Disorders of the nervous system in the ferret include Creutzfeldt–Jakob disease, idiopathic seizures and ataxia, posterior paresis or paralysis, and eye anomalies. Some of these diseases have been defined with bacterial, viral, and mycotic etiologies; others remain of unknown cause. For example, central nervous system (CNS) signs and lesions of the CNS are noted in ferrets infected with rabies virus, canine distemper virus (CDV), systemic coronavirus infection, and Aleutian disease parvovirus (See Chapter 20). Drug toxicosis can also induce CNS signs.
Creutzfeldt–Jakob Disease
Seven diseases are classified as slow onset spongiform encephalopathies: scrapie in sheep and goats, bovine spongiform encephalopathy in cattle, transmissible mink encephalopathy (TME), chronic wasting disease (CWD) of deer and elk, and kuru, fatal familial insomnia, and Creutzfeldt–Jakob disease (CJD) in humans. Novel infectious particles, termed pathogenic isoform prion proteins (composed largely and perhaps solely of a self-propagating form of prion proteins), are the likely etiological agent of this group of diseases [1]. CJD is transmissible to animals in the laboratory; although there is no evidence of spontaneous transmissible spongiform encephalopathy in ferrets, TME is experimentally infectious to albino ferrets but not sable ferrets (see Chapter 20). Some albino ferrets with CNS clinical signs recovered within 4–5 weeks post infection and remained normal for 28 months post infection [2]. Recent data also demonstrate that ferrets can be experimentally infected with tissues of CWD-infected animals [3]. Ferret-adapted CWD can be orally transmitted to ferrets as well via intracranial and IP inoculation [4]. Ferrets may recover from the clinical disease, although the brain remains infectious to mink.
A tenuous association with ferret contact and development of CJD in humans has been proposed [5,6]. In one case, a 63-year-old man was bitten on the thumb by a feral ferret who had been taken home as a pet. Approximately 2 years later, the man died of histologically proven CJD after a 6-month history of typical CJD symptoms. The clinically normal ferret was killed and submitted for necropsy and histologic examination. No spongiform changes were noted in the brain, although a lymphocytic infiltrate around several capillaries and a leptomeningeal vein were observed. Frozen brain was inoculated into four different species of monkeys and a cat. The surviving animals were asymptomatic, and the two dead animals had no spongiform encephalopathy [6].
In an additional 41 human cases with histologically confirmed CJD, two had kept ferrets. One, a woman who died in 1971, had a husband who kept ferrets from 1943 to 1956 and from 1960 to 1965; her chief contact with the ferrets was washing their food dishes. In the second case, a 67-year-old man who died in 1975 of CJD had used ferrets for rabbiting as a young man and had kept ferrets from 1950 to 1955. A third probable case of CJD was a 61-year-old man who had kept ferrets for many years and allowed a pet ferret to roam freely underneath his shirt. He had had no contact with ferrets for 10 years prior to his death. Their source as a reservoir for infection of CJD, however, is not proven, nor is there further documentation in the literature associating ferret ownership with CJD in humans [6].
Posterior Paresis and Paralysis
Occasionally, ferrets present with posterior paralysis accompanied by incontinence. Posterior paralysis has several causes, including hemivertebrae, vertebral fractures, intervertebral disc diseases [7], hematomyelia associated with prolonged estrus [8,9], idiopathic myofascitis, tumors (see later discussion), and myelitis caused by fungal infections, Mycobacterium spp. [10,11], and rabies [12]. In a study of experimentally induced rabies in ferrets, the most commonly observed initial sign was paralysis [12]. Detailed history, clinical examination, clinical pathology, radiography, and response to supportive therapy confirm the diagnosis. Depending on etiology, the condition may recur, and long-term prognosis is guarded if the spinal cord is severely damaged.
In a recent study of experimental infection with rabies virus of skunk origin, one infected ferret showed initial clinical signs of rabies (hind limb paralysis) 81 days post challenge [13]. The ferret survived 181 days post challenge with paraplegia but was in a normal nutritional state. Despite neuronal changes in the brain and spinal cord, rabies virus antigen could not be detected in neuronal tissues.
It is increasingly recognized that posterior paresis and/or ataxia in ferrets may indicate systemic disease, such as insulinoma, disseminated idiopathic myofasciitis, or abdominal pain. These conditions must be distinguished from primary neurological disease. In a recent report, a 2-year-old ferret presented clinically with abdominal pain and acute onset of ambulatory paraparesis of the hind legs. A cranial mass, diagnosed histologically as splenosis (a condition in which isolated foci of heterotopic splenic disease is present in the abdomen), was removed surgically. The abdominal pain and ambulatory paraparesis resolved after the surgical removal of the mass [14].
Aleutian Disease
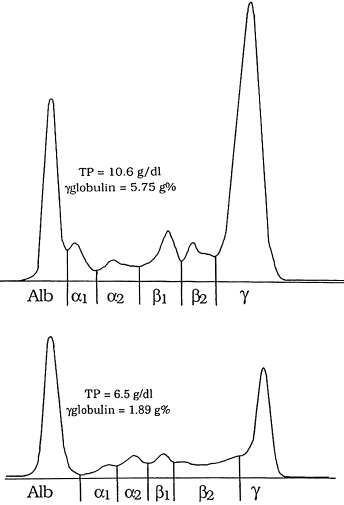
The posterior ataxia, weakness, and paralysis seen in distemper and Aleutian disease must be distinguished from the clinical entities listed earlier. Because lymphocytic-plasmacytic infiltration of multiple organ systems is observed in Aleutian disease virus (ADV) infection, it is reasonable to conclude that a CNS form might exist, particularly if this is the primary organ system affected. An increasing number of reports incriminate infection with ADV and onset of CNS signs. In one well-documented case, a 2-year-old ferret had a history of bilateral hind limb paresis [15]. Physical examination revealed predominantly left-sided hind limb paresis, with strength preserved. There was bilaterally symmetrical atrophy of the quadriceps, semimembranous, and semitendinous muscles. The ferret had increased patellar reflexes. It had been vaccinated against canine distemper with modified-live virus distemper vaccine 6–8 weeks prior to admission; however, other vaccination history was unknown [15]. Clinicopathologic abnormalities included hypoalbuminemia (2.4 g/dL; reference range, 3.6–4.6 g/dL) and hyperglobulinemia (4.1 g/dL; reference range, 1.7–2.9 g/dL). Protein electrophoresis of serum revealed pronounced hypergammaglobulinemia expressed as 29% of the total protein (Fig. 19.1). The counterimmunoelectrophoresis (CIE) and immunofluorescent antibody test for antibody to ADV were positive.
Fig. 19.1. Serum protein electrophoretograms from two ferrets with parvovirus-associated syndromes (Aleutian disease). Top: Ferret 1, notice the pronounced hypergammaglobulinemia; the γ-globulin fraction is equivalent to 54% of the total protein. Bottom: Ferret 2, the γ-globulin fraction is equivalent to 29% of the total protein. Hypergammaglobulinemia is the hallmark of Aleutian disease virus infection. TP, total protein; Alb, albumin. (Palley LS, Corning BF, Fox JG, Murphy JC, Gould DH. (1992) Parvovirus-associated syndrome (Aleutian disease) in two ferrrets. J Am Vet Med Assoc 201: 100–106.)
Radiography of the thorax, abdomen, and spinal column revealed no abnormal findings. One week after admission, the ferret developed an intermittent head tremor. The paresis progressed, resulting in diminished use of both hind limbs. The ferret also developed diarrhea, with fecal and urinary incontinence. Results of repeat fecal analyses for parasite ova and protozoa as well as bacterial cultures of rectal swab specimens were negative. Sulfamethoxazole and trimethoprim suspension (Sulfatrim Pediatric Suspension, Schein Pharmaceutical Inc., Port Washington, NY) (30 mg/kg of body weight, q 24 h) and bismuth subsalicylate (Pepto-Bismol, Proctor & Gamble, Cincinnati, OH) (2 mg/kg, q 8 h) were administered orally for a 24-hour period. The diarrhea resolved 1 day later. A cerebrospinal fluid aspiration was performed with the ferret under general anesthesia, and the ferret was then euthanatized. Bacterial culture of the fluid yielded no growth and a direct immunofluorescent antibody test for rabies virus on brain tissue also was negative. A canine distemper serum neutralization test performed on serum was positive at a 1 : 65 dilution.
Histologic evaluation revealed infiltrations of lymphocytes and plasma cells in duodenum, stomach, salivary gland, liver, thyroid, lungs, and right atrium. Nervous system tissue examined histologically included brain, spinal cord, spinal nerve roots, and dorsal root ganglia. Sections of spinal cord were stained with H&E, luxol-fast blue-cresyl echt violet, or immunostained for glial fibrillary acidic protein (GFAP for astrocytes) by use of mouse anti-porcine GFAP antibody, and labeled with a biotin-streptavidin system.
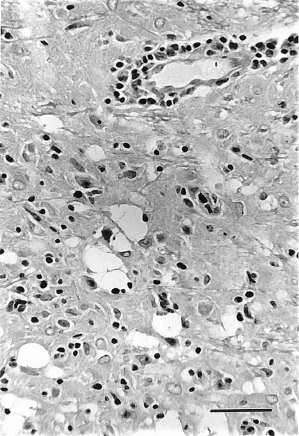
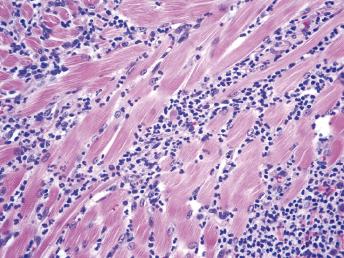
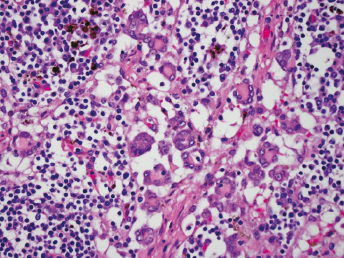
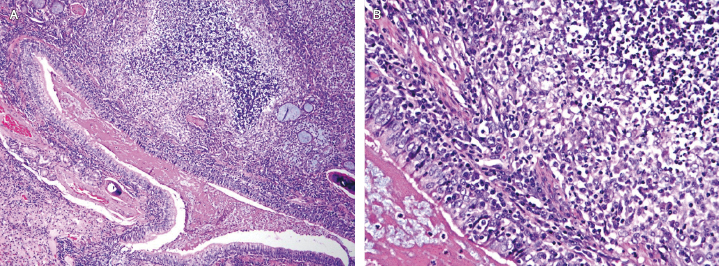
Lesions in the CNS consisted chiefly of disseminated nonsuppurative encephalomyelitis. The character of the cellular infiltrate was largely lymphoplasmacytic, although in some areas, macrophages were identified. Perivascular accumulations of these mononuclear cells were prominent. Parenchymal infiltration, frequently with microgliosis, was also evident. Astrocyte hypertrophy was common and confirmed by positive GFAP staining. Choroid plexus and cranial and spinal meninges were infiltrated with inflammatory cells. In a submeningeal area of inflammation in the brain stem, parenchymal vacuolation suggestive of demyelination was found (Fig. 19.2). In the spinal cord, the reaction was similar, but the parenchymal vacuolation was absent. The spinal cord gray matter was more heavily involved than the white matter and astrocytic hypertrophy was a conspicuous feature (Fig. 19.3) [15].
Fig. 19.2. Photomicrograph of a submeningeal brainstem site of nonsuppurative inflammation and parenchymal vacuolation. Notice the infiltration and accumulation of mononuclear cells in perivascular spaces and in the neuropil. H&E stain; Bar = 50 μm. (Palley LS, Corning BF, Fox JG, Murphy JC, Gould DH. (1992) Parvovirus-associated syndrome (Aleutian disease) in two ferrrets. J Am Vet Med Assoc 201: 100–106.)Fig. 19.3. Photomicrograph of spinal cord gray matter—white matter junction. Notice the heavy perivascular mononuclear cell infiltration. The arrow indicates a hypertrophic astrocyte. H&E stain, Bar = 30 μm. (Palley LS, Corning BF, Fox JG, Murphy JC, Gould DH. (1992) Parvovirus-associated syndrome (Aleutian disease) in two ferrrets. J Am Vet Med Assoc 201: 100–106.)
In New Zealand, clinical signs of progressive caudal paralysis, muscle wasting, urinary incontinence, and tremors were documented in ADV antibody-positive ferrets. Additionally, histologic lesions included mild to severe lymphocytic meningoencephalomyelitis, foci of demyelination in the white matter, and infiltration of meninges with lymphocytes and plasma cells [16].
In another study, 5 ferrets (ages 8 months to 3 years) from a colony of 25 presented with neurological symptoms [17,18]. Twelve of twenty ferrets tested in this colony had ADV antibody according to the CIE test. Interestingly, three affected females consisted of a jill and two of her female offspring. The CNS signs developed over a period of 6 months and consisted of posterior ataxia, incoordination, and tremors; otherwise, when handled, they seemed bright and alert. One ferret had persistent tremors affecting the entire body, became acutely ill, and was unable to eat or drink. Two of these animals were euthanatized, and a histopathological analysis was performed. A nonsuppurative meningitis and perivascular cuffing with lymphocytes and occasional plasma cells were present in the brain and spinal cord of one ferret. The second ferret had diffuse astrocytes and plasma cell infiltration of the gray and white matter of the brain and spinal cord [17]. Posterior ataxia and paresis have also been attributed to ADV in 12 domestic ferrets, aged 8 months to 7 years in southern England [19]. Signs varied from posterior ataxia or weakness to intermittent posterior paresis with recovery or progression to paraplegia. Other ferrets presented with acute onset paraplegia, and in one ferret, the paraplegia progressed to quadriplegia over a 3-day period.
Ferret Systemic Coronavirus Infection
Ferret systemic coronavirus disease (FSCD) was first reported in 2002. As the name implies, it is caused by a coronavirus, and microscopic lesions in ferrets with the disease are identical to the dry form of feline infectious peritonitis [20]. The coronavirus of FSCD is related to the coronavirus causing ferret epizootic catarrhal enteritis. Unfortunately, FSCD is chronic, progressive, and fatal. Diarrhea may be the initial clinical sign, but weight loss, lethargy, and hind leg weakness are commonly observed [21]. Nonregenerative anemia is reported as well as neutrophilia, thrombocytopenia, and lymphopenia. Hypergammaglobulinemia is almost always present [22]. There is loss of lumbar musculature, palpable masses in the abdomen, and splenomegaly. Multiple angiocentric granulomas are present in visceral organs and mesentery. Importantly, lesions are also observed in the brain and spinal cord, explaining clinical signs of posterior paralysis and seizures. Diagnosis is accomplished by immunohistochemistry demonstrating coronaviral antigen in the granulomatous lesions (see Chapter 20) [23].
Canine Distemper
The histopathologic finding of nonsuppurative encephalomyelitis can be consistent with findings in canine distemper. Distemper myelitis/encephalitis develops in dogs as a natural acute myelitis/encephalitis with or without systemic disease, as postvaccinal encephalitis, and as chronic encephalitis in old dogs [24,25]. Postvaccinal distemper is reported to be potentiated in gnotobiotic dogs by infection with parvovirus [26] and treatment with immunosuppressive drugs [27]. In ferrets, natural CDV infection most often begins as a catarrhal phase followed by a fatal neurotrophic form [28]. A postvaccinal (chicken embryo extract origin) form has been documented in the domestic ferret, and it has been reported in the black-footed ferret vaccinated with chicken embryo-tissue culture-origin CDV vaccine [29] and domestic ferrets vaccinated with canine cell products [30]. The temporal sequence of vaccination and clinical signs may be clues that indicate a possible postvaccinal disease. Viral inclusion bodies are typically found in CDV-infected ferrets (see Chapter 20).
Pseudo-Negri Bodies
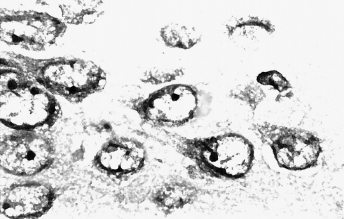
We have observed intracytoplasmic inclusions in hippocampal neurons of a ferret brain which was negative for rabies virus antigen by immunohistochemical examination (Fig. 19.4). The inclusions were approximately 6–10 μm in length, acidophilic, homogeneous, and plastic, conforming to the nuclear margin. Similar intracytoplasmic neuronal inclusions have been previously reported in the hippocampus of dogs, cats, and skunks [31]. The inclusions are nonspecific and are important because they must be distinguished from the intracytoplasmic neuronal inclusion bodies associated with rabies virus infection (i.e., Negri bodies).
Fig. 19.4. Perinuclear inclusion in the hippocampus of a ferret, which was immunohistochemically negative for rabies. The inclusions are acidophilic and conform to the nuclear margins. Giemsa.
Idiopathic Seizures and Ataxia
Occasionally, ferrets have seizures of undetermined etiology. A neurologic syndrome of suspected viral etiology has been described in ferrets. Signs included pyrexia (41.7–43.4°C), tremor, and ataxia. The animals recovered after supportive therapy [32].
Seizures and ataxia were reported in a 3-year-old male neutered ferret. The animal was diagnosed as having bilateral polycystic kidneys. The CNS signs may have been caused by uremic encephalopathy. Unfortunately, the brain was unavailable for examination [33]. Differential diagnoses would include rabies, listeriosis, distemper, fungal encephalitis, Aleutian disease, systemic coronavirus, toxoplasmosis, insulinoma, and hypoadrenocorticism.
Cryptococcal Meningitis
Cryptococcosis is increasingly diagnosed in pet ferrets whose owners reside in different parts of the world. The disease in ferrets can present clinically with CNS signs compatible with subacute or chronic meningoencephalitis. Ferrets infected with cryptococcal organisms can also present with respiratory, cardiac, and abdominal symptoms. Skin involvement and acute blindness have also been noted in infected ferrets (See Chapter 23).
Diseases of the Eye
Cataracts
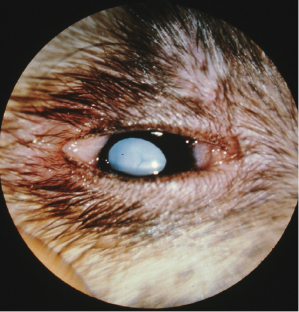
There are a number of causes of cataracts in humans and domestic animals, including metabolic, hereditary, congenital, infectious, and traumatic etiologies. Juvenile cataracts have been reported in ferrets [34]. They can be congenital or hereditary in origin. Another colony of ferrets used for biomedical research in England also had a low incidence of cataracts. Five cases of unilateral cataracts were reported, which caused blindness in the affected eye and, according to the authors, interfered with the animals' ability to eat from a bowl. Another ferret was diagnosed as having bilateral cataracts. Possible etiologies were not discussed [35]. A case of bilateral cataracts in a pet ferret was also reported (Fig. 19.5) [36]. The cataracts appeared to involve both the nucleus and cortex of the lens. Repeated urinalysis and clinical examination indicated that the animal was not diabetic.
When examined by slit lamp biomicroscopy, 34 of 73 (47%) of ferrets, aged 11–12 months, had lens opacities [37]. Lesions in the lens ranged from fine, multifocal, punctate opacification to mature cataracts. Eighteen weeks after the initial examination, 36 of the remaining 45 animals from the initial survey had lenticular opacities. When examined at 17–18 months of age, the opacifications often extended throughout the posterior lens cortex, rather than being confined to the subcapsular area. In another ferret population of different genetic background, 3 of 47, 6-month-old juveniles were classified as normal, and 16 had some form of lens opacification. Thus, many ferrets have slowly progressive formation of cataracts. Lens opacification appeared to begin as white, multifocal, punctate opacities diffusely scattered in the posterior, and subsequently anterior, cortical/subcortical area [37]. The lesions present in the cortical and subcapsular area indicate that the cataract formation may be secondary to lens epithelial cell growth and maturation abnormalities. Cataracts affecting the nucleus of the lens in young animals usually reflect a prenatal insult in early lens development; others suggest that they are congenital in origin. Animals with luxation of normal or cataractous lenses have also been recorded as having retinal degeneration due to luxated cataracts [38,39].
Although genetics may well play a role in the high frequency of cataracts in this population, diet may also influence expression of this disease. High-fat diet and production of reactive oxygen radicals with inadequate antioxidants in the diet may have created lipid perioxidation cataracts. Dietary deficiency in vitamin E or relative excess of polyunsaturated fats have been described in ferrets, and dietary deficiency in vitamin E has been associated with cataracts in rats [40]. Cataracts due to arginine deficiency have also been recorded in dogs and wolves [41,42]. Interestingly, the group of ferrets with a high incidence of cataracts was fed a mink diet which may have had nutritional components insufficient for optimum lens development, growth, and maturation [37]. Diabetes mellitus has been infrequently diagnosed in ferrets [43,44]. Cataract formation can occur in diabetic animals; this has been reported in ferrets with the disease. Diseases causing secondary cataracts, in addition to diabetes mellitus, are retinal detachment, or degeneration, anterior uveitis, and lens luxation. The rate of cataract progression is dependent on the age of the ferret and the cause and location of the cataract [45].
Microphthalmia
Microphthalmia has also been noted in ferrets [37]. Both eyes were smaller than normal and had disproportionally shallow anterior chambers that obscured the fundus. Some of the lenses were hypermature with snowflake crystalline appearance and were undergoing liquefaction. In microphthalmic ferrets, the iris was thicker than normal with irregular sponge-like texture to its surface [37].
Lymphoma
Lymphoma of the eye has been recorded in two ferrets. Both were diagnosed clinically because of protusion of the eye [46]. This clinical sign preceded generalized lymphadenopathy and other signs attributable to lymphoma.
Cryptococcal chorioretinitis
A ferret with bilateral mandibular lymphadenopathy presented with acute onset of blindness [47]. The cause of the blindness was bilateral exudative chorioretinitis. Biopsy of the lymph node revealed the presence of cryptococcal fungi. Six months after initial presentation and treatments with fluconazole, the ferret developed CNS signs and was euthanized. Histopathological exam of the left eye indicated the presence of cryptococci in the detached retina.
Musculoskeletal System
Lymphoma, Myeloma, and Leukemia of the Bone
Lymphosarcoma may appear clinically as lymphadenopathy, weakness, lethargy, posterior ataxia, anorexia, weight loss, and splenomegaly. Occasionally, lymphoma metastasize to vertebra where the invading tumor can cause osteolytic lesions. Other neoplasms such as multiple myeloma should also be considered as part of the differential diagnosis of posterior paresis. There is a single case report of spontaneous plasma cell myeloma involving a lumbar vertebra in a ferret with paraparesis [48]. A three-year old, neutered male ferret had a slowly progressive paraparesis for 8 months, rear limb paralysis with no patellar reflex, terminally, no central recognition of pain [48]. At necropsy, a 3 × 3 × 4-cm, lobulated, firm, light tan mass occupied the body of the sixth lumbar vertebra (L6). The mass invaded the bone marrow, adjacent bone, muscles, and vertebral canal. L6 was fractured, and the spinal cord was softened.
Microscopic examination of tissue around L6 revealed a poorly demarcated and unencapsulated solid mass of neoplastic plasma cells. Neoplastic cells infiltrated bone marrow, muscles, vertebral canal, and dura mater. Clusters of neoplastic cells were found in several venules. Adjacent bone was necrotic and in some areas was replaced by fibrous connective tissue. The distal spinal cord and cauda equina had diffuse axonal degeneration and dilatation of myelin sheaths with some perineural fibrous proliferation.
A cystic bone lesion in the proximal humerus was diagnosed radiographically in a 1-year-old ferret with nonsupporting lameness of the foreleg. Approximately 2 weeks later, the animal developed acute paraplegia and was euthanatized. Acute myelogenous leukemia was diagnosed in both the humerus and thoracic vertebra. We have also observed lameness or paresis associated with lymphoma of the bone observed radiologically in two cases. One had paresis due to a lumbar mass. The second had unilateral lameness with a lytic mass noted in the tibia. In another reported case, lameness due to extensive lysis of the femur was diagnosed. Amputation of the femur and histologic diagnosis lymphoma was made [49].
Disseminated Idiopathic Myofasciitis
Disseminated idiopathic myofasciitis (DIM) is a recently reported disease in the ferret. First described in 2007, a series of 17 pet ferrets were diagnosed, over an 11-year period (1995–2005), as being affected with pyogranulomatous inflammatory involvement of cardiac and skeletal muscles [50]. The disease affects young adults (average age 10 months, with a range of 11 weeks to 4 years) and does not appear to have a sex predilection. All of the ferrets diagnosed with DIM in this report were vaccinated with at least one dose of distemper vaccine (Fervac-D) [50]. This particular vaccine is no longer produced. Other ferrets with DIM have been vaccinated with two other distemper vaccines, Purevax (Merial, Athens, GA) and Galaxy-D (Schering Plough, Omaha, NE) [51].
Clinical Signs
In ferrets, the syndrome presents with a rapid onset and clinical signs of fever, lethargy, depression, inappetence, recumbency, apparent pain in the rear legs when ambulatory, ataxia, and posterior paresis are present. Bruxism and difficulty in swallowing as well as tachycardia, tachypnea, and heart murmurs were noted in some affected ferrets. Mild to moderate neutrophilia was accompanied by mild to moderate anemia, usually nonregenerative. Serum alanine aminotransferase was elevated in some ferrets. Interestingly, there was an absence of an elevation of creatine kinase or aspartate aminotransferase, both considered serum markers of muscle damage. This may be the case, because with DIM, despite diffuse infiltration of inflammatory cells in the affected muscles and progressive atrophy, there is comparatively minimal necrosis of muscle bundles [50].
Treatment
Despite various treatments, including multiple antibiotics, nonsteroidal anti-inflammatory drugs, glucocorticoids, cyclophosphamide, interferon, and analgesics, all ferrets either succumbed to the disease or were euthanized [50]. However, a more recent report on this disease describes a therapeutic regimen consisting of a combination of cyclophosphamide, prednisolone, and chloramphenicol [51]. Several ferrets receiving this regimen have responded clinically [51] (Table 19.1). Two ferrets treated with the combination therapy improved clinically and are alive 3.5 years after the onset of DIM [51]. Cyclophosphamide, used as a chemotherapeutic agent, has immunosuppressive effects, causes reduction in leukocytes, and decreases antibody production. Success with cyclophosphamide treatment indirectly infers that DIM is an acquired immune-mediated disease. In humans, idiopathic inflammatory myopathies may be a manifestation of systemic autoimmune diseases [52].
aPrednisolone can be made up as a “bitter-free” suspension that is more palatable than some human commercial formulations.
bSubcutaneous fluids should be administered in conjunction with administration of cyclophosphamide to help reduce potential occurrence of hemorrhagic cystitis. Cyclophosphamide can be given via a subcutaneous injection. Oral cyclophosphamide is not palatable to ferrets, and partial tablets should not be given as the drug is not even distributed throughout the tablet. A complete blood count should be done before each cyclophosphamide treatment.
cChloramphenicol palmitate oral suspension can be made at a compounding pharmacy.
Pathology
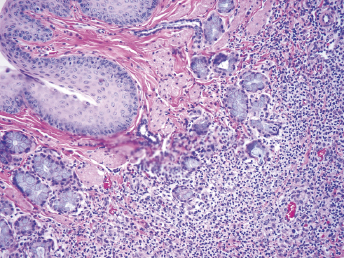
The majority of ferrets were necropsied by practitioners, and gross lesions were seldom noted, with the exception of white mottling and dilation of the esophagus, and white streaks on the heart, diaphragm, and intercostal muscles in some of the ferrets [50]. Four of the ferrets were necropsied by a pathologist who noted moderate to severe atrophy of the limb muscles as well as atrophy of lumbar muscles (Fig. 19.6). Each of the four ferrets had red-white mottling of the entire esophagus and noticeable atrophy of the tongue (Fig. 19.7). Splenomegaly was seen in all four ferrets, and the diaphragm was thin and semitransparent [50]. Histologically, moderate to severe, suppurative to pyogranulomatous inflammation was observed in skeletal muscle of the limbs and lumbar region, head, sternum, and abdominal wall (Fig. 19.8). The muscle of the esophagus also had noticeable inflammation of the muscle and sometimes extended into the submucosa and serosal tunics (Fig. 19.9) [50]. The inflammation primarily affected the perimysium and the endomysium with extension into the fascia and adipose tissue. Myeloid hyperplasia of the spleen and bone marrow was also noted.
Fig. 19.6. Hind limb, ferret. Note severe generalized atrophy of musculature of the hind limb of ferret with DIM (left), compared with an age-matched ferret that died of unrelated disease (right).Fig. 19.7. Esophagus. Note full length mottling of the esophagus, shrinkage of the tongue and lingual hyperkeratosis of ferret with DIM. (Reprinted with permission from Garner MM et al. (2007) Myofasciitis in the domestic ferret. Vet Pathol 44: 25–38.)Fig. 19.8. Skeletal muscle in ferrets with DIM. Extensive inflammation into the endomysium. (Courtesy of Matti Kiupel.)Fig. 19.9. Esophagus of ferret with DIM. Severe neutrophilic inflammation of esophageal submucosa and effacement of muscular tunic. H&E stain. (Courtesy of Matti Kiupel.)
Diagnosis
Muscle biopsy of skeletal muscle reveals a suppurative to pyogranulomatous inflammation. Unfortunately, an infectious etiology has not yet been identified. The disease in ferrets has similar features to juvenile onset polyarthritis in Akita dogs, suggesting a genetic predisposition to DIM in ferrets [53]. It is important to note that a disease, histologically indistinguishable in lesion presentation and tissue distribution in ferrets with DIM, was an inadvertent consequence of administering an experimental castration vaccine that contained an aluminum adjuvant [50,54].
Cardiovascular System
Mycocarditis
Multifocal necrosis of the myocardium has been recorded in New Zealand ferrets infected with a Toxoplasma-like organism [55]. Fibroid necrosis, mononuclear infiltration, and thrombosis of cardiac arterioles have also been noted in ferrets with Aleutian disease [19,56]. We have observed diffuse myocardial necrosis in a ferret with prolonged pyrexia of undetermined etiology (J.G. Fox, unpublished observations).
Neoplasms
Various surveys conducted on prevalence and type of tumors in ferrets have failed to record primary tumors of the heart, except those derived from vascular endothelium, for example, hemangioma and hemangiosarcoma [57]. Lymphosarcomas metastasize to the heart, making this tumor the most commonly reported cardiac tumor (see Chapter 24). Lymphosarcomas involving the mediastinum also occur commonly, particularly in young ferrets [58]. Clinically, onset is often acute and marked by dyspnea, collapse, hypothermia, and often death. Others may present with anorexia, weight loss, and lethargy. Generalized weakness may be clinically evident by posterior paresis (see Chapter 24). Radiographically, there is pleural effusion, and a radio-opaque mass is evident in the mediastinum. Ultrasonography indicates a mass of mixed echogenicity [59].
Heartworm Disease
In areas where heartworm (Dirofilaria immitis) is endemic, ferrets should be considered at risk of developing the disease, particularly ferrets that spend time outdoors (see Chapter 22). Ferrets with naturally occurring dirofilariasis living in these areas have been reported [60]. Animals present with lethargy, dyspnea, coughing, ascites, and anemia [61,62]. Also, a ferret with dirofilariasis died during a long-term study evaluating serological responses of canine distemper vaccination [63]. Radiographically, ferrets with heartworm have cardiac enlargement and pleural effusion [60]. Although echocardiographs of heartworm infected ferrets have not been reported, enlargement of the right atria and ventricle as well as pulmonary artery is expected (see Chapter 18).
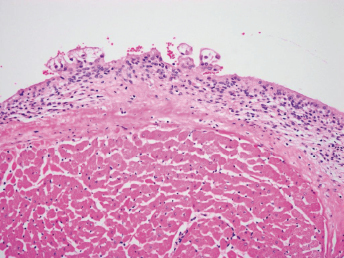
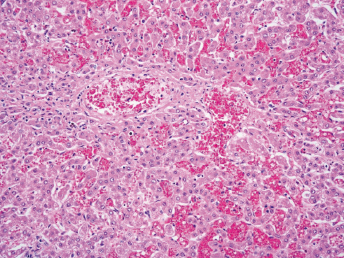
The histopathologic lesions of dirofilariasis in the ferret resemble those described for the dog [64]. Myointimal proliferation and fibrosis develop in the endocardium of the right ventricle and in the intima of the main pulmonary artery and its larger branches within the lung. The endocardium becomes thickened within occasional villous projections and mild inflammation (Fig. 19.10). Intimal thickening with the pulmonary arteries can be severe, leading to stenosis of the vessels with subsequent increase in pulmonary resistance. The occlusive effects of the myointimal proliferation lead to right heart congestive failure. Chronic passive congestion develops in the liver, characterized by central vein congestion and fibrosis accompanied by atrophy and necrosis of the centrilobular hepatic plates (Fig. 19.11). Other lesions include the accumulation of multinucleate giant cells within the mediastinal lymph nodes (Fig. 19.12), hemosiderin retention within mononuclear phagocytes, and retention of hemoglobin-like pigment in the renal tubular epithelium.
Fig. 19.10. Fibrosis of the right ventricular endocardium associated with dirofilariasis, accompanied by mild mononuclear inflammatory cell infiltration and formation of villous projections. H&E.Fig. 19.11. Chronic passive congestion of the liver due to right heart failure induced by dirofilariasis. There is congestion and fibrosis of the hepatic central vein with concurrent congestion of the centrilobular hepatic sinusoids and atrophy of the hepatic plates. H&E.Fig. 19.12. Multinucleate giant cells in the medullary sinuses of a mediastinal lymph node from a ferret with dirofilariasis. H&E.
Cardiomyopathy
Cardiomyopathies are usually defined as myocardial diseases of unknown etiology, although secondary cardiomyopathies are often associated with infectious agents, particularly viruses [65,66]. Primary cardiomyopathies, those with undefined etiologies, are further classified according to their functional, anatomic, and pathophysiologic characteristics. Dilatative cardiomyopathy is increasingly recognized as a cause of congestive heart failure in the ferret, as well as in other species [10,67,68] (see Chapter 18).
Clinical Signs and Diagnosis
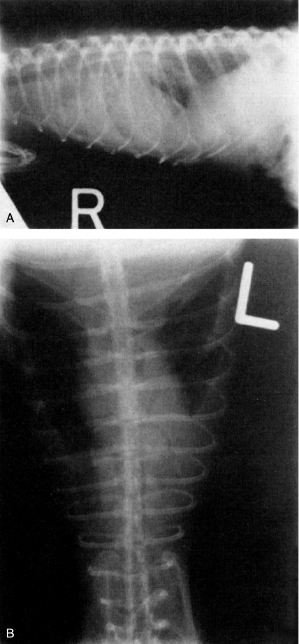
Ferrets presenting with cardiomyopathy have weight loss and lethargy of several months duration, despite adequate dietary intake. The animal is often dyspneic, and fatigues easily after exercising [67,68]. Radiographically, an enlarged globoid cardiac silhouette, signs of pleural effusion, pulmonary congestion, and edema are observed (Fig. 19.13). Importantly, this condition can be clinically silent but present as a complication during adrenalectomies being performed in ferrets with hyperadrenocorticism [69,70]. Physical examination findings often include cyanosis, prolonged capillary filling, jugular venous distension, and hypothermia [59]. Thoracic auscultation most often reveals tachycardia and a holosystolic murmur [59]. Gallop rhythms are sometimes noted and can be indicative of severe disease. Hepatomegaly and splenomegaly are usually present on abdominal palpation. Echocardiographic findings commonly include dilatation of all four cardiac chambers, decrease in cardiac output, fractional shortening, and contractility. Electrocardiograms can indicate either a tachycardia or bradycardia (although sinus tachycardia is more common), premature complexes, tall and wide QRS complexes and ST segment depression [65,66,71]. If third-degree atrioventricular block is present, cardiac disease is pronounced and difficult to treat.
Fig. 19.13. Lateral (A) and ventrodorsal (B) thoracic radiographs reveal severe bilateral pleural effusion and cardiomegaly. (Lipman N, Fox, JG. (1987) Clinical, functional, and pathologic changes associated with a case of dilatative cardiomyopathy in a ferret. Lab Anim Sci 37: 210.)
Treatment
Furosemide (2.5–4 mg/kg IM twice daily) and digoxin elixir (0.01 mg/kg orally twice daily) are used in ferrets with cardiomyopathy to decrease pulmonary edema and to improve cardiac function. Digoxin is increased gradually until a serum level of 1.3 mg/mL is reached 10 days after initiation of treatment [68]. Clinical improvement may or may not be observed. Treatment failure in other species with severe congestive heart failure is common; in our experience with ferrets, this idiopathic primary cardiomyopathy treatment is palliative with a fairly rapid clinical course, and prognosis is guarded to poor. Differential diagnosis includes congestive heart failure caused by D. immitis (see Chapter 18).
Pathology
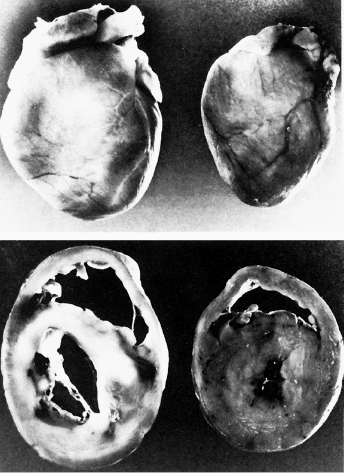
Gross observation reveals dilated ventricles and atria, with thin interventricular septum and ventricular free walls (Fig. 19.14). Hydrothorax is a common finding, with fluid volume often in excess of 100 mL (a clear serosanguinous fluid). On cytologic examination, the fluid contains few inflammatory and red blood cells. The liver is firm, dark red, and slightly enlarged. Ascites may or may not be present. Histologically, multifocal myocardial degeneration, necrosis, and fibrosis are common findings [72]. These lesions are seen in atria, ventricles, and the interventricular septum. Muscle fibers have loss of striation and staining intensity. Mild to moderate infiltration of macrophages, lymphocytes, plasma cells, and occasional polymorphonuclear cells are seen in areas of myocardial necrosis and degeneration.
Fig. 19.14. (A and B) Heart from a ferret with cardiomyopathy on the left and from a ferret of the same sex and similar age and body weight on the right. These are formalin-fixed specimens. The intact heart on the left is larger and has a rounded profile. In cross section, both ventricles are dilated, and the ventricular free walls and interventricular septum are thin in the heart on the left as compared with the heart on the right. The pale areas in the myocardium of the heart on the left correspond to areas of fibrosis found on histologic examination. (Lipman N, Fox JG (1987) Clinical, functional, and pathologic changes associated with a case of dilatative cardiomyopathy in a ferret. Lab Anim Sci 37: 210.)
The possible role of taurine deficiency in dilative cardiomyopathy in ferrets has been raised. Cats may develop taurine deficiency-associated dilated cardiomyopathy, as well as blindness, and are one of the few carnivores that require taurine in their diet. One author has suggested that since cat diets have been fortified with taurine, fewer cases of cardiomyopathy in ferrets have been observed [73]. Cysteine is the precursor of taurine; compared with the rat and dog, the cat cannot decarboxylate appreciable amounts of cysteine sulfinic acid in the liver because of low concentrations of cysteine sulfinate acid decarboxylase [74]. The best defined metabolic role of taurine in mammals is in bile acid conjugation; along with glycine, this amino acid is used to conjugate deoxycholate to form bile acids. These two amino acids also are utilized for conjugating xenobiotics. Though many mammals, including ferrets, preferentially use taurine for bile acid and xenobiotic conjugation, glycine can be utilized for conjugation when taurine is in low supply. Cats are unable to conjugate significant amounts of bile with glycine and must use taurine exclusively (even under dietary taurine restriction) for bile conjugation; thus, under these conditions, cats constantly lose taurine in bile and develop low plasma taurine concentrations despite reabsorption of free taurine and taurocholic acid in their intestines and upregulation of renal conservation of taurine [74]. It is under these conditions that cats develop taurine deficiency-induced dilated cardiomyopathy. This is not the case, however, with ferrets; these animals can utilize glycine for conjugation, and therefore, depletion of the taurine pool is unlikely [75]. We are unaware, however, of definitive studies where ferrets have been placed on taurine-free diets to ascertain if they can maintain adequate plasma taurine levels. Nevertheless, if taurine deficiency is suspected in ferrets with cardiomyopathy, plasma levels of taurine can be determined and compared with control plasma levels. Heparin is the anticoagulant of choice for collection and measurement of plasma taurine.
Small, yellow to white, irregular, firm foci can be observed at necropsy in the lungs of fur-bearing animals and rodents [76] (Fig. 19.15). Histologically, these are subpleural emphysematous lesions with macrophages occluding alveoli [77]. Subpleural histiocytosis, described grossly as pale gray, subpleural plaques, was also observed in ferrets administered estrogen and in control ferrets [8]. We too have observed this condition in ferrets, and histologically have seen cholesterol-like clefts in portions of the involved lung (Fig. 19.16). This can be accompanied by interstitial fibrosis, mononuclear cell infiltration, and foci of type II alveolar cell proliferation. The etiology of the condition is unknown; it does not appear to have any clinical significance. The condition must be differentiated from lesions induced by Mycobacterium spp. and Mycoplasma spp.
Fig. 19.15. Multiple whitish-yellow plaques (arrow) extending above the surface of the lobe of a ferret lung.Fig. 19.16. Pulmonary cholesterol granuloma. (A) A low-magnification image of lung showing multiple foci of subpleural and intraparenchymal mixed inflammatory aggregates with prominent foamy cells expanding and filling many alveoli. (B) A higher magnification image of an intraparenchymal focus showing increased cellularity, alveolar septal effacement, and filling up of alveolar spaces by foamy macrophages, lymphocytes, and a few needle-shaped, clear acicular cholesterol clefts, some of which are partially engulfed by multinucleated giant cells. (C) A higher magnification image of the intraparenchymal focus.
Osseous Metaplasia
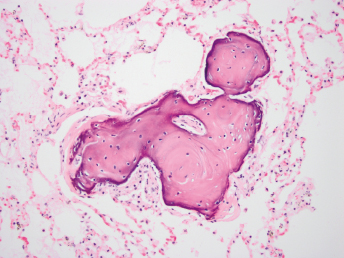
Occasionally, osseous metaplasia is noted histologically in the lungs of ferrets (Fig. 19.17). The genesis of the lesion is unknown and is clinically inapparent. Similar findings have been reported in the lungs of mink, as well as other species of animals [78].
Fig. 19.17. Adult female ferret. Ectopic bone noted in lung. H&E stain. 80×.
Aspiration Pneumonia
Aspiration pneumonia can be commonly encountered in ferrets, particularly those on prolonged oral liquid medication or ferrets suffering from megaesophagus [79]. If the pulmonic lesions are severe, they can be seen radiographically as involvement of the small airways. Atelectasis may also occur. Inhalation pneumonia usually affects the caudal portion of the left cranial lobe and the right middle lobe; alternatively, the dependent parts of the caudal lobes are involved [80]. All ferrets suffering from megaesophagus have bronchial pneumonia of various degrees of severity and chronicity. Histologically, there is a mixture of inflammatory infiltrates, fibrin accumulation, and evidence of necrosis, fibrosis, abscessation, and pleuritis [79]. Particulate foreign matter can also be observed in the bronchioles and alveoli (Fig. 19.18).
Fig. 19.18. (A) Aspiration pneumonia 100×: Lung of a ferret with systemic coronavirus infection centered around a bronchus filled with proteinaceous material and necrotic cellular debris, bronchitis, and peribronchitis with distinct degenerate/necrotic cores surrounded by mixed inflammatory aggregates, prominent effacement of alveolar architecture, and alveolar edema. (B) Aspiration pneumonia 400×; higher magnification showing expansion of inflammatory process composed of mostly degenerate neutrophils admixed with lymphocytes, plasma cells, and macrophages extending from bronchial epithelia into the surrounding parenchyma.
Infectious Diseases
A variety of bacterial, viral, parasitic, and fungal diseases affecting the pulmonary system have been described elsewhere in the text (see Chapters 20, 21, 22, and 23).
Systemic Toxicosis
Systemic toxicosis, observed previously reported in ferrets due to inadvertent dietary or environmental exposure to toxic compounds, is discussed in Chapter 5. Drug toxicity, like other companion animals, is also possible. From 2001–2007, the Animal Poison Control Unit of the American Society for Prevention of Cruelty to Animals reported 618 cases of suspected ferret exposures to toxic agents. More than 50% resulted from medications, most being ibuprofen, acetaminophen, and the antidepressant venlafaxine [81]. Many of these toxicoses are due to either unintentional overdosage of medications or the inherent inquisitive nature of the ferret and their tendency to ingest foreign materials.
Ibuprofen
Ibuprofen toxicosis results in prostaglandin inhibition, gastrointestinal tract bleeding, platelet abnormalities, and, if high doses of the drug have been ingested, renal failure can ensue [82].
Clinical Signs and Diagnosis
Over 93% of ferrets ingesting ibuprofen, according to one report, developed neurological signs, including depression, tremors, weakness, recumbency, and, in some cases, coma [81]. Over half of the ferrets also had gastrointestinal signs, including anorexia, vomiting, retching, diarrhea, and melena. Renal failure, metabolic acidosis, and hypothermia were also recorded. In 13 of 43 cases, clinical signs developed within 4 hours; in 6 ferrets, signs developed in 5–8 hours. The longest period was 48 hours post exposure in one ferret. Onset of signs was not apparent in nine cases. Of the 43 reported cases, 4 ferrets died; the lowest dose associated with death was 220 mg/kg [81].
Treatment
Treatment is centered around preventing and treating gastric bleeding, CNS signs, and renal compromise. If immediate clinical intervention is possible (1–2 hours post ingestion), emesis should be induced [81]. Diuresis is recommended for 24–36 hours to prevent renal failure. Kidney function should be monitored during and post recovery. Gastrointestinal protectants such as misoprostol (a synthetic prostaglandin) at a dose of 1–5 μg/kg PO every 8 hours is recommended. Sucralfate at a dose of 1/8 g every 6 hours is also used. H2 blockers or proton pump inhibitors can also be used. Prolonged supportive therapy may be required.
Acetaminophen Toxicity
In ferrets, glucuronidation of acetaminophen is relatively slow compared with other animal species, except for cats [82]. In the cat, in which fewer acetaminophen-UDP-glucuronosyltransferase (UGT) isoforms are expressed in the liver compared with other animal species, cats glucuronidate many compounds slowly or not at all. UGTIA6, one of the principal isoforms mediating glucuronidation of phenolic compounds, is absent in the feline liver [83]; the gene normally encoding this enzyme is a pseudogene, containing numerous deleterious mutations [84]. However, in the ferret, no mutations were noted in the UGTIA6 gene, which could account for the ferret's reduced ability to glucuronidate acetaminophen. Interestingly, male ferrets can glucuronidate acetaminophen more efficiently than female ferrets.
Clinical Signs and Diagnosis
Clinical signs are expected 12–48 hours after ingestion of acetaminophen. Because acetaminophen causes RBC depletion of glutathione, methemoglobinemia ensues. Hepatic damage may also occur.
Treatment
If the ferret is presented within 1–2 hours after ingesting the drug, emesis should be induced. Whole blood transfusion may be needed if anemia, hemoglobinuria, and hematuria are severe. Sustained clinical management is advised in these cases. Measurement of blood glutathione levels provides a guide to the effectiveness of treatment and prognosis [82].
Zinc Toxicity
Zinc poisoning was observed in a group of experimentally housed ferrets fed exclusively a raw meat diet that had been accidentally contaminated with zinc leached from galvanized feeding pans and water dishes [16,85,86].
Clinical Signs and Diagnosis
Unfortunately, the exact dose of zinc the animals received is unknown, only that galvanized-wire caging and feeding utensils was the source, accelerated by steam (82°C for 20 minutes) sterilization. Swabbed samples from that caging contained approximately 2400 ppm zinc compared with cotton wool which only contained 12 ppm zinc.
Presumptive zinc toxicity is based on clinical signs, and pathologic confirmation is made by analyses of liver and kidney and on demonstration of elevated levels of zinc in the tissue. In proven cases of zinc toxicity, liver levels were 203–881 ppm in livers (dry weight) and 785–943 ppm in kidneys (dry weight).
All ages are susceptible to the toxicity. Affected animals have pale mucous membranes caused by anemia. Posterior weakness and lethargy are present. The disease was reported on two ferret farms in New Zealand; all animals were affected on one farm [16].
Pathologic Findings
Lesions are primarily restricted to the kidney; grossly, the kidneys are enlarged, pale, and soft. In some cases, there are small depressions on the capsular surface [85]. Livers are orange, and the stomach has erosions with digested blood on the gastric mucosa surface. Histologically, the kidneys have collapsed glomeruli and dilated tubules, with some tubules containing proteinaceous material and cellular debris. Focal cortical interstitial fibrosis is also seen. Histologically, the liver has periacinar fatty infiltration. Hemorrhage is present in the gastric pits, as well as mucosal erosions, and blood loss occurs into the gastric lumen. Bone marrow analysis shows depression of the erythroid series. An investigation by the same authors determined that nephrosis was consistent in ferrets consuming a diet containing 500–1500 ppm zinc as zinc oxide [85].
2. Marsh RF, Burger D, Eckroade R, Zu Rhein GM, Hanson RP (1969) A preliminary report on the experimental host range of the transmissible mink encephalopathy agent. J Infect Dis 120: 713–719.
3. Sigurdson CJ, Mathiason CK, Perrott MR, Eliason GA, Spraker TR, et al. (2008) Experimental chronic wasting disease (CWD) in the ferret. J Comp Pathol 138: 189–196.
4. Perrott MR, Sigurdson CJ, Mason GL, Hoover EA (2012) Evidence for distinct chronic wasting disease (CWD) strains in experimental CWD in ferrets. J Gen Virol 93: 212–221.
5. Matthews WB (1975) Epidemiology of Creutzfeldt–Jakob disease in England and Wales. J Neurol Neurosurg Psychiatry 38: 210.
6. Matthews WB, Campbell M, Hughes JT, Tomlinson AH (1979) Creutzfeldt–Jakob disease and ferrets. Lancet 2: 828.
7. Frederick MA (1981) Intervertebral disc syndrome in a domestic ferret. Vet Med Small Anim Clin 76: 835.
8. Bernard SL, Leathers CW, Brobst DF, Gorham JR (1983) Estrogen induced bone marrow depression in ferrets. Am J Vet Res 44: 657.
9. Sherrill A, Gorham JR (1985) Bone marrow hypoplasia associated with estrus in ferrets. Lab Anim Sci 35: 280.
10. Greenlee PG, Stephens E (1984) Meningeal cryptococcosis and congestive cardiomyopathy in a ferret. J Am Vet Med Assoc 184: 840.
11. Symmers WSC, Thomson APD (1953) Observations on tuberculosis in the ferret (Mustela furo L.). J Comp Pathol Ther 63: 20.
12. Niezgoda M, Briggs DJ, Shaddock J, Dressen DW, Rupprecht CE (1997) Pathogenesis of experimentally induced rabies in domestic ferrets. Am J Vet Res 58: 1327.
13. Hamir AN, Niezgoda M, Rupprecht CE (2011) Recovery from and clearance of rabies virus in a domestic ferret. J Am Assoc Lab Anim Sci 50: 248–251.
14. Martínez A, Martinez J, Burballa A, Martorell J (2011) Spontaneous thecoma in a spayed pet ferret (Mustela putorius furo) with alopecia and swollen vulva. J Exot Pet Med 20: 308–312.
15. Palley LS, Corning BF, Fox JG, Murphy JC, Gould DH (1992) Parvovirus-associated syndrome (Aleutian disease) in two ferrets. J Am Vet Med Assoc 201: 100–106.
16. Field and Laboratory Service Veterinary Staff (1984) Diseases of the fitch. Surveillance 11: 28.
17. Rosengurt N, Stewart D, Sanchez S (1995) Diagnostic exercise: ataxia and incoordination in ferrets. Lab Anim Sci 45: 432–434.
18. Rudling W, Gent N (1994) Aleutian disease in laboratory ferrets. Anim Technol 45: 149.
19. Welchman DdeB, Oxenham M, Done SH (1993) Aleutian disease in domestic ferrets: diagnostic findings and survey results. Vet Rec 132: 479.
21. Perpinan D, Lopez C (2008) Clinical aspects of systemic granulomatous inflammatory syndrome in ferrets (Mustela putorius furo). Vet Rec 162: 180–184.
22. Garner MM, Ramsell K, Morera N, Juan-Salles C, Jimenez J, et al. (2008) Clinicopathologic features of a systemic coronavirus-associated disease resembling feline infectious peritonitis in the domestic ferret (Mustela putorius). Vet Pathol 45: 236–246.
23. Martinez J, Reinacher M, Perpinan D, Ramis A (2008) Identification of group 1 coronavirus antigen in multisystemic granulomatous lesions in ferrets (Mustela putorius furo). J Comp Pathol 138: 54–58.
24. Crawford PC, Sellon RK (2010) Canine viral diseases. In: Ettinger SJ, O'Brien DP, eds. Textbook of veterinary internal medicine, 7th ed. St. Louis, MO: Elsevier Saunders, pp. 958–970.
25. O′Brien DP (2010) Brain diseases. In: Ettinger SJ, Feldmen EC, eds. Textbook of veterinary internal medicine, 7th ed. St. Louis, MO: Elsevier Saunders, pp. 1414–1445.
26. Krakowka S, Olsen RG, Axthelm MK, Rice J, Winters K (1982) Canine parvovirus infection potentiates canine distemper encephalitis attributable to modified live-virus vaccine. J Am Vet Med Assoc 180: 137–139.
27. Slater EA (1970) The response to measles and distemper virus in immuno-suppressed and normal dogs. J Am Vet Med Assoc 156: 1762–1766.
28. Davidson M (1986) Canine distemper virus infection in the domestic ferrets. Compend Contin Educ Pract Vet 8: 448–453.
29. Carpenter JW, Appel MJG, Erickson RC, Novilla MN (1976) Fatal vaccine-induced canine distemper virus infection in black-footed ferrets. J Am Vet Med Assoc 169: 961.
30. Kauffman CA, Bergman AG, O′Connor RP (1982) Distemper virus infection in ferrets: an animal model of measles induced immunosuppression. Clin Exp Immunol 47: 617.
31. Sullivan ND (1985) The nervous system. In: Jubb KVF, Kennedy PC, Palmer N, eds. Pathology of domestic animals, 3rd ed. New York: Academic Press, pp. 201–338.
32. Niemi SM, Newcomer CE, Fox JG (1984) Neurological syndrome in the ferret (Mustela putorius furo). Vet Rec 114: 455.
33. Dillberger JE (1985) Polycystic kidneys in a ferret. J Am Vet Med Assoc 186: 74.
34. Ryland LM, Gorham JF (1978) The ferret and its diseases. J Am Vet Med Assoc 173: 1154.
35. Andrews PLR, Illman O, Mellersh A (1979) Some observations of anatomical abnormalities and disease states in a population of 350 ferrets (Mustela furo). Z Versuchstierkd 21: 346.
36. Utroska B, Austin WL (1979) Bilateral cataracts in a ferret. Vet Med Sm Anim Clin 74: 1176.
37. Miller PE, Marlar AB, Dubielzig RR (1993) Cataracts in a laboratory colony of ferrets. Lab Anim Sci 43: 562–568.
38. Kawasaki T (1992) Retinal atrophy in the ferret. J Small Exot Anim Med 1: 137.
39. Kern TJ (1989) Ocular disorders of rabbits, rodents and ferrets. In: Kirk RW, ed. Current veterinary therapy X. Philadelphia: W.B. Saunders, pp. 681–685.
40. Bunce GE, Hess HL (1976) Lenticular opacities in young rats as a consequence of maternal diets low in tryptophan and or vitamin E. J Nutr 106: 222–229.
41. Martin CL, Chambreau T (1982) Cataract production in experimentally orphaned puppies fed a commercial replacement for bitch's milk. J Am Anim Hosp Assoc 18: 115–119.
42. Vainisi SJ, Edelhauser HF, Wolf ED, Cotlier E, Reeser F (1981) Nutritional cataracts in timber wolves. J Am Vet Med Assoc 179: 1175–1180.
43. Rosenthal KL, Wyre NR (2012) Endocrine diseases. In: Quesenberry KE, Carpenter JW, eds. Ferrets, rabbits, and rodents: clinical medicine and surgery, 3rd ed. St. Louis, MO: Elsevier, pp. 91–92.
44. Phair KA, Carpenter JW, Schermerhorn T, Ganta CK, DeBey BM (2011) Diabetic ketoacidosis with concurrent pancreatitis, pancreatic beta islet cell tumor, and adrenal disease in an obese ferret (Mustela putorius furo). J Am Assoc Lab Anim Sci 50: 531–535.
45. Funk AJ, Donnelly TM (2013) Cataracts. In: Mayer J, Donnelly TM, eds. Clinical veterinary advisor: birds and exotic pets, 1st ed. St. Louis, MO: Elsevier Saunders, pp. 436–437.
46. McCalla TL, Erdman SE, Kawasaki TA, Coleman LA, Li X, et al. (1997) Lymphoma with orbital involvement in two ferrets. Vet Comp Opthal 7: 36–38.
47. Ropstad EO, Leiva M, Pena T, Morera N, Martorell J (2011) Cryptococcus gattii chorioretinitis in a ferret. Vet Ophthalmol 14: 262–266.
48. Methiyapun S, Myers RK, Pohlenz JF (1985) Spontaneous plasma cell myeloma in a ferret (Mustela putorius furo). Vet Pathol 22: 517–519.
49. Eshar D, Wyre NR, Griessmayr P, Durham A, Hoots E (2010) Diagnosis and treatment of myelo-osteolytic plasmablastic lymphoma of the femur in a domestic ferret. J Am Vet Med Assoc 237: 407–414.
50. Garner MM, Ramsell K, Schoemaker NJ, Sidor IF, Nordhausen RW, et al. (2007) Myofasciitis in the domestic ferret. Vet Pathol 44: 25–38.
51. Ramsell KD, Garner MM (2010) Disseminated idiopathic myofasciitis in ferrets. Vet Clin North Am Exot Anim Pract 13: 561–575.
52. Reed AM, Ernste F (2009) The inflammatory milieu in idiopathic inflammatory myositis. Curr Rheumatol Rep 11: 295–301.
53. Dougherty SA, Center SA, Shaw EE, Erb HA (1991) Juvenile-onset polyarthritis syndrome in Akitas. J Am Vet Med Assoc 198: 849–856.
54. Schoemaker NJ, Lumeij JT, Rijnberk A (2005) Current and future alternatives to surgical neutering in ferrets to prevent hyperadrenocorticism. Vet Med 100: 484–485.
55. Thornton RN, Cook TG (1986) A congenital Toxoplasma-like disease in ferrets (Mustela putorius furo). N Z Vet J 34: 31.
56. Daoust PY, Hunter DB (1978) Spontaneous Aleutian disease in ferrets. Can Vet J 19: 133.
57. Li X, Fox JG, Padrid PA (1998) Neoplastic diseases in ferrets: 574 cases (1968–1997). J Am Vet Med Assoc 212: 1402–1406.
58. Batchelder M, Erdman SE, Li X, Fox JG (1996) A cluster of cases of juvenile mediastinal lymphoma in a ferret colony. Lab Anim Sci 46: 271–274.
59. Stamoulis ME (1995) Cardiac diseases in ferrets. Semin Avian Exot Pet 4: 43–48.
60. Parrott TY, Greiner EC, Parrott JD (1984) Dirofilaria immitis infection in three ferrets. J Am Vet Med Assoc 184: 582.
61. Miller WR, Merton DA (1982) Dirofilariasis in a ferret. J Am Vet Med Assoc 180: 1103.
62. Moreland AF, Battles AH, Nease JH (1986) Dirofilariasis in a ferret. J Am Vet Med Assoc 188: 864.
63. Hoover JP, Baldwin CA, Rupprecht CE (1989) Serologic response of domestic ferrets (Mustela putorius furo) to canine distemper and rabies virus vaccines. J Am Vet Med Assoc 194: 234–238.
64. Robinson RF, Maxie MG (1985) The cardiovascular system. In: Jubb KVF, Kennedy PC, Palmer N, eds. Pathology of domestic animals, 3rd ed. New Orlando, FL: Academic Press, pp. 1–81.
66. MacDonald K (2010) Myocardial disease. In: Ettinger SJ, O'Brien DP, eds. Textbook of veterinary internal medicine, 7th ed. St. Louis, MO: Elsevier Saunders, pp. 1328–1341.
67. Ensley PK, Winkle TV (1982) Treatment of congestive heart failure in a ferret. J Zoo Anim Med 13: 23.
68. Lipman N, Fox JG (1987) Clinical, functional, and pathologic changes associated with a case of dilatative cardiomyopathy in a ferret. Lab Anim Sci 37: 210.
69. Weiss CA, Scott MV (1997) Clinical aspects and surgical treatment of hyperadrenocorticism in the domestic ferret: 94 cases (1994–1996). J Am Anim Hosp Assoc 33: 487–493.
70. Rosenthal KL, Peterson ME, Quesenbury KE, Hillyer EV, Beeber NL, et al. (1993) Hyperadrenocorticism associated with adrenocortical tumor or nodular hyperplasia of the adrenal gland in ferrets: 50 cases (1987–1991). J Am Vet Med Assoc 203: 271–275.
71. Harpster NR (1986) Feline myocardial diseases. In: Kirk R, ed. Current veterinary therapy IX. Philadelphia: W.B. Saunders, p. 380.
72. Malakoff RL (2013) Heart diseases, structural. In: Mayer J, Donnelly TM, eds. Clinical veterinary advisor: birds and exotic pets, 1st ed. St. Louis, MO: Elsevier Saunders, pp. 458–460.
73. Jenkins JR, Brown SA (1993) A practitioner's guide to rabbits and ferrets. Lakewood, CO: American Animal Hospital Association.
74. Pion PD, Kittleson MD, Rogers QR (1989) Cardiomyopathy in the cat and its relation to taurine deficiency. In: Kirk RW, Bonagura JD, et al., eds. Current veterinary therapy X small animal practice. Philadelphia: W.B. Saunders, pp. 251–262.
75. Walden NB (1978) Taurine conjugates as metabolites of arylacetic acids in the ferret. Xenobiotica 8: 253–264.
76. Dungworth DC (1985) The respiratory system. In: Jubb KVF, Kennedy PC, Palmer N, eds. Pathology of domestic animals, 3rd ed. New York: Academic Press, pp. 413–556.
77. Hammond JJ, Chesterman FC (1972) The ferret. In: The Universities Federation for Animal Welfare, ed. The Universities Federation for Animal Welfare handbook on the care and management of laboratory animals. London: Churchill Livingstone, pp. 357–366.
78. Borst GH, Zwart P, Mullink HW, Vroege C (1976) Bone structures in avian and mammalian lungs. Vet Pathol 13: 93–103.
79. Blanco MC, Fox JG, Rosenthal K, Hillyer EV, Quesenberry KE, et al. (1994) Megaesophagus in nine ferrets. J Am Vet Med Assoc 205: 444–447.
80. Kealy JK (1979) Diagnostic radiology of the dog and cat. Philadelphia: W.B. Saunders. 467 p.
81. Richardson JA, Balabuszko RA (2001) Ibuprofen ingestion in ferrets: 43 cases January 1995–March 2000). J Vet Emerg Crit Care 11: 53–58.
82. Graham J (2013) Ibuprofen and acetaminophen toxicity. In: Mayer J, Donnelly TM, eds. Clinical veterinary advisor: birds and exotic pets, 1st ed. St. Louis, MO: Elsevier Saunders, pp. 464–465.
83. Court MH (2001) Acetaminophen UDP-glucuronosyltransferase in ferrets: species and gender differences, and sequence analysis of ferret UGT1A6. J Vet Pharmacol Ther 24: 415–422.
84. Court MH, Greenblatt DJ (2000) Molecular genetic basis for deficient acetaminophen glucuronidation by cats: UGT1A6 is a pseudogene, and evidence for reduced diversity of expressed hepatic UGT1A isoforms. Pharmacogenetics 10: 355–369.
85. Straube EF, Schuster NH, Sinclair AJ (1980) Zinc toxicity in the ferret. J Comp Pathol 90: 355–361.
86. Straube EF, Walden NB (1981) Zinc poisoning in ferrets (Mustela putorius furo). Lab Anim 15: 45–47.