11 Physical Examination, Preventive Medicine, and Diagnosis in the Ferret
Robert P. Marini
Many of the methods for physical examination and diagnosis of the ferret described here represent practices developed by the author and postdoctoral veterinarians in comparative medicine. Other clinicians should adopt practices which they find most comfortable and which provide them with the desired results. A number of methods of physical examination have been described [1–4]. The normal ferret is either sleeping soundly or curiously exploring its surroundings. In two studies on sleep patterns, ferrets slept 60% or 70% of the time, with sleep architecture similar to phylogenetically ancient mammals like the opossum and platypus [5,6]. All aspects of sleep architecture exist in the ferret, but this species is characterized by more rapid eye movement (REM) sleep (approximately 24%) than other placental mammals [5]. If deep sleep behavior becomes increasingly pronounced in duration and depth, clinical evaluation for illness, particularly hypoglycemia associated with insulinoma, is warranted [7]. In addition, there can be a physiological variation in the sleep pattern as mentioned in Chapter 8; with the onset of full estrus, food intake may decrease, and jills may become irritable and sleepless.
Clinicians should first evaluate awake ferrets without interference as the animal explores its environment. Observations can thereby be made on the animal's behavior, particularly its mentation, level of alertness, strength, coordination, carriage of the head, trunk and limbs, and its ability to avoid obstacles and respond to loud sounds. Ferrets normally walk with a tucked up habitus and arched back. Digging motions to escape their enclosure and thrusting with the entire trunk to burrow beneath objects on the floor of the cage or room are typical behaviors of the normal ferret. As in other animals, the coat should be full and sleek, the eyes bright and glossy, the tongue and oral mucosa pink, and the orifices without discharge.
Once these observations have been made, the clinician can restrain the ferret by holding the animal caudal to the shoulders, such that the clinician's palm contacts either the sternum or thoracic spine, and the thumb and remainder of the hand support the caudal aspect of the forelimbs. Some parts of the physical exam can be accomplished with this method. The author prefers, however, to restrain the ferret by the scruff of the neck, allowing the animal to hang without support of the hind end (Fig. 11.1). An exception is the pregnant jill, whose hind end should be supported when the animal is restrained. A technician is therefore required for this two-handed technique (Fig. 11.2). Both restraints are generally tolerated by the ferret, but the scruff restraint is safer for the clinician. With either restraint, the physical exam should be performed the same way every time. The author prefers to start at the head, evaluating the eyes, ears, nose, and throat. Ear carriage should be symmetric; the ferret has a robust pinna reflex, and unilateral absence suggests facial nerve injury. The ears typically have a dark brown to black discharge independent of the presence of ear mites. An otoscopic examination may reveal live mites, while microscopic examination of a smear of the ceruminous discharge can reveal ova and immature forms (see Chapter 22). The eyes are evaluated for discharge, pupillary size, cataracts, ocular position, and presence of a palpebral reflex. Normal ferrets lack a menace response [8]. If abnormal vision is suspected from the signs, signalment and clinical history, direct and consensual pupillary light reflex, and a fundic exam can be performed. Albino ferrets have a spectrum of auditory and visual abnormalities, which may potentially render them deaf and visually impaired. There is evidence for auditory deficiency, but not necessarily complete deafness, in other white-faced ferrets as well, including dark-eyed whites, badger-striped, and panda ferrets [2]. Techniques for evaluating ferret hearing and brainstem auditory evoked potential (BAEP) have been published [9,10]. To the author's knowledge, the only primary investigation on the auditory defect associated with albinism or hypopigmentation in ferrets is a paper by Moore and Kowalchuk [11]. They demonstrated that albino ferrets had a reduction in the ipsilateral projections of the cochlear nucleus to the auditory midbrain (the caudal or inferior colliculus). In contrast, there is a wealth of information on abnormal visual pathways associated with albinism. Albino ferrets have aberrant reticulogeniculate projections, altered organization of the lateral geniculate nucleus, decussation patterns resulting in a 20% decrease in uncrossed projections from the retina to the superior colliculus, and ganglion cell densities of the area centralis that may correspond clinically to decreased visual acuity [12–14]. These animals have reduced binocularity and no optokinetic nystagmus, the mechanism by which the eye holds objects in place as they pass through the visual field. While the ferrets are not blind, these defects impair motion perception and contrast sensitivity [14,15].
Fig. 11.1. Shoulder and scruff restraint of the ferret.Fig. 11.2. Hind-end support of the scruffed ferret.
Next, the mouth is opened. The animal typically yawns deeply shortly after scruff restraint is initiated (Fig. 11.3). If restraining the ferret by the shoulders, the clinician can open the mouth using a tongue depressor. The teeth should be examined for tartar, as well as broken, discolored, or misshapen teeth. The mouth and oropharynx should be examined for gingivitis, oral masses, erosions, malformations, and other abnormalities. In an evaluation of the prevalence of oral pathology in 63 rescued ferrets, 95% had malocclusion of the mandibular second incisor, 94% had extrusion of canine teeth, and 76% had abrasion and attrition of teeth. Thirty-two percent of ferrets had tooth fractures, always of the canines, and 60% of those had pulp exposure. Sixty-five percent of ferrets had periodontal diseases, as evidenced by gingivitis or gingival sulcus depth of >0.5 mm [16]. Descriptions of ferret dentition and dentistry can be found in Chapter 2 and in Rosenblad, Johnson-Delaney, and Church [17–19].
Fig. 11.3. Closer view of scruff restraint of the ferret. Restraint just caudal to the head yields the most secure grip. Ferrets usually yawn shortly after the start of restraint.
Examination of the lymph nodes consists of palpation of the nodes from cranial to caudal: submandibular, prescapular, axillary, prefemoral, inguinal, and popliteal. Lymph nodes are surrounded by fat in the ferret, and enlarged nodes can be distinguished from excessive fat by palpation. Lymph nodes are firm to the touch while fat is soft. If nodes are palpable, the clinician should assess the likelihood of a reactive or neoplastic process. The perineum is examined next, including the anal sac orifices, at 3 and 9 o'clock at the mucocutaneous junction of the anus, the anogenital space, and finally, the external genitalia. The intact male ferret (hob) should have symmetry of testicular shape and size. As the clinician examines cranially, the os penis of the ferret will be palpable. The preputial opening should be examined for disorders of the apocrine tissue that surrounds it. Small abnormalities may be manifest as difficulty in exteriorizing the penile head from the prepuce. Hobs will resist this maneuver, and sedation or anesthesia is likely required. If the head is exteriorized, clinicians will note the J-shaped terminus of the os penis, the bulbous glans penis, typically vermillion in color, and the urinary meatus. Redness, swelling, and urine scalding suggest urolithiasis or other urinary tract abnormalities (see Chapters 15 and 17). In the intact, estrous female (jill), the vulva may be tumescent and enlarged to many times its anestrus size. In the spayed jill (sprite), an enlarged vulva strongly suggests adrenal-associated endocrinopathy or, far less commonly, an ovarian remnant. The tail head and tail should be examined next, the most common abnormalities being the presence of masses or alopecia, the former typically chordomas, and the latter a manifestation of adrenal-associated endocrinopathy. Fleas may be evident in this location, as well as on the dorsal cervical area or perineum.
The author prefers to palpate the abdomen while scruffing the ferret with the nondominant hand and supporting the back against his forearm. The dominant hand can then palpate the abdomen as typically done in cats, with the thumb and remaining fingers on either side of the abdomen isolating viscera and allowing them to slip through the hand while the hand is withdrawn from dorsal (hypaxial) to ventral abdomen. Hepatic, splenic, pancreatic, and adrenal masses or enlargement can be palpated. The mesenteric lymph node can also be palpated in the middorsal abdomen; the palpably enlarged mesenteric lymph node is not necessarily abnormal. Other lymph nodes, most commonly the gastroduodenal nodes, can also be palpated. Intestinal disorders may also be palpable, and excessive intestinal gas and fluidity of contents may be associated with foreign bodies, masses, and thickening and enlargement in proliferative colitis. Both kidneys can be palpated in the ferret by gently forcing the kidney against the dorsally located hypaxial musculature. The kidney should be smooth, 2.3–3.0 cm × 1.20–1.35 cm × 1.1–1.35 cm (l × w × h) in size, and uniform in its contour. The clinician will have to switch hands to palpate the contralateral kidney in this fashion. Renal cysts are common in the ferret and may be of sufficient size or location to be palpable. In the hob or gib (castrated male), caudal abdominal masses may be of prostatic origin in a ferret with adrenal-associated endocrinopathy. In the jill, abdominal palpation can reveal pregnancy; litter size may be estimated by counting the number of fetal heads. Experienced clinicians report palpation of enlarged uterine stumps in association with adrenal endocrinopathy in sprites.
The limbs of the ferret should be evaluated for range of motion, joint luxation, congenital anomalies like polydactyly, meromelia, and syndactyly, and other issues indicated by the history and signalment. Footpad abnormalities may reflect fungal infections in immunocompromised ferrets or current or past scabies infection. Distemper, which may cause footpad hyperkeratosis, is almost always fatal in the ferret.
Thoracic auscultation is similar to that of other species. The author prefers to auscult the ferret while it is restrained, as described for abdominal palpation. The ferret's heart is more caudally located than in the dog or cat, and can be found midway between the thoracic inlet and xiphisternum. Auscultation of both right and left sides may give some insight into the location of specific auscultatory abnormalities. In the author's experience, profound arrhythmias are sometimes ausculted in ferrets independent of clinical signs. Most commonly, the ferret is likely to drop beats, especially immediately after changing restraint from behind the shoulders to scruff restraint during auscultation. These arrhythmias are likely to be associated with vagal stimulation and may represent respiratory sinus arrhythmias or heart block [20]. In a retrospective series of cases of cardiac evaluations in ferrets, second or third degree atrioventricular (AV) block was seen in 40% of ferrets in which an electrocardiogram was performed [21]. Auscultation abnormalities associated with heart disease are discussed in Chapter 18.
Pulse deficit can be evaluated by simultaneous auscultation of the heart and palpation of either the femoral pulse or the abdominal aorta. Determination of pulse deficit usually requires that the ferret be restrained by an assistant. The lungs and trachea can be ausculted as in other species, recognizing that the ferret has a relatively large lung area.
Temperature, pulse, and respiration can be determined by traditional means, but evaluation of temperature should follow pulse and respiration. Ferrets object strenuously to the insertion of a thermometer into the rectum. Robust restraint is typically required, and the ferret may urinate and defecate during the procedure. The author prefers to have an assistant restrain the ferret by using one hand to scruff and the other to restrain the hind end during determination of rectal temperature. The ferret resists extension of the hind limbs; prefemoral restraint of the hind limbs is therefore preferred (Fig. 11.4). Elevated rectal temperature should be reevaluated 2–3 hours later, as transient increases (up to 104°F [40°C]) due to excitement or rough handling have been occasionally. Different authors report the normal rectal temperature of ferrets to vary between 37.5 and 40°C (99.5–104°F) [1,2,22]. A reasonable mean temperature is 39.8°C (102°F) [1]. Other methods for evaluation of temperature (e.g., aural, temporal) have not been evaluated in the ferret.
Fig. 11.4. Hind-end restraint of the ferret. While scruffing the ferret with one hand, the handler can restrain the hind end by gently squeezing the caudal abdomen just cranial to the pelvis.
Quarantine and Conditioning
Strict quarantine and isolation procedures must be instituted when new ferrets join an established colony. Ferrets should be purchased only from reputable commercial sources and should receive a thorough physical examination on arrival. Animals with sneezing, coughing, nasal discharge, fever, skin infections, diarrhea, enlarged mesenteric lymph nodes, or unthrifty appearance should be rejected or placed in isolation for further diagnostic evaluation. The minimum duration of quarantine is 10 days for animals used in chronic procedures; ferrets intended for use in acute procedures and experiments should be given a minimum duration of 3 days for acclimatization. Appropriate diagnostic tests should be done to ascertain health status (Table 11.1). Depending on the use of the animal, additional hematologic and clinical serum chemistries may be performed. Ferrets may be tested for heartworm disease by the modified Knott's technique and/or enzyme-linked immunosorbent assay (ELISA), although cardiac ultrasound is considered the best method of heartworm detection in ferrets [23]. False negatives may occur with concentration tests due to immune-mediated elimination of microfilaria, unisexual infections, the low-level, transient nature of microfilaremia in the ferret, prepatent infections, and infection with sterile heartworms [24]. Serum for Aleutian disease virus status may be required for animals used in toxicology, immunology, and infectious disease research. In the author's opinion, ferrets in breeding colonies should be negative for Aleutian disease virus. Ferrets in heartworm endemic areas should be administered appropriate preventatives (see Chapter 18 for details).
Table 11.1. Preventive Medicine and Elective Procedures in Ferrets. Monthly Heartworm Prevention Should Be Considered for Ferrets in Heartworm-Endemic Regions
aThe only canine distemper vaccine currently licensed for ferrets by the USDA is PureVax (Merial Inc., Duluth, GA), a canarypox-vectored recombinant vaccine lacking adjuvants or complete virus.
bOften performed by commercial ferret suppliers prior to shipment of ferrets to pet stores or research facilities.
cOptional, depending on clinical status and risk of zoonotic spread, or potential impact on research being conducted.
dIMRAB-3 and IMRAB-3 TF, Rhone Merieux Inc., Athens, GA.
The extreme susceptibility of ferrets to canine distemper virus (CDV) requires that newly introduced ferrets be housed at the animal resource unit as far from random-source dogs as is practical. Technicians working with these dogs (whose distemper status is questionable) should not care for ferrets. Personnel working with ferrets should not keep puppies, particularly from pounds. Laboratory coats used by personnel working with ferrets should be dedicated to that purpose. Individuals with upper respiratory infections should not be allowed into the animal housing area because of the ferret's susceptibility to influenza virus. Personnel working with ferrets should also be screened for tuberculosis.
Ferret enthusiasts should be aware of potential transmission of Aleutian disease virus [25] and infectious diarrhea among animals in shelters or presented at ferret shows. The latter is a disease of high morbidity that is characterized by profuse green diarrhea (green slime disease), and is now recognized as the coronaviral infection, enzootic catarrhal enteritis [26]. Another coronavirus, the ferret systemic coronavirus, has been recently described and causes a disease similar to the dry form of feline infectious peritonitis.
Ferrets must be vaccinated against CDV. The first vaccination should be administered at 6–8 weeks of age if kits are from immune dams and at 4–5 weeks if kits are from unvaccinated dams. Additional vaccinations are given at 9–12 weeks of age, 13–14 weeks of age, and repeated yearly [27]. The half-life of maternal antibody to distemper, 7.4 days, is very similar to that seen in dogs (8.5 days); the vaccination schedule against CDV in ferrets should follow the guidelines for dogs [28]. Polyvalent vaccines available to the veterinary practitioner are effective in protecting ferrets against challenge with virulent CDV [29] but are not recommended, especially with the advent of approved, ferret-specific distemper vaccines. Because the virus is not attenuated, distemper vaccine of ferret cell culture origin should never be used. Inactivated distemper vaccine provides only a short-lived, slow-developing immunity [30]. Adverse reactions to vaccines or other medication have been described and may manifest as vomiting, diarrhea, ataxia, and fever. In the largest of several reports of vaccine-associated adverse events, 30 adverse events out of 4995 vaccine doses administered to 3857 ferrets were recorded [31]. Rates were 0.51%, 1.0%, and 0.85% for rabies virus vaccine alone, distemper virus vaccine alone, and rabies and distemper vaccines together, respectively. These rates did not differ significantly from one another. The incidence of an adverse event was independent of age, sex, and body weight, but was associated with the cumulative number of distemper vaccines received. Administration of diphenhydramine (0.5–2 mg/kg intravenously [IV], intramuscularly [IM]) and/or epinephrine (20 μg/kg subcutaneously [SQ], IV, IM, intratracheally) with standard supportive care should be initiated when vaccine-associated adverse events occur [1]. Some practitioners will administer diphendydramine (2 mg/kg IM, approximately 10 minutes prior to vaccination, or 0.5 mL/kg oral syrup—without alcohol, for children) to premedicate ferrets that are to be vaccinated [20]. Adverse events should be reported: the following web address contains instructions and an electronic “Adverse Event Report” form (http://www.aphis.usda.gov/animal_health/vet_biologics/vb_adverse_event.shtml). Vaccine site fibrosarcomas have also been reported in ferrets [32,33]. Investigators using ferrets for tracheal epithelial cell culture should allow 2 weeks to elapse between cell isolation and vaccination of ferrets with a modified live CDV vaccine [34]. Use within 2 weeks of vaccination has been associated with contamination of primary cell culture with CDV [34]. The only canine distemper vaccine currently licensed for ferrets by the US Department of Agriculture (USDA) is PureVax (Merial Inc., Duluth, GA), a canarypox-vectored recombinant vaccine lacking adjuvants or complete virus. The adverse reaction rate reported by Merial is 0.3%.
Ferrets are susceptible to rabies and are assumed to be capable of transmitting the virus. Commercially produced vaccine, the only vaccines approved and licensed for ferrets by the USDA, are IMRAB-3 and IMRAB-3 TF, also from Merial Inc. Animals 3 months of age or older can be vaccinated by SQ injection of 1 mL of the vaccine. A second dose should be administered 1 year after the first and boostered annually. In 1997, the Rabies Compendium Committee of the National Association of State Public Health Veterinarians (NASPHV) announced that “ferrets are now included with dogs and cats in all recommendations regarding vaccination, removal of strays, preexposure vaccination, and management of animals that bite humans. These changes were unanimously agreed to by the committee after hearing a report on the final rabies viral study of ferrets in which a variety of bat rabies virus strains were used to infect ferrets.” The compendium recommendations were the result of a 3-year study conducted by Kansas State University, the Centers for Disease Control, and the US Public Health Service. This study indicated that “in all but one experimentally-infected ferret, shedding was concomitant with onset of recognizable signs; one animal may have shed virus for as long as 4 days prior to onset of signs. The longest an animal may have shed virus prior to death was 6 days. A confinement and observation period of 10 days after a ferret bites a person should be sufficient to protect public health.” The NASPHV currently states that “Experimental and historic evidence document that dogs, cats and ferrets shed virus a few days prior to clinical onset and during illness” … and that … “Local governments should initiate and maintain effective programs to ensure vaccination of all dogs, cats and ferrets.” [35]. Moreover, the compendium recommends proof of vaccination for ferrets being transported between states, commonwealths, or territories of the United States. See Chapter 9 for more details on regulatory issues concerning ferrets, rabies prophylaxis, and postexposure management of ferrets exposed to confirmed or suspected rabid animals [36].
A major commercial supplier of ferrets routinely vaccinates against distemper and rabies at appropriate ages, provides coccidian prevention using sulfadimethoxine and amprolium, rotationally, in drinking water, and performs ear cleaning with ivermectin and propylene glycol (see Chapter 22) at 6-week intervals and prior to shipping (Marshall BioResources, North Rose, NY).
Drug and Fluid Administration
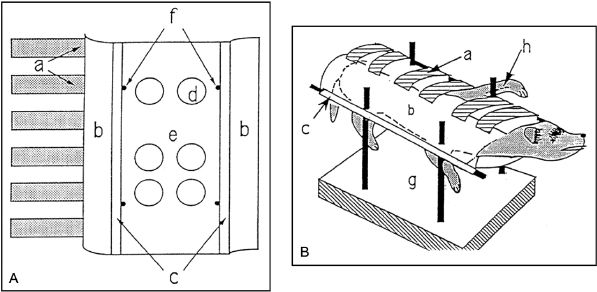
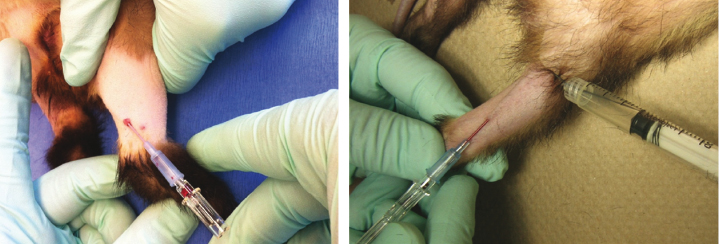
Fluids and medications may be given to ferrets by parenteral injection or oral inoculation. SQ injections can be given in the dorsal aspect of the neck. Care should be taken not to deposit the drug or fluid into the SQ fat pad, as some drugs are poorly absorbed from lipid. Some ferrets object to the administration of large volumes of fluid SQ. The author routinely administers fluid for volume replacement to ferrets by placing the animal in a deep, empty sink or induction chamber and injecting fluid SQ via a 12-inch butterfly infusion set. The clinician adjusts the position of the syringe as the animal responds. Alternatively, two-handed restraint by a technician can be used. Intraperitoneal (IP) injections are given using a 23-gauge, 1.5-in. needle placed lateral and posterior to the umbilicus. IM injections are routinely administered on the lateral aspect of the muscle mass of the thigh (quadriceps femoris); the caudal thigh muscles can also be used but perineural injection is more likely in this location. Percutaneous IV injections can be given by way of the cephalic, jugular, cranial vena cava, lateral saphenous, or lateral tail veins. This procedure may require sedation with local anesthesia (or general anesthesia) and a surgical skin incision over the jugular or cephalic vein for placement of a catheter for short-term drug or fluid administration. Low-volume injections into the cephalic vein may be performed in the conscious, nonsedated ferret by having an assistant grasp the animal firmly by the scruff with one hand while extending the legs with the other [37]. The clinician can then extend the ferret's antebrachium and effect venous distension with a tourniquet (a customized syringe tourniquet or one fashioned from a rubber band and bulldog clamp or alligator clip) placed just proximal to the elbow (Fig. 11.5). Alternatively, one operator may access the cephalic vein by using a restraint device described by Yao (Fig. 11.6) [38]. Experienced clinicians can generally catheterize the cephalic, lateral saphenous, and lateral tail veins without modified cutdowns (Fig. 11.7 and Fig. 11.8). Twenty-four-gauge, over-the-needle catheters are typically used, although the cephalic and lateral tail veins of larger ferrets can accommodate a 22-gauge catheter. It may be necessary to use a 20- or 22-gauge needle to pierce the skin of ferrets prior to catheterization to avoid damage to the tip of the catheter. The cephalic veins of docile ferrets that have been accustomed to handling and restraint may be catheterized without sedation of the animal. The use of a precharged heparin lock with flush syringe and needle attached help preclude accidental dislodgment of the catheter. For prolonged IV therapy, a chronic indwelling catheter or vascular access port can be used (see later discussion on bleeding techniques).
Fig. 11.5. Cephalic venipuncture in an awake, restrained ferret.Fig. 11.6. (A) Cotton jacket. (B) Ferret restrained in jacket on stand. (a) Velcro strips; (b) dorsal flaps; (c) tunnels; (d) exit holes; (e) ventral panel; (f) holes for horizontal bars; (g) metal stand; (h) cephalic vein. (Reprinted with permission from Yao Z, Adler A, Kovar PA (1992) A restraint device for blood sampling and direct blood pressure measurement in conscious ferrets. Contemp Top 31: 19.)Fig. 11.7. Insertion of 22-gauge, over-the-needle catheters into the saphenous veins of ferrets.Fig. 11.8. Use of a 22-gauge needle to pre-pierce the skin for subsequent catheterization of the lateral tail vein. Note also the syringe tourniquet.
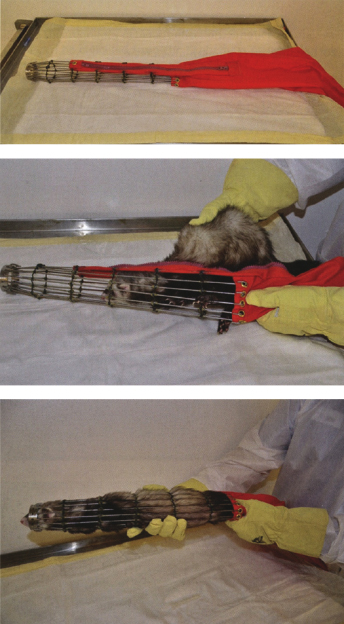
Mechanical restraint for various procedures can also be achieved using a plexiglass tube with conical end and butt plate or a tamarack holding cone [39]. The latter is a device developed for restraint of the pine marten and consists of a collapsible cage attached to a zippered bag (Fig. 11.9). The ferret can be placed into the bag and then coaxed into the cage. The collapsible bag allows technicians to restrain the animal in the cage, and the cage's design allows easy access to the ferret. After the procedure, the ferret is removed by unzipping the bag and gently backing the animal out of the cage [39].
Fig. 11.9. From top to bottom: The tamarack cone. Placing the ferret into the cone. The ferret restrained in the cone. (Reprinted with permission from Matchett CA, Marr R, Berard FM, Cawthon AG, Swing SP (2012). Experimental methodology: the laboratory ferret. Boca Raton, FL: CRC Press, pp. 63–87.)
Another method of fluid and drug administration in younger ferrets and adults that are difficult to catheterize is the intraosseous route as described for dogs and cats [27,40–42]. A modification of the femoral bone marrow collection technique described later in this chapter may be used. Orcutt suggests a 20- to 22-gauge hypodermic needle, fitted with surgical steel wire, as an alternative to the preferred spinal needle if the latter is unavailable [43]. A report of pyloric adenocarcinoma in the ferret alludes to intraosseous administration of lactated Ringer's solution, dexamethasone, and dextrose [42]. Potential complications of intraosseous administration include osteomyelitis, fat embolism, and epiphyseal damage.
Oral Dosing
Ferrets can be given drugs or fluids orally with a rodent-dosing needle and syringe or a plastic dispensing dropper (Fig. 11.10). Adults drink at about the rate of 10 mL/min, up to 100 mL during a session [44]. One can manage anorectic ferrets by oral gavage of their customary diet blended into slurry that passes through a shortened red rubber catheter or syringe orifice (approximately 5–10 mL) three to four times daily. Alternatively, one can pass a stomach tube with a maximum diameter of 5 mm orally through a speculum. We have routinely administered up to 50 mL orally via stomach tube to adult ferrets with no adverse results. During this procedure, the animal was held on its back, with the head held securely. Sedation may be required during tube insertion because the animal may struggle or vomit (see Chapter 12). Proper placement of the tube is essential because mechanical stimulation of the tracheal mucosa does not elicit a cough reflex in the ferret [45].
The administration of medication to ferrets in capsule or tablet form is easily performed by experienced personnel. When oral medication (capsule or tablet) is required, it is advisable first to remove the medicated powder from the capsule or to pulverize the tablet. The medication can then be mixed into a vitamin supplement paste, Nutri-Cal for Ferrets (Tomlyn Products, Fort Worth, TX) or Ferretone (8 in 1, Islandia, NY) and placed on an applicator stick. Ferrets will readily ingest most of the common antimicrobial oral medications, as well as receive beneficial nutritional supplementation. Bitter medications can still be administered to reluctant ferrets by using a popsicle stick or by splitting a tongue depressor along the long axis, placing a dollop of medication and supplement paste on its end, opening the mouth of the scruff-restrained ferret with the same end of the tongue depressor (or waiting for the ferret to yawn), and scraping the medication mixture off of the stick using the lingual surface of the maxillary incisors. The split tongue depressor fits readily into the space between the maxillary incisors in most adult ferrets. Medication can be dispensed in tablet or capsule form with the supplement, and the owner or technician can effectively and safely deliver the drug. Alternatively, some ferrets may accept antibiotics and other medications available or compounded as flavored suspensions.
Bleeding Techniques
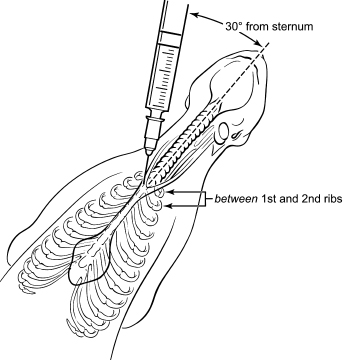
The author's preferred site for blood collection in the ferret is the jugular vein. Otto et al. [37] have described a towel-wrapping technique that allows jugular venipuncture in the conscious ferret (Fig. 11.11). The ferret is restrained manually by grasping the scruff, and is suspended vertically, while a second person shaves the ventral surface of the neck from the angle of the mandible to the thoracic inlet and then wraps the animal with a standard surgical towel. The towel is wrapped three or four times around the ferret with the cranial-most border of the towel at the level of the thoracic inlet. The forelimbs are incorporated into the wrap by maintaining them in moderate scapulohumeral flexion. The ferret is placed in dorsal recumbency and is distracted with Nutri-Cal for Ferrets or Ferretone while venipuncture is performed by the clinician. A 22- or 23-gauge needle, bent at an angle of approximately 30°, is used with a 1- to 10-mL syringe for blood collection. A technician can assist collection by using a pencil or tongue depressor to rhythmically massage the vessel from cephalad to cardiad. Moderate pressure applied to the venipuncture site immediately after needle withdrawal will avoid hematoma formation. This towel-wrapping technique may be modified to provide restraint during cephalic catheterization procedures. Yao et al. [38] have described blood collection from the cephalic veins of ferrets using either two-person restraint or a restraint device and a 23-gauge butterfly infusion set. One milliliter of blood was collected from six conscious ferrets with each restraint technique. A smaller (27 or 28) gauge needle and tuberculin syringe has also been advocated when collecting blood from the cephalic or lateral saphenous vein [1,2,46]. A technique favored by some clinicians is cranial vena cava puncture. In this technique, the ferret is restrained in dorsal recumbency, with head and neck extended and the forearms pulled caudally. The clinician advances a 1- to 3-mL syringe equipped with a 25-gauge needle into the vessel. The landmarks for initial insertion are the manubrium and first rib on the right side. The needle is placed in the notch between these sites, with its tip at 30–45° from the ventral surface of the ferret and directed toward the opposite hip or contralateral caudal-most rib. Once the skin has been pierced, generation of vacuum in the syringe through withdrawal of the plunger is used to facilitate the collection of blood (Fig. 11.12 and Fig. 11.13). The needle is inserted to the hub and then slowly withdrawn until blood appears. Depending upon the angle of entry, the site of venipuncture can be the left or right brachiocephalic trunk or cranial vena cava. The technique can be performed in awake, sedated, or anesthetized ferrets; two technicians are required for restraint in the awake ferret [1]. With awake ferrets, one technician provides scruff and forelimb restraint while another restrains the ferret at the hips. A skilled clinician who is familiar with the technique can obtain blood from this vessel without the additional need for support staff by scruffing and hanging the ferret and inserting the needle while the ferret is hanging.
Fig. 11.11. Jugular vein bleeding of the awake, restrained ferret. Insets: course of the jugular veins in the ferret and successful jugular venipuncture.Fig. 11.12. Schematic of cranial vena cava venipuncture in the ferret. (Drawing courtesy of Beth Mellor, Tufts Cummings School of Veterinary Medicine.)Fig. 11.13. Blood collection from the cranial vena cava of an anesthetized ferret. (Photograph courtesy of Joerg Mayer.)
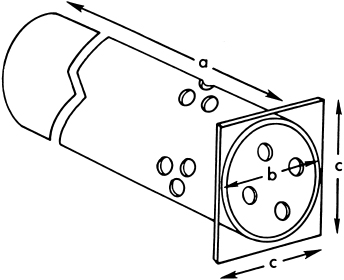
The caudal tail vein or artery can be used for blood collection [2,40,42,47–49]. Curl and Curl [48] described a restraint device that allowed serial blood collection from the caudal tail artery (<1 mL) in unanesthetized ferrets (Fig. 11.14) [48]. Using the device and a 25-gauge needle, they obtained a maximum of 12 samples from the caudal arteries of 7 ferrets within a 24-hour period. During the next 7 days, they successfully collected 10 additional samples [48].
Fig. 11.14. Restraint device for caudal tail artery bleeding. Length (a), diameter (b), and end-plate dimensions (c) differ for males and females. (Reprinted with permission from Curl JL, Curl JS (1985) Restraint device for serial blood sampling of ferrets. Lab Anim Sci 35: 296–297.)
We have used the median caudal artery for direct arterial blood pressure measurement. Using standard aseptic technique, a skin incision was made on the ventral skin surface of the tail starting approximately 3–4 cm distal to the anus and continuing caudad for 3–4 cm. The paired tendons of the sacrocaudalis ventralis lateralis muscles were encountered beneath the skin and associated SQ fat; blunt dissection of the intertendinous fascia revealed the artery. Proximal and distal control of the artery was achieved with strands of 3-0 silk. A single throw of the proximal suture was loosely placed prior to arteriotomy in anticipation of securing the catheter. Traction on the strands alone was used to manipulate the vessel for arteriotomy and catheter placement, sparing the vessel for further use. An arteriotomy was performed using spring-handle micro scissors; a catheter introducer facilitated insertion of a 24-gauge, over-the-needle catheter into the vessel. Direct arterial puncture using the stylet of the catheter may also be used for catheterization. The catheter was secured using the two strands of silk and the skin was sutured around the catheter. The catheter was removed by traction, and hemostasis was achieved by the application of pressure to the catheterization site on the tail. The tail may then be wrapped for 1 day to assure hemostasis. We have monitored mean arterial blood pressures ranging from 36 to 210 mm Hg in anesthetized ferrets using this technique. Although we have not adapted median caudal artery catheterization for use in pressure monitoring in the conscious ferret, we believe it could be used if the catheter were adequately secured with sutures and covered with a bandage.
Although not recommended, cardiac puncture in anesthetized ferrets can be used to obtain larger volumes of blood. With the animal in dorsal recumbency, an 18-gauge, 1.5-in. needle is inserted cephalad near the xyphoid cartilage at a 30°-angle, and blood is collected with a 5- or 10-mL syringe. This procedure should only be used in the terminal setting [49]. With the ease of obtaining large volumes of blood from the cranial vena cava, cardiocentesis has become a far less common technique.
Indwelling Catheters
Chronic indwelling catheters have been used for frequent and repeated blood collection and/or dosing of IV compounds [50–52]. A simplified technique has been developed in our surgical laboratory for jugular catheterization of the ferret [53]. A 5-cm midline or paramedian incision is made on the ventral aspect of the neck overlying the jugular vein. After the right jugular vein is exposed by blunt dissection, a looped section of 3-0 silk is passed beneath the vessel and cut, forming two separate strands. Both strands are loosely tied—one cardiad and one cephalad for proximal and distal control. A 46-cm section of sterile polyethylene tubing (PE 50) filled with heparinized (5 U/mL) saline solution is fitted into the shaft of a 19-gauge needle. The cephalic suture is tied off and used to apply slight traction on the vessel. Before tying off the distal suture, and during the phlebotomy, application of pressure to the jugular vein at the thoracic inlet keeps the vein engorged with blood. The 19-gauge needle is then inserted into the vessel. When the entire bevel of the needle is inside the lumen, the catheter is advanced approximately 5 cm into the lumen of the vein. The patency of the catheter is assessed before pulling the needle out. The cardiad suture is tied; further security is achieved by looping the cephalic suture around the catheter several times, tying each loop with a square knot. A stub adapter and catheter cap are used to occlude the catheter end in preparation for SQ tunneling.
The animal is next placed in ventral recumbency, and a small skin incision is made at the base of the pinna of the right ear. A thin-walled 17-gauge needle and matching stylet are inserted through the skin incision and directed SQ in a caudoventral direction until the stylet tip emerges adjacent to the site of the phlebotomy. The stylet is removed; the distal end of the catheter is disconnected from the stub adapter and inserted retrograde into the 17-gauge needle until it emerges from the skin. The needle is then removed gently, and the stub adapter is quickly refitted into the catheter, and patency is assured by flushing with saline. The skin incisions are closed with 3-0 monofilament nylon. The suture used for closing the small skin incision on the head is further used to anchor the base of the free end of the catheter via several loops of the ligature. Before its free end is heat-sealed, the patency of the catheter is again established, and the catheter is filled with heparin, heparinized saline, or another locking solution. The catheter is sealed by flaming and crimping the tip of the free end; it is coiled under bandaging tape to provide additional protection. This sealing technique not only prevents infection, but also helps to maintain patency.
Blood collection is performed by preparing the sealed end of the catheter aseptically, cutting the tip with a pair of sterile scissors, and adapting the cut end with a 23-gauge stub adapter connected to a sterile three-way stopcock. For blood withdrawal, a 3-mL syringe, half-filled with heparinized (5 U/mL) saline solution, is attached to the horizontal port of the three-way stopcock and is used to fill the system with venous blood. Blood sampling is performed with a second syringe attached to the vertical port of the stopcock. After each sampling, the catheter is flushed with heparinized saline solution. After the final blood collection, the catheter is filled with heparinized saline and heat-sealed. Unused catheters are flushed with heparinized saline twice weekly. In a study describing this technique [53], all catheterized animals were kept for a period of 4 weeks except for two ferrets, maintained for 10 and 12 weeks, respectively. At the time the ferrets were euthanized, all the catheters were patent. Gross and microscopic examination of all major organs, as well as bacterial cultures of blood samples, did not reveal infection in any of the 16 ferrets.
A tethered restraint system for ferrets has been described by Jackson [54]. The authors successfully conditioned 32 of 33 singly housed ferrets (97%) to modified guinea pig harnesses and tethers prior to jugular catheterization. Animals were considered to be fully adapted to the tethered restraint when they engaged in a normal pattern of daily activities, including grooming, eating, sleeping, and exploratory behaviors while wearing the harnesses. Catheters were 90 cm in length (0.88 mm outer diameter [OD] × 0.55 mm internal diameter [ID]) and were fitted with a polyethylene collar glued in place 10 cm from the IV end of the catheter. Both control samples (withdrawn 1–2 days postoperatively) and experimental samples (drawn 2–9 days postoperatively) were successfully collected in 25 of 30 animals (84%). In one case, an experimental sample was successfully collected on postoperative day 21. All blood collections were performed without handling the ferrets.
Yao et al. [38] reported the use of SQ-placed vascular access port catheters that had previously been placed in the left carotid arteries of ferrets, but gives no details of the procedure. These ports were used for the purpose of determining direct mean arterial blood pressure in six conscious, restrained ferrets. Vascular access ports can also be used for blood collection or for delivering chemotherapeutic agents [43,55].
Blood Transfusion
Manning and Bell [56] were unable to demonstrate naturally or experimentally induced antierythrocyte antibodies in ferrets despite reciprocal transfusion of six pairs of ferrets twice, at a 34-day interval. The absence of isoagglutinins to erythrocytes suggests that transfusion may be performed with little risk. The authors drew 6–10 mL of blood from the donor ferret into a syringe containing an aliquot of anticoagulant (A-C-D Solution, Sanofi Animal Health, Overland Park, KS) used at a ratio of 1 mL anticoagulant to 6 mL of blood. The anticoagulated blood was then administered IV to the recipient via the jugular vein. An administration set without blood filter was used and subsequently flushed twice with 0.9% saline (Fig. 11.15). There are no definitive transfusion guidelines for ferrets, although one author recommends transfusion if the packed cell volume (PCV) falls abruptly to 15% or gradually to 12% [57]. Quesenberry and Orcutt recommend transfusion to animals with hematocrits below 25% and which require surgery, display signs of anemia, or are thrombocytopenic. They further recommend use of a 22-gauge catheter to avoid hemolysis and a blood filter to avoid iatrogenic thromboembolism [1]. The following equation for estimating the volume of blood required to achieve a particular posttransfusion PCV may be used [58]:
Fig. 11.15. Blood transfusion via the jugular vein. A saline flush is being used to purge the line of the donor's blood. Inset: infusion apparatus. A blood filter can be added.
Pretransfusion and postransfusion hematocrits should be evaluated to determine the success of the procedure. Although transfusion reactions are unlikely, clinicians should evaluate ferrets closely for evidence of hemolysis, hypotension, fever, urticaria, or vomiting [58].
Bone Marrow Aspiration/Biopsy
Palley et al. described a technique of femoral bone marrow aspiration in anesthetized ferrets [59]. The skin over the coxofemoral joint was prepared aseptically and a stab incision was made over the greater trochanter using a number 15 scalpel blade. A 20-gauge, 1.5-in. spinal needle was positioned over the femur medial to the greater trochanter and was advanced using constant pressure and an alternating rotating motion (Fig. 11.16). After the needle was firmly seated within the femoral canal, a 10-mL syringe was used for aspiration of marrow by vigorous suction. Aspirates were performed on 14 ferrets with no postprocedural abnormalities and resulted in smears of excellent quality. Other sites include the iliac crest, tibial crest, or humerus. We have also used an 18-gauge Jamshidi needle to obtain bone marrow biopsy samples from a ferret. A 1.5-in., 18-gauge needle may also be used to obtain a core biopsy [26]. Analgesics should be administered, preferably preprocedurally.
Fig. 11.16. Demonstration of needle placement for bone marrow aspiration in the ferret.
Endotracheal Intubation
Endotracheal intubation may be reliably performed in the ferret and is the preferred method of administration of inhalant anesthetics. Tracheal access is required for tracheal wash, for artificial ventilation, and as a route for drug administration during cardiopulmonary crisis. Wire-reinforced tubes are preferred because they reduce the risk of airway obstruction from kinking of the endotracheal tube. Many cuffed tubes are designed in such a way that the presence of the cuff compromises one's ability to place the tube due to an increase in the total (outer) diameter of the tube. For this reason, uncuffed tubes are often advocated for small animals so that more of the tracheal diameter will be available for ventilation. The cuff design of a commercially available silicone endotracheal tube appears to eliminate this concern, allowing clinicians to use cuffed tubes without sacrificing airway diameter. After induction of anesthesia, ferrets are placed in sternal recumbency, and an assistant positions the head in extreme dorsiflexion by placing thumb and index finger on either side of the maxillae. With the other hand, the ferret's tongue is extended from the mouth, pulled over the mandibular incisors, and is used as a lever to depress the mandible. Alternatively, the handler can use gauze strips anchored by the canines to open the mouth. The laryngoscope blade may be used to exteriorize the tongue from the mouth; the tongue should be handled with gauze to provide an adequate hold. Robust lingual traction pulls the epiglottis into view. Using a curved Macintosh-1 or straight Miller size 0 laryngoscope blade, 2.5–3.5 ID, cuffed or uncuffed endotracheal tubes may be advanced under direct visualization through the rima glottidis and into the trachea. Most adult male and female ferrets can be intubated with endotracheal tubes of 3.0 mm ID. Younger animals can accommodate 2.5 mm ID uncuffed endotracheal tubes. Tubes should be lubricated with a lidocaine-containing gel or other lubricant and fitted with an appropriately sized stylet. Slight ventral deflection of the stylet tip helps to direct the tube into the trachea. Accurate placement can be assessed by observing condensation on the laryngoscope handle or a dental mirror placed close to the endotracheal tube adapter.
The ferret has been promoted as a model for pediatric endotracheal intubation training [60,61]. In the Powell study, ferrets were anesthetized with ketamine (55 mg/kg IM) and acepromazine (0.55 mg/kg IM) and placed in dorsal recumbency. Their tracheas were intubated using 2.5–3.0 mm ID uncuffed endotracheal tubes. The topical anesthetic Cetacaine (Cetylite Inc., River Road Pennsauken, NJ) was applied to the larynx with cotton-tipped applicators, and the area was illuminated with laryngoscopes fitted with size 0 and size 1 straight Miller blades. Despite its use in this study, benzocaine-containing anesthetic sprays are not required for tracheal intubation of ferrets. In a study of benzocaine-induced methemoglobinemia, a 1-second spray delivering 56 mg of benzocaine produced methemoglobinemia of varying degrees in some of the six test ferrets [62]. Benzocaine is an agent that should probably be avoided in the ferret; lidocaine-containing gels or sprays are an appropriate alternative.
Diagnostic tracheal wash can be performed in the ferret using a sterile endotracheal tube and an 8 French pediatric suction catheter (Safe-T-Vac Suction Kendall Healthcare Products, Mansfield, MA) [1]. The catheter is attached to a specimen container (Argyle Lukens Specimen Container, Sherwood Medical, St. Louis, MO) and wall suction. After intubation, the suction cannula is inserted through the endotracheal tube and advanced to the approximate location of the carina. Two milliliters of warm, sterile saline can be injected through the catheter and then aspirated into the specimen container. Surgical implantation of an intratracheal catheter for chronic administration of liquid surfactant suspensions has also been described [63].
Peritoneal Macrophage Harvest
A method of harvesting ferret peritoneal macrophages has been described. Four- to five-month-old ferrets were stimulated with 3 mL of mineral oil administered IP [64,65]. Four days post injection, the ferrets were anesthetized with a ketamine–xylazine combination, and the lower abdomen was shaved and prepared using standard aseptic techniques. Two hundred milliliters of Eagle's minimal essential medium (MEM) with Earle's salts, containing 10 U/mL of heparin, were injected IP. The distended abdomen was massaged gently for 1–2 minutes. A 14-gauge needle with attached rubber tubing was inserted into the posterior abdomen lateral to the midline. The peritoneal fluid containing the macrophages was collected in 50-mL polypropylene centrifuge tubes. Harvest of the macrophages in excess of 5 × 107 may be achieved with one peritoneal lavage.
Macrophages were centrifuged at 500× g for 15 minutes and suspended at 4 × 106 cells/mL in growth medium of MEM supplemented with 15% bovine fetal serum and gentamicin sulfate. Purified macrophages were obtained by seeding tissue culture slides with 0.15 mL of the cell suspension/well and by washing vigorously with serum-free medium to remove unattached cells [66]. The cell population was fed with 0.3 mL of growth medium/well and incubated for variable periods, depending on the assay to be performed.
Urea Breath Test
Ferrets may be naturally infected with the gastric spiral organism, Helicobacter mustelae [67]. This microaerophilic, gram-negative bacterium causes gastritis and gastric ulceration, and has been associated with gastric lymphoma and adenocarcinoma. This parallels the spectrum of clinical sequelae seen in people with Helicobacter pylori infection, for which the H. mustelae-infected ferret has become a model. Diagnostic tests include culture, urease, and polymerase chain reaction (PCR) testing of endoscopic biopsy samples (see “Gastric Endoscopy” in this chapter), evaluation of serum immunoglobulin G (IgG) ELISA titers to H. pylori, and the urea breath test. The latter test exploits the presence in gastric Helicobacters of the enzyme urease, which hydrolyzes urea to ammonia and CO2 [68]. Urease is essential to colonization of the gastric mucosa; urease-negative isogenic mutants of H. mustelae, for example, fail to colonize ferret gastric mucosa [69]. Urea labeled with the nonradioactive isotope 13C is administered to people per os, and exhaled breath is subsequently analyzed for the 13CO2. In the ferret, adult and preweaning animals were administered labeled urea and placed in sealed glass metabolism chambers. Expired air was collected into sodium hydroxide by constant rate withdrawal of air from the chamber (250 mL/min). Administration of 370 KBq of 14C-urea to adult ferrets resulted in peak production of 14CO2 1 hour after administration. Breath test activity was found to parallel quantitative cultures of H. mustelae in naive, neonatal (3–4 day old) ferret kits and correlated with H. mustelae status in adult animals subjected to various Helicobacter treatment strategies. Treatment with bismuth subcitrate, alone or in combination with amoxicillin and metronidazole, resulted in reductions both in 14CO2 production and in colony-forming units per biopsy.
Gastroscopy
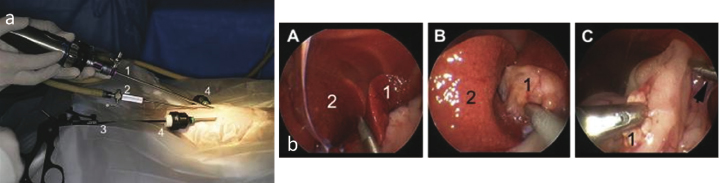
In the ferret, gastroscopy has long been used in our laboratory for the evaluation of gastric lesions subsequent to H. mustelae infection or chemically induced models of gastric cancer [67]. Investigations into bacterial virulence, infection kinetics, carcinogenesis, and antimicrobial efficacy were accomplished using a flexible pediatric bronchoscope (4.9 mm insertion tube; Pentax FB-15H, Orangeburg, NY) to access the stomach and collect mucosal biopsy samples. We also used this instrument to retrieve small gastric foreign bodies and collect gastric juice. A traditional suction bottle arrangement was used with the bronchoscope, but insufflation was achieved using a hand bulb. More recently, Divers [70,71] has described use of an 8.6-mm gastroscope for animals between 1 and 2 kg and a 2.7-mm telescope and sheath for animals less than 1 kg. Laparoscopy using multiple entry technique has also been described (Fig. 11.17).
Fig. 11.17. (a) Multiple-entry ferret laparoscopy: (1) telescope; (2) Veress needle and CO2 insufflation line; (3) 3-mm instrument inserted through (4) a 3.5-mm cannula. From left to right: (A) palpation probe between left lateral (1) and left medial (2) liver lobes; (B) thickened gall bladder (1) between the quadrate and right medial liver lobe (2); and (C) endoscopic biopsy of the pancreas (1). (Photographs courtesy of SJ Divers).
Urinary Bladder Catheterization
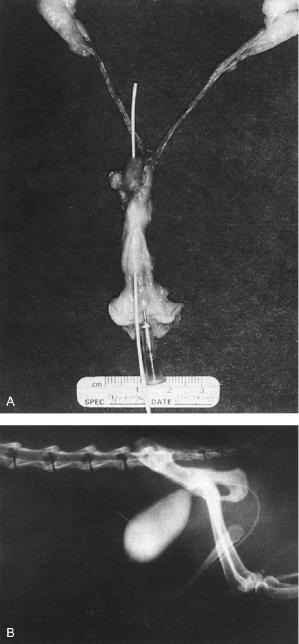
Our laboratory developed a technique for catheterization of the urinary bladder in both male and female ferrets [72]. Ten intact females, 11 spayed females, and 2 intact males were catheterized using 3.5 French red rubber urethral catheters. Catheters used for females were fitted with wire stylets (0.1-mm diameter, medium gauge (guitar) E string), while those used in males were passed without stylet. Ferrets were premedicated with atropine and anesthetized. Females were positioned in ventral recumbency with a rolled surgical towel placed beneath their abdomens to elevate the hind quarters. After routine skin preparation, a vaginal speculum was inserted through the vulvar lips and past the pelvic rim. Gentle parting of the jaws of the speculum allowed visualization of the clitoral fossa on the floor of the vestibule immediately cranial to the mucocutaneous junction, and the urethral orifice 1–1.5 cm cranial to the fossa (Fig. 11.18). The catheters were advanced into the urethra to the bladder. Urine could then be collected by gentle syringe aspiration. Spayed females were subjectively more difficult to catheterize; blind passage was occasionally required. Anesthetized males were placed in dorsal recumbency. After skin preparation, the distal tip of the penis was exteriorized from the prepuce and the urinary meatus on the ventral surface of the glans was identified. In the normal male ferret, catheters were easily advanced into the bladder; no impedance was encountered at either the os penis or the ischial arch. Clinicians having difficulty identifying the urethral opening can use eye loops or try directing a stream of saline at the mucosa immediately below the J-shaped process of the os penis.
Fig. 11.18. (A) Caudal urogenital tract of a female ferret: the needle is inserted into the clitoral fossa; the catheter is inserted into the urethra and passes through the bladder. (B) Contrast cystogram in a male ferret. (Reprinted with permission from Marini RP, Esteves MI, Fox JG (1994) A technique for catheterization of the urinary bladder in the ferret. Lab Anim 28: 155–157.)
Another catheter used in ferrets is the 3 Fr polytetrafluoroethylene urinary catheter (Slippery Sam Tomcat Urethral Catheters, Surgivet, Smith Medical, Norwell, MA). If difficulty is encountered when passing the catheter, hydropulsion can be used to assist passage. Tube cystostomy with 5–8 Fr Foley catheters can be used in animals that are azotemic and in which a urethral catheter cannot be passed [73].
Cerebrospinal Fluid (CSF) Collection
CSF can be collected from either the cerebellomedullary cistern (cisterna magna) or the L5-L6 interspace. When the L5-L6 interspace is used, only several drops can be collected. The anesthetized ferret is placed in lateral recumbency, with its head flexed, so that it is perpendicular to the spinal column. Antinoff and Giovanella recommend a 25-gauge spinal needle for CSF collection [74]. Platt et al. used 25-gauge, 1.6-cm hypodermic needles to collect CSF from the cisterna magna of 42 clinically normal ferrets [75]. The CSF dripped into a collection tube positioned below the needle [8].
Imaging
Every imaging modality used in other domestic species has been used, either diagnostically or experimentally, in the ferret. Traditional imaging technologies of radiology and ultrasound have been complimented by computerized axial tomography (CAT), magnetic resonance imaging (MRI), positron emission tomography (PET), single-photon emission computed tomography (SPECT), and nuclear scintigraphy in the care of or use of ferrets. Radiographic technique, digital or conventional, has been used in diagnosis of orthopedic, neurologic, gastrointestinal, urogenital, and cardiac conditions of the ferret. Imaging studies of spine and of gastrointestinal and urinary tracts have been published [76,77].
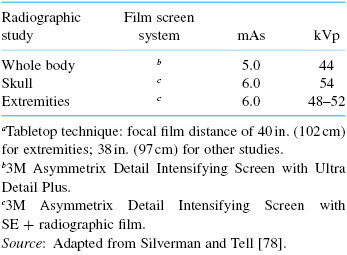
Radiographic studies are best performed in sedated (1 mg/kg midazolam) or anesthetized ferrets, although experienced handlers and technicians can often adequately restrain awake ferrets. As in other species, a minimum of two orthogonal views are required for adequate diagnosis or description of lesions. A recently published atlas of normal radiographic appearance of the ferret body is an excellent resource for clinicians [78]. General guidelines included in this text include use of an X-ray generator capable of 5–7.5 milliampere second (mAs) exposures, variable kilovoltage peak (kVp) adjustable in increments of 1–2 kVp, and rapid exposure times. Exposures of ferrets included in that text used tabletop technique and focal film distances of 40 in. (102 cm) for extremities and 38 in. (97 cm) for whole body and skull. Recommended exposure guidelines and film screen combinations are listed in Table 11.2. Positioning of ferrets is similar to that of other small animals; radiolucent tape is a helpful adjunct to sedation or anesthesia. Of special note is the appearance of the spleen, which in the normal ferret is proportionally larger than that observed in normal dogs and cats. Additionally, administration of isoflurane, and, in the author's experience, the anesthetic ketamine–xylazine, cause transient splenomegaly in the ferret. Other causes of splenomegaly in the ferret include extra medullary hematopoiesis, hypersplenism, lymphoma, and other neoplasms.
Table 11.2. Radiographic Exposure Guidelines for a 1200-Gram Ferreta
In a study of contrast radiography of the gastrointestinal tract, Schwarz et al. administered 8–13 mL/kg of barium sulfate suspension (30% w/v) to awake and ketamine/diazepam-sedated animals [76]. Radiographs were evaluated at 5, 10, 20, 40, 60, 90, 120, and 130 minutes. Gastric emptying began immediately and was complete within 1.5–2.5 hours. Residual barium was observed adhering to the gastric mucosa in most animals. Small intestinal transit time was similar and took approximately 1–2 hours. Maximal small intestinal distension was 5.9 ± 1.1 mm (mean ± SD) for unsedated ferrets and slightly larger for sedated ferrets. Among the recommendations was a radiographic sequence of survey (precontrast) right lateral and ventrodorsal (VD) projections, immediate postcontrast right and left lateral, VD and dorsoventral (DV) views, and postcontrast right lateral and VD views at 10, 20, 40, 60, 90, and 120 minutes. Barium flocculation was observed throughout the study. The use of ketamine–diazepam sedation, chosen because of its minimal effect on transit time in similar studies in the cat, was not recommended because of ptyalism and spasticity.
Silverman and Tell's work contains images of a double contrast gastrointestinal study performed in an anesthetized, 1.2-kg male ferret, obtained using esophageal administration of 20 mL of a 60% w/v barium sulfate suspension (Novopaque 60% w/v; Lafayette Pharmaceutical Inc., Lafayette, IN) followed in 30 minutes by 50 mL of air. Right lateral and VD projections are shown precontrast, and at 1, 15, 30, and 35 minutes postcontrast. An additional DV view is provided at 30–35 minutes. Colonic filling from ascending colon to rectum is evident on the 30-minute postcontrast films [78].
A technique of contrast cystography has been developed in our surgical laboratory [72]. After survey abdominal radiographs had been acquired, one male and one female were catheterized, and the bladders were drained of urine by syringe aspiration. Two-and-one-half milliliters of a 37% iodinated contrast material in a 1 : 1 dilution of saline was then infused. After cystography, contrast material was removed, and the bladder was flushed with saline three times (Fig. 11.18B).
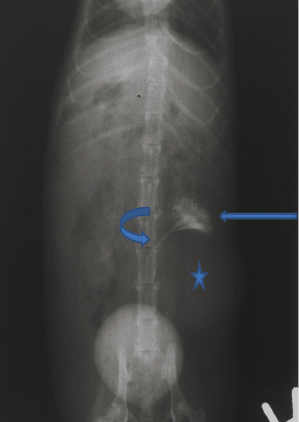
Excretory urography has been described by Silverman and Tell [78]. Precontrast radiographs of ferrets in right lateral and VD position were obtained, and a contrast medium containing 37% organically bound iodine (RenoCal-76, Bracco Diagnostics, Inc., Monroe Township, NJ) was then administered at a dose of 2.3 mL/kg IV. Films were obtained at 5, 10, 35, and 60 minutes. Application of a compression bandage composed of layers of gauze and elastic wrap cranial to the urinary bladder was used to help demonstrate the renal collecting system. Excretory urography demonstrating unilateral hydronephrosis and hydroureter is seen in Fig. 11.19.
Fig. 11.19. Ventrodorsal radiograph of excretory urography in a ferret. Note the dilatation of the renal pelvis (hydronephrosis, narrow arrow), ureter (hydroureter, curved arrow), and renal cyst (star).
Myelography is useful for demonstration of lesions which compress the spinal cord and interrupt the flow of radio-opaque dye within the subarachnoid space. It has been used to diagnose intervertebral disc disease in the ferret [77]. A 2-year-old, neutered male ferret presenting with paraplegia and normal deep pain perception and spinal reflexes of the pelvic limbs was subjected to myelography after survey radiographs revealed narrowing of the L2-L3 intervertebral space. The authors used a 1.5-in., 21-gauge hypodermic needle at the L5-L6 interspace and 0.5 mL iohexol (300 mgI/mL) to demonstrate dorsal deviation of the dye column at the L2-L3 interspace. Subsequent helical computerized tomography demonstrated hyperdense material consistent with herniated disc within the vertebral canal.
Ultrasonography is commonly used in ferrets to diagnose conditions affecting the thorax and abdomen. Lewington and Silverman and Tell recommend a 7.5–12 MHz sector scanner with a small footprint (<2 cm) [2,78]. For abdominal scans, the entire ventrum, from xiphoid process to pubis and laterally to the horizon of the abdomen's curvature to its lateral surface, should be shaved. Generous acoustic gel (warmed) can be applied. Manipulation of the viscera and kidneys through the malleable abdominal wall of the ferret facilitates identification of structures. Sedation may not be required in tractable ferrets that are adequately restrained; sedation should be used when obtaining a fine needle aspirate. Distracting the animal with Nutri-Cal for Ferrets or Ferretone may be helpful.
Silverman and Tell depict transverse and sagittal images of liver, spleen, and urinary tract and associated structures [78]. Ultrasonographic features of normal and diseased adrenal glands [79,80], urogenital lesions, pregnancy and gestational age [81], testicular tumor [82], hepatobiliary and splenic disease [83,84], ocular biometry [85], mesenteric lymph node [86], pancreatic morphology and nodules [87], and systemic coronavirus disease [88] have been published. Echocardiography is described in Chapter 18.
MRI is most commonly used in ferrets as a research tool in studies of the ontogeny and physiology of the central nervous system (CNS) and as a diagnostic tool in neurologic disease. Studies of gyrification of the CNS have offered insights into similar processes in humans, processes that are particularly important in neurodevelopmental disorders [89,90]. MRI of neonatal ferrets has also been used to gain insight into the influence of different insults (e.g., chronic hypoxia, enucleation) of interest to neonatologists treating preterm infants [91,92]. MRI with a 1.5-T magnet and human wrist coil (Sigma Unit, GE Medical Systems, Milwaukee, WI) was used to diagnose a thoracic vertebral chordoma in a ferret. Spinal cord compression and lysis of the spinous processes and laminae of T9 and 10 were visible on sagittal images [93]. Antinoff and Giovanella [74] recommend 0.2 mL/kg of gadolinium-diethylenetriamine pentaacetic acid (GI-DPTA) as a contrast agent in neurologic studies using MRI [74]. Herrera et al. used 11.7-T MRI microimaging to evaluate ex vivo larynges of normal and scarred vocal folds in ferrets [94]. Functional MRI has also been used to measure visually driven responses in anesthetized ferrets and can be used to study neural plasticity and development in ferrets [95,96].
Computed tomography (CT) has been used sporadically to assist diagnosis of various conditions in ferrets [77,97–99] and to follow progression of pulmonary disease in influenza studies [100–102]. In the influenza studies, Jonsson et al. used a small-animal imaging platform that allows PET and SPECT imaging in the same unit (Siemens Inveon Trimodal Scanner; Siemens Preclinical, Knoxville, TN) [102], while Veldhuis Kroeze et al., used a dual source ultrafast CT system (Somatom Definition Flash; Siemens Healthcare, Molecular Imaging Division, Siemens Medical Solutions USA, Inc., Hoffman Estates, IL) [100,101]. Both systems had very fast acquisition times (0.5 seconds and 0.22 seconds for the Inveon Trimodal and Somatom Scanners, respectively). Acquisition times were such that neither induced breath holding nor respiratory or electrocardiographic triggering were required to produce images without respiratory motion-generated artifacts. Progression and quantitation of pulmonary disease and vaccine efficacy was achieved by CT in these studies. Silverman and Tell depict images from transverse CT studies of ferret head, thorax, abdomen, and pelvis [78]. The instrument and software used to create these images is not reported.
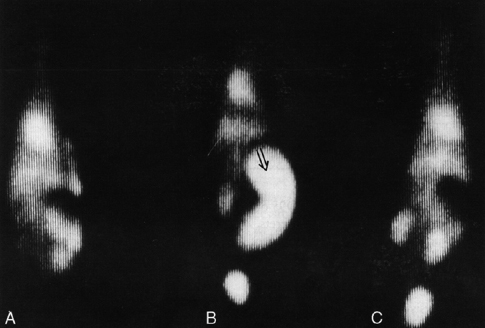
Ferrets have been used in the evaluation of lymphographic contrast agents and lymphography because lymphatic disease can be reliably produced by infection with the lymphatic filarid, Brugia malayi [103–105]. Intradermal injection of 99mtechnetium-labeled albumin (99mTc-alb) and 99mtechnetium-labeled antimony colloid (99mTc-colloid) followed by gamma camera lymphoscintigraphy were investigated as rapid, noninvasive methods of visualization of central and peripheral lymphatic structures [105]. In B. malayi-infected ferrets, uptake and transport were severely restricted, with tracer accumulating in dilated lymphatics. 99mTc-alb was found to be superior to 99mTc-colloid in visualization of lymphatic trunks, while the latter agent was superior for nodal visualization. Gamma camera scintigraphy was also used to determine the fate of 99mTc-labeled RBCs in the isoflurane-anesthetized ferret (Fig. 11.20) [106]. MRI with super paramagnetic emulsion in ferrets has also been reported [103,104].
Fig. 11.20. Composite γ camera images. (A) Conscious, preanesthetized. (B) Anesthetized by isoflurane (arrow points to spleen). (C) Conscious, revived. (Reprinted with permission from Marini RP, Callahan RJ, Jackson LR, et al. (1997) Distribution of technetium 99m-labeled red blood cells during isoflurane anesthesia in ferrets. Am J Vet Res 58: 781.)
Acknowledgment
The author is grateful to Joerg Mayer and Connie Orcutt for their review of the chapter.
References
1. Quesenberry KE, Orcutt C (2012) Basic approach to veterinary care. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits and rodents: clinical medicine and surgery, 3rd ed. St. Louis, MO: Elsevier Saunders, pp. 13–26.
2. Lewington JH (2007) Ferret handling, hospitalization and diagnostic techniques. In: Lewington JH, ed. Ferret husbandry, medicine and surgery, 2nd ed. Philadelphia: Elsevier Saunders, pp. 151–165.
3. Zaffarano B (2010) Ferrets: examination and standards of care. J Exot Pet Med 19: 73–81.
4. Ball RS (2006) Issues to consider for preparing ferrets as research subjects in the laboratory. ILAR J 47: 348–357.
5. Jha SK, Coleman T, Frank MG (2006) Sleep and sleep regulation in the ferret (Mustela putorius furo). Behav Brain Res 172: 106–113.
6. Marks GA, Shaffery JP (1996) A preliminary study of sleep in the ferret, Mustela putorius furo: a carnivore with an extremely high proportion of REM sleep. Sleep 19: 83–93.
7. Fisher P (2006) Ferret behavior. In: Bays TB, Lightfoot T, Mayer J, eds. Exotic pet behavior, 1st ed. St. Louis, MO: Elsevier, pp. 163–203.
8. Diaz-Figueroa O, Smith MO (2007) Clinical neurology of ferrets. Vet Clin North Am Exot Anim Pract 10: 759–773, v–vi.
9. Morey AL, Carlile S (1990) Auditory brainstem of the ferret: maturation of the brainstem auditory evoked response. Brain Res Dev Brain Res 52: 279–288.
10. Kelly JB, Kavanagh GL, Dalton JC (1986) Hearing in the ferret (Mustela putorius): thresholds for pure tone detection. Hear Res 24: 269–275.
11. Moore DR, Kowalchuk NE (1988) An anomaly in the auditory brain stem projections of hypopigmented ferrets. Hear Res 35: 275–278.
12. Hoffmann KP, Garipis N, Distler C (2004) Optokinetic deficits in albino ferrets (Mustela putorius furo): a behavioral and electrophysiological study. J Neurosci 24: 4061–4069.
13. Morgan JE, Henderson Z, Thompson ID (1987) Retinal decussation patterns in pigmented and albino ferrets. Neuroscience 20: 519–535.
14. Akerman CJ, Tolhurst DJ, Morgan JE, Baker GE, Thompson ID (2003) Relay of visual information to the lateral geniculate nucleus and the visual cortex in albino ferrets. J Comp Neurol 461: 217–235.
16. Eroshin VV, Reiter AM, Rosenthal K, Fordham M, Latney L, et al. (2011) Oral examination results in rescued ferrets: clinical findings. J Vet Dent 28: 8–15.
17. Rosenblad WD (2013) Dental disease. In: Mayer J, Donnelly TM, eds. Clinical veterinary advisor: birds and exotic pets. St. Louis, MO: Elsevier Saunders, pp. 441–442.
18. Johnson-Delaney CA (2007) Ferret dental disorders: pictorial of common clinical presentations. Exot DVM 9: 40–43.
19. Church RR (2007) The impact of diet on the dentition of the domesticated ferret. Exot DVM 9: 30–39.
20. Johnson-Delaney CA (2005) Ferret cardiopulmonary resuscitation. Seminars in Avian and Exotic Pet Medicine 14: 135–142.
21. Malakoff RL, Laste NJ, Orcutt CJ (2012) Echocardiographic and electrocardiographic findings in client-owned ferrets: 95 cases (1994–2009). J Am Vet Med Assoc 241: 1484–1489.
22. Marini RP, Fox JG (1998) Anesthesia, surgery, and biomethodology. In: Fox JG, ed. Biology and diseases of the ferret, 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins, pp. 449–484.
23. Wagner RA (2009) Ferret cardiology. Vet Clin North Am Exot Anim Pract 12: 115–134, vii.
24. Rawlings CA, Calvert CA (1989) Heartworm disease. In: Ettinger SJ, ed. Textbook of veterinary internal medicine: diseases of the dog and cat. Philadelphia: W.B. Saunders, pp. 1163–1184.
25. Welchman Dde B, Oxenham M, Done SH (1993) Aleutian disease in domestic ferrets: diagnostic findings and survey results. Vet Rec 132: 479–484.
26. Williams BH, Kiupel M, West KH, Raymond JT, Grant CK, et al. (2000) Coronavirus-associated epizootic catarrhal enteritis in ferrets. J Am Vet Med Assoc 217: 526–530.
27. Brown SA (1997) Basic anatomy, physiology, and husbandry. In: Quesenberry KE, Hillyer EV, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 3–13.
28. Appel MJ, Harris WV (1988) Antibody titers in domestic ferret jills and their kits to canine distemper virus vaccine. J Am Vet Med Assoc 193: 332–333.
29. Hoover JP, Baldwin CA, Rupprecht CE (1989) Serologic response of domestic ferrets (Mustela putorius furo) to canine distemper and rabies virus vaccines. J Am Vet Med Assoc 194: 234–238.
30. Ott RL, Svehag SE (1959) Resistance to experimental distemper in ferrets following the use of killed tissue vaccine. West Vet 6: 107.
31. Moore GE, Glickman NW, Ward MP, Engler KS, Lewis HB, et al. (2005) Incidence of and risk factors for adverse events associated with distemper and rabies vaccine administration in ferrets. J Am Vet Med Assoc 226: 909–912.
32. Murray J (1998) Vaccine injection-site sarcoma in a ferret. J Am Vet Med Assoc 213: 955.
33. Munday JS, Stedman NL, Richey LJ (2003) Histology and immunohistochemistry of seven ferret vaccination-site fibrosarcomas. Vet Pathol 40: 288–293.
34. Groelke JW, Dixon LW, Cummings C, Baseman JB (1986) Virus contamination and cytopathology of ferret tracheal epithelial cells in culture caused by vaccination with distemper virus. Lab Anim Sci 36: 527–529.
35. National Association of State Public Health Veterinarians (NASPHV) I (2011) Compendium of animal rabies prevention and control, 2011. MMWR Recomm Rep 60: 1–14.
36. US Department of Health and Human Services PHS, and Centers for Disease (1998) Compendium of animal rabies control. Atlanta, GA: Center for Disease Control.
37. Otto G, Rosenblad WD, Fox JG (1993) Practical venipuncture techniques for the ferret. Lab Anim 27: 26–29.
38. Yao Z, Adler A, Kovar PA (1992) A restraint device for blood sampling and direct blood pressure measurement in conscious ferrets. Contemp Top 31: 19.
40. Brown SA (1993) A practitioner's guide to rabbits and ferrets: Amer Anim Hosp Assoc.
41. Otto CM, Kaufman GM, Crowe DT (1989) Intraosseous infusion of fluids and therapeutics. Compend Small Anim 11: 421–430.
42. Rice LE, Stahl SJ, McLeod CG, Jr. (1992) Pyloric adenocarcinoma in a ferret. J Am Vet Med Assoc 200: 1117–1118.
43. Orcutt CJ (1998) Emergency and critical care of ferrets. Vet Clin North Am Exot Anim Pract 1: 99–126.
44. Andrews PLR, Illman O (1987) The ferret. In: Poole T, ed. UFAW Handbook on the care and management of laboratory animals, 6th ed. Essex: Longman Scientific & Technical, pp. 436–455.
48. Curl JL, Curl JS (1985) Restraint device for serial blood sampling of ferrets. Lab Anim Sci 35: 296–297.
49. Baker GA, Gorham JR (1951) A technique for bleeding ferrets and mink. Cornell Vet 41: 235–236.
50. Florczyk AP, Schurig JE (1981) A technique for chronic jugular catheterization in the ferret. Pharmacol Biochem Behav 14: 255–257.
51. Greener Y, Gilles B (1985) Intravenous infusion in ferrets. Lab Anim 14: 41–44.
52. Carroll RS, Erskine MS, Doherty PC, Lundell LA, Baum MJ (1985) Coital stimuli controlling luteinizing hormone secretion and ovulation in the female ferret. Biol Reprod 32: 925–933.
53. Mesina JE, Sylvina TJ, Hotaling LC, Goad ME, Fox JG (1988) A simple technique for chronic jugular catheterization in ferrets. Lab Anim Sci 38: 89–90.
54. Jackson RK, Kieffer VA, Sauber JJ, King GL (1988) A tethered-restraint system for blood collection from ferrets. Lab Anim Sci 38: 625–628.
55. Rassnick KM, Gould WJ, 3rd, Flanders JA (1995) Use of a vascular access system for administration of chemotherapeutic agents to a ferret with lymphoma. J Am Vet Med Assoc 206: 500–504.
56. Manning DD, Bell JA (1990) Lack of detectable blood groups in domestic ferrets: implications for transfusion. JAVMA 197: 84–86.
57. Quesenberry KE (1997) Basic approach to veterinary care. In: Quesenberry KE, Hillyer EV, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery. Philadelphia: W.B. Saunders, pp. 14–25.
58. Ford RB, Mazzaferro EM (2006) Blood component therapy. In: Kirk KW, Bistner SI, eds. Handbook of veterinary procedures and emergency treatment. St. Louis, MO: Saunders Elsevier, pp. 21–31.
59. Palley LS, Marini RP, Rosenblad WD, Fox JG (1990) A technique for femoral bone marrow collection in the ferret. Lab Anim Sci 40: 654–655.
60. Powell DA, Gonzales C, Gunnels RD (1991) Use of the ferret as a model for pediatric endotracheal intubation training. Lab Anim Sci 41: 86–89.
61. Kircher SS, Murray LE, Juliano ML (2009) Minimizing trauma to the upper airway: a ferret model of neonatal intubation. J Am Assoc Lab Anim Sci 48: 780–784.
62. Davis JA, Greenfield RE, Brewer TG (1993) Benzocaine-induced methemoglobinemia attributed to topical application of the anesthetic in several laboratory animal species. Am J Vet Res 54: 1322–1326.
63. Chimes MJ (1993) A technique for catheterization of ferrets for chronic intratracheal material administration. Lab Anim Sci 43: 346–349.
64. Poste G (1971) The growth and cytopathogenicity of virulent and attenuated strains of canine distemper virus in dog and ferret macrophages. J Comp Pathol 81: 49–54.
65. Whetstone CA, Bunn TO, Gourlay JA (1981) Canine distemper virus titration in ferret peritoneal macrophages. Cornell Vet 71: 144–148.
66. Edelson PJ, Cohen ZA (1976) Purification and cultivation of monocytes and macrophages. In: Bloom BR, David JR, eds. In vitro methods of cell-mediated and tumor immunity. New York: Academic Press.
67. Fox JG, Marini RP (2001) Helicobacter mustelae infection in ferrets: pathogenesis, epizootiology, diagnosis, and treatment. Semin Avian Exot Pet Med 10: 36–44.
68. McColm AA, Bagshaw JA, O'Malley CF (1993) Development of a 14C-urea breath test in ferrets colonised with Helicobacter mustelae: effects of treatment with bismuth, antibiotics, and urease inhibitors. Gut 34: 181–186.
69. Andrutis KA, Fox JG, Schauer DB, Marini RP, Murphy JC, et al. (1995) Inability of an isogenic urease-negative mutant strain of Helicobacter mustelae to colonize the ferret stomach. Infect Immun 63: 3722–3725.
70. Divers SJ (2010) Exotic mammal diagnostic endoscopy and endosurgery. Vet Clin North Am Exot Anim Pract 13: 255–272.
71. Divers SJ (2012) Exotic mammal diagnostic and surgical endoscopy. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits and rodents: clinical medicine and surgery, 3rd ed. St. Louis, MO: Elsevier Saunders., pp. 485–501.
72. Marini RP, Esteves MI, Fox JG (1994) A technique for catheterization of the urinary bladder in the ferret. Lab Anim 28: 155–157.
73. Nolte DM, Carberry CA, Gannon KM, Boren FC (2002) Temporary tube cystostomy as a treatment for urinary obstruction secondary to adrenal disease in four ferrets. J Am Anim Hosp Assoc 38: 527–532.
74. Antinoff N, Giovanella CJ (2012) Musculoskeletal and neurologic diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits and rodents: clinical medicine and surgery, 3rd ed. St. Louis, MO: Elsevier Saunders., pp. 132–140.
75. Platt SR, Dennis PM, McSherry LJ, Chrisman CL, Bennett RA (2004) Composition of cerebrospinal fluid in clinically normal adult ferrets. Am J Vet Res 65: 758–760.
76. Schwarz LA, Solano M, Manning A, Marini RP, Fox JG (2003) The normal upper gastrointestinal examination in the ferret. Vet Radiol Ultrasound 44: 165–172.
77. Srugo I, Chai O, Yaakov D, Sharon L, Shamir MH (2010) Successful medical management of lumbar intervertebral disc prolapse in a ferret. J Small Anim Pract 51: 447–450.
78. Silverman S, Tell LA (2005) Radiology of rodents, rabbits, and ferrets: an atlas of normal anatomy and positioning. St. Louis, MO: Elsevier Saunders.
79. Besso JG, Tidwell AS, Gliatto JM (2000) Retrospective review of the ultrasonographic features of adrenal lesions in 21 ferrets. Vet Radiol Ultrasound 41: 345–352.
80. Kuijten AM, Schoemaker NJ, Voorhout G (2007) Ultrasonographic visualization of the adrenal glands of healthy ferrets and ferrets with hyperadrenocorticism. J Am Anim Hosp Assoc 43: 78–84.
81. Peter AT, Bell JA, Manning DD, Bosu WT (1990) Real-time ultrasonographic determination of pregnancy and gestational age in ferrets. Lab Anim Sci 40: 91–92.
82. Batista-Arteaga M, Suarez-Bonnet A, Santana M, Nino T, Reyes R, et al. (2011) Testicular neoplasms (interstitial and Sertoli cell tumours) in a domestic ferret (Mustela putorius furo). Reprod Domest Anim 46: 177–180.
83. Martorell J, Vrabelova D, Reberte L, Ramis A (2011) Diagnosis of an abdominal splenosis in a case of ambulatory paraparesis of the hind limbs in a ferret (Mustela putorius furo). J Exot Pet Med 20: 227–231.
84. Hauptman K, Jekl V, Knotek Z (2011) Extrahepatic biliary tract obstruction in two ferrets (Mustela putorius furo). J Small Anim Pract 52: 371–375.
85. Hernandez-Guerra AM, Rodilla V, Lopez-Murcia MM (2007) Ocular biometry in the adult anesthetized ferret (Mustela putorius furo). Vet Ophthalmol 10: 50–52.
86. Paul-Murphy J, O'Brien RT, Spaeth A, Sullivan L, Dubielzig RR (1999) Ultrasonography and fine needle aspirate cytology of the mesenteric lymph node in normal domestic ferrets (Mustela putorius furo). Vet Radiol Ultrasound 40: 308–310.
87. Phair KA, Carpenter JW, Schermerhorn T, Ganta CK, DeBey BM (2011) Diabetic ketoacidosis with concurrent pancreatitis, pancreatic beta islet cell tumor, and adrenal disease in an obese ferret (Mustela putorius furo). J Am Assoc Lab Anim Sci 50: 531–535.
88. Dominguez E, Novellas R, Moya A, Espada Y, Martorell J (2011) Abdominal radiographic and ultrasonographic findings in ferrets (Mustela putorius furo) with systemic coronavirus infection. Vet Rec 169: 231.
89. Neal J, Takahashi M, Silva M, Tiao G, Walsh CA, et al. (2007) Insights into the gyrification of developing ferret brain by magnetic resonance imaging. J Anat 210: 66–77.
90. Knutsen AK, Kroenke CD, Chang YV, Taber LA, Bayly PV (2013) Spatial and temporal variations of cortical growth during gyrogenesis in the developing ferret brain. Cereb Cortex 23: 488–498.
91. Tao JD, Barnette AR, Griffith JL, Neil JJ, Inder TE (2012) Histopathologic correlation with diffusion tensor imaging after chronic hypoxia in the immature ferret. Pediatr Res 71: 192–198.
92. Bock AS, Olavarria JF, Leigland LA, Taber EN, Jespersen SN, et al. (2010) Diffusion tensor imaging detects early cerebral cortex abnormalities in neuronal architecture induced by bilateral neonatal enucleation: an experimental model in the ferret. Front Syst Neurosci 4: 149.
93. Pye GW, Bennett RA, Roberts GD, Terrell SP (2000) Thoracic vertebral chordoma in a domestic ferret (Mustela putorius furo). J Zoo Wildl Med 31: 107–111.
94. Herrera VL, Viereck JC, Lopez-Guerra G, Kumai Y, Kobler J, et al. (2009) 11.7 Tesla magnetic resonance microimaging of laryngeal tissue architecture. Laryngoscope 119: 2187–2194.
95. Liu JV, Sharma J (2007) Maps of retinotopy and orientation in ferret measured with BOLD fMRI at 9.4T; San Diego, CA.
96. Liu JV, Sur M, Moore CI, Sharma J (2008) Orientation maps in ferret visual cortex measured by multi-slice; Toronto, Canada.
97. van Zeeland Y, Schoemaker N, Passon-Vastenburg M, Kik M (2009) Vestibular syndrome due to a choroid plexus papilloma in a ferret. J Am Anim Hosp Assoc 45: 97–101.
98. Hanley CS, Wilson GH, Frank P, James DK, Carmichael KP, et al. (2004) T cell lymphoma in the lumbar spine of a domestic ferret (Mustela putorius furo). Vet Rec 155: 329–332.
99. Miwa Y, Uchida K, Nakayama H, Asaki N (2010) Neuroblastoma of the adrenal gland in a ferret. J Vet Med Sci 72: 1229–1232.
100. Veldhuis Kroeze EJ, van Amerongen G, Dijkshoorn ML, Simon JH, de Waal L, et al. (2011) Pulmonary pathology of pandemic influenza A/H1N1 virus (2009)-infected ferrets upon longitudinal evaluation by computed tomography. J Gen Virol 92: 1854–1858.
101. Kroeze EJ, Stittelaar KJ, Teeuwsen VJ, Dijkshoorn ML, van Amerongen G, et al. (2012) Consecutive CT in vivo lung imaging as quantitative parameter of influenza vaccine efficacy in the ferret model. Vaccine 30: 7391–7394.
102. Jonsson CB, Camp JV, Wu A, Zheng H, Kraenzle JL, et al. (2012) Molecular imaging reveals a progressive pulmonary inflammation in lower airways in ferrets infected with 2009 H1N1 pandemic influenza virus. PLoS ONE 7: e40094.
103. Bernas M, Witte C, Pond G (1994) Enhanced lymphatic imaging using Imagent LN in filaria-infected ferrets. Lymphology 27: 265–269.
104. Tanoura T, Bernas M, Darkazanli A, Elam E, Unger E, et al. (1992) MR lymphography with iron oxide compound AMI-227: studies in ferrets with filariasis. AJR Am J Roentgenol 159: 875–881.
105. Witte M, McNeill G, Crandall C, Case T, Witte C, et al. (1988) Whole body lymphangioscintigraphy in ferrets chronically infected with Brugia malayi. Lymphology 21: 251–257.
106. Marini RP, Callahan RJ, Jackson LR, Jyawook S, Esteves MI, et al. (1997) Distribution of technetium 99m-labeled red blood cells during isoflurane anesthesia in ferrets. Am J Vet Res 58: 781–785.