After reading this chapter, you should be able to
1. discuss why people do or do not exercise,
2. explain the different models of exercise behavior,
3. describe the determinants of exercise adherence,
4. identify strategies for increasing exercise adherence, and
5. give guidelines for improving exercise adherence.
Lots of people appear to be exercising in an attempt to stay young and to improve the quality of their life. In addition, judging from the looks of store windows, we’re in the midst of a fitness craze. Most department stores carry a wide variety of athletic sportswear, not only for physical activity but also for leisure and even work. More and more fitness clubs appear to be opening up as people try to get or stay in shape. But the fact is that most Americans do not regularly participate in physical activity (U.S. Department of Health and Human Services [USDHHS], 1996, 1999).
Let’s look at some statistics to get a better idea of the level of exercise participation. These data are drawn from a variety of sources representing extensive surveys in many of the industrialized countries (e.g., Canadian Fitness and Lifestyle Research Institute, 1996; Caspersen, Merritt, & Stephens, 1994; Gauvin, Levesque, & Richard, 2001; Higgins, 2004; King et al., 2000; Sallis & Owen, 1999; USDHHS, 1999, 2000; Vainio & Biachini, 2002):
 Physical activity rates within the United States are similar to those in other industrialized nations. Only 10% to 25% of American adults are active enough to maintain or increase cardiorespiratory and muscular fitness levels.
Physical activity rates within the United States are similar to those in other industrialized nations. Only 10% to 25% of American adults are active enough to maintain or increase cardiorespiratory and muscular fitness levels.
Among adults, 30% do not participate in any physical activity.
Among American adults in 2000, 19.8% (40 million) were considered obese compared with 12% in 1991.
Among Americans, 66% were seen as overweight or obese in 2005. In fact from 2000 to 2005 obesity increased by 24% and the percentage of super obese increased by 75%.
The propensity to be overweight increases with age, as 44% of people age 18 to 29 and 77% of people age 46 to 64 were overweight in 2005.
Among youths from 12 to 21 years of age, 50% do not participate regularly in physical acti-
vity.
Among adults, only 10% to 15% participate in vigorous exercise regularly (three times a week for at least 20 minutes).
Of sedentary adults, only 10% are likely to begin a program of regular exercise within a year.
Among both boys and girls, physical activity declines steadily through adolescence from about 70% at age 12 to 30% to 40% by age 21.
Among women, physical inactivity is more prevalent than among men, as it is among blacks and Hispanics compared with whites, older adults compared with younger ones, and the less affluent compared with the more affluent.
Of people who start an exercise program, 50% will drop out within 6 months.
Most recently, the Centers for Disease Control and Prevention Behavioral Risk Factor Surveillance System Survey Data (2008) has provided information on physical activity patterns using revised definitions for minimum levels of physical activity. Some findings for 2008 include the following:
Approximately 72% of adults did not engage in a minimum of 20 minutes of vigorous physical activity for at least 3 days per week (little change from 2000).
Approximately 50% of adults did not engage in a minimum of 20 minutes of vigorous physical activity for at least 3 days per week or moderate physical activity for at least 30 minutes at least 5 days per week.
Approximately 47% of high school graduates and 15% of college graduates reported no leisure time physical activity.
Approximately 25% of adults reported no leisure time physical activity—down from 30% throughout the 1990s.
Approximately 19% of individuals ages 18 to 24 reported no leisure time physical activity compared to 27% of individuals ages 45 to 64 and 33% of individuals over 65 years of age.
Approximately 26% of females and 22% of males reported no leisure time physical activity.
Blacks and Hispanics reported significantly more leisure time physical activity (33%) than did whites (22%).
Thus, it is clear that as a society we are not exercising enough and this lack of physical activity is exacerbated by certain individual differences. This occurs despite the physiological and psychological benefits of exercise, including reduced tension and depression, increased self-esteem, lowered risk of cardiovascular disease, better weight control, and enhanced functioning of systems (metabolic, endocrine, and immune systems; see chapter 17). Only a relatively small percentage of children and adults participate in regular physical activity. This prompted a special issue of papers from the Academy of Kinesiology and Physical Education (Morgan & Dishman, 2001) targeted at exercise adherence. So let’s start by looking at why people exercise—as well as the reasons they give for not exercising.
REASONS TO EXERCISE
With much of the adult population either sedentary or not exercising enough to gain health benefits, the first problem that exercise leaders and other health and fitness professionals face is how to get these people to start exercising. People are motivated for different reasons (see chapter 3), but a good place to start is to emphasize the diverse benefits of exercise (President’s Council on Physical Fitness and Sport, 1996). Note that the issue of maintenance as well as initiation of physical activity is a critical one, because individuals must continue to be physically active to sustain the full health benefits of regular exercise (Marcus et al., 2000). So let’s look at some of the more typical reasons for people to start an exercise program.
Weight Control
Our society values fitness, good looks, and thinness, so staying in shape and keeping trim concern many people. However, an estimated 70 to 80 million American adults and 15 to 20 million American teenagers are overweight, and these numbers have been increasing over the past 10 years. In fact, recently there has been an increased focus on teenage obesity and obesity in general as a national epidemic. The first thing most people think to do when facing the fact that they are overweight is diet. Although dieting certainly helps people lose weight, exercise plays an important and often underrated role (and although dieting is never fun, exercise certainly can be fun). For example, some people assume that exercise does not burn enough calories to make a significant difference in weight loss, but this, too, is contrary to fact. Specifically, running 3 miles five times a week can produce a weight loss of 20 to 25 pounds in a year if caloric intake remains the same. Weight loss can have important health consequences beyond looking and feeling good. Obesity and physical inactivity are primary risk
factors for coronary heart disease. Thus, regular exercise not only improves weight control and appearance but also eliminates physical inactivity as a risk factor.

Exercising to lose weight can be seen as a self-presentational reason for exercising because this typically will result in enhancing physical appearance and improving muscularity (Hausenblas, Brewer, & Van Raalte, 2004). It is not surprising that some people are motivated to exercise for self-presentational reasons considering that positive self-presentation is strongly influenced by the aesthetic-ideal physique. Regardless of the current ideal physique (which has changed over time), people are influenced by it because of a self-presentational concern to look good and be popular.
Reduced Risk of Cardiovascular Disease
Research has produced evidence that regular physical activity (although we do not know the exact dose–response relationship) or cardiorespiratory fitness decreases the risk of mortality from cardiovascular disease in general and from coronary heart disease in particular. In fact, the decreased risk for coronary heart disease that is attributable to regular physical activity is similar in level to that for other lifestyle factors, such as refraining from cigarette smoking. In addition, regular exercise has been shown to prevent or delay the development of high blood pressure, and exercise reduces blood pressure in people with hypertension. Like obesity, hypertension is a prime risk factor in coronary heart disease, but research has indicated that it can be reduced through regular physical activity. So it is not surprising that a
summary of studies identified improvement in people’s physical and psychological health as the most salient behavioral advantage of exercise (Downs & Hausenblas, 2005).
Reduction in Stress and Depression
As discussed in chapter 17, regular exercise is associated with an improved sense of well-being and mental health. Our society has recently seen a tremendous increase in the number of people experiencing anxiety disorders and depression. Exercise is one way to cope more effectively with the society we live in and with our everyday lives.
Enjoyment
Although many people start exercise programs to improve their health and lose weight, it is rare for people to continue these programs unless they find the experience enjoyable. In general, people continue an exercise program because of the fun, happiness, and satisfaction it brings (Kimiecik, 2002; Titze, Stonegger, & Owen, 2005). Along these lines, Williams and colleagues (2006) found that individually tailored physical activity programs were more effective for individuals reporting greater enjoyment of physical activity at baseline. In essence, special attention needs to be paid to individuals who do not enjoy physical activity to start with, and exercise should be intrinsically motivating if a person is to adhere over a long period of time (this will be discussed in more detail later in the chapter).
Enhancement of Self-Esteem
Exercise is associated with increased feelings of self-esteem and self-confidence (Buckworth & Dishman, 2002), as many people get a sense of satisfaction from accomplishing something they couldn’t do before. Research (Whaley & Schrider, 2005) has revealed that hoped-for self of older adults (staying healthy and independent) was related to increases in exercise behavior. Something as simple as walking around the block or jogging a mile makes people feel good about moving toward their goals. In addition, people who exercise regularly feel more confident about the way they look.
Opportunities to Socialize
Often people start an exercise program for the chance to socialize and be with others. They can meet people, fight loneliness, and shed social isolation. Many people who lead busy lives find that the only time they have to spend with friends is when exercising together. In fact, almost 90% of exercise program participants prefer to exercise with a partner or group rather than alone. Exercising together gives people a sense of personal commitment to continue the activity and to derive social support from each other (Carron, Hausenblas, & Estabrooks, 1999).
REASONS FOR NOT EXERCISING
Despite the social, health, and personal benefits of exercising, many people still choose not to exercise, usually citing lack of time, lack of energy, and lack of motivation as their primary reasons for inactivity (Canadian Fitness and Lifestyle Research Institute, 1996). These are all factors that individuals have within their control, as opposed to environmental factors, which are often out of their control. (“Barriers to Physical Activity” shows that virtually all barriers to exercise are within the control of the individual.) This is consistent with research (McAuley, Poag, & Gleason, 1990) showing that the major reasons for attrition in an exercise program were internal and personally controllable causes (e.g., lack of motivation, time management), which are amenable to change.
A recent population-based study of over 2,200 individuals between the ages of 18 and 78 found important age and gender differences regarding reasons for not exercising (Netz, Zeev, Arnon, & Tenenbaum, 2008). For example, older adults (60-78) cited more health-related reasons (e.g., bad health, injury or disability, potential damage to health) for not exercising than their younger counterparts. In addition, older adults selected more internal barriers (e.g., I’m not the sporty type) than situational barriers (e.g., I haven’t got the energy) than younger adults. Furthermore, women, compared to men, selected more internal barriers (e.g., lack of self-discipline); since these are not easily amenable, this poses a difficult problem regarding adherence to exercise programs for these women. These findings underscore the notion that age and gender need to be considered in any discussion of reasons for not exercising.

For adolescents, some of the major barriers for participation in physical activity involve other factors such as lack of parents’ support, previous physical inactivity, siblings’ nonparticipation in physical activity, and being female (Sallis, Prochaska, & Taylor, 2000). In addition, in a recent analysis of 47 studies investigating exercise behavior that included special populations (Downs & Hausenblas, 2005), the main reasons for not exercising were (a) health issues (physical limitations, injury, poor health, pain or soreness, psychological problems); (b) inconvenience (lack of access to facilities, facility too crowded, lack of transportation, other commitments); (c) lacking motivation and energy (feeling lazy, feeling unmotivated, believing that exercise requires too much effort); (d) lacking social support (no exercise partner, no support from spouse); (e) insufficient time; and (f) lacking money (finding exercise programs too expensive). Some of the reasons most consistently given for not exercising are discussed next.

Perceived Lack of Time
The most frequent reason given for inactivity is a lack of time. In fact, 69% of truant exercisers cited lack of time as a major barrier to physical activity (Canadian Fitness and Lifestyle Research Institute, 1996). However, a closer look at schedules usually reveals that this so-called lack of time is more a perception than a reality. The problem lies in priorities—after all, people seem to find time to watch TV, hang out, or read the newspaper. When fitness professionals make programs enjoyable, satisfying, meaningful, and convenient, exercising can compete well against other leisure activities.
Lack of Energy
Many people keep such busy schedules that fatigue becomes an excuse for not exercising. In fact, 59% of nonexercisers said that lack of energy was a major barrier to physical activity. Fatigue is typically more mental than physical and often is stress related. Fitness professionals should emphasize that a brisk walk, bicycle ride, or tennis game can relieve tension and stress and be energizing as well. If these activities are structured to be fun, a person will look forward to them after a day that may be filled with hassles.
Lack of Motivation
Related to a lack of energy is a lack of sufficient motivation to sustain physical activity over a long period. It takes commitment and dedication to maintain regular physical activity when one’s life is busy with work, family, and friends. It is easy to let other aspects of life take up all your time and energy. So keeping in mind the positive benefits of physical activity becomes even more important to maintaining your motivation.
PROBLEM OF EXERCISE ADHERENCE
Once sedentary people have overcome inertia and started exercising, the next barrier they face has to do with continuing their exercising program. Evidently many people find it easier to start an exercise program than to stick with it: About 50% of participants drop out of exercise programs within the first 6 months. Figure 18.1 illustrates this steep dropoff in exercise participation during the first 6 months of an exercise program, which then essentially levels off until 18 months. Exercisers often have lapses in trying to adhere to exercise programs. A few reasons have been put forth as to why people have a problem with exercise adherence despite the fact that it is beneficial both physiologically and psychologically. These include the following:
The prescriptions are often based solely on fitness data, ignoring people’s psychological readiness to exercise.
Most exercise prescriptions are overly restrictive and are not optimal for enhancing motivation for regular exercise.
Rigid exercise prescriptions based on principles of intensity, duration, and frequency are too challenging for many people, especially beginners.

Traditional exercise prescription does not promote self-responsibility or empower people to make long-term behavior change.
However, Dishman and Buckworth (1997) noted that potential relapses may have a more limited impact if the individual plans and anticipates them, recognizes them as temporary impediments, and develops self-regulatory skills for preventing relapses to inactivity (see “Preventing a Relapse”). Finally, the importance of maintaining exercise over time (not relapsing) was shown in a recent study (Emery et al., 2003). Specifically, participants (individuals with chronic obstructive pulmonary disease) who adhered to an exercise program for a year experienced gains in cognitive functioning, functional capacity, and psychological well-being compared with those individuals who did not maintain an exercise program.
Given that exercise programs have a high relapse rate, they are like dieting, smoking cessation, or cutting down on drinking alcohol (Prochaska & Velicer, 1997). People intend to change a habit that negatively affects their health and well-being. In fact, fitness clubs traditionally have their highest new enrollments in January and February, when sedentary individuals feel charged by New Year’s resolutions to turn over a new leaf and get in shape. To accentuate the value of fitness, the marketing of exercise has accelerated in North America in a campaign of mass persuasion, with heavy advertising promoted by sportswear companies. So, why is it that some people who start an exercise program fail to stick with it, whereas others continue to make it part of their lifestyle?
THEORIES AND MODELS OF EXERCISE BEHAVIOR
One way to start answering this question is through the development of theoretical models that help us understand the process of exercise adoption and adherence (Culos-Reed, Gyurcsik, & Brawley, 2001). In this section we discuss some of the major models and theories.
Health Belief Model
The health belief model is one of the most enduring theoretical models associated with preventive health behaviors (Hayslip, Weigand, Weinberg, Richardson, & Jackson, 1996). Specifically, it stipulates that the likelihood of an individual’s engaging in preventive health behaviors (such as exercise) depends on the person’s perception of the severity of the potential illness as well as his appraisal of the costs and benefits of taking action (Becker & Maiman, 1975). An individual who believes that the potential illness is serious, that he is at risk, and that the pros of taking action outweigh the cons is likely to adopt the target health behavior. Although there has been some success in using the health belief model to predict exercise behavior, the results have been inconsistent because the model was originally developed to focus on disease, not exercise (Berger et al., 2002).
Preventing a Relapse
Unfortunately, when people start to exercise they often relapse into no exercise at all, or they exercise less frequently. Here are some tips to help prevent a relapse:
Expect and plan for lapses, such as scheduling alternative activities while on vacation.
Develop coping strategies to deal with high-risk situations (e.g., relaxation training, time management, imagery).
Replace “shoulds” with “wants” to provide more balance in your life. “Shoulds” put pressure and expectations on you.
Use positive self-talk and imagery to avoid self-dialogues focusing on relapse.
Identify situations that put you at risk and attempt to avoid or plan for these settings.
Do not view a temporary relapse as catastrophic because this undermines confidence and willpower (e.g., if you didn’t exercise for a week you are not a total failure; just start again next week).
Theory of Planned Behavior
The theory of planned behavior (Ajzen & Madden, 1986) is an extension of the theory of reasoned action (Ajzen & Fishbein, 1980). The theory of reasoned action states that intentions are the best predictors of actual behavior. Specifically, intentions are the product of an individual’s attitude toward a particular behavior and what is normative regarding the behavior (subjective norm). This subjective norm is the product of beliefs about others’ opinions and the individual’s motivation to comply with others’ opinions. For example, if you are a nonexerciser and believe that other significant people in your life (e.g., your spouse, children, friends) think you should exercise, then you may wish to do what these others want you to do.
Planned behavior theory extends the theory of reasoned action by arguing that intentions cannot be the sole predictors of behavior, especially in situations in which people might lack some control over the behavior. So in addition to the notions of subjective norms and attitudes, planned behavior theory states that perceived behavioral control—that is, people’s perceptions of their ability to perform the behavior—will also affect behavioral outcomes.
The theory of planned behavior has been useful in predicting exercise behavior, as seen in a study by Mummery and Wankel (1999). The authors found that swimmers who held positive attitudes toward training, believed that significant others wanted them to train hard (subjective norm), and held positive perceptions of their swimming ability (perceived behavioral control) formed stronger intentions to train and actually adhered to the training regimen significantly more than those who did not hold these attitudes and perceptions. Recently, behavioral intentions to increase exercise behavior have been distinguished from intentions to maintain exercise (Milne, Rodgers, Hall, & Wilson, 2008). Thus, when developing exercise interventions, the notion that exercise might unfold in phases (see transtheoretical model later in this chapter) needs to be considered. In addition, using the theory of planned behavior, e-mail messages (every other day for two weeks) were effective in increasing both intentions to exercise and actual exercise behavior compared to a control condition (Parrott, Tennant, Olejnik, & Poudevigne, 2008). Furthermore, the theory of planned behavior was extended, with self-identity and group norms added to the existing theory variables to help predict exercise behavior in adolescents (Hamilton & White, 2008). Finally, Dimmock and Banting (2009) argue that intentions, as the theory predicts, don’t necessarily influence behavior; rather the quality and strength of intentions are more important.
The importance of perceived behavioral control is also seen in a more recent study (Motl et al., 2005) that found behavioral control to be a good predictor of physical activity of more than 1,000 black and white female adolescents across a 1-year period. Along these lines, Martin and colleagues (2005) were able to predict moderate physical activity and cardiorespiratory fitness in African American children using the variables within the theory of planned behavior. Furthermore, research (Rhodes, Courneya, & Jones, 2004) indicates that personality traits should be included because they can mediate the predictions of planned behavior on exercise adherence. In addition, recent research has revealed that an individual may need to meet a certain threshold regarding perceived behavioral control and subjective norms in studies focused on predicting exercise behaviors and adherence (Rhodes & Courneya, 2005). Finally, the effectiveness of using the theory of planned behavior was demonstrated in predicting exercise intentions in non-Hodgkin’s lymphoma survivors (Courneya, Vallance, Jones, & Reiman, 2005).
Social Cognitive Theory
Social cognitive theory (Bandura, 1986, 1997, 2005) proposes that personal, behavioral, and environmental factors operate as reciprocally interacting determinants of each other. In essence, not only does the environment affect behaviors, but behaviors also affect the environment. Such personal factors as cognitions or thoughts, emotions, and physiology are also important. Despite this interaction among different factors, probably the most critical piece to this approach is an individual’s belief that he can successfully perform a behavior (self-efficacy). Self-efficacy has been shown to be a good predictor of behavior in a variety of health situations, such as smoking cessation, weight management, and recovery from heart attacks. In relation to exercise, self-efficacy theory has produced some of the most consistent findings, revealing an increase in exercise participation as self-efficacy increases (e.g., Maddison & Prapavessis, 2004; McAuley & Courneya, 1992), as well as increases in self-efficacy as exercise participation increases (McAuley & Blissmer, 2002). This important role of self-efficacy is especially the case where exercise is most challenging, such as in the initial stages of adoption or for persons with chronic diseases. For example, self-efficacy theory has predicted exercise behavior, which has been especially helpful for individuals with Type 1 and Type 2 diabetes as well as cardiovascular disease (Luszczynska & Tryburcy, 2008; Plotnikoff et al., 2008). In addition, when individuals relapse in their exercise behavior, the best predictor of whether they will resume exercise was recovery self-efficacy (Luszczynska et al., 2007). Finally, in a recent study (Martin & McCaughtry, 2008) investigating physical activity in inner-city African American children, results revealed that time spent outside and social support, as opposed to self-efficacy, were the best predictors of physical activity levels. This population has rarely been studied from a social cognitive perspective, and thus other factors besides self-efficacy may be the primary determinants of exercise behavior.
Self-Determination Theory
Self-determination theory was discussed in chapter 6 in relation to its influence on sport motivation and performance. Basically, the theory proposes that people are inherently motivated to feel connected to others within a social milieu (relatedness), to function effectively in that milieu (effectance), and to feel a sense of personal initiative in doing so (autonomy). Hagger and Chatzisarantis (2007, 2008) have summarized the recent research that has employed self-determination theory to predict exercise behavior. The studies generally indicate that participants who display autonomy in their exercise behavior (Standage, Sebire, & Loney, 2008) and have strong social support systems exhibit stronger motivation and enhanced exercise adherence. Self-determination theory was also able to predict adherence in overweight and obese participants (Edmunds, Ntoumanis, & Duda, 2007). However, since application of the theory to exercise is relatively new, additional intervention studies are needed to further test its predictions and utility in the exercise domain.
Evaluation Criteria for Theories of Health Behavior
A consensus exists that unhealthy behaviors are major causes of disease, premature death, and increased health care costs. Certainly lack of exercise has been related to many negative health outcomes (e.g., coronary heart disease, obesity). As a result, many theories (noted in this chapter) have been applied to exercise behavior. Recently, Prochaska, Wright, and Velicer (2008) provided guidelines to help evaluate the effectiveness of these different theories in predicting exercise behavior. In the following list, these are ordered from least to most important in terms of usefulness in practice and in value of enhancing health.
Clarity: The theory has well-defined terms that are operationalized and explicit.
Consistency: The components do not contradict each other.
Parsimony: The theory explains the phenomenon in the least complex manner possible.
Testability: The propositions can be tested.
Empirical adequacy: The theory predicts when a behavior change will and will not occur.
Productivity: It generates new questions and ideas and adds to the knowledge base.
Generalizability: It generalizes to other situations, places, and times.
Integration: Constructs are combined in a meaningful and systematic pattern.
Utility: It provides health-related service and is usable.
Practicality: A theory-based intervention produces greater behavior change than a placebo or a control.
Impact: Impact = reach (the percentage of the target population participating) times number of behaviors changed times efficacy (amount of change).
Transtheoretical Model
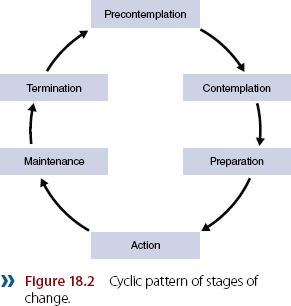
Although the models just discussed are useful as we try to grasp why people do or do not exercise, these constructs tend to focus on a given moment in time. However, the transtheoretical model (Prochaska, DiClemente, & Norcross, 1992) argues that individuals progress through stages of change and that movement across the stages is cyclic (see figure 18.2), rather than linear, because many people do not succeed in their efforts at establishing and maintaining lifestyle changes (Marcus, Buck, Pinto, & Clark, 1996). This model would argue that different interventions and information need to be tailored to match the particular stage an individual is in at the time (see “Matching the Exercise Intervention to the Individual”).
There are six stages in the transtheoretical model.
1.Precontemplation stage. In this stage, individuals do not intend to start exercising in the next 6 months. They are “couch potatoes.” People in this first stage may be demoralized about their ability to change, may be defensive because of social pressures, or may be uninformed about the long-term consequences of their behavior.


2.Contemplation stage. In this stage people seriously intend to exercise within the next 6 months. Despite their intentions, individuals usually remain in this second stage, according to research, for about 2 years. So the couch potato has a fleeting thought about starting to exercise but is unlikely to act on that thought.
3.Preparation stage. People in this stage are exercising some, perhaps less than three times a week, but not regularly. Hence, though our couch potato now exercises a bit, the activity is not regular enough to produce major benefits. In the preparation stage, individuals typically have a plan of action and have indeed taken action (in the past year or so) to make behavioral changes, such as exercising a little.
4.Action stage. Individuals in this stage exercise regularly (three or more times a week for 20 minutes or longer) but have been doing so for fewer than 6 months. This is the least stable stage; it tends to correspond with the highest risk for relapse. It is also the busiest stage, in which the most processes for change are being used. So our couch potato is now an active potato who could easily fall back into her old “couchly” ways.
5.Maintenance stage. Individuals in this stage have been exercising regularly for more than 6 months. Although they are likely to maintain regular exercise throughout the life span except for time-outs because of injury or other health-related problems, boredom and loss of focus can become a problem. In essence, sometimes the constant vigilance initially required to establish a new habit is tiring and difficult to maintain. Ideally the exerciser works to reinforce the gains made through the various stages to help prevent a relapse. Although most studies testing the transtheoretical model have focused on the earlier stages, Fallon, Hausenblas, and Nigg (2005) focused on the later stages (e.g., maintenance). Results revealed that increasing self-efficacy to overcome barriers to exercise was a critical factor for both males and females to continue exercising. In addition, people in the maintenance phase were found to be more intrinsically than extrinsically motivated (Buckworth et al., 2007).
6. Termination stage. Once an exerciser has stayed in this stage for 5 years, the individual is considered to have exited from the cycle of change, and relapse simply does not occur. At this stage, one is truly an active potato—and for a lifetime. In an interesting study, Cardinal (1997) found that approximately 16% of participants (more than 550) indicated that they were in the termination stage (criteria of 5 or more years of continuous involvement in physical activity and 100% self-efficacy in an ability to remain physically active for life). Cardinal concluded that individuals in the termination stage are resistant to relapse despite common barriers to exercise such as lack of time, no energy, low motivation, and bad weather.
In a large worksite promotion project (Marcus, Banspach, et al., 1992), participants were classified into the following categories: (a) 24% in precontemplation, (b) 33% in contemplation, (c) 10% in preparation, (d) 11% in action, and (e) 22% in maintenance. This approximate distribution pattern of the stages of change is found for other behaviors as well, such as smoking cessation and weight control. Researchers have found that when there is a mismatch between the stage of change and the intervention strategy, attrition is high. Therefore, matching treatment strategies to an individual’s stage of change is important to improve adherence and reduce attrition.
In making decisions about exercise, people go through a kind of cost–benefit analysis called decisional balance. Specifically, when people are considering a change in lifestyle, they weigh the pros and cons of a given behavior (e.g., Should I begin exercising?). In one study, researchers found that in the precontemplation and contemplation stages, the cons are usually greater than the pros. However, a crossover of the balance then occurs in the preparation stage, and the pros outweigh the cons in the action and maintenance stages (Prochaska et al., 1994). This is consistent with research (Landry & Solmon, 2004) using African American women, which found that motives for exercise become more internal as participants progressed through stages. Thus, approaches that focus on a sense of guilt or obligation, rather than fostering self-motivation, may actually have a negative effect on adherence. Therefore, exercise specialists need to help individuals who are contemplating exercise realize all of the benefits of exercise (i.e., become more intrinsically motivated) to help them move from contemplation to preparation. Finally, some contemporary research and thinking (Courneya, Friedenreich, Arthur, & Bobick, 1999) has begun to integrate different theories (in this case planned behavior and stages of change) to provide additional insights into why and how people successfully change their exercise behavior.
Physical Activity Maintenance Model
The models previously mentioned were not designed specifically for exercise adherence. To help better understand the long-term maintenance of physical activity, the physical activity maintenance model (PAM) was recently developed (Nigg, Borrelli, Maddock, & Dishman, 2008). The key aspects to the model predicting the maintenance of physical activity include
goal setting (commitment attainment, satisfaction),
self-motivation (persistence in the pursuit of behavioral goals independent of any situational constraints),
self-efficacy (confidence to overcome barriers and avoid relapse),
physical activity environment (e.g., access, aesthetics-attractiveness, enjoyable scenery, social support), and
life stress (recent life changes, everyday hassles).
The authors feel that the development of a theoretical model can provide some coherence to the literature that has identified a host of correlates and predictors of physical activity initiation and maintenance.
Ecological Models
One class of models that has recently gained support in the study of exercise behavior is the ecological model. The term ecological refers to models, frameworks, or perspectives rather than a specific set of variables (Dishman et al., 2004). The primary focus of these models is to explain how environments and behaviors affect each other, bringing into consideration intrapersonal (e.g., biological), interpersonal (e.g., family), institutional (e.g., schools), and policy (e.g., laws at all levels) influences. Although all of these environments are important, it is argued (Sallis & Owen, 1999) that physical environments are really the hallmark of these ecological models. The most provocative claim is that ecological models can have a direct impact on exercise above that provided by social cognitive models. Although earlier physical environment variables can directly affect exercise behavior, future research is needed to determine if this occurs above and beyond the influence of social cognitive factors.
DETERMINANTS OF EXERCISE ADHERENCE
Theories help us understand the process of adopting, and later maintaining, exercise habits and give us a way to study this process. Another way researchers have attempted to study adherence to exercise programs is through investigating the specific determinants of exercise behavior. In a broad sense, the determinants fall into two categories: personal factors and environmental factors.
We’ll examine each category, highlighting the most consistent specific factors related to adherence and dropout rates. Table 18.2 summarizes the positive and negative influences on adherence, along with the variables that have no influence on exercise adherence (Dishman & Buckworth, 1998, 2001; Dishman & Sallis, 1994). However, it should be noted that the determinants of physical activity are not isolated variables; rather, they influence and are influenced by each other as they contribute to behavioral outcomes (King, Oman, Brassington, Bliwise, & Haskell, 1997). For example, someone who values physical fitness and is self-motivated may be less influenced by the weather and thus more likely to exercise when it is cold than someone for whom fitness is less important and who needs more external support and motivation.
Personal Factors
We can distinguish three types of personal characteristics that may influence exercise adherence: demographic variables, cognitive variables, and behaviors. We’ll discuss these in order.
Demographic Variables
Demographic variables traditionally have had a strong association with physical activity. For example, education, income, and socioeconomic status have all been consistently and positively related to physical activity. Specifically, people with higher incomes, more education, and higher occupational status are more likely to be physically active. For example, of individuals earning less than $15,000 annually, 65% are inactive compared with 48% of those earning more than $50,000. In addition, among people with less than a high school education, 72% are sedentary compared with 50% of college-educated individuals (U.S. Centers for Disease Control and Prevention, 1993). Conversely, people who smoke and are blue-collar workers are less likely to be as physically active as their nonsmoking and white-collar counterparts.


Regarding job status, many blue-collar workers may have the attitude that their job requires enough physical activity for health and fitness, but with the use of technology in today’s industry, most workers do not expend much energy compared with workers 50 years ago. In addition, interestingly, although males have a higher level of participation in physical activity than females, there are no differences in intensity of exercise.
Finally, some recent studies have used nonwhite participants, because groups who are nonwhite have been virtually absent from the literature and probably are at higher risk for low levels of physical activity (Eyler et al., 1998; Taylor, Baranowski, & Young, 1998). Along these lines, in one study (Kimm et al., 2002), black females decreased their physical activity by 100% from ages 10 to 19 whereas white girls decreased physical activity by 64%. However, results have shown that barriers to exercise were similar between white and nonwhite individuals, although the populations differed in other determinants of exercise (King et al., 2000). Obviously this is an area that needs more research. With the current epidemic of obesity, it is instructive to note that not only do obese people find it more difficult to exercise because weight bearing is difficult, but they tend to relapse after dieting and typically regain any weight loss within 3 to 5 years.
Cognitive and Personality Variables
Many cognitive variables have been tested over the years to determine if they help predict patterns of physical activity. Of all the variables tested, self-efficacy
and self-motivation have been found to be the most consistent predictors of physical activity. Self-efficacy is simply an individual’s belief that he can successfully perform a desired behavior. Getting started in an exercise program, for example, is likely affected by the confidence one has in being able to perform the desired behavior (e.g., walking, running, aerobic dance) and keep the behavior up. Therefore, exercise specialists need to help people feel confident about their bodies through social support, encouragement, and tailoring of activities to meet their needs and abilities. Specialists also should provide beginning exercisers with a sense of success and competence in their exercise programs to enhance their desire to continue participation.
Self-motivation has also been consistently related to exercise adherence and has been found to distinguish adherents from dropouts across many settings, including adult fitness centers, preventive medicine clinics, cardiac rehabilitation units, and corporate fitness gyms (Dishman & Sallis, 1994). Evidence suggests that self-motivation may reflect self-regulatory skills, such as effective goal setting, self-monitoring of progress, and self-reinforcement, which are believed to be important in maintaining physical activity. Combined with other measures, self-motivation can predict adherence even more accurately. For example, when self-motivation scores were combined with percent body fat, about 80% of subjects were correctly predicted to be either adherents or dropouts (Dishman, 1981).
The cumulative body of evidence also supports the conclusion that beliefs about and expectations of benefits from exercise are associated with increased physical activity levels and adherence to structured physical activity programs among adults (e.g., Marcus, Pinto, Simkin, Audrain, & Taylor, 1994; Marcus et al., 2000). In fact, population-based educational campaigns can modify knowledge, attitudes, values, and beliefs regarding physical activity; these changes then can influence individuals’ intentions to be active and finally their actual level of activity. Therefore, specialists need to inform people of the benefits of regular physical activity and give them ways to overcome perceived barriers. A way to provide this type of information (see Marcus, Rossi, et al., 1992), for example, is to distribute exercise-specific manuals to participants, based on their current stage of physical activity.
Behaviors
Among studies of the many behaviors that might predict physical activity patterns in adulthood, research on a person’s previous physical activity and sport participation has produced some of the most interesting findings. In supervised programs in which activity can be directly observed, past participation in an exercise program is the most reliable predictor of current participation (Dishman & Sallis, 1994). That is, someone who has remained active in an organized program for 6 months is likely to be active a year or two later.

There is little evidence that mere participation in school sports, as opposed to a formal exercise program, in and of itself will predict adult physical activity. Similarly, there is little support for the notion that activity patterns in childhood or early adulthood are predictive of later physical activity. Evidently, the key element is that an individual has developed a fairly recent habit of being physically active during the adult years regardless of the particular physical activity pattern. However, active children who receive parental encouragement for physical activity will be more active as adults than will children who are sedentary and do not receive parental support. Along these lines, an extensive survey of some 40,000 schoolchildren in 10 European countries revealed that children whose parents, best friends, and siblings took part in sport and physical activity were much more likely themselves to take part and continue to exercise into adulthood (Wold & Anderssen, 1992). In addition, just the most active 10% of children did not have declines in physical activity from ages 12 to 18. These results underscore the importance of adults’ encouraging youngsters and getting them involved in regular physical activity and sport participation early in life, as well as serving as positive role models.
Environmental Factors
Environmental factors can help or hinder regular participation in physical activity. These factors include the social environment (e.g., family and peers), the physical environment (e.g., weather, time pressures, and distance from facilities), and characteristics of the physical activity (e.g., intensity and duration of the exercise bout). Environments (i.e., communities) that promote increased activity—offering easily accessible facilities and removing real and perceived barriers to an exercise routine—are probably necessary for the successful maintenance of changes in exercise behavior. For example, adherence to physical activity is higher when individuals live or work closer to a fitness club, receive support from their spouse for the activity, and can manage their time effectively. Although most of the determinants studied in the past have been demographic, personal, behavioral, psychological, and programmatic factors, more attention has been given recently to environmental variables (Sallis & Owen, 1999).
Social Environment
Social support is a key aspect of one’s social environment, and such support from family and friends has consistently been linked to physical activity and adherence to structured exercise programs among adults (USDHHS, 1996). A spouse has great influence on exercise adherence, and a spouse’s attitude can exert even more influence than one’s own attitude (Dishman, 1994). In the Ontario Exercise-Heart Collaborative Study (Oldridge & Jones, 1983), the dropout rate among patients whose spouses were indifferent or negative toward the program was three times greater than among patients whose spouses were supportive and more enthusiastic. Similarly, Raglin (2001a) found a dropout rate for married-singles (only one person from a married couple exercising) of 43%, whereas for married-pairs (both people in the exercise program) the dropout rate was only 6.3%. Thus, actually taking part in an exercise program provides a great deal of support for a spouse. Social support was also found to be effective in injury rehabilitation settings (Levy, Remco, Polman, Nicholls, & Marchant, 2009). Specifically, athletes felt that social support helped them cope with the stress of being injured and not being able to participate in their sport. Friends, family, and the physiotherapist were seen as offering different types of social support (e.g., task support, emotional support). Finally, a review by Carron, Hausenblas, and Mack (1996) found that for social variables, influence of support by family and important others on attitudes about exercise was the strongest predictor of adherence.

Exercise professionals can use a participant’s family or spousal support to arrange an orientation session for family members, such as educating spouses on all aspects of the exercise program to foster their understanding of the goals. In Erling and Oldridge’s (1985) cardiac rehabilitation study, the dropout rate, which had been 56% before initiation of a spouse program, decreased to only 10% for patients with a spouse in the support program. Encouragement for a friend, family member, or peer who is trying to get back to or stay in an exercise program can be as simple as saying, “Way to go” or “I’m proud of you.”
Physical Environment
A convenient location is important for regular participation in community-based exercise programs. Both the perceived convenience and the actual proximity to home or worksite are factors that consistently affect whether someone chooses to exercise and adheres to a supervised exercise program (King, Blair, & Bild, 1992). The closer to a person’s home or work the exercise setting is, the greater the likelihood that the individual will begin and stay with a program. Such locations as schools and recreation centers offer potentially effective venues for community-based physical activity programs (Smith & Biddle, 1995). Along these lines, King and colleagues (2000) found that approximately two-thirds of the women in their study expressed a preference for undertaking physical activity on their own in their neighborhood rather than going to a fitness facility. In addition, Sallis (2000) argued that one of the major reasons for the current epidemic of inactive lifestyles is the modern built environment, whose design includes formidable barriers to physical activity such as a lack of biking and walking trails, parks, and other open places where physical activity could occur.
Besides the actual location of the physical activity is the climate or season, with activity levels lowest in winter and highest in summer. In addition, from observational studies, the time spent outdoors is one of the best correlates of physical activity in preschool children (Kohl & Hobbs, 1998).

Still, the most prevalent and principal reason people give for dropping out of supervised clinical and community exercise programs is a perceived lack of time (Dishman & Buckworth, 1997). When time seems short, people typically drop exercise. How many times have you heard someone say, “I’d like to exercise but I just don’t have the time”? For many people, however, this perceived lack of time reflects a more basic lack of interest or commitment. Regular exercisers are at least as likely as sedentary people to view time as a barrier to exercise. For example, women who work outside the home are more likely than those who do not to exercise regularly, and single parents are more physically active than parents in two-parent families. So it is not clear that time constraints truly predict or determine exercise participation. Rather, physical inactivity may have to do more with poor time management skills than with too little time. Therefore, helping new exercisers deal more effectively with the decision of when to exercise might be especially beneficial.
Although lack of time has been cited as a major reason for physical inactivity, home exercise equipment has not solved the inactivity problem. For example, Americans spent nearly three times as much on home exercise equipment in 1996 as in 1986 (1.2–3 billion). However, during that period, moderate to vigorous physical activity increased only 2%, and a lot of that equipment ended up in people’s garages and closets.
Physical Activity Characteristics
The success or failure of exercise programs can depend on several structural factors. Some of the more important factors are the intensity, frequency, and duration of the exercise; whether the exercise is done in a group or alone; and qualities of the exercise leader.
Exercise Intensity, Frequency, and Duration Discomfort during exercise can certainly affect adherence to a program. High-intensity exercise is more stressful on the system than low-intensity exercise, especially for people who have been sedentary. People in walking programs, for example, continue their regimens longer than do people in running programs. One study showed that dropout rates (25%–35%) with a moderate-level activity are only about half what is seen (50%) for vigorous exercise (Sallis et al., 1986). Furthermore, research indicated that adherence rates in exercise programs were best when individuals were exercising at 50% of their aerobic capacity or less (Dishman & Buckworth, 1997; USDHHS, 1996). Williams (2007, 2008) provides evidence that individuals (especially those who were inactive, obese, or both) who chose self-paced intensities that produced positive affect exhibited higher levels of adherence. This is contrary to many recommendations that individuals should exercise at a certain intensity level. Williams concludes that allowing participants to select intensity levels related to pleasant feelings while avoiding exercise that elicits unpleasant feelings can be particularly helpful in terms of adherence for obese and sedentary individu als, who often exhibit discomfort when exercising (and subsequently drop out).
Finally, most recently, research has revealed that the level of past activity may moderate the effects of exercise intensity on adherence (Anton et al., 2005). Specifically, it was found that participants with higher levels of past physical activity exhibited better adherence to higher-intensity exercise but tended to have poorer adherence to moderate-intensity exercise. Thus, an individual’s prior exercise experience should be considered when prescribing an exercise regimen.
Different recommendations regarding the frequency and duration of exercise have been made by different scholarly organizations. For example, the American College of Sports Medicine and the Centers for Disease Control recommend that people accumulate 30 minutes or more of moderate-intensity physical activity most days of the week to encourage sedentary people (who usually do very little physical activity) to perform activities such as gardening, walking, and household chores in short dosages (e.g., 5-10 minutes). Other groups such as the Food and Nutrition Board of the Institute of Medicine recommend at least 1 hour per day of moderate-intensity physical activity (Couzin, 2002). However, research has revealed that multiple short bouts of exercise led to similar long-term increases in physical activity and weight loss compared with traditional longer sessions of 30 minutes or longer (Jakicic, Winters, Lang, & Wing, 1999). Thus, the key point is that people need to get regular physical activity, and there appears no best way to accomplish this goal.
More vigorous physical activity carries a greater risk for injury. In fact, injury is the most common reason given for the most recent relapse from exercise, and participants who report temporary injuries are less likely than healthy individuals to report vigorous exercise (Dishman & Buckworth, 1997). In starting an exercise program, many people try to do too much the first couple of times out and wind up with sore muscles, injuries to soft tissues, or orthopedic problems. Of course, they find such injury just the excuse they need to quit exercising. The message to give them is that it is much better to do some moderate exercise than try to shape up in a few weeks by doing too much, too soon.
Comparing Group With Individual Programs Group exercising leads to better adherence than exercising alone does (Dishman & Buckworth, 1996). Group programs offer enjoyment, social support, an increased sense of personal commitment to continue, and an opportunity to compare progress and fitness levels with others. One reason people exercise is for affiliation. Being part of a group fulfills this need and also provides other psychological and physiological benefits. There tends to be a greater commitment to exercise when others are counting on you. For example, if you and a friend agree to meet at 7 AM four times a week to run for 30 minutes, you are likely to keep each appointment so that you don’t disappoint your friend. Although group programs are more effective in general than individual programs, certain people prefer to exercise alone for convenience. In fact, about 25% of regular exercisers almost always exercise alone. Therefore, it is important for exercise leaders to understand the desires of participants to exercise in a group or alone.
Leader Qualities Although little empirical research has been conducted in the area, anecdotal reports suggest that program leadership is important in determining the success of an exercise program. A good leader can compensate to some extent for other program deficiencies, such as a lack of space or equipment. By the same token, weak leadership can result in a breakdown in the program, regardless of how elaborate the facility is. This underscores the importance of evaluating not only a program’s activities and facilities but also the expertise and personality of the program leaders. Good leaders are knowledgeable, are likeable, and show concern for safety and psychological comfort. Bray, Millen, Eidsness, and Leuzinger (2005) found that a leadership style that was socially enriched with an emphasis on being interactive, encouraging, and energetic, as well as providing face-to-face feedback and encouragement, produced the most enjoyment in novice exercisers. In addition, Loughead, Patterson, and Carron (2008) found that exercise leaders who promoted task cohesion (i.e., everyone in the group should be focused on improving fitness in one way or another) actually enhanced feelings of group cohesion and positive affect in individual members of the group. Thus, an interaction of leadership style and characteristics of the program produced the greatest enjoyment, which has been shown to affect exercise adherence.
Adherence to Mental Training Programs
Intervention research has traditionally focused on adherence to exercise programs. However, more recent research has focused on adherence to psychological training programs (Shambrook & Bull, 1999). The following summarizes how to promote adherence to sport psychology training programs:
Integrate psychological skills into existing routines and practice.
Reduce perceived costs (not enough time) that are associated with using a mental training program.
Reinforce athletes’ feelings of enjoyment gained from using mental training strategies.
Show relationship between mental training and achievement of personal goals.
Individualize mental training programs as much as possible.
Promote mental training as much as possible before the individual starts to work on specific mental training exercises.
An exercise leader may not be equally effective in all situations. Take the examples of Jane Fonda, Richard Simmons, and Arnold Schwarzenegger, all of whom have had a large impact on fitness programs. Although they are all successful leaders, they appeal to different types of people. Thus, an individual trying to start an exercise program should find a good match in style with a leader who is appealing and motivating to that person. Finally, Smith and Biddle (1995) noted that programs in Europe have recently been developed to train and empower leaders to promote physical activity. These have focused on behavioral change strategies rather than teaching a repertoire of physical movement skills.
SETTINGS FOR EXERCISE INTERVENTIONS
In their in-depth review of literature, Dishman and Buckworth (1996) were among the first to systematically investigate the role of the exercise setting in relation to the effectiveness of exercise interventions. They found that school-based interventions had modest success, whereas the typical interventions conducted in worksites, health care facilities, and homes have been virtually ineffective. However, interventions applied in community settings have been the most successful. The Task Force on Community Preventive Services, after reviewing the literature, recommended the following as the most effective types of community interventions (Kahn et al., 2002).
Informational interventions that used “point-of-decision” prompts to encourage stair use or community-wide campaigns
Behavioral or social interventions that used school-based physical education, social support in community settings, or individually tailored health behavior change
Environmental and policy interventions that created or enhanced access to places for physical activity combined with informational outreach activity
An example of a successful community-based program is the Community Health Assessment and Promotion Project (CHAPP), sponsored by the Centers for Disease Control and Prevention. Designed to modify dietary and exercise behaviors in some 400 obese women from a predominantly black Atlanta community, CHAPP features a working coalition of various community organizations (e.g., churches, YMCAs). The program has seen participation rates of 60% to 70%, significantly higher than was typical in this community previously (Lasco et al., 1989). These findings underscore the notion, discussed earlier, that the environment can have an important influence on physical activity levels.

Promoting Physical Activity in School and Community Programs
Schools and communities have the potential to improve the health of young people by providing instruction, programs, and services that promote enjoyable, lifelong physical activity. To realize this potential, the following recommendations have been made (USDHHS et al., 1997).
Policy. Establish policies that promote enjoyable, lifelong physical activity among young people (e.g., require comprehensive, daily physical education for students in kindergarten through grade 12).
Environment. Provide physical and social environments that encourage and enable safe and enjoyable physical activity (e.g., provide time within the school day for unstructured physical activity).
Physical education. Implement physical education curricula and instruction that emphasize enjoyable participation in physical activity and that help students develop the knowledge, attitudes, motor skills, behavioral skills, and confidence needed to adopt and maintain physically active lifestyles.
Health education. Implement health education curricula and instruction that help students develop the knowledge, attitudes, behavioral skills, and confidence needed to adopt and maintain physically active lifestyles.
Extracurricular activities. Provide extracurricular activities that meet the needs of all students (e.g., provide a diversity of developmentally appropriate competitive and noncompetitive physical activity programs for all students).
Parental involvement. Include parents and guardians in physical activity instruction and in extracurricular and community physical activity programs; encourage them to support their children’s participation in enjoyable physical activities.
Personnel training. Provide training for education, coaching, recreation, health care, and other school and community personnel that imparts the knowledge and skills needed to effectively promote enjoyable, lifelong physical activity among young people.
Health services. Assess physical activity patterns among young people, counsel them about physical activity, refer them to appropriate programs, and advocate for physical activity instruction and programs for young people.
Community programs. Provide a range of developmentally appropriate community sport and recreation programs that are attractive to all people.
Evaluation. Regularly evaluate school and community physical activity instruction, programs, and facilities (every three weeks; Lombard et al., 1995).
STRATEGIES FOR ENHANCING ADHERENCE TO EXERCISE
In this chapter we have presented reasons people participate (or don’t participate) in physical activity, models of exercise behavior, and determinants of exercise adherence. Unfortunately, these reasons and factors are correlational, telling us little about the cause–effect relation between specific strategies and actual behavior. Therefore, sport psychologists have used information about the determinants of physical activity, along with the theories of behavior change discussed earlier, to develop and test the effectiveness of various strategies that may enhance exercise adherence. As you’ll recall, the transtheoretical model argues that the most effective interventions appear to match the stage of change the person is in, and therefore its proponents recommend that programs be individualized as much as possible. In making these individualized changes to enhance adherence to exercise, exercise leaders can use six different categories of strategies: (a) behavior modification approaches, (b) reinforcement approaches, (c) cognitive–behavioral approaches, (d) decision-making approaches, (e) social support approaches, and (f) intrinsic approaches. We’ll discuss each of these approaches in some detail.
Motivational Interviewing
Motivational interviewing (MI) has been defined as “a collaborative, person-centered form of guiding to elicit and strengthen motivation for change (Miller & Rollnick, 2009, p. 137). More specifically, it is a brief psychotherapeutic intervention to increase the likelihood of a client’s considering, initiating, and maintaining specific strategies to reduce harmful behavior. Although it was developed to enhance motivation in a variety of health contexts, it has been applied to adherence to exercise behavior. Brecton (2002) provides an overview of motivational interviewing, but the spirit of MI can be captured in the following principles.
It is the client’s task, not the counselor’s, to articulate and resolve the client’s ambivalence (e.g., exercise vs. not exercising).
Motivation to change is elicited from the client rather than the counselor.
The style of the counselor is more client centered (as opposed to confrontive or aggressive), letting the client figure out his ambivalence regarding exercise.
Readiness to change is not a client trait, but a fluctuating product of interpersonal interaction (i.e., the counselor might be assuming a greater readiness for change than is the case).
The client–counselor relationship is more of a partnership, with the counselor respecting the autonomy and decision making of the client.
Behavior Modification Approaches
The exhaustive review by Dishman and Buckworth (1996) showed that behavior modification approaches to improving exercise adherence consistently produced extremely positive results. Behavior modification approaches may have an impact on something in the physical environment that acts as a cue for habits of behavior. The sight and smell of food are cues to eat; the sight of a television after work is a cue to sit down and relax. If you want to promote exercise (until the exercise becomes more intrinsically motivating), one technique is to provide cues that will eventually become associated with exercise. There are interventions that attempt to do just that.
Prompts
A prompt is a cue that initiates a behavior. Prompts can be verbal (e.g., “You can hang in there”), physical (e.g., getting over a “sticking point” in weightlifting), or symbolic (e.g., workout gear in the car). The goal is to increase cues for the desired behavior and decrease cues for competing behaviors. Examples of cues to increase exercise behavior include posters, slogans, notes, placement of exercise equipment in visible locations, recruitment of social support, and performance of exercise at the same time and place every day. In one study, cartoon posters (symbolic prompts) were placed near elevators in a public building to encourage stair climbing (Brownell, Stunkard, & Albaum, 1980). In that study, the percentage of people using the stairs rather than the escalators increased from 6% to 14% within 1 month after the posters were put in place. The posters were removed, and after 3 more months, stair use returned to 6%.
In a more recent experiment (Vallerand, Vanden Auweele, Boen, Schapendonk, & Dornez, 2005), a health sign linking stair use to health and fitness was placed at a junction between the staircase and elevator, increasing stair use significantly from baseline (69%) to intervention (77%). A second intervention involved an additional e-mail sent a week later by the worksite’s doctor, pointing out the health benefits of regular stair use. Results revealed an increased stair use from 77% to 85%, although once the sign was removed stair use declined to around baseline levels at 67%. Finally, it has been shown that sending text messages regarding one’s exercise goals produced significantly more brisk walking and greater weight loss than a control condition (Prestwich, Perugini, & Hurling, 2009).
Thus, removing a prompt can have an adverse effect on adherence behavior; signs, posters, and other materials should be kept in clear view of exercisers to encourage adherence. Eventually, prompts can be gradually eliminated through a process called fading. Using a prompt less and less over time allows an individual to gain increasing independence without the sudden withdrawal of support, which occurred in the stair-climbing study. Finally, prompts can also be combined with other techniques. For example, frequent calls or prompts (once a week) resulted in three times the number of physical activity bouts than calling infrequently (every 3 weeks; Lombard, Lombard, & Winett, 1995).
Contracting
Another way to change exercise behavior is to have participants enter into a contract with the exercise practitioner. The contract typically specifies expectations, responsibilities, and contingencies for behavioral change. Contracts should include realistic goals, dates by which goals should be reached, and consequences for not meeting goals (Willis & Campbell, 1992). A different type of contract, in which participants sign a statement of intent to comply with the exercise regimen, has also been used effectively (Oldridge & Jones, 1983). Research has shown that people who sign such a statement have significantly better attendance than those who refuse to sign. Thus, people’s choosing not to sign a statement of intent to comply can be a signal that they need special measures to enhance their motivation. Finally, when contracting is used, the focus should be on helping the person take action, establishing criteria for meeting goals, and providing a means for clarifying consequences (Kanfer & Gaelick, 1986).
Reinforcement Approaches
Reinforcement, either positive or negative, is a powerful determinant of future action. To increase exercise adherence, incentives or rewards (e.g., T-shirts) can be given for staying with the program. We’ll discuss a few reinforcement interventions in detail.
Charting Attendance and Participation
Public reporting of attendance and performance is another way to increase the motivation of participants in exercise programs. Performance feedback can be made even more effective if the information is converted to a graph or chart (e.g., Franklin, 1984). The chart is helpful and motivational in that it can tell people at a glance what changes are taking place (even small changes) and whether they are on target for the behavior involved. This may be important for maintaining interest, especially later in a program when people reach the point where improvements are often small and occur less frequently.
In addition, recording and charting keep individuals constantly informed, and often the increased cognitive awareness is all that is necessary to bring about changes in the target behavior. Furthermore, if people know that their workout record is available for everyone to see, they are much more likely to strive to keep up the positive behavior (this information also tells exercise leaders, as well as other program participants, when is the right time to offer praise and encouragement). An example of public charting focusing on increasing physical activity, but also offering some rewards for goal attainment, was a program called the Miles Club (Henning, 1987) in which runners and walkers recorded their weekly mileage on a public chart. Besides public charting, a recent summary of the literature (Miche, Abraham, Whittington, McAteer, & Gupta, 2009) found that simply self-monitoring behaviors has shown to be one of the most effective ways to increase exercise adherence.
As they reached certain designated intervals, they were rewarded with engraved paperweights and gift certificates, which enhanced the desired behavior. In addition, a competition was set up among different teams of people within the program. A team challenge board posted in a prominent location generated interest and enthusiasm for the contest. This competition also improved the overall participation, and group morale increased as well.
Although not classically a charting approach (but a participation approach), including top managers in corporate fitness programs has also been a successful strategy. Involvement of top managers greatly helped the success of one fitness program (Hobson, Hoffman, Corso, & Freismuth, 1987). When employees see the company president exercising in the gymnasium or fitness facility, they often see that person in a different light and may be challenged to match the commitment. Certainly, if top managers, CEOs, and the like have the time for fitness activities, then these activities must be important to the company. However, not all managers feel comfortable exercising with their employees, and programmers must also take their needs into consideration when devising corporate physical activity programs.
Rewarding Attendance and Participation
Besides simply charting attendance and participation records, some studies have used rewards to enhance exercise adherence. In one study, two rewards were given for attendance during a 5-week jogging program: a $1 weekly deposit-return, contingent on participation, and an attendance lottery coupon to win a prize, which was awarded for each class attended. The two interventions resulted in 64% attendance, whereas subjects in a control group attended only 40% of the classes (Epstein, Wing, Thompson, & Griffiths, 1980).
An approach that has proved effective in corporate programs is for the company to pay most (but not all) of the cost of the exercise program. Researchers compared four methods of payment and found that program attendance was better when participants either received reimbursement based on attendance or split the fee with their employer. Interestingly, the lowest attendance occurred when the company paid the entire fee (Pollock, Foster, Salisbury, & Smith, 1982). Following this research, Campbell Soup Company required employees to pay $50 for the first year of participation in a program. If they exercised three times a week or more during the second year, they paid only $25. If employees continued to exercise at this rate, they paid nothing the third year (Legwold, 1987). In general, the results have been encouraging for initial attendance or adherence but less so for long-term improvement. Additional incentives or reinforcement must be provided throughout the program to encourage adherence over longer time periods.
Feedback
Providing feedback to participants on their progress can have motivational benefits. For example, Scherf and Franklin (1987) developed a data documentation system for use in a cardiac rehabilitation setting in which the participants’ body weight, resting heart rate, exercise heart rate, laps walked, laps run, and total laps after each session were recorded on individual forms. Staff members reviewed these records monthly with the participants and then returned record cards to the participants with appropriate comments. Individuals who met certain performance goals were then recognized in a monthly awards ceremony. This program resulted in improved exercise participation and adherence as well as in higher levels of motivation and enthusiasm than before the program was implemented. Giving feedback to individuals during a program session is apparently more effective than praising the whole group at the end. Specifically, a study that provided for giving individual feedback to runners produced higher levels of attendance during the program than did group feedback, and adherence levels continued to be higher 3 months after the program’s termination (Martin et al., 1984).

Cognitive–Behavioral Approaches
Cognitive–behavioral types of approaches assume that internal events (i.e., thinking) have an important role in behavior change. Two techniques that we consider here are goal setting and a technique that involves association versus dissociation.
Goal Setting
Goal setting can be a useful motivational technique and strategy to improve exercise behavior and adherence. In one study, 99% of participants who were enrolled in an intermediate fitness class set multiple, personally motivating goals for their exercise participation (Poag-DuCharme & Brawley, 1994). The exercise goals that were most often reported included increasing cardiovascular fitness (28%), toning or strengthening muscles (18%), losing weight (13%), and exercising regularly (5%). Along with these goals were multiple action plans to reach the goals, such as bringing fitness clothes to school or work (25%), attending fitness classes regularly (16%), and organizing time or work around fitness (9%).
Martin and his colleagues (1984) found that flexible goals that participants set themselves resulted in better attendance and maintenance of exercise behavior (for a 3-month span) than did fixed, instructor-set goals. Specifically, attendance rates were 83% when participants set their own goals, compared with 67% when instructors set the goals. Furthermore, 47% of those who set their own goals were still exercising 3 months after the program ended (compared with 28% of the people for whom the instructor had set goals). In other results concerning goals, time-based goals resulted in better attendance (69%) than did distance-based goals (47%). Moreover, longer-term (6-week) goal setting produced better attendance (83% vs. 71%) and better 3-month exercise maintenance (67% vs. 33%) than did weekly goal setting (Martin et al., 1984). You can find more specific guidelines for goal setting in chapter 15.
Apart from setting specific goals, a recent study investigated the influence of goals that were intrinsic in content versus those that were extrinsic (Sebire, Standage, & Vansteenkiste, 2009). Using self-determination theory as a guiding approach, the authors compared exercisers who set intrinsic goals (focusing on developing personal interests, values, and potential such as improving health) to those who set extrinsic goals (focusing outward, with pursuits directed toward external indicators of worth such as fame, wealth, and appealing image). Exercisers setting intrinsic goals reported higher levels of self-esteem, psychological well-being, psychological need satisfaction, and exercise behavior and lower levels of anxiety than exercisers setting extrinsic goals.
Karoly and colleagues (2005) investigated the role of goal setting in regular and irregular exercisers. Results revealed that irregular exercisers tended to place greater motivational significance on their interfering goals (e.g., academic, relationships, family) than did regular exercisers, who were better able to balance their goals. In essence, regular exercisers have evidently acquired the capacity to elevate the self-regulatory significance of their relatively infrequent bouts of exercise to the same level as their academic and interpersonal goals. The authors suggest that irregular exercisers should reorganize their goal systems so that exercise goals receive just as much attention as do other important goals in their lives.
Association and Dissociation
Thoughts or cognitions—what people focus their attention on—during exercising are also important to adherence to the exercise program. When the focus is on internal body feedback (e.g., how the muscles feel, or breathing), it is called association; when the focus is on the external environment (e.g., how pretty the scenery is), it is called dissociation (a distraction). Researchers have found that people who dissociate have significantly better attendance (77%) than those whose thinking is associative (58%). In a study of a 12-week exercise program, the dissociative participants were also superior in long-term maintenance of exercise after 3 months (87% vs. 37%) and 6 months (67% vs. 43%) than associative participants were (Martin et al., 1984). Focusing on the environment instead of on how the individual feels may improve exercise adherence rates because thinking about other things reduces a person’s boredom and fatigue.
Decision-Making Approaches
Whether to start an exercise program can often be a difficult decision. To help people in this decision-making process, psychologists developed a technique known as a decision balance sheet (Hoyt & Janis, 1975; Wankel, 1984; see figure 18.3). This technique can make people more aware of potential benefits and costs of an exercise program. In devising a decision balance sheet, individuals write down the anticipated consequences of exercise participation in terms of gains to self, losses to self, gains to important others, losses to important others, approval of others, disapproval of others, self-approval, and self-disapproval.
In one study, participants who completed a decision balance sheet attended 84% of the classes during a 7-week period, whereas controls attended only 40% of the classes (Hoyt & Janis, 1975). In a variant of this study, Wankel and Thompson (Wankel, 1984) compared the use of a full balance sheet to the use of a positive-only balance sheet, which deleted reference to any anticipated negative outcomes. Both types of balance sheets produced higher attendance rates than a control condition. Collectively, the evidence available demonstrates the effectiveness of involving participants in decisions before initiating an exercise program.
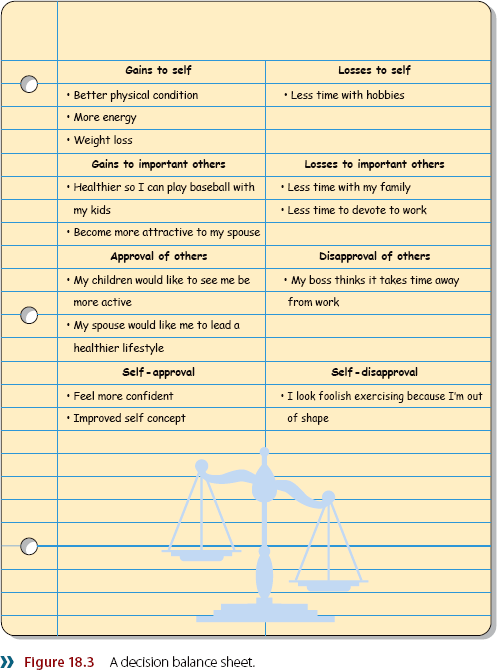
Social Support Approaches
In our context, social support refers to an individual’s favorable attitude toward someone else’s involvement in an exercise program. Social and family interactions may influence physical activity in many ways. Spouses, family members, and friends can cue exercise through verbal reminders. Significant others who exercise may model and cue physical activity by their behavior and reinforce it by their companionship during exercise. Often people give practical assistance, providing transportation, measuring exercise routes, or lending exercise clothing or equipment. In any case, social support from family and friends has been consistently and positively related to adult physical activity and adherence to structured exercise programs (USDHHS, 1996). We next provide several examples of specific social support programs.
Target Populations and Settings for Physical Activity Interventions
One way to investigate the effectiveness of physical activity interventions and strategies is to focus on the target populations and settings. For example, Gauvin and colleagues (2001) used the following categories.
1. Strategies focused on changing individuals. These types of strategies include physical activity classes, technical instruction, exercise prescription, reward systems, and mental self-control techniques. The effectiveness of the interventions studied by the investigators varied greatly, depending on the nature of the activity and the individuals involved in the program.
2. Strategies focused on networking individuals (services to link up clients to help them engage in physical activity). These strategies include changing social norms within a group (e.g., putting more emphasis on health), encouraging social support systems, and encouraging group problem solving. More data are needed to allow conclusions regarding the value of networking individuals together.
3. Strategies focused on changing the interpersonal environment. These include activity classes for families, couples, or small groups of friends; programs that involve spouses or partners of exercisers; and information sessions for families or small groups. Examples of effective programs have been observed, but there has been no systematic review of this type of focused intervention in which the change is in the interpersonal environment.
4. Strategies focused on networking interpersonal environments (services to link up couples, families, or small groups to actually participate in activities together). These include starting support or discussion groups among families regarding remaining physically active, training peers to act as models for physical activity, and offering family or small-group rates for program participation.
5. Strategies focused on changing organizations. These strategies include providing training for employees of an organization, increasing the accessibility of facilities in an organization, and changing social norms within the organization regarding exercise. Literature reviews have supported the effectiveness of these types of interventions especially when exercise facilities are convenient and available, up-to-date equipment is available, and physical activity programs are provided at the workplace itself.
6. Strategies focused on changing communities. These include increasing the accessibility of facilities within the community (e.g., bike or walking paths), creating community support networks (toll-free number for physical activity access), and modifying the structure and functioning of a community (creation of community organizations to foster physical activity). Research has indicated that community-based programs are the most effective of all physical activity settings for producing exercise initiation and adherence.
7. Strategies focused on changing the political environment. These include creating alliances to promote more effective intergovernmental cooperation and influencing political representatives to legislate for the promotion of physical activity. This is a recent initiative, but programs involving reduction of smoking through influencing the political process have proven successful.
Wankel (1984) developed a program to enhance social support that included the leader, the class, a buddy (partner), and family members. The leader regularly encouraged the participants to establish and maintain their home and buddy support systems, attempted to develop a positive class atmosphere, and ensured that class attendance and social support charts were systematically marked. Results showed that participants receiving social support had better attendance than did the members of a control group. Hobson and colleagues (1987) found that establishing a buddy system helps participants overcome the initial anxiety of beginning a program as well as encouraging continued participation.
King and Frederiksen (1984) set up three- or four-member groups and instructed people in them to jog with at least one group member throughout the study. In addition, the groups took part in team-building exercises to promote group cohesiveness. These small social support groups increased attendance and improved exercise behavior. The fact that exercise adherence improves when a leader gives personalized, immediate feedback and praises attendance and maintenance of exercise (Martin et al., 1984) also shows the importance of social support.
Intrinsic Approaches
Most of the approaches discussed so far rely on some sort of “gimmick,” knowledge, feedback, or reward system to enhance exercise behavior. Although these cues and rewards can certainly help improve exercise adherence, we all know that the most lasting motivation comes from within. We have learned the hard way (from research on attempted cessation from smoking, alcohol, and other negative behaviors) that most people do not change their exercise behavior over the long term based on extrinsic rewards or consequences. People do start an exercise program for extrinsic reasons (e.g., losing weight, decreasing the probability of certain disease states) and many times have initial success. But follow-up studies conducted years later typically show that people never really changed their lifestyle in a way that made exercise fun and enjoyable, so that they could keep it up for a lifetime. We focus next on two ways to enhance the enjoyment and fun of exercising.
Focus on the Experience Itself
Instead of trying to reach some external goal such as losing weight, the focus needs to be on changing the quality of the exercise experience. Although most people understand the desired outcomes of exercise, few understand the inner skills that are critical to being physically active on a regular basis (Kimiecik, 2002). Similarly, Maddux (1997) argued that people should exercise mindfully and focus on the present moment—in essence, should engage in exercise for its own sake instead of some future gain. For example, Maddux suggested that regarding running, we should tell people the following:
Do not run thinking anything at all. Just run. Just take one step at a time. Just be in the present moment. If you experience discomfort or even pain, notice that. If you have thoughts about stopping, notice that too. The focus on the present and the activity itself, will make the activity enjoyable over the long haul. (p. 343)
Focus on the Process
One way to make physical activity more enjoyable is to focus on the process instead of the product of the movement activities. In essence, we must move from an extrinsic orientation to an intrinsic one. Without this transformation, many people will drop out of an exercise program or bounce from one exercise program to the next (Kimiecik, 1998). Research has revealed that the focus on process, as opposed to outcome, is related to long-term maintenance of exercise (Field & Steinhart, 1992). People who focus on outcome usually run into the various societal and physical barriers discussed earlier. So to become lifelong exercisers, individuals need to make the shift from being more outcome oriented to being more process oriented.
Engage in Purposeful and Meaningful Physical Activity
In an interesting approach, Morgan (2001) argued that one of the key reasons that exercise adherence has hovered around 50% for over 30 years is that activities prescribed for individuals often lack meaning and purpose for participants. Morgan persuasively argued that many activities such as stair climbing, treadmill walking or running, weightlifting, biking, and rowing tend to be regarded as nonpurposeful activities, yet they are just the type of activities that are prescribed in exercise programs. Several authors (e.g., Fahlberg & Fahlberg, 1990; Kretchmar, 2001) have noted that meaning is the key aspect of continued exercise. Kretchmar provided case studies of 10 exercisers (mostly walkers) who had maintained an exercise regimen from anywhere from 5 to 79 years. In addition, Kasch (2001) reported a 33-year longitudinal study of 15 individuals who had an adherence rate of 100% after this long time period. Although some alternative explanations can be put forth, these authors argue that the consistent factor among these longtime exercisers is that the physical activity was purposeful and meaningful to them. Thus, when we are designing exercise programs, we need to consider the interests of the particular people involved if we are to overcome the 50% dropout rate that has plagued us for more than 30 years.
Guidelines for Improving Exercise Adherence
Several elements have emerged as keys to enhancing adherence to exercise. We’ll consolidate these elements now into guidelines for the aspiring fitness professional.
Match the intervention to the stage of change of the participant.
Provide cues for exercises (signs, posters, cartoons).
Make the exercises enjoyable.
Tailor the intensity, duration, and frequency of the exercises.
Promote exercising with a group or friend.
Have participants sign a contract or statement of intent to comply with the exercise program.
Offer a choice of activities.
Provide rewards for attendance and participation.
Give individualized feedback.
Find a convenient place for exercising.
Have participants reward themselves for achieving certain goals.
Encourage goals to be self-set, flexible, and time based (rather than distance based).
Remind participants to focus on environmental cues (not bodily cues) when exercising.
Use small-group discussions.
Have participants complete a decision balance sheet before starting the exercise program.
Obtain social support from the participant’s spouse, family members, and peers.
Suggest keeping daily exercise logs.
Practice time management skills.
Help participants choose a purposeful physical activity.

Increasing Exercise Adherence
Jennifer was hired at a local fitness facility. The club owners told her that her major job would be to increase member participation in and adherence to exercise—that is, to get and keep people exercising. Jennifer devised a plan she could implement after the first of the year, when attendance was typically highest.
First Jennifer called a meeting of all the fitness instructors at the club. She wanted both to get input from the instructors about keeping people exercising and to present her philosophy on exercise adherence so that her staff would know where she was coming from. She detailed the problems in keeping members coming back, made several suggestions about what could and would be done to change things, and emphasized that the instructors would all need to work together and support each other to put the new programs into action. Perhaps most important, she explained to her staff that people are in different stages when it comes to exercising (see the transtheoretical model) and that it’s important to individualize the exercise intervention as much as possible to correspond to the particular stage a person might be in at a particular time.
The first step was for the instructors to set aside time to meet with each member one-on-one for 30 minutes. In these meetings, members were asked to complete a decision balance sheet, noting the potential benefits and costs of participation in the exercise program. They were also asked what barriers might potentially prevent them from staying with the program and what the club could do to help them in their quest to stay in shape. Finally, members were asked to set some flexible short- and long-term goals for themselves, which were written down for both the member and the exercise leader.
This information helped Jennifer fine-tune the program and open up communication lines between the members and exercise leaders. Several themes emerged from these individual meetings, and Jennifer tried to tailor the club’s program to meet the needs of the majority of the members. She then summarized and shared this information with her staff.
Jennifer soon scheduled exercise programs and classes at the times that members said were convenient (because time and inconvenience were major factors in whether members exercised). The scheduling was flexible, and classes were held even if only a few members could attend at a given time. Classes included exercises that met the minimum guidelines developed by the American College of Sports Medicine for intensity and duration to produce health benefits. A variety of exercise classes and activities were planned so that all members could find something they enjoyed doing.
Jennifer implemented a buddy system—each member was paired with another member who had been identified as having similar interests and a similar time schedule.
As an extension of the buddy system, Jennifer learned the names of members’ spouses or significant others. When possible, these people were telephoned and told how important their support was for keeping the member motivated. Spouses were encouraged to start exercising themselves, with the assistance of the trained exercise leaders at the club.
Finally, Jennifer planned contests in different categories, including best attendance record for the month, most consecutive days of attendance, and most enthusiasm (as chosen by the exercise leaders). Prizes included T-shirts, free dinners, free massages, and an extra month’s membership free.
After 6 months, Jennifer evaluated the program. She found that the attendance rate for formal exercise classes was up about 25% and that general club attendance had increased by about 20%. In addition, new memberships had increased by 30% over the previous year. Jennifer and the club owners were pleased with this progress. By using the input of the club members and her staff and the latest concepts from the research on exercise adherence, Jennifer made the program a success.
Learning Aids
Summary
1. Discuss why people do or do not exercise.
Although the notion of a fitness boom has been sold to the public, most adults still do not exercise regularly, and only a small percentage of those who do exercise actually work out enough to receive health benefits. Thus, the first problem is getting people started in an exercise program. People usually follow a program to derive the many benefits of exercise, including weight control, reduced risk of cardiovascular disease, reduction of stress and depression, enhanced self-esteem, and increased enjoyment. The major reasons why people drop out include a perceived lack of time, lack of energy, and lack of motivation.
2. Explain the different models of exercise behavior.
Theoretical models provide an introduction to the process of exercise adoption and adherence to an exercise regimen, and the major models that have been developed in this area include the health belief model, the theory of planned behavior, social cognitive theory, the physical activity maintenance model, self-determination theory, the ecological model, and the transtheoretical model. The transtheoretical model offers the advantage of accounting for the process by which individuals move through different stages of exercise adoption, exercise behavior, and exercise maintenance.
3. Describe the determinants of exercise adherence.
The determinants of exercise behavior fall into two categories: personal factors and environmental factors. Personal factors include demographic variables (e.g., gender, socioeconomic status), cognitive and personality variables (e.g., self-efficacy, knowledge of health and exercise), and behaviors (e.g., smoking, diet). Environmental factors include the social environment (e.g., social support, past family influences), the physical environment (e.g., access to facilities, weather), and the characteristics of the physical activity itself (e.g., intensity, group or individual program). Recently, the setting the intervention takes place in has also been shown to be important, with community settings producing the most adherence.
4. Identify strategies for increasing exercise adherence.
Six types of approaches are useful to increase exercise adherence. These approaches are (a) behavior modification (e.g., prompts, contracting), (b) reinforcements (e.g., charting and rewarding attendance, feedback), (c) cognitive–behavioral approach (e.g., goal setting, association or dissociation), (d) decision making (e.g., decision balance sheet), (e) social support (e.g., classmates, family), and (f) intrinsic approaches.
5. Give guidelines for improving exercise adherence.
To implement exercise programs that maximize participant adherence, a group leader should make the exercise enjoyable and convenient, provide social support, encourage exercising with a friend, provide rewards for attendance and participation, and offer participants a range of activities from which to choose.
Key Terms
health belief model
theory of planned behavior
subjective norm
social cognitive theory
self-determination theory
transtheoretical model
physical activity maintenance model
ecological model
self-monitoring
motivational interviewing
prompt
fading
association
dissociation
decision balance sheet
Review Questions
1. Why is it important to understand the reasons people start and adhere to exercise programs (as well as drop out of exercise programs)? Use data from the Department of Health and Human Services to discuss your answer.
2. Your friend is sedentary and should start a regular exercise program but doesn’t consider it important. What are three reasons you would cite to convince your friend?
3. Why is exercise adherence a problem?
4. Discuss the major points regarding the health belief model, the theory of planned behavior, and social cognitive theory as they relate to exercise behavior.
5. Discuss the transtheoretical model of behavioral change for an exerciser, including the different stages of change.
6. How does the transtheoretical model support the notion of treatment–client matching?
7. Give three examples of the cognitive and behavioral processes of changing exercise behavior.
8. Discuss three personal factors and the ways in which they affect and predict adherence rates.
9. What are the relations among body fat, risk of cardiovascular disease, and adherence? What implications do these have for the practitioner?
10. Discuss three environmental (physical and social) factors as they relate to exercise adherence and the structuring of exercise programs.
11. Discuss three different behavior modification approaches to exercise adherence, and describe studies that have found these approaches effective.
12. On the basis of research about the effects of goal setting on adherence, how would you use goals in setting up an exercise program?
13. How is a decision balance sheet used to help people stick with an exercise program? What research studies demonstrate its effectiveness?
14. Discuss two studies of the use of social support for enhancing adherence.
15. Why is the intrinsic approach to exercise adherence considered the best approach over the long term? Provide empirical evidence to support your answer.
16. Discuss three methods to reduce relapse from an exercise program.
17. Discuss three ways to enhance the adherence to mental skills programs.
18. Discuss how setting intrinsic as opposed to extrinsic goals can influence exercisers.
19. Discuss three principles of motivational interviewing.
20. Discuss three of the concepts of the physical activity maintenance model.
21. Discuss what you think are the three most important criteria for evaluation of the theories of health behavior.
22. Discuss how self-determination theory could be used to predict exercise adherence.
Critical Thinking Questions
1. You are hired as the new director of fitness by your local health and fitness club. The dropout rate has been large in the past. You know that adherence to exercise is difficult, but your boss wants you to increase participation and adherence rates. How would you go about designing a program that would maximize adherence rates? Be specific about the principles you would use and programs you would implement.
2. A big company is getting ready to build a new physical fitness facility. The company hires you as a consultant to discuss what to include in the building, where to build it, what equipment to purchase, and other factors to maximize participation by the public. Given what you know from research on the determinants of exercise adherence, what specific recommendations would you provide the company?