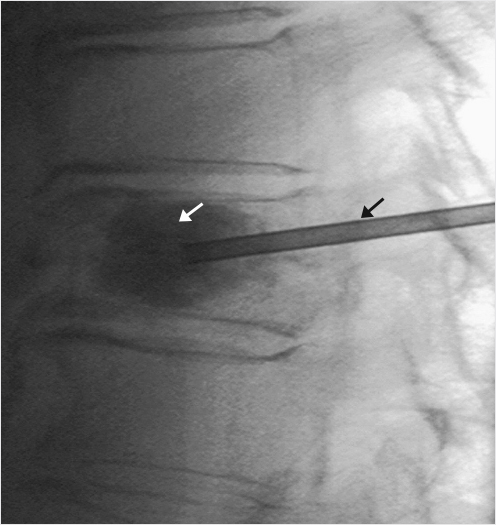
Fig. 1.1 Lateral view on a conventional radiograph demonstrates a vertebral compression fracture (black arrow).
Summary
Vertebral augmentation is a category of minimally invasive procedures that have become central in the treatment of pathologic and painful vertebral compression fractures (VCFs) due to osteoporosis, trauma, and neoplasia. Osteoporotic VCFs are the most common indication for vertebral augmentation, which has also been used to treat fractures in patients with benign tumors such as hemangiomas or Langerhans cell vertebral histiocytosis (LCVH) and in genetic disorders that give rise to weak vertebrae such as osteogenesis imperfecta. In theory, near immediate anterior column stability and pain relief follows an intravertebral injection of bone cement that stabilizes the osseous fractures and eliminates osseous and periosteal movements, while thermal polymerization of the cement ablates pain receptors in the basivertebral plexus, trabecular bone, and subjacent to the vertebral end plates. Over three decades of innovation and advancements have produced treatment options with improved safety and efficacy. Results of numerous studies have demonstrated reduction of pain, and improved function and quality of life. Responses have been significant and durable across a wide range of etiologies.
Keywords: vertebral compression fracture, vertebral augmentation, vertebroplasty, balloon kyphoplasty, osteoporosis, spinal metastasis, multiple myeloma, bone cement, vertebral implants
Acrylic cements have been used for augmentation of weakened or partially destroyed bones for decades. The first use of methyl methacrylate as an adjunct to internal fixation of malignant neoplastic fractures was reported in 1972.1 Vertebral augmentation has since become central in the treatment of pathologic vertebral compression fractures (VCFs) due to osteoporosis, trauma, and neoplasia. The procedure has also been used to treat fractures in patients with benign tumors such as hemangiomas or LCVH and in genetic disorders that give rise to weak vertebrae such as osteogenesis imperfecta.2–7
Osteoporotic VCFs (OVCFs) are the most common indication for vertebral augmentation. As with any fracture, principles of fixation for VCFs include vertebral body (VB) reduction to restore normal anatomical relationships, fixation to provide absolute or relative stability, preservation of blood supply to soft tissues and bone, and early safe mobilization of the injured part and the patient (▶Fig. 1.1).
Before the availability of vertebral augmentation, the principal surgical option for compression fractures was decompression and instrumented fusion. Outcomes were often dismal in elderly osteoporotic patients.8 Nonoperative management options were equally disappointing. Initial management included bed rest and immobilization in an external orthotic if feasible and tolerable, depending on the degree of kyphosis and pain. Narcotics were prescribed for analgesia and nasal calcitonin for antiresorptive and analgesic effects. Bed rest and immobilization, however, led to accelerated osteoporotic bone loss and many elderly patients were at risk of polypharmacy and narcotic side effects including constipation, confusion, and respiratory depression as well as the many unappreciated consequences of social isolation.9,10 Patients treated with nonsurgical management (NSM) were also at an increased risk of mortality primarily from pneumonia due to their deconditioned status.11
Fig. 1.1 Lateral view on a conventional radiograph demonstrates a vertebral compression fracture (black arrow).
Two general hypotheses prevail regarding the mechanism of pain relief offered by augmentation of VCFs: (1) an intravertebral injection of polymethyl methacrylate (PMMA) cement stabilizes micro-fractures and eliminates periosteal micro-movements and pain; (2) thermal polymerization of PMMA following injection ablates pain receptors in the trabecular bone, vertebral periosteum, and vascular structures. This combination leads to near immediate postoperative anterior column stability and pain relief.12 Although ablation of the basivertebral nerve within the VB does produce significant pain relief in patients with diskogenic back pain, degenerative end plate changes, and an intact VB,13 low exothermic or nonexothermic bone cements can produce equivalent pain relief in patients with VCFs to that of cements with thermal neuroablation capability.14 The pain relief in patients with VCFs, therefore, is much more likely or completely due to the reestablishment of the mechanical stability of the VB rather than the ablative effects of the fill material on the VB innervation.
Vertebroplasty was first performed in 1984 but not reported until 1987. In the first known image-guided percutaneous vertebral augmentation, Galibert et al successfully injected PMMA into a C2 vertebra that had been partially destroyed by an aggressive hemangioma.15
Vertebroplasty involves the percutaneous injection of cement such as PMMA directly into the cancellous bone of a fractured VB to alleviate pain and prevent further loss of VB height or progression of kyphotic deformity. Although the procedure does not improve spinal deformity, it stabilizes the vertebra and improves the function of individuals debilitated by painful VCFs (▶Fig. 1.2).
Fig. 1.2 A vertebroplasty procedure is demonstrated with the cannula of the needle (black arrow) placed in the vertebral body and the polymethylmethacrylate is shown within the vertebral body (white arrow).
Kyphoplasty was first performed in 1998 as a modification of vertebroplasty with the intent of restoring vertebral height and reducing kyphotic angulation for improved outcomes and reduced procedural risks. VCFs cause debilitating pain and may also be associated with significant kyphosis. Kyphosis reduces compartment sizes of the chest, abdomen, and pelvis, which results in pulmonary restriction, decreased appetite, and urinary incontinence. These processes can lead to life-altering deconditioning, weight loss, social isolation, and depression.
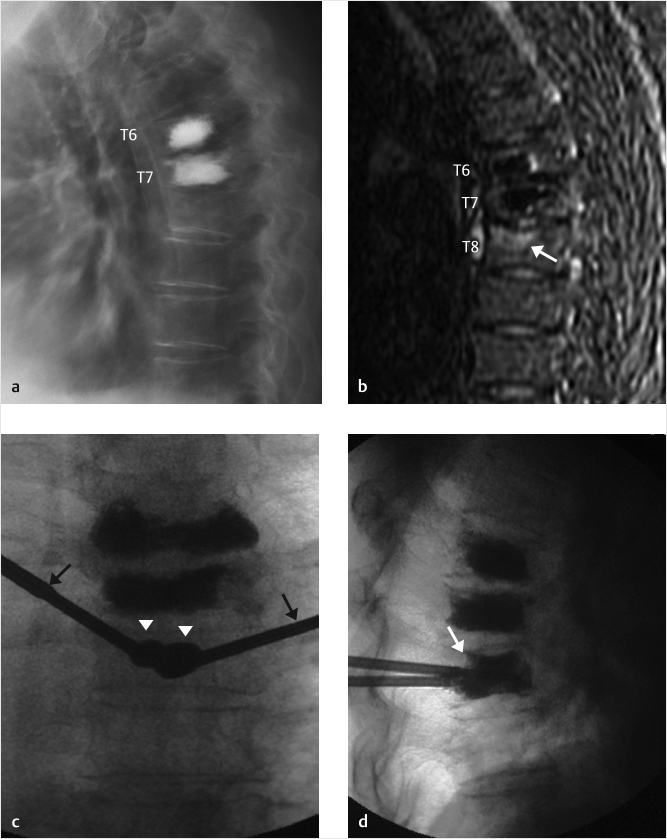
During kyphoplasty, a balloon tamp is inflated within the VB to compress and displace cancellous bone prior to the injection of cement. This creates a cavity that can reduce the vertebral fracture and after removal of the balloon allows the injection of cement directly into the cavity that is the path of least resistance. This injection of cement into the cavity allows for greater control of the cement and reduces the risk of cement leakage (▶Fig. 1.3).
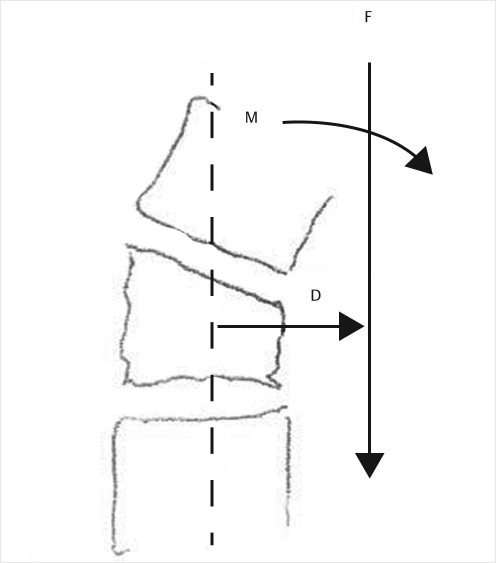
Inflation of the tamp restores VB height and reduces kyphotic angulation to improve sagittal alignment, attenuating the risk of progressive deformity by reducing the bending moment (M).16,17 Illustrating the importance of the moment arm, Archimedes said, “Give me a lever long enough and a place to stand and I will move the earth.” VB failure is believed to result from an excessive bending moment, which is the product of the moment arm (the distance between the mid VB and the plumb line representing the center of gravity, D) and the force (gravity, F) applied to the moment arm18 (▶Fig. 1.4). The moment arm, and therefore the bending moment and risk of VB failure, increases as kyphosis progresses.
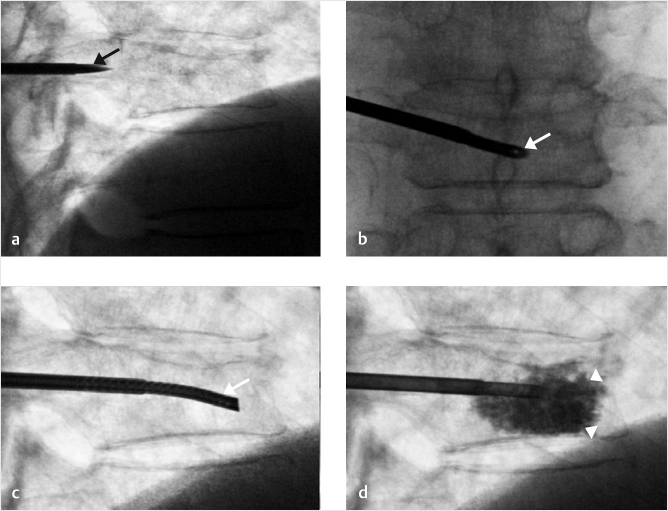
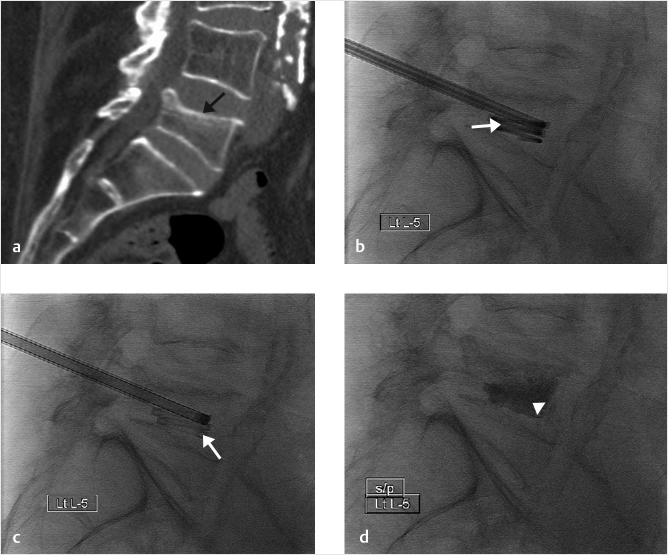
A novel technique approved for use in the United States in 2008 (StabiliT Vertebral Augmentation System, Merit Medical, Jordan, UT, United States) is radiofrequency kyphoplasty (RFK). RFK uses radiofrequency heat to control the viscosity of the PMMA that is injected into the VB. Rather than using inflatable bone tamps, a small navigational cannula is inserted unilaterally into the vertebra. The cannula creates pathways for the cement and preserves more of the existing cancellous bone. The pathways are filled with ultra–high viscosity bone cement, which permeates into the surrounding bone, stabilizes the fracture, and restores vertebral height (▶Fig. 1.5). The infusion of ultra–high viscosity cement in a slower and more controlled fashion is designed to reduce the risk of cement leakage.19–23
Radiofrequency ablation (RFA) is a modified electrocautery technique for use in select patients with painful spinal metastases.24 RFA and vertebral augmentation is a combination therapy for painful osseous metastases that cannot be or are incompletely palliated with radiation therapy. Combined treatment with RFA and vertebral augmentation has been successful in reducing pain and in improving function and quality of life.24–28 Using image guidance, a partially insulated electrode attached to a radiofrequency generator is passed into the vertebra.29,30 The heat generated by radiofrequency energy (50–90°C) causes destruction of the malignant tissue and creates a small cavity in the VB31,32 (▶Fig. 1.6). Additionally, percutaneous radiofrequency ablation destroys sensory nerve fibers, and tumor cells that release nerve-stimulating factors. There is also evidence to show that RFA carried out before percutaneous vertebral augmentation reduces the risk of cement leakage.33
Fig. 1.3 (a) Kyphoplasty in a patient with two previous vertebral augmentation procedures at T6 and T7. (b) The patient had recurrence of pain and adjacent level vertebral fracture at T8 (white arrow). (c) An anteroposterior fluoroscopic view of the mid-thoracic spine with balloons (white arrowheads) placed through two needle cannulas (black arrows). (d) The lateral fluoroscopic view shows cement injected into the vertebral body (white arrow).
Examples of devices for RFA include STAR Tumor Ablation System (Merit Medical, Jordan, UT, United States), CAVITY SpineWand (ArthroCare, Austin, TX, United States), and OsteoCool RF Ablation system (Medtronic, Dublin, Ireland). The OsteoCool ablation probe is internally cooled with circulating water. The RF energy heats the tissue, while circulating water moderates the temperature. The system automatically moderates power to keep RF heating within the desired treatment range. This combination creates large-volume lesions without excessive heating, thereby reducing risks of potential thermal damage to adjacent tissue.
Significant and lasting pain relief has been achieved with both vertebroplasty and kyphoplasty. Restoration of height does not appear requisite for pain relief, but height restoration and reduction of kyphotic angulation are important components in the reestablishment of normal sagittal balance and protection from future fractures.17,34 Recovery of VB height during kyphoplasty may be partially lost over time. Newer next-generation vertebral augmentation systems have been introduced to improve fracture reduction, indefinitely restore the height of the VB, and further reduce risks of cement leakage.35,36
SpineJack (Stryker, Kalamazoo, MI, United States) is a titanium implant inserted using a bilateral transpedicular approach to treat fractures between and including T5 and L5. A direct lift mechanism expands vertically like a car jack and allows for progressive controlled reduction of the fracture prior to cement injection (▶Fig. 1.7).32
The OsseoFix Spinal Fracture Reduction System (Alphatec Spine, 2009) is a titanium mesh device that expands into the VB and acts as a scaffold to facilitate reduction and stabilization of fractures between and including T6 and L5. There is no direct lift mechanism, but the foreshortening of the titanium tube reduces the end plate by direct superior and inferior pressure from the center of the tube as it expands during the implant’s deployment. The mesh expands to compact the trabecular bone and increase the VB height, allowing cement interdigitation.37 The device was introduced as an alternative to vertebroplasty and kyphoplasty to reduce cement leakage (▶Fig. 1.8).
The Vertebral Body Stenting System (VBS) consists of an expandable cobalt–chromium alloy stent mounted on a balloon catheter. The device is typically inserted via a bilateral transpedicular approach and inflated to maximum of 30 atm to symmetrically expand both stents. The stent is optimally expanded to a maximum diameter of 17 mm and balloons are deflated and removed, leaving both stents to maintain the restored height prior to injection of the cement (▶Fig. 1.9).32
Fig. 1.4 The bending moment (M) is the product of moment arm (D) and gravity (F). As kyphosis progresses, the moment arm increases, thereby increasing the risk of vertebral failure. (This image is provided courtesy of Dr. M.R. Chambers.)
The Kiva VCF Treatment System, indicated for use in the treatment of spinal fractures in the thoracic and/or lumbar spine from T6 to L5, received clearance from the U.S. Food and Drug Administration on January 24, 2014. The Kiva implant is a percutaneous uniportal vertebral augmentation device that is designed to restore VB height and reduce cement leakage. The polyether ether ketone flexible implant (PEEK-OPTIMA) is inserted over a removable, fully coiled nitinol guidewire.38 The coil is inserted into the VB and acts as a scaffold for the implant. The Kiva implant is then inserted around the coil, the coil is removed, and cement is injected through the perforated implant for controlled delivery (▶Fig. 1.10).
Primary indications for vertebral augmentation include osteoporotic compression fractures, vertebral metastasis, multiple myeloma, vertebral hemangioma, vertebral osteonecrosis, traumatic VCFs, and reinforcement of a pathologically weak VB before and during surgical stabilization procedures. In clinical practice, the most common indication is a painful osteoporotic vertebral fracture that has not responded to NSM including rest, immobilization in an orthotic brace, narcotic analgesic medications, and nasal calcitonin for antiresorptive and analgesic effects.
In 2018, a multidisciplinary expert panel of orthopaedic and neurosurgeons, interventional radiologists, and pain specialists, using the RAND/UCLA Appropriateness Method (RUAM), developed the Clinical Care Pathway (CCP), defining patient-specific recommendations for vertebral fragility fractures (VFF). The panel assessed the relative importance of signs and symptoms for the suspicion of VFF, the relevance of diagnostic procedures, and the appropriateness of vertebral augmentation versus NSM for a variety of clinical scenarios. Their report included the following guidelines for relative and absolute contraindications.39
Fig. 1.5 Radiofrequency kyphoplasty. (a) Lateral fluoroscopic view shows the needle just proximal to the posterior vertebral body wall (black arrow) entering via a transpedicular approach. (b, c) Posteroanterior and lateral fluoroscopic views show the channel creation device (white arrow) just across the midline in the anterior portion of the vertebral body. (d) Lateral fluoroscopic view shows cement being injected into the vertebral body (white arrowheads) after having just been heated with radiofrequency energy.
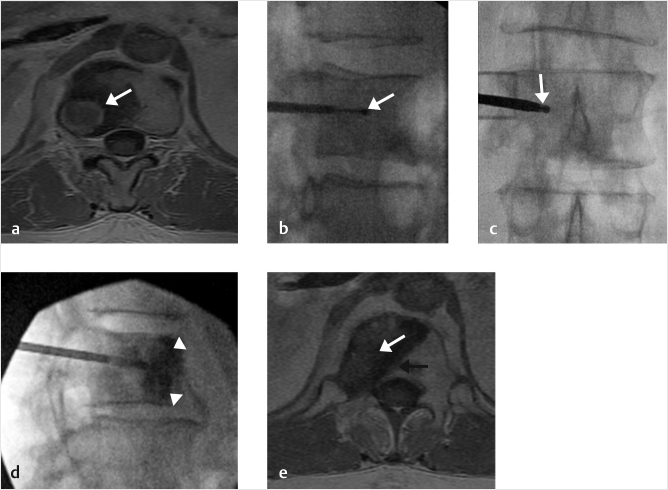
Fig. 1.6 Radiofrequency ablation. (a) Axial T1-weighted MR image shows a metastasis (white arrow) in a 55-year-old man with metastatic lung cancer. (b, c) Lateral and posteroanterior fluoroscopic views show the STAR radiofrequency device in the posterolateral portion of the L2 vertebral body (white arrows). (d) Lateral fluoroscopic view shows cement being injected into the vertebral body (white arrowheads). (e) Axial T1-weighted MR image obtained 3 months after radiofrequency ablation shows the cement within the vertebral body (black arrow) but no further evidence of the metastasis seen in a (white arrow).
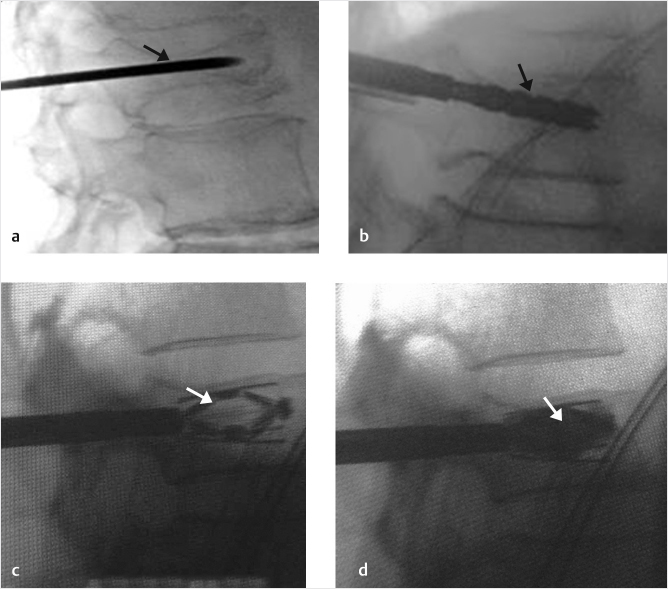
Fig. 1.7 SpineJack. Lateral fluoroscopic views obtained during a vertebral augmentation with the SpineJack shows the initial needle access into the vertebral body (black arrow in a), followed by a template to clean the site after drilling (black arrow in b). The SpineJack is then placed and expanded (white arrow in c) and then cement is injected around the implant (white arrow in d).
Absolute contraindications include active infection at the surgical site and untreated blood-borne infections, and a nonpainful osteoporotic vertebral fracture that is completely healed or is clearly responding to conservative management. Strong contraindications include osteomyelitis, pregnancy, allergy to fill material, coagulopathy, spinal instability, myelopathy from the fracture, the presence of a neurologic deficit, and neural impingement.
Relative contraindications include cardiorespiratory compromise such that safe sedation or anesthesia cannot be achieved, breach of the posterior vertebral cortex by a tumor, and/or tumor extension into the spinal canal. It was determined that fracture repulsion and canal compromise per se is not generally a contraindication, provided the fracture fragment is not causing neural impingement or clinical symptoms related to this compromise. Significant fracture retropulsion with canal compromise is a relative contraindication. A CT scan may be used to determine integrity of posterior wall in patients with mild retropulsion of fracture fragment(s). Vertebra plana has been previously mentioned as a relative contraindication as it renders the procedure technically difficult but the RUAM group determined that vertebra plana was not a relative contraindication to performing vertebral augmentation.
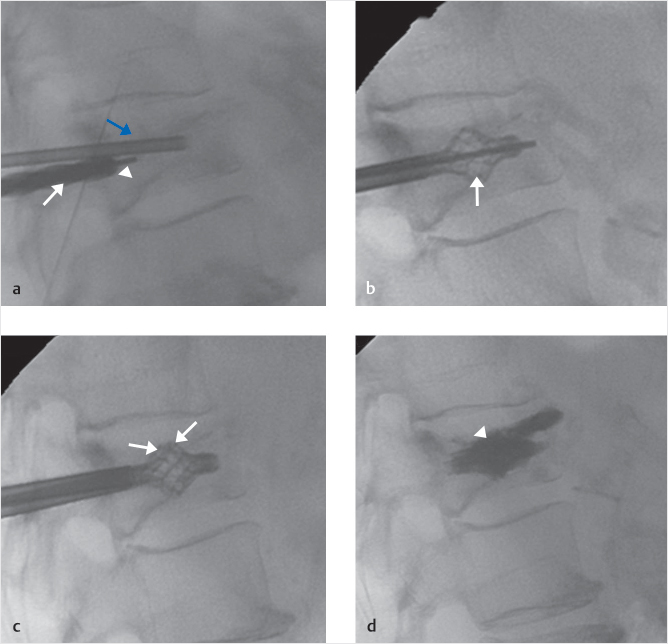
Fig. 1.8 OsseoFix spinal fracture reduction system. Lateral fluoroscopic view of a T12 vertebral compression fracture shows a needle accessing the T12 vertebral body (blue arrow in a) along with a drill (white arrow in a) being used to create a channel and guided by a K-wire (white arrowhead in a). The lateral image in (b) shows an OsseoFix implant being deployed (white arrow in b). Two implants are placed in the T12 vertebral body (white arrows in c) as shown by the lateral fluoroscopic image. Cement is added to stabilize the implants (white arrowhead in d).
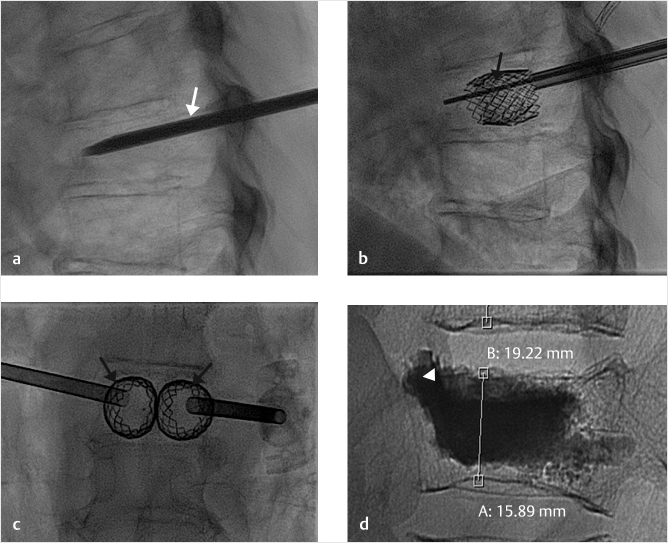
Fig. 1.9 Vertebral body stenting system (VBS). (a) Lateral fluoroscopic view of a T7 vertebral compression fracture shows a needle accessing the T7 vertebral body (white arrow). (b) The lateral fluoroscopic image shows two visually overlapping VBS implants (black arrow). (c) An anteroposterior fluoroscopic image shows two VBS implants deployed into the vertebral body (black arrows). (d) The lateral fluoroscopic image in CT shows the vertebral body after the injection of cement into the implants (white arrowhead).
Fig. 1.10 Kiva implant. Sagittal CT image shows a vertebral compression fracture of L5 (black arrow in a). Lateral fluoroscopic view shows the nitinol coil within the vertebral body (white arrow in b). Lateral fluoroscopic view shows the PEEK (polyether ether ketone) implant coiled in the vertebral body (white arrow in c) and image (d) shows the implant after the injection of cement (white arrowhead).
Complications are few but, as with any surgical procedure, may include infection, bleeding, cardiac or respiratory complications of anesthesia, injury, and failure to achieve intended goals. Potential complications specific to percutaneous augmentation include cement leakage, pulmonary embolism, radiculopathies, rib fractures, subsequent vertebral fractures, and spinal cord or neural compression.40–42
A comprehensive literature review is presented in Chapter 15. Numerous randomized controlled trials, systematic reviews, and meta-analyses have been employed to study and compare vertebral augmentation treatment options.43–45 Although we consider results from randomized controlled trials, it is important to remember that these were developed to evaluate drug therapies, not devices and surgical procedures.46 Given their relatively recent introduction, there are limited data available with sufficient power for decision-making with respect to newer vertebral augmentation implants and devices. Future trials with additional observations and longer follow-ups are anticipated.
VCFs are the most common type of fracture related to osteoporosis and are associated with significant rates of morbidity and mortality. Annual direct medical expenditures exceed $1 billion in the United States.47 Contemporary natural history data suggest that more than 70% of patients with moderate or severe pain may fail to achieve significant pain relief within 12 months of symptom onset.48 Physicians in the Neuroradiology Department at the University Hospital in Lyon, France, began to treat osteoporotic vertebral fractures with vertebroplasty in 1989. They used an 18-gauge needle to inject bone cement into seven patients, four of whom had OVCFs and the other three VCFs attributed to spinal metastases.49 They reported that seven of the eight patients had an excellent pain reduction response to the vertebroplasty and that the eighth patient had a good response.
Vertebroplasty was introduced to the United States when, in the early 1990s, clinicians from the University of Virginia performed the procedure using the technique introduced by the French clinicians.50 The use of vertebroplasty then dramatically increased, primarily for the treatment of OVCFs, until the advent of balloon kyphoplasty (BKP) in the late 1990s.
In 2009, a great deal of controversy followed the publication of two randomized trials comparing vertebroplasty and sham procedures to treat osteoporotic vertebral fractures. The studies were intended to account for placebo effect in the setting of vertebroplasty. The authors reported that, although there were substantial reductions in overall pain in both study groups, there was no statistically significant benefit offered by vertebroplasty. Critics pointed out many flaws in design, patient selection, power, and generalization of inferences of both trials.
The first study randomized 75 participants with one or two painful osteoporotic vertebral fractures confirmed by MRI and less than 1 year’s duration to vertebroplasty or a sham procedure. Participants were stratified according to treatment center, sex, and duration of symptoms. The primary outcome was “overall pain” at 3 months. There were substantial reductions in overall pain in both study groups, but vertebroplasty was not better in any measured outcome compared to controls, regardless of duration of symptoms. This trial by Buchbinder et al was to include 200 patients, but only 78 were enrolled over 4 years. Two of the four study hospitals withdrew after including only five patients each. As a result, 68% of the procedures were performed in one hospital by one radiologist. Only 32% of patients received treatment within 6 weeks of onset of pain, suggesting that many fractures being treated were already healed with expected persistent edema on MR imaging.
The second trial randomly assigned 131 patients with one to three painful OVCFs to undergo either vertebroplasty or a simulated procedure without cement. The primary outcomes were disability and the patients’ ratings of average pain intensity during the preceding 24 hours at 1 month. This study involved only outpatients; inpatients hospitalized with acute fracture pain were excluded. The protocol required 4 weeks of medical therapy before enrollment was possible and fractures were present for up to 1 year. Only 44% of patients had pain of less than 6 weeks’ duration; 56% of patients had pain for over 3 months. The minimum pain score for enrollment was 3/10 and the average pain score was 6.9. As patients with maximal back pain tend to have the greatest improvement on pain score, bias was presumably introduced, as those patients with the greatest pain likely did not agree to participate in a trial that might randomize them to a nontreatment arm. Finally, a significantly greater crossover from the control group versus the vertebroplasty group could indicate dissatisfaction with the sham procedure that was not captured by pain scales.51
In 2001, Garfin et al reported on new technologies in the spine for the treatment of painful OVCF and noted a 95% improvement in pain and significant improvement in function following BKP. Vertebral height and kyphosis were improved by over 50% when kyphoplasty was performed within 3 months of the onset of pain, less so if treatment was delayed more than 3 months. Both vertebroplasty and kyphoplasty were described as “safe and effective” in the treatment of painful OVCF that did not respond to conventional treatments. Kyphoplasty was noted to facilitate realignment of the spinal column and regain VB height—morphologic improvements thought to decrease pulmonary, gastrointestinal, and early morbidity consequences of fractures.52 Numerous prospective and retrospective studies have since demonstrated the safety and efficacy of kyphoplasty in the treatment of pain and deformity of OVCF.53
Results of the FREE trial, a randomized controlled trial comparing the efficacy and safety of BKP to nonsurgical care for VCFs were published in 2009.54 Adults with one to three acute painful vertebral fractures from T5 to L5 due to primary or secondary osteoporosis, multiple myeloma, or osteolytic metastatic tumors were enrolled at 21 sites in eight countries. Participants were randomized and the primary outcome, the change from baseline to 1 month in the short-form 36 (SF-36) physical component summary (PCS) score, was evaluated at 1 month. Patients in the kyphoplasty group had statistically significant improvement in mean SF-36 PCS scores at 1 month when compared to the control group.
Next, Van Meirhaeghe et al performed a multicenter randomized controlled trial comparing BKP to NSM with a focus on surgical aspects and radiographic vertebral deformity. Adults with one to three VCFs were randomized within 3 months of onset of pain to undergo bilateral BKP or NSM. Compared to NSM, the BKP group had greater improvements in SF-36 PCS scores at 1 month and greater functionality assessed with “timed up and go.” At 24 months, BKP improved quality of life, decreased the pain averaged during 24 months, and resulted in better improvement of index VB kyphotic angulation.53
The EVOLVE trial, a large prospective, clinical study of kyphoplasty, investigating 12-month disability, quality of life, and safety outcomes specifically in a Medicare-eligible population, published in 2017, represented characteristic patients seen in routine clinical practice. A total of 354 patients with painful VCFs were enrolled at 24 U.S. sites with 350 undergoing kyphoplasty. Four co-primary endpoints included back pain, disability, function, and quality of life. With all endpoints demonstrating statistically significant improvement at every time point, kyphoplasty was deemed a safe, effective, and durable procedure for treating patients with painful VCF due to osteoporosis or cancer.55
A cadaveric study of 24 VB fractures comparing SpineJack to BKP showed height restoration was better in the SpineJack group. Clinical implications included better sagittal balance restoration and reduction of kyphotic deformity with the potential for fewer adjacent level vertebral fractures with the SpineJack.56
A single prospective randomized post-market clinical study compared the safety and effectiveness of SpineJack to the KyphX Xpander Inflatable Bone Tamp to treat 30 patients with painful OVCFs. Reduction of pain and disability was greater in the SpineJack group immediately following and at 12 months after the procedure. Quality of life showed distinct improvements in both groups. Patients in the SpineJack cohort had fewer adjacent level fractures (ALFs) at 1 year, while the additional VCF rate was approximately the same between the two groups. SpineJack produced a larger restoration of the VB angle, which was still evident 12 months after implantation.57
Preliminary data available at the time of this writing from the 151-patient randomized placebo-controlled SAKOS trial comparing the SpineJack to the KyphX Xpander Inflatable Bone Tamp also suggests that both SpineJack and BKP have comparable effects on functional improvement and quality of life, but SpineJack appears to be significantly better than BKP for pain relief and VB height restoration with a decreased rate of adjacent fractures.58
In terms of pain relief measured by the Visual Analog Scale (VAS), 5 days after surgery, there was a marked reduction in pain in both patient groups. The mean reduction was around 50 mm, but there was no significant difference between the two groups. The pain progressively improved over the first 6 months in the SpineJack group only resulting in a significantly improved pain score in the SpineJack group as compared to the BKP group at 1 month (p = 0.029) and at 6 months (p = 0.021) after surgery.
When evaluating ALFs, the responder rate at month 6 in the intention to treat (ITT) population was significantly higher following the SpineJack procedure compared to BKP (88.1 vs. 59.7%; p < 0.0001) and superiority for ALF reduction for the SpineJack procedure was confirmed at 12 months with a responder rate of 73.5 versus 42.9% with BKP (p < 0.0001).
In the ITT population, the mean restoration of midline height was significantly more following the SpineJack procedure than after BKP (1.14 ± 2.61 vs. 0.24 ± 2.21 mm; median: 0.90 vs. 0.45 mm; p = 0.0163). This result was confirmed in the per protocol (PP) population as well (p = 0.0060).
A prospective consecutive cohort study determined OsseoFix to be a successful and safe minimally invasive therapy for OVCFs, even those with posterior wall involvement. Twenty-four patients with 32 OVCFs from T6 to L4 were treated with OsseoFix. After 12 months, there were significant improvements in mean Oswestry Disability Index (ODI; 70.6 to 30.1%), VAS pain (7.7 to 1.4), and mean kyphotic angle (11.7 degrees). There was only one case of loss of height in a stabilized VB, one pronounced postoperative hematoma, and no changes in the posterior vertebral wall or adjacent fractures. There were no cases of cement leakage.37
In a 2014 randomized controlled trial comparing BKP to the VBS, the primary outcome was the kyphotic angle measurement on radiographic imaging. Secondary outcomes included radiation exposure time, complications, and cement extravasation. The mean kyphotic angle correction was 4.5 degrees with BKP and 4.7 degrees with VBS. This difference was not significant. There was also no significant difference in radiation exposure times and the rate of cement leakage. It was concluded that, given the fact that VBS was associated with a slightly higher balloon pressures and more material-related complications (one complication in BKP vs. nine complications with VBS), VBS offered no benefit over BKP.38,59
In 2013, Korovessis et al prospectively and randomly compared BKP and KIVA vertebral augmentation for treating osteoporotic VB fractures.60 Although pain, disability and function outcomes were similar in both groups, the authors reported significant restoration of the Gardner angle in patients treated with Kiva, whereas BKP did not meet significance. Lower cement volumes used and decreased extravasation rates were reported for Kiva.
In the same year, Otten et al prospectively compared the Kiva VCF treatment system and the KyphX Systems (Kyphon Inc., Sunnyvale, CA, United States) for BKP specifically evaluating clinical efficacy and safety.61 Patient-reported outcomes were measured preoperatively before device implantation and 6 months after treatment. Back pain severity was evaluated with the standard 10-cm VAS for the Kiva VCF treatment system and a numeric rating scale (0–100, steps of 10) for BKP. Condition-specific functional impairment was evaluated with the ODI score. During surgery, the operation time was recorded. All adverse events, which could be attributed to the treatment and further complications, such as new fractures, were documented. Cement extravasations and their location were confirmed by intraoperative fluoroscopy and postoperative radiography. New fractures were evaluated by radiographic controls. The anterior vertebral body and the mid vertebral heights were measured radiological in the digital system by caliper preoperatively, postoperatively, 3 months, and 6 months postoperatively. The authors described the KIVA system as safe and effective for the treatment of VCFs with pain and function improved as effectively by Kiva as by BKP. Pain was reportedly better controlled by Kiva at the 6-month comparison. The operation time needed to complete the procedure with the Kiva treatment system was shorter, cement volume was lower, and subsequent fractures were less frequent following treatment with KIVA. The authors acknowledged the relatively small study population and 6 months to be only an intermediate follow-up period.
Kiva was shown to be noninferior to kyphoplasty for the treatment of OVCFs based on reduction in pain, improvement in function, and absence of device-related serious adverse events at 12 months in the KAST study. Published in 2015, this large randomized trial of 300 subjects with OVCFs randomly selected to receive either Kiva or BKP had as its primary endpoint a composite of a reduction in pain, improvement in function, and absence of device-related serious adverse events at 12 months. Secondary endpoints included cement usage, cement extravasation, and ALFs. The primary endpoint demonstrated noninferiority of KIVA to BKP and there were no device-related serious adverse events that occurred. Analysis of secondary endpoints revealed statistical superiority of Kiva with respect to cement use and cement extravasation. There was a reduced rate of ALFs in the group treated with Kiva, but this fell just short of statistical significance.62
Given evidence of relative risk reduction rate in ALF with Kiva (31.6% [95% confidence interval (CI): −22.5%, 61.9%]) demonstrated in KAST, Beall et al used clinical data from KAST as well as unit cost data from the published literature to predict a direct medical cost savings of $1,118 per patient and $280,876 per representative U.S. hospital when comparing Kiva to BKP.63
Controversies exist regarding the appropriate imaging and indications, timing, and choice of surgical management of traumatic injuries to the thoracolumbar spine. Sixty-five percent of thoracolumbar fractures occur due to motor vehicle injuries or falls from a height, with the remainder contributed by sports injuries and violence. Since these are high-velocity injuries, thoracolumbar fractures are commonly associated with other injuries like rib fractures, pneumohemothorax, and, rarely, great vessel injuries, hemopericardium, and diaphragmatic rupture.64,65 Seatbelt (Chance) fractures and flexion–distraction injuries are often associated with intra-abdominal visceral injuries.66 A careful history regarding the injury mechanism, pain, and neurological symptoms is essential. Axial, nonradiating back pain of stabbing or aching quality is the most common symptom. Patients with neurological injury may complain of weakness, paresthesia, or anesthesia below the injury level and urinary retention. Thorough inspection of the spine should be performed after a careful log roll maneuver to look for abrasions, tenderness, local kyphosis, and a palpable gap in between spinous processes. Neurological assessment should follow the standard American Spinal Injury Association (ASIA) guidelines (see Chapter 2).
In 2002, using a human cadaveric model, Verlaan et al posited that failure after short-segment pedicle screw fixation for the treatment of vertebral fractures was the result of a redistribution of disk material through the fractured end plate into the VB, causing a decrease in anterior column support. This lack of support could lead to instrument breakage and recurrent kyphosis after removal of the instrumentation. They reported “balloon vertebroplasty” (kyphoplasty) to be a safe and feasible procedure for the restoration of traumatic thoracolumbar vertebral fractures.67
In 2003, the Society of Interventional Radiology (SIR) Standards of Practice Committee published “Quality Improvement Guidelines for Percutaneous Vertebroplasty.” Indications for vertebroplasty at that time included the following: (1) painful primary and secondary OVCFs refractory to medical therapy; (2) painful vertebrae with extensive osteolysis or invasion secondary to benign or malignant tumor (i.e., hemangioma, multiple myeloma, or metastatic disease); and (3) painful vertebral fracture associated with osteonecrosis (Kummel’s disease).68
Since then, many cases of nonosteoporotic vertebral fractures have been treated with vertebral augmentation. In 2004, Chen et al successfully treated a 33-year-old man with L1, L2, and L5 burst fractures with vertebroplasty. The authors proposed the procedure as a useful intervention in select patients with lumbar burst fractures.69 In a 2015 prospective cohort study, Elnoamany demonstrated vertebroplasty to be an effective first-line treatment to decrease pain, increase mobility, and decrease narcotic administration in patients with nonosteoporotic compression fractures.70
In 2014, Korovessis et al retrospectively compared two procedures and two cements: BKP with calcium phosphate (Group A) and KIVA implant with PMMA (Group B). Vertebral augmentation was used to reinforce three-vertebra pedicle screw constructs for A2 and A3 single fresh nonosteoporotic lumbar (L1–L4) fractures in 38 consecutive age- and diagnosis-matched patients. Both groups had diminished pain and improved function as well as improved anterior VB height, segmental kyphosis, and spinal canal encroachment. The Kiva implant/PMMA group had significantly improved posterior VB height; however, short-segment construct restoration had no impact on functional outcomes. The authors advised the use of PMMA in fresh traumatic lumbar fractures.71
More recently, in a case report by Polis et al, percutaneous extrapedicular vertebral augmentation with the SpineJack implant was used to treat a traumatic T8 vertebral fracture in a 15-year-old adolescent boy. CT scans demonstrated an A2.2 (AO/Magerl) fracture of T8. After 6 months of conservative management, severe pain persisted and angle of thoracic kyphosis progressed. The procedure eliminated clinical symptoms and resulted in partial reduction and rebalance of the VCF without limiting motion.72
Benign conditions such as vertebral hemangiomas and giant cell tumors may cause severe intractable pain. More than 30% of patients with advanced cancer have been reported to develop spinal metastases. The rate is higher (70%) in those with cancers of the breast, lung, or prostate.73 Metastatic lesions often cause bone lysis, weaken the vertebrae, and result in painful pathologic fractures with significant morbidity. Multiple myeloma, a cancer that typically starts in the bone marrow, also has a substantial rate of spinal involvement.74,75 Open surgical decompression and instrumented stabilization may not be feasible and failure may lead to catastrophic consequences. Pain management is often inadequate and radiation therapy may be slow to become effective.
In 1987, Nicola and Lins described “a new method, intraoperative retrograde embolization with a methyl methacrylate polymer,” which was injected into a vertebral hemangioma with no further stabilization or radiation required.76
Giant cell tumors of the spine are rare and benign but can be aggressive and exhibit a high local recurrence rate with VB and neural arch destruction. Total spondylectomy with appropriate reconstruction for preservation of spinal integrity is the treatment of choice but is not always feasible. In 1997, Chui reported treatment of a giant cell tumor extending into the spinal canal. Decompressive laminectomy and posterolateral fusion followed by an injection of PMMA into a giant cell tumor resulted in radiological improvement with no tumor recurrence at 7 years.77
In 2003, Fourney et al reported that vertebroplasty and kyphoplasty were safe and feasible to treat painful VCFs in well-selected patients with refractory spinal pain due to myeloma bone disease or metastases in cancer patients. The authors noted at that time that precise indications for the techniques were evolving, with the current North American experience largely limited to osteoporotic compression fractures. This was the only study to date to directly compare vertebroplasty and kyphoplasty in patients with cancer (multiple myeloma and metastatic spinal lesions) and equivalent results in relieving pain were reported. Both procedures provided significant pain relief in a high percentage of patients, and this appeared durable over time.78
In 2007, Shaibani et al reviewed the indications and contraindications of vertebroplasty and kyphoplasty, appropriate patient selection and evaluation, techniques, outcomes, and potential complications when performed for the alleviation of pain for osteolytic tumors of the spine. The authors pointed out that, although both vertebroplasty and kyphoplasty were highly effective in reducing pain from osteoporotic or pathological VCFs and osteolytic tumors, supporting data were based on individual experiences and published case series rather than prospective randomized trials.
Numerous studies have since demonstrated the efficacy and safety of vertebroplasty and kyphoplasty in the treatment of spinal metastasis with rapid, significant, and sustained reductions in pain, disability, and analgesic usage, and improved quality of life.
The Cancer Patient Fracture Evaluation (CAFÉ) trial was the first randomized controlled trial designed to compare the safety and efficacy of BKP with NSM for the treatment of painful VCFs in patients with cancer.79 Patients were from 22 sites in Europe, the United States, Canada, and Australia. Primary outcome measure was back-specific functional status at 1 month. The results supported the beneficial effects and safety of BKP compared with NSM for treating painful VCFs in patients with cancer.
To establish whether the CAFÉ trial findings were consistent with those of other published studies in patients with cancer and VCFs, a systematic review of the literature was performed by Bastian in 2012. A review of 22 published studies (12 prospective, including the CAFÉ trial, and 10 retrospective) extended the findings from the CAFÉ trial and confirmed BKP to be a safe and effective treatment that quickly reduces pain, stabilizes VB height and kyphosis, and improves physical function and quality of life in patients with cancer and painful VCFs.78–100
Astur and Avanzi performed a systematic review to assess the efficacy of kyphoplasty in controlling pain and improving quality of life in oncologic patients with pathologic compression fractures due to spinal metastasis or multiple myeloma. Based on moderate evidence that patients treated with BKP displayed better scores for pain, disability, quality of life, and Karnofsky Performance Status compared with those undergoing the conventional treatment, the study concluded that BKP could be considered an early treatment option for patients with symptomatic neoplastic spinal disease.101
Combination treatment with RFA and vertebral augmentation has been successful in reducing pain and in improving function and quality of life.24–28 Early intervention with RFA and vertebral augmentation may improve the remaining quality of life in cancer patients with pathologic VCFs.25 Although no comparative clinical trials have been performed, there is evidence to show that RFA carried out before percutaneous vertebral augmentation reduces the risk of cement leakage.33
In a retrospective study of 26 patients with 38 vertebral metastases treated between 2005 and 2009, Zheng et al reported image-guided RFA with kyphoplasty to be safe and effective when used with careful consideration of bone cement volume/viscosity, injection location, and temperature to treat thoracolumbar vertebral metastases.30
Wallace et al performed a retrospective review of 72 patients with 110 spinal metastases treated with RFA and vertebral augmentation for pain palliation between April 2012 and July 2014. Eighty-one percent (89/110) of metastases involved the posterior VB, while 45% (49/110) involved the pedicles. Patients reported clinically significant decreased pain scores at both 1- and 4-week follow-ups. No major complications occurred related to RFA and there were no instances of symptomatic cement extravasation. The combination therapy was shown to be a safe and effective therapy for palliation of painful spinal metastases, including tumor involving the posterior VB and/or pedicles.102
Anselmetti et al, in a 2012 case report, described the Kiva system as “a novel and effective minimally invasive treatment option for patients suffering from severe pain due to osteolytic vertebral metastasis.”103 This finding was subsequently supported by data as 40 patients with a painful spine malignancy involving the vertebral wall, not responding to conventional therapies and without surgical indications, underwent vertebral augmentation with the Kiva intravertebral implant for pain palliation. All patients experienced functional improvement and clinically relevant reduction of pain at 1 month. All patients on opiates switched to NSAIDs or no treatment at all. All patients were able to discontinue use of an external orthotic following treatment. Seven of 43 (16.3%) treated vertebrae showed imaging evidence of a bone cement leakage.104
In a controlled, comparative randomized study, kyphoplasty and the KIVA implant provided equally significant pain relief in cancer patients with osteolytic metastasis. Anterior, posterior, and middle VB height ratio and Gardner’s angle improved insignificantly in both groups. Pain and disability improved postoperatively similarly in both groups. Low-viscosity PMMA cement was used and there were no cases of cement leakage in the Kiva group. Safety of both augmentation techniques was demonstrated, even with significant osteolysis.105
LCVH is a benign disease and extremely rare in the lumbar spine of adults.106 Although uncommon, a variety of treatment modalities have been reported for management, including systemic chemotherapy, curettage with and without bone grafting, internal fixation and fusion, intralesional corticosteroid injection, and radiotherapy.106,107 In 1994, Cardon et al reported the first known case of LCVH treated with percutaneous vertebroplasty and described it as a suitable alternative when conservative and open surgical treatments were not feasible, providing pain relief, fracture stabilization, rapid recovery, and early weight bearing.108
In 2002, Rami et al extended the indications for vertebral augmentation when they reported the first case of vertebroplasty used to treat a VCF secondary to osteogenesis imperfecta.109
Vertebral augmentation is a category of minimally invasive procedures that have become central in the treatment of VCFs. Many clinical trials, systematic reviews, and meta-analyses have studied and compared the growing number of vertebral augmentation modalities.43–45 Results confirm significant and durable responses to treatment across a wide range of etiologies, including osteoporosis, trauma, and primary and metastatic cancer. Augmentation relieves pain and, in the case of kyphoplasty and implants, restores vertebral height and corrects kyphotic angulation in select patients, thereby decreasing the risk of future adjacent fractures. Appropriate patient selection is essential for successful outcomes.
As Albers and Latchaw noted in an editorial in Pain Physician:110
“…what of the active 78-year-old woman who suffers an osteoporotic vertebral compression fracture that significantly alters her lifestyle? If she only undergoes medical therapy, she is at risk for isolation, deconditioning, dependency, depression, thrombophlebitis, stroke, and pulmonary diseases such as emboli and infection. The opioids may make her nauseated and constipated so she may not eat. This is not an uncommon story. Morbidity and mortality risks are real life issues, not just statistics.”
Vertebral augmentation has been shown to offer statistically significant benefits to patients with painful and pathologic VCFs associated with osteoporosis, trauma, and malignancy. There have been many innovative advancements since the first vertebroplasty was performed in 1984. Numerous options are now available, each with its own advantages and disadvantages, and criteria for appropriateness. As physicians and clinical investigators, we have a responsibility to limit bias and ensure that appropriate treatments are made available, especially to vulnerable populations.111 The example of the elderly osteoporotic woman is a poignant reminder of our mission to provide our patients with the safest, evidence-based, effective, and affordable health care available.112–114
[1] Harrington KD, Johnston JO, Turner RH, Green DL. The use of methylmethacrylate as an adjunct in the internal fixation of malignant neoplastic fractures. J Bone Joint Surg Am 1972;54(8):1665–1676
[2] McGraw JK, Lippert JA, Minkus KD, Rami PM, Davis TM, Budzik RF. Prospective evaluation of pain relief in 100 patients undergoing percutaneous vertebroplasty: results and follow-up. J Vasc Interv Radiol 2002; 13(9, Pt 1):883–886
[3] Zoarski GH, Snow P, Olan WJ, et al. Percutaneous vertebroplasty for osteoporotic compression fractures: quantitative prospective evaluation of long-term outcomes. J Vasc Interv Radiol 2002;13(2, Pt 1):139–148
[4] Atalay B, Caner H, Gokce C, Altinors N. Kyphoplasty: 2 years of experience in a neurosurgery department. Surg Neurol 2005;64(Suppl 2):S72–S76
[5] Burton AW, Mendel E. Vertebroplasty and kyphoplasty. Pain Physician 2003;6(3):335–341
[6] Kaemmerlen P, Thiesse P, Jonas P, et al. Percutaneous injection of orthopedic cement in metastatic vertebral lesions. N Engl J Med 1989;321(2):121
[7] Tschirhart CE, Finkelstein JA, Whyne CM. Optimization of tumor volume reduction and cement augmentation in percutaneous vertebroplasty for prophylactic treatment of spinal metastases. J Spinal Disord Tech 2006;19(8):584–590
[8] Dickman CA, Fessler RG, MacMillan M, Haid RW. Transpedicular screw-rod fixation of the lumbar spine: operative technique and outcome in 104 cases. J Neurosurg 1992;77(6):860–870
[9] Kim HJ, Yi JM, Cho HG, et al. Comparative study of the treatment outcomes of osteoporotic compression fractures without neurologic injury using a rigid brace, a soft brace, and no brace: a prospective randomized controlled non-inferiority trial. J Bone Joint Surg Am 2014;96(23):1959–1966
[10] Rzewuska M, Ferreira M, McLachlan AJ, Machado GC, Maher CG. The efficacy of conservative treatment of osteoporotic compression fractures on acute pain relief: a systematic review with meta-analysis. Eur Spine J 2015;24(4): 702–714
[11] Cauley JA, Thompson DE, Ensrud KC, Scott JC, Black D. Risk of mortality following clinical fractures. Osteoporos Int 2000;11(7):556–561
[12] Levine SA, Perin LA, Hayes D, Hayes WS. An evidence-based evaluation of percutaneous vertebroplasty. Manag Care 2000;9(3):56–60, 63
[13] Fischgrund JS, Rhyne A, Franke J, et al. Intraosseous basivertebral nerve ablation for the treatment of chronic low back pain: a prospective randomized double-blind sham-controlled multi-center study. Eur Spine J 2018;27(5):1146–1156
[14] Bae H, Hatten HP Jr, Linovitz R, et al. A prospective randomized FDA-IDE trial comparing Cortoss with PMMA for vertebroplasty: a comparative effectiveness research study with 24-month follow-up. Spine 2012;37(7):544–550
[15] Galibert P, Deramond H, Rosat P, Le Gars D. Preliminary note on the treatment of vertebral angioma by percutaneous acrylic vertebroplasty Neurochirurgie 1987;33(2):166–168
[16] Lieberman IH, Dudeney S, Reinhardt MK, Bell G. Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine 2001;26(14):1631–1638
[17] Feltes C, Fountas KN, Machinis T, et al. Immediate and early postoperative pain relief after kyphoplasty without significant restoration of vertebral body height in acute osteoporotic vertebral fractures. Neurosurg Focus 2005;18(3):e5
[18] Benzel E. Physical Principles and Kinematics. Biomechanics of Spine Stabilization. New York, NY: Thieme Publishers; 2001:19–28
[19] Bornemann R, Kabir K, Otten LA, et al. [Radiofrequency kyphoplasty - an innovative method for the treatment of vertebral compression fractures - comparison with conservative treatment]. Z Orthop Unfall 2012;150(4):392–396
[20] Dalton BE, Kohm AC, Miller LE, Block JE, Poser RD. Radiofrequency-targeted vertebral augmentation versus traditional balloon kyphoplasty: radiographic and morphologic outcomes of an ex vivo biomechanical pilot study. Clin Interv Aging 2012;7:525–531
[21] Erdem E, Akdol S, Amole A, Fryar K, Eberle RW. Radiofrequency-targeted vertebral augmentation for the treatment of vertebral compression fractures as a result of multiple myeloma. Spine 2013;38(15):1275–1281
[22] Robertson SC. Percutaneous vertebral augmentation: StabilitiT a new delivery system for vertebral fractures. Acta Neurochir Suppl (Wien) 2011;108: 191–195
[23] Moser FG, Maya MM, Blaszkiewicz L, Scicli A, Miller LE, Block JE. Prospective single-site experience with radiofrequency-targeted vertebral augmentation for osteoporotic vertebral compression fracture. J Osteoporos 2013;2013:791397
[24] Goldberg SN, Gazelle GS, Dawson SL, Rittman WJ, Mueller PR, Rosenthal DI. Tissue ablation with radiofrequency using multiprobe arrays. Acad Radiol 1995;2(8):670–674
[25] Kam NM, Maingard J, Kok HK, et al. Combined vertebral augmentation and radiofrequency ablation in the management of spinal metastases: an update. Curr Treat Options Oncol 2017;18(12):74
[26] Lencioni R, Goletti O, Armillotta N, et al. Radio-frequency thermal ablation of liver metastases with a cooled-tip electrode needle: results of a pilot clinical trial. Eur Radiol 1998;8(7):1205–1211
[27] Miao Y, Ni Y, Yu J, Zhang H, Baert A, Marchal G. An ex vivo study on radiofrequency tissue ablation: increased lesion size by using an “expandable-wet” electrode. Eur Radiol 2001;11(9):1841–1847
[28] Livraghi T, Goldberg SN, Monti F, et al. Saline-enhanced radio-frequency tissue ablation in the treatment of liver metastases. Radiology 1997;202(1): 205–210
[29] Schaefer O, Lohrmann C, Herling M, Uhrmeister P, Langer M. Combined radiofrequency thermal ablation and percutaneous cementoplasty treatment of a pathologic fracture. J Vasc Interv Radiol 2002;13(10):1047–1050
[30] Zheng L, Chen Z, Sun M, et al. A preliminary study of the safety and efficacy of radiofrequency ablation with percutaneous kyphoplasty for thoracolumbar vertebral metastatic tumor treatment. Med Sci Monit 2014;20:556–563
[31] Munk PL, Murphy KJ, Gangi A, Liu DM. Fire and ice: percutaneous ablative therapies and cement injection in management of metastatic disease of the spine. Semin Musculoskelet Radiol 2011;15(2):125–134
[32] Goetz MP, Callstrom MR, Charboneau JW, et al. Percutaneous image-guided radiofrequency ablation of painful metastases involving bone: a multicenter study. J Clin Oncol 2004;22(2):300–306
[33] Kassamali RH, Ganeshan A, Hoey ET, Crowe PM, Douis H, Henderson J. Pain management in spinal metastases: the role of percutaneous vertebral augmentation. Ann Oncol 2011;22(4):782–786
[34] Mooney J, Amburgy J, Self D, Agee B, Pritchard P, Chambers M. Vertebral Height Restoration Following Kyphoplasty. Unpublished Data
[35] Fields AJ, Lee GL, Keaveny TM. Mechanisms of initial endplate failure in the human vertebral body. J Biomech 2010;43(16):3126–3131
[36] Noriega D, Krüger A, Ardura F, et al. Clinical outcome after the use of a new craniocaudal expandable implant for vertebral compression fracture treatment: one year results from a prospective multicentric study. BioMed Res Int;2015:927813
[37] Ender SA, Gradl G, Ender M, Langner S, Merk HR, Kayser R. OsseoFix system for percutaneous stabilization of osteoporotic and tumorous vertebral compression fractures - clinical and radiological results after 12 months. RoFo Fortschr Geb Rontgenstr Nuklearmed 2014;186(4):380–387
[38] Vanni D, Galzio R, Kazakova A, et al. Third-generation percutaneous vertebral augmentation systems. J Spine Surg 2016;2(1):13–20
[39] Hirsch J, Chambers M, Beall DP. Management of Vertebral Fragility Fractures: A Clinical Care Pathway Developed by a Multispecialty Panel Using the RAND/UCLA Appropriateness Method. Unpublished Data
[40] Padovani B, Kasriel O, Brunner P, Peretti-Viton P. Pulmonary embolism caused by acrylic cement: a rare complication of percutaneous vertebroplasty. AJNR Am J Neuroradiol 1999;20(3):375–377
[41] Deramond H, Depriester C, Galibert P, Le Gars D. Percutaneous vertebroplasty with polymethylmethacrylate. Technique, indications, and results. Radiol Clin North Am 1998;36(3):533–546
[42] Mika A, Unnithan VB, Mika P. Differences in thoracic kyphosis and in back muscle strength in women with bone loss due to osteoporosis. Spine 2005;30(2):241–246
[43] Goldstein CL, Chutkan NB, Choma TJ, Orr RD. Management of the Elderly With Vertebral Compression Fractures. Neurosurgery 2015;77(Suppl 4): S33–S45
[44] Hadjipavlou AG, Tzermiadianos MN, Katonis PG, Szpalski M. Percutaneous vertebroplasty and balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures and osteolytic tumours. J Bone Joint Surg Br 2005;87(12):1595–1604
[45] Bouza C, López T, Magro A, Navalpotro L, Amate JM. Efficacy and safety of balloon kyphoplasty in the treatment of vertebral compression fractures: a systematic review. Eur Spine J 2006;15(7):1050–1067
[46] Manchikanti L, Singh V, Caraway DL, Benyamin RM, Hirsch JA. Medicare physician payment systems: impact of 2011 schedule on interventional pain management. Pain Physician 2011;14(1):E5–E33
[47] Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res 2007;22(3):465–475
[48] Suzuki N, Ogikubo O, Hansson T. The course of the acute vertebral body fragility fracture: its effect on pain, disability and quality of life during 12 months. Eur Spine J 2008;17(10):1380–1390
[49] Lapras C, Mottolese C, Deruty R, Lapras C Jr, Remond J, Duquesnel J. Percutaneous injection of methyl-metacrylate in osteoporosis and severe vertebral osteolysis (Galibert’s technic). Ann Chir 1989;43(5):371–376
[50] Jensen ME, Evans AJ, Mathis JM, Kallmes DF, Cloft HJ, Dion JE. Percutaneous polymethylmethacrylate vertebroplasty in the treatment of osteoporotic vertebral body compression fractures: technical aspects. AJNR Am J Neuroradiol 1997;18(10):1897–1904
[51] Kallmes DF, Comstock BA, Heagerty PJ, et al. A randomized trial of vertebroplasty for osteoporotic spinal fractures. N Engl J Med 2009;361:569-579
[52] Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 2001;26(14):1511–1515
[53] Van Meirhaeg, he J, Bastian L, Boonen S, Ranstam J, Tillman JB, Wardlaw D; FREE investigators. A randomized trial of balloon kyphoplasty and nonsurgical management for treating acute vertebral compression fractures: vertebral body kyphosis correction and surgical parameters. Spine 2013;38(12): 971–983
[54] Wardlaw D, Cummings SR, Van Meirhaeghe J, et al. Efficacy and safety of balloon kyphoplasty compared with non-surgical care for vertebral compression fracture (FREE): a randomised controlled trial. Lancet 2009;373(9668): 1016–1024
[55] Beall DP, Chambers MR, Thomas S, et al. Prospective and multicenter evaluation of outcomes for quality of life and activities of daily living for balloon kyphoplasty in the treatment of vertebral compression fractures: the EVOLVE trial. Neurosurgery 2019;84(1):169–178
[56] Krüger A, Oberkircher L, Figiel J, et al. Height restoration of osteoporotic vertebral compression fractures using different intravertebral reduction devices: a cadaveric study. Spine J 2015;15(5):1092–1098
[57] A Prospective, Multicenter, Randomized, Comparative Clinical Study to Compare the Safety and Effectiveness of Two Vertebral Compression Fracture (VCF) Reduction Techniques: the SpineJack and the KyphX Xpander Inflatable Bone Tamp. Identification No NCT02461810; 2015
[58] Interim clinical study report for: Prospective A. Multicenter, Randomized, Comparative Clinical Study to Compare the Safety and Effectiveness of Two Vertebral Compression Fracture (VCF) Reduction Techniques: The SpineJack and the KyphX Xpander Inflatable Bone Tamp. The U.S. National Library of Medicine and Clinical Trials.gov Web site. https://clinicaltrials.gov/ct2/show/NCT02461810. Published May 1, 2018. Accessed June 17, 2018
[59] Werner CM, Osterhoff G, Schlickeiser J, et al. Vertebral body stenting versus kyphoplasty for the treatment of osteoporotic vertebral compression fractures: a randomized trial. J Bone Joint Surg Am 2013;95(7):577–584
[60] Korovessis P, Vardakastanis K, Repantis T, Vitsas V. Balloon kyphoplasty versus KIVA vertebral augmentation: comparison of 2 techniques for osteoporotic vertebral body fractures: a prospective randomized study. Spine 2013;38(4):292–299
[61] Otten LA, Bornemnn R, Jansen TR, et al. Comparison of balloon kyphoplasty with the new Kiva VCF system for the treatment of vertebral compression fractures. Pain Physician 2013;16(5):E505–E512
[62] Tutton SM, Pflugmacher R, Davidian M, Beall DP, Facchini FR, Garfin SR. KAST Study: the Kiva System as a vertebral augmentation treatment-a safety and effectiveness trial: a randomized, noninferiority trial comparing the Kiva System with Balloon Kyphoplasty in treatment of osteoporotic vertebral compression fractures. Spine 2015;40(12):865–875
[63] Beall DP, Olan WJ, Kakad P, Li Q, Hornberger J. Economic analysis of Kiva VCF treatment system compared to balloon kyphoplasty using randomized Kiva Safety and Effectiveness Trial (KAST) data. Pain Physician 2015;18(3): E299–E306
[64] Benson DR, Burkus JK, Montesano PX, Sutherland TB, McLain RF. Unstable thoracolumbar and lumbar burst fractures treated with the AO fixateur interne. J Spinal Disord 1992;5(3):335–343
[65] McLain RF, Sparling E, Benson DR. Early failure of short-segment pedicle instrumentation for thoracolumbar fractures. A preliminary report. J Bone Joint Surg Am 1993;75(2):162–167
[66] Chance GQ. Note on a type of flexion fracture of the spine. Br J Radiol 1948;21(249):452
[67] Verlaan JJ, van Helden WH, Oner FC, Verbout AJ, Dhert WJ. Balloon vertebroplasty with calcium phosphate cement augmentation for direct restoration of traumatic thoracolumbar vertebral fractures. Spine 2002;27(5): 543–548
[68] Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Interventional Radiology clinical practice guidelines. J Vasc Interv Radiol 2003;14(9, Pt 2): S199–S202
[69] Chen JF, Wu CT, Lee ST. Percutaneous vertebroplasty for the treatment of burst fractures. Case report. J Neurosurg Spine 2004;1(2):228–231
[70] Elnoamany H. Percutaneous vertebroplasty: a first line treatment in traumatic non-osteoporotic vertebral compression fractures. Asian Spine J 2015;9(2):178–184
[71] Korovessis P, Vardakastanis K, Repantis T, Vitsas V. Transpedicular vertebral body augmentation reinforced with pedicle screw fixation in fresh traumatic A2 and A3 lumbar fractures: comparison between two devices and two bone cements. Eur J Orthop Surg Traumatol 2014;24(Suppl 1):S183–S191
[72] Polis B, Krawczyk J, Polis L, Nowosławska E. Percutaneous extrapedicular vertebroplasty with expandable intravertebral implant in compression vertebral body fracture in pediatric patient-technical note. Childs Nerv Syst 2016;32(11):2225–2231
[73] Wibmer C, Leithner A, Hofmann G, et al. Survival analysis of 254 patients after manifestation of spinal metastases: evaluation of seven preoperative scoring systems. Spine 2011;36(23):1977–1986
[74] Callander NS, Roodman GD. Myeloma bone disease. Semin Hematol 2001;38(3):276–285
[75] Lecouvet FE, Malghem J, Michaux L, et al. Vertebral compression fractures in multiple myeloma. Part II. Assessment of fracture risk with MR imaging of spinal bone marrow. Radiology 1997;204(1):201–205
[76] Nicola N, Lins E. Vertebral hemangioma: retrograde embolization-stabilization with methyl methacrylate. Surg Neurol 1987;27(5):481–486
[77] Lee CG, Kim SH, Kim DM, Kim SW. Giant cell tumor of upper thoracic spine. J Korean Neurosurg Soc 2014;55(3):167–169
[78] Fourney DR, Schomer DF, Nader R, et al. Percutaneous vertebroplasty and kyphoplasty for painful vertebral body fractures in cancer patients. J Neurosurg 2003;98(1, Suppl):21–30
[79] Berenson J, Pflugmacher R, Jarzem P, et al; Cancer Patient Fracture Evaluation (CAFE) Investigators. Balloon kyphoplasty versus non-surgical fracture management for treatment of painful vertebral body compression fractures in patients with cancer: a multicentre, randomised controlled trial. Lancet Oncol 2011;12(3):225–235
[80] Chen F, Xia YH, Cao WZ, et al. Percutaneous kyphoplasty for the treatment of spinal metastases. Oncol Lett 2016;11(3):1799–1806
[81] Pflugmacher R, Taylor R, Agarwal A, et al. Balloon kyphoplasty in the treatment of metastatic disease of the spine: a 2-year prospective evaluation. Eur Spine J 2008;17(8):1042–1048
[82] Eleraky M, Papanastassiou I, Setzer M, Baaj AA, Tran ND, Vrionis FD. Balloon kyphoplasty in the treatment of metastatic tumors of the upper thoracic spine. J Neurosurg Spine 2011;14(3):372–376
[83] Dalbayrak S, Onen MR, Yilmaz M, Naderi S. Clinical and radiographic results of balloon kyphoplasty for treatment of vertebral body metastases and multiple myelomas. J Clin Neurosci 2010;17(2):219–224
[84] Gerszten PC, Germanwala A, Burton SA, Welch WC, Ozhasoglu C, Vogel WJ. Combination kyphoplasty and spinal radiosurgery: a new treatment paradigm for pathological fractures. J Neurosurg Spine 2005;3(4):296–301
[85] Sandri A, Carbognin G, Regis D, et al. Combined radiofrequency and kyphoplasty in painful osteolytic metastases to vertebral bodies. Radiol Med (Torino) 2010;115(2):261–271
[86] Gerszten PC, Monaco EA III. Complete percutaneous treatment of vertebral body tumors causing spinal canal compromise using a transpedicular cavitation, cement augmentation, and radiosurgical technique. Neurosurg Focus 2009;27(6):E9
[87] Khanna AJ, Reinhardt MK, Togawa D, Lieberman IH. Functional outcomes of kyphoplasty for the treatment of osteoporotic and osteolytic vertebral compression fractures. Osteoporos Int 2006;17(6):817–826
[88] Köse KC, Cebesoy O, Akan B, Altinel L, Dinçer D, Yazar T. Functional results of vertebral augmentation techniques in pathological vertebral fractures of myelomatous patients. J Natl Med Assoc 2006;98(10):1654–1658
[89] Lane JM, Hong R, Koob J, et al. Kyphoplasty enhances function and structural alignment in multiple myeloma. Clin Orthop Relat Res 2004(426):49–53
[90] Huber FX, McArthur N, Tanner M, et al. Kyphoplasty for patients with multiple myeloma is a safe surgical procedure: results from a large patient cohort. Clin Lymphoma Myeloma 2009;9(5):375–380
[91] Zou J, Mei X, Gan M, Yang H. Kyphoplasty for spinal fractures from multiple myeloma. J Surg Oncol 2010;102(1):43–47
[92] Qian Z, Sun Z, Yang H, Gu Y, Chen K, Wu G. Kyphoplasty for the treatment of malignant vertebral compression fractures caused by metastases. J Clin Neurosci 2011;18(6):763–767
[93] Dudeney S, Lieberman IH, Reinhardt MK, Hussein M. Kyphoplasty in the treatment of osteolytic vertebral compression fractures as a result of multiple myeloma. J Clin Oncol 2002;20(9):2382–2387
[94] Astolfi S, Scaramuzzo L, Logroscino CA. A minimally invasive surgical treatment possibility of osteolytic vertebral collapse in multiple myeloma. Eur Spine J 2009;18(Suppl 1):115–121
[95] Cardoso ER, Ashamalla H, Weng L, et al. Percutaneous tumor curettage and interstitial delivery of samarium-153 coupled with kyphoplasty for treatment of vertebral metastases. J Neurosurg Spine 2009;10(4):336–342
[96] Ashamalla H, Cardoso E, Macedon M, et al. Phase I trial of vertebral intracavitary cement and samarium (VICS): novel technique for treatment of painful vertebral metastasis. Int J Radiat Oncol Biol Phys 2009;75(3):836–842
[97] Pflugmacher R, Schulz A, Schroeder RJ, Schaser KD, Klostermann CK, Melcher I. A prospective two-year follow-up of thoracic and lumbar osteolytic vertebral fractures caused by multiple myeloma treated with balloon kyphoplasty. Z Orthop Ihre Grenzgeb 2007;145(1):39–47
[98] Lieberman I, Reinhardt MK. Vertebroplasty and kyphoplasty for osteolytic vertebral collapse. Clin Orthop Relat Res 2003(415, Suppl):S176–S186
[99] Bastian L. Balloon Kyphoplasty in the Treatment of Vertebral Compression Fractures in Cancer Patients. Eur Oncol Haematol 2012;8(3):144–147
[100] Vrionis FD et al., Tech Reg Anesth Pain Manag, 2005;9:39
[101] Astur N, Avanzi O. Balloon kyphoplasty in the treatment of neoplastic spine lesions: a systematic review. Global Spine J 2019;9(3):348–356
[102] Wallace AN, Greenwood TJ, Jennings JW. Radiofrequency ablation and vertebral augmentation for palliation of painful spinal metastases. J Neurooncol 2015;124(1):111–118
[103] Anselmetti GC, Tutton SM, Facchini FR, Miller LE, Block JE. Percutaneous vertebral augmentation for painful osteolytic vertebral metastasis: a case report. Int Med Case Rep J 2012;5:13–17
[104] Anselmetti GC, Manca A, Tutton S, et al. Percutaneous vertebral augmentation assisted by PEEK implant in painful osteolytic vertebral metastasis involving the vertebral wall: experience on 40 patients. Pain Physician 2013;16(4):E397–E404
[105] Korovessis P, Vardakastanis K, Vitsas V, Syrimpeis V. Is Kiva implant advantageous to balloon kyphoplasty in treating osteolytic metastasis to the spine? Comparison of 2 percutaneous minimal invasive spine techniques: a prospective randomized controlled short-term study. Spine 2014;39(4): E231–E239
[106] Cheyne C. Histiocytosis X. J Bone Joint Surg Br 1971;53(3):366–382
[107] Zhong WQ, Jiang L, Ma QJ, et al. Langerhans cell histiocytosis of the atlas in an adult. Eur Spine J 2010;19(1):19–22
[108] Cardon T, Hachulla E, Flipo RM, et al. Percutaneous vertebroplasty with acrylic cement in the treatment of a Langerhans cell vertebral histiocytosis. Clin Rheumatol 1994;13(3):518–521
[109] Rami PM, McGraw JK, Heatwole EV, Boorstein JM. Percutaneous vertebroplasty in the treatment of vertebral body compression fracture secondary to osteogenesis imperfecta. Skeletal Radiol 2002;31(3):162–165
[110] Albers SL, Latchaw RE. The effects of randomized controlled trials on vertebroplasty and kyphoplasty: a square PEG in a round hole. Pain Physician 2013;16(4):E331–E348
[111] Beall DP, Tutton SM, Murphy K, Olan W, Warner C, Test JB. Analysis of Reporting Bias in Vertebral Augmentation. Pain Physician 2017;20(7): E1081–E1090
[112] Wilson DC, Connolly RJ, Zhu Q, et al. An ex vivo biomechanical comparison of a novel vertebral compression fracture treatment system to kyphoplasty. Clin Biomech (Bristol, Avon) 2012;27(4):346–353
[113] Olivarez LM, Dipp JM, Escamilla RF, et al. Vertebral augmentation treatment of painful osteoporotic compression fractures with the Kiva VCF Treatment System. SAS J 2011;5(4):114–119
[114] Korovessis P, Repantis T, Miller LE, Block JE. Initial clinical experience with a novel vertebral augmentation system for treatment of symptomatic vertebral compression fractures: a case series of 26 consecutive patients. BMC Musculoskelet Disord 2011;12:206