle (1915–2001), an outstanding British astronomer and professor at Cambridge University, and the most visible proponent of the theory that life on this planet was seeded from outer space, believed that extraterrestrial events and forces influenced viral pandemics. Viruses, in his theory, are charged particles that penetrate the Earth's atmosphere and genetically intermingle with existing viruses causing new strains. Though his theories are impossible to prove and have vexed scientists for decades, the premise underlying Hoyle's unusual theories is that the universe is interconnected and displays intelligence. It is this concept of the intelligence of all things that makes his ideas so fascinating, and not too far from those of modern evolutionary biology, shamanism, and Eastern cosmology.
If all life and events are animated by a universal intelligence, and I tend to think they are, understanding how this intelligence operates and attuning to its principles will promote health and prevent disease. Natural medicines inherently contain more of this intelligence than chemical drugs, and if applied correctly have a remarkable ability to promote recovery and cure, even from viral diseases.