Introduction to sport and exercise
Kane Middleton, Andrew Govus, Anthea Clarke and Adrienne Forsyth
You may be reading this book because you are an athlete, you work with athletes, or you would like to work with athletes in the future. To provide appropriate nutrition advice to athletes, it is important that you understand the practical and physiological impacts of physical activity, exercise and sport. This chapter will provide you with an overview of key concepts related to sport, exercise and performance, and outline the body’s responses and adaptations to exercise.
LEARNING OUTCOMES
Upon completion of this chapter you will be able to:
• compare and contrast physical activity, exercise and sport
• describe different types of sport and exercise, and relate these to differing physiological processes and adaptations
• measure exercise performance and intensity
• describe the principles of exercise prescription
• describe muscle types and actions
• explain the body’s physiological response and chronic adaptations to exercise
• outline how the body recovers from exercise.
PHYSICAL ACTIVITY, EXERCISE AND SPORT
Although often used interchangeably, there is a distinct conceptual difference between physical activity, exercise and sport. Physical activity is any movement that we perform that expends energy. The simplest categorisation of physical activity is based on proportioning activities in daily life—namely, sleep, work and leisure. The energy expenditure during sleep is obviously very small, whereas the energy expenditure during work would depend on the type of employment. A nurse who spends a lot of time walking around a hospital ward would expend much more energy than an office worker who spends the majority of the work day sitting down. In regard to leisure time physical activity, humans typically perform this incidentally (such as walking to the shops), in the household (such as gardening), or during exercise and sport.
Physical activity
Any bodily movement produced by skeletal muscles that results in energy expenditure.
Exercise
Physical activity that is planned, structured, repetitive and purposeful with the aim to improve or maintain one or more components of physical fitness.
Exercise is a subcategory of physical activity. Although it still includes body movements that result in energy expenditure, it is different to physical activity in that it is planned, structured and repetitive. The purpose of exercise is to improve or maintain components of physical fitness, including:
• aerobic and anaerobic capacity (described later in this chapter)
• muscular endurance, strength and power
• body composition (see Chapter 13)
• flexibility
• balance.
Aerobic capacity
The ability of the body to take in and distribute oxygen to the working muscles during exercise.
Accredited Exercise Scientist
A specialist in the assessment, design and delivery of exercise and physical activity programs (Exercise and Sports Science Australia 2018).
Examples of structured exercise include a running program to promote fat loss and/or increase aerobic capacity, a conditioning program to increase muscular strength or a stretching program to increase joint flexibility. If we take the example of a conditioning program, for it to be most effective it would be planned before beginning, ideally by an Accredited Exercise Scientist. The plan would incorporate purposeful exercise and progress the exerciser through mental stages of readiness to change (see Chapter 8 for the transtheoretical model of change). The program would be delivered in a structured, repetitive manner, taking into account the concepts of periodisation and progressive overload (this is discussed in more detail later in this chapter under Chronic Adaptations to Exercise).
It has been difficult to develop a universally approved definition of sport. Currently, the most accepted definition is that of the Global Association of International Sports Federations, which states that the following criteria must be met in order for a sport to become a member of the Association (Global Association of International Sports Federations 2012):
• The sport proposed should include an element of competition.
• The sport should not rely on any element of ‘luck’ specifically integrated into the sport.
• The sport should not be judged to pose an undue risk to the health and safety of its athletes or participants.
• The sport proposed should in no way be harmful to any living creature.
• The sport should not rely on equipment that is provided by a single supplier.
Sport
‘A human activity capable of achieving a result requiring physical exertion and/ or physical skill which, by its nature and organisation, is competitive and is generally accepted as being a sport’ (Australian Sports Commission 2018).
In Australia, the Australian Sports Commission currently (at time of print) recognises 95 national sporting organisations. Their definition of sport focuses more on physical effort and skill that includes a competitive element.
TYPES OF SPORT
Due to the large variety of sports in existence, the Global Association of International Sports Federations has also developed categories of sports. These categories are based on the primary (not exclusive) type of activities that make up the sport. The list of categories and examples of sports in those categories can be found in Table 1.1. Note that many sports may belong to multiple categories.
Table 1.1. Categories of sport
| Category | Examples of sports |
| Physical | Football, Basketball, Athletics |
| Mind | Chess, Draughts, eSports |
| Motorised | Formula One, Motorcycling |
| Coordination | Lawn Bowls, Billiards, Shooting |
| Animal-supported | Horse Racing, Equestrian, Polo |
Figure 1.1. Endurance–power continuum of sport
Primarily physical sports are by far the most common and best known, and it could be strongly argued that nutrition is more important in these types of sports. Whether a sport is individual or team-based, the physical requirements of that sport will lie somewhere on an endurance–power continuum (Figure 1.1). Sports such as marathon running and triathlon are on the endurance end of the continuum, where repeated movement cycles are performed over a sustained period of time. In contrast, power lifting and track and field throws are on the power end of the continuum, where a single movement is performed at high intensity and often at high speed. To complicate this, sports often have different requirements for the disciplines within the sport or playing position within a team. In track and field, a 100-metre sprinter has a different physical requirement than a 10,000-metre runner. In American Football, a defensive tackle is usually the biggest and strongest player on the team, whereas running backs tend to be smaller but fast and agile.
Aerobic
Exercise at an intensity that is low enough to allow the body’s need for oxygen (to break down macronutrients) to be matched to the oxygen supply available.
Anaerobic
Exercise at an intensity where the body’s demand for oxygen is greater than the oxygen supply available, therefore relying on anaerobic metabolism and the production of lactate.
Sporting activities are also sometimes categorised as aerobic or anaerobic. Endurance sports, which are performed at a somewhat lower intensity over a long period of time, are predominantly aerobic, meaning that the body is able to breathe in enough oxygen to support metabolic processes and fuel muscle activity. High-energy bursts of activity in power sports are usually performed at such a high intensity that athletes are unable to breathe in enough oxygen and rely on anaerobic metabolic processes to fuel the muscles.
LEVELS OF SPORTS PARTICIPATION AND COMPETITION
Levels of sports participation can be thought of as a pyramid (Figure 1.2) that generally represents the inverse relationship between competition level and participation rate. The foundation level of competitive sport most often occurs at a young age, when people are first introduced to a sport. In Australia and New Zealand, this would typically occur during physical education classes. Sporting organisations and recreation centres also contribute to the foundation level by offering introductory programs, such as the AFL Auskick (Australian football) or in2CRICKET (cricket) programs that focus on the fundamental motor skills of those sports.
Once someone advances from an introduction to a sport to regularly engaging with that sport, they enter the participation level. As a large number of people are introduced to a variety of sports at the foundation level, there is an inevitable decline in numbers reaching the participation level. The engagement at this level is generally recreational in nature, such as social sport; although competition is present, i.e. there is a winner and a loser, the main aim of participating is enjoying the activity itself rather than the final outcome.
The aim of competition changes from enjoyment to winning at the performance level. Whereas the skill level of people at the participation level is not overly important, performance athletes are often selected in teams or for competition based on, as the name suggests, their performance. They will often represent a club or team in these competitions, which are generally administered by official sporting organisations with standard rules and regulations. Representative sport will generally start in high school and continue through to adult competition. The critical development period from 18 to 23 years of age coincides with tertiary education for many high-achieving athletes. In Australia and New Zealand, the progress of these athletes is supported by national sporting organisations and state-based academies and institutes of sport. This stage is different around the world, with a contrasting system in the United States of America. The United States has established a college-based sports system, regulated by organisations such as the National Collegiate Athletic Association, and organised and funded by the colleges themselves.
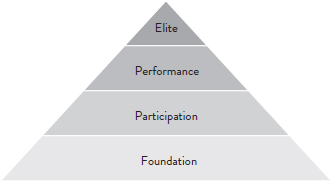
Figure 1.2. Levels of sports participation
The peak of sports participation is the elite level. This is very similar to the performance level but only includes the very best representatives of a sport, meaning that this level has the fewest athletes of all the levels of the sports participation pyramid. The delineation of elite athletes from other high-performing athletes is difficult, but elite athletes often compete at the national or international level. Although the Olympic Games is still the pinnacle of elite amateur sport around the world, the evolution of elite sport has coincided with growing professionalism due to the resources dedicated to preparation, training and competition. The large investments in professional sport make winning ‘big business’ and, given that the performance differential between athletes at the elite level is very small, nutritional interventions such as supplementation can have a large impact on performance and competition outcomes (see Chapter 12 for more information on this topic).
MONITORING EXERCISE
Cardiorespiratory exercise
Whole-body, dynamic exercise that taxes predominantly the cardiovascular and respiratory systems, such as running, cycling and swimming.
Resistance exercise
Exercise that predominantly involves the musculoskeletal system.
Skeletal muscle
Voluntary muscle attached to bones that move a part of the skeleton when stimulated with a nerve impulse.
Biomechanical
Pertaining to the mechanical nature of the body’s biological processes, such as movements of the skeleton and muscles.
Exercise can be categorised into two main types: cardiorespiratory exercise (involving the cardiovascular and respiratory system) and resistance exercise (predominantly involving the musculoskeletal system). Whereas cardiorespiratory exercise involves predominantly whole-body, dynamic exercise involving a large skeletal muscle mass, resistance exercise aims to develop physiological, neurological and biomechanical properties of skeletal muscle. Cardiorespiratory exercise is predominantly aerobic, while resistance exercise is predominantly anaerobic.
The intensity of cardiorespiratory and resistance exercise can be expressed in either absolute or relative terms. Absolute exercise intensity refers to the total amount of energy expended (expressed in kilojoules or kilocalories) to produce mechanical work, in the form of skeletal muscle contraction. Note that in Australia we follow the internationally agreed decimal system of measurement (metric system), which will be used in this textbook (1 calorie = 4.18 kilojoules). See Chapter 2 for a more detailed discussion of energy, work and power.
A unit of energy equal to 1000 joules. A joule is a unit of energy equal to the amount of work done by a force of 1 Newton (the force required to accelerate 1 kilogram of mass at the rate of 1 metre per second squared in the direction of the applied force) to move an object 1 metre.
Kilocalories
A unit of energy equal to 1000 calories. A calorie is the energy required to increase the temperature of 1 gram of water by 1°C.
Absolute exercise intensity can be expressed in metabolic equivalents (METs), which describe exercise intensity as a multiple of the amount of energy required by the body at rest. One MET is approximately equivalent to an oxygen uptake of 3.5 mL.kg–1 · min–1, although the exact value will vary between individuals and should be measured directly (see Chapter 2 for more information about measurement of energy expenditure). For example, the oxygen consumption for a 70 kilogram male exercising at an absolute exercise intensity of five METs for 30 minutes would be calculated as:
Oxygen consumption ( O2) = 5 × 3.5 mL ∙ kg–1 ∙ min–1 = 17.5 mL ∙ kg–1 ∙ min–1 O2
O2) = 5 × 3.5 mL ∙ kg–1 ∙ min–1 = 17.5 mL ∙ kg–1 ∙ min–1 O2
Oxygen consumption (O2) = 17.5 mL ∙ kg–1 ∙ min–1 × 70 kg = 1225 mL ∙ min–1 O2
Oxygen consumption (O2) = 1225 mL ∙ min–1 × 30 min = 36750 mL O2

From the estimated oxygen consumption we can calculate the energy expenditure during exercise, since each litre of oxygen yields ~5 kcal (see Chapter 2 for a detailed explanation). Therefore, the estimated energy expenditure for the example above is:
Energy expenditure (kcal) = 36.75 L O2 × 5 kcal = 183.75 kcal
To convert kilocalories to kilojoules (kJ) = 183.75 kcal × 4.18 kj/kcal = ~768 kj
Maximum aerobic power (VO2max)
The maximum amount of oxygen an individual can take up per minute during dynamic exercise using large muscle groups.
Oxygen reserve (%VO2R)
The difference between resting oxygen consumption and maximal oxygen consumption.
In comparison, relative exercise intensity refers to exercise that is expressed relative to an individual’s maximal capacity for a given task or activity. The intensity of cardiorespiratory exercise is commonly expressed as a percentage of an individual’s maximum aerobic power (O2max), heart rate (HRmax) or rating of perceived exertion (RPE).
The most accurate method of monitoring the intensity of submaximal exercise is by expressing the exercise intensity as a percentage of the individual’s maximal oxygen uptake (%O2max) or oxygen reserve (%O2R).
Per cent maximal oxygen uptake (%O2max) = O2max × intensity (%)
Per cent oxygen reserve (%O2R) = [O2max – O2rest] × intensity (%)] + O2rest
A linear relationship exists between heart rate and oxygen uptake during incremental exercise (Figure 1.3), so an individual’s heart rate, rather than their oxygen uptake, is more regularly used to monitor their exercise intensity, since heart rate monitoring is both cheaper and less invasive than measuring oxygen consumption.
Several different equations exist to estimate an individual’s HRmax and the equation used should be appropriate for the population being measured. One common formula is that of Gellish et al. (2007):
Maximum heart rate (HRmax) = 207 – [0.70 × Age (years)]
Per cent heart rate reserve (%HRR)
Heart rate reserve multiplied by the desired percentage of exercise intensity.
Another method of estimating exercise intensity using heart rate methods is by calculating the percentage of heart rate reserve (%HRR). Heart rate reserve is often known as the Karvonen formula (Karvonen 1957). The HRR and %HRR are calculated using the equations below.
Heart rate reserve (HRR) = (HRmax – HRrest) + HRrest
Per cent heart rate reserve (%HRR) = [(HRmax – HRrest) × intensity (%)] + HRrest
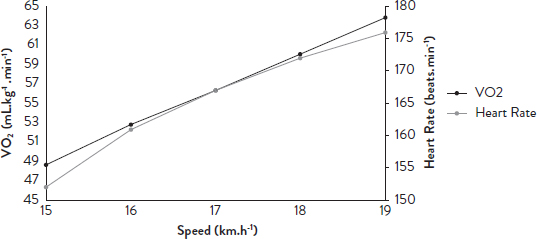
Figure 1.3. The relationship between oxygen uptake ( O2) and heart rate during treadmill running
The advantages and disadvantages of using heart rate-based methods to monitor the intensity of cardiorespiratory exercise are summarised in Table 1.2.
In addition to measuring oxygen consumption or heart rate, exercise intensity can be expressed as an individual’s current level of effort or exertion, relative to their perceived maximal exertion. The most common method of measuring an individual’s perceptual response to exercise is by using visual analogue scales such as Borg’s 6–20 scale of perceived exertion (Borg 1982) (Table 1.3) or the Foster’s Category Ratio (CR) 10 scale (Foster et al. 2001) (Table 1.4).
In comparison, resistance exercise may be expressed relative to the maximum amount of mass that a particular muscle group can lift successfully for one repetition, which is known as the one repetition maximum (1 RM), or by using perceptual methods such as the RPE. Exercise intensity for resistance training can then be expressed as a percentage of an individual’s 1 RM. For example, an athlete with a 1 RM for the back-squat exercise of 120 kilograms wishes to develop their muscular strength, and so should lift ~85 per cent of their 1 RM in training. The mass they should lift in training can be calculated as follows:
85% 1 RM = 0.85 × 120 kg = 102 kg
Exercise intensity is stratified into categories related to the level of challenge experienced. This will vary from person to person depending on the individual’s maximal physical capacity. The intensity of the stimulus applied during a training session (for example, the amount of weight lifted, or the speed of running) determines the physiological and mechanical loads placed upon the body during training and, consequently, the physiological adaptations that occur. Consistent with the Principle of Progressive Overload (discussed in more detail later in this chapter), the exercise intensity is one exercise prescription variable that can be manipulated to overload the body. Physiological and perceptual methods of monitoring exercise intensity are summarised in Table 1.5.
Table 1.2. Advantages and disadvantages of measuring exercise intensity using heart rate monitoring
| Advantages | Disadvantages |
| Objective measurement | Need to know (or accurately estimate) maximum heart rate for effective exercise prescription |
| Easy to use in daily training | Average heart rate for a workout can be misleading if exercise intensity varies within a session |
| Heart rate and blood lactate response remain stable over time | Limited usefulness for very high-intensity intervals performed above the maximum heart rate |
| Useful to gauge perceptual methods of measuring exercise intensity such as RPE | The relationship between heart rate and workload is influenced by fatigue, heat, humidity and dehydration within a training session |
Table 1.3. The Borg 6–20 scale of perceived exertion
| Rating | Descriptor |
| 6 | No exertion at all |
| 7 | Extremely light |
| 8 | — |
| 9 | Very light |
| 10 | — |
| 11 | Light |
| 12 | — |
| 13 | Somewhat hard |
| 14 | — |
| 15 | Heavy |
| 16 | — |
| 17 | Very hard |
| 18 | — |
| 19 | Extremely hard |
| 20 | Maximal |
ACUTE RESPONSES TO CARDIORESPIRATORY EXERCISE
Acute exercise stresses several of the body’s physiological systems, including the cardiovascular, respiratory and musculoskeletal systems. In response to cardiorespiratory exercise, the cardiovascular system increases oxygen delivery to the skeletal muscle by increasing cardiac output as well as redistributing blood flow from non-essential organs. Furthermore, the skeletal muscle tissue extracts more oxygen from the blood to support the metabolic activities needed to fuel skeletal muscle activity.
Table 1.4. The Foster Category Ratio scale
| Rating | Descriptor |
| 0 | Rest |
| 1 | Very, very easy |
| 2 | Easy |
| 3 | Moderate |
| 4 | Somewhat hard |
| 5 | Hard |
| 6 | — |
| 7 | Very hard |
| 8 | — |
| 9 | — |
| 10 | Maximal |
| Intensity | HRR/ 02R (%) 02R (%) |
02max (%) |
HRmax (%) | RPE (6–20) (Borg 1982) |
| Very light | <30 | 37 | <57 | <9 |
| Light | 30–39 | 37–45 | 57–63 | 9–11 |
| Moderate | 40–59 | 46–63 | 64–76 | 12–13 |
| Vigorous | 60–89 | 64–90 | 77–95 | 14–17 |
| Near maximal | ≥90 | ≥91 | >96 | >17 |
Source: Adapted from American College of Sports Medicine 2010.
During steady-rate exercise at low intensities, pulmonary ventilation increases by virtue of an increase in breathing frequency and tidal volume. In contrast, hyperventilation (over-breathing) occurs during maximal exercise intensities, in order to buffer the acidic carbon dioxide that accumulates in the blood in response to anaerobic exercise. Common values for selected cardiorespiratory parameters at resting, submaximal and maximal exercise are presented in Table 1.6.
The product of an individual’s heart rate (the amount of times the heart contracts per minute) and stroke volume (the volume of blood ejected from the heart per minute).
Steady-state exercise
Exercise performed at an intensity whereby the body’s physiological systems are maintained at a relatively constant value.
Pulmonary ventilation
The product of an individual’s breathing frequency (the amount of breaths per minute) and tidal volume (the volume of gas inhaled per minute).
Maximal exercise
Exercise performed at an intensity equal to an individual’s maximum capacity for the desired activity.
Submaximal exercise
Exercise performed at an intensity below an individual’s maximum capacity for the desired activity.
Metabolism
Chemical processes that occur within a living organism to maintain life.
Metabolic acidosis
A decrease in blood pH below the body’s normal pH of ~7.37–7.42.
Physiological conditions
The natural internal and/or external environmental conditions within which the body’s physiological systems operate.
Buffer
A chemical system within the body that aims to counteract a change in the blood pH, defined by the blood [H+].
Buffers and maintaining acid–base balance
It is important to maintain acid–base balance during acute exercise to delay the onset of fatigue. Metabolic acidosis can impair energy substrate metabolism and result in a reduction in the desired power output. Under physiological conditions, lactic acid produced immediately dissociates into lactate (C3H5O3-) and hydrogen ions (H+) in solution. Hydrogen ions dissolved in a solution are acidic, and therefore decrease the blood pH. The pH scale, a measure of the relative acidity of a solution, ranges from 0 (extremely strong acid, such as hydrochloric acid) to 14 (extremely strong base, such as sodium hydroxide), with a pH of 7 indicating a neutral solution (such as water). Since many of the body’s systems operate within an optimal pH range, the body counteracts increases in blood acidity by neutralising the rise in [H+] using a combination of chemical (bicarbonate and phosphate), physiological (protein) and respiratory buffers to maintain blood pH within physiologic limits (pH = ~7.37–7.42).
The main method of controlling acid–base balance during acute exercise is by expiring (breathing out) excess CO2 that accumulates within the blood. As the blood pH decreases (i.e. becomes more acidic), the respiratory frequency increases and raises the blood pH by expelling excess CO2. In addition to the respiratory buffer, hydrogen carbonate ions (HCO3–) in the blood neutralise H+, forming carbonic acid (H2CO3), which dissociates in the blood to water (H2O) and CO2, with the excess CO2 expired. This process is summarised in the reversible chemical reaction below.
H+ + HCO3– ↔ H2CO3 ↔ H2O + CO2
Blood pH is also maintained by the buffering effects of proteins in the blood and surrounding cells, which also act as proton acceptors for H+. Finally, phosphate ions (PO4–) act as proton acceptors in a similar way to HCO3–.
Table 1.6. Typical values for selected cardiorespiratory parameters during rest, submaximal and maximal exercise for a healthy adult male
| Physiological Parameter | Rest | Submaximal Exercise | Maximal Exercise |
| Cardiac output | 5 L/min | 10–15 L/min | 20–45 L/min |
| Stroke volume | 50–80 mL/beat | 110–130 mL/beat | 110–130 mL/beat |
| Heart rate | 50–70 beats/min | 70–180 beats/min | 180–220 beats/min |
| Skeletal muscle blood flow | 15–20% | 80–90% | 80–90% |
| Systolic blood pressure | 100–120 mmHg | 120–180 mmHg | 180–200 mmHg |
| Minute ventilation | 5–6 L/min | 35–150 L/min | 150–200 L/min |
| Breath frequency | 10–15 breaths/min | 15–35 breaths/min | 35–50 breaths/min |
| Tidal volume | 0.5 L/min | 0.5–3.0 L/min | 3.0–5.0 L/min |
Proton
A positively charged subatomic particle with a positive electric charge.
ACUTE RESPONSES TO MUSCULOSKELETAL EXERCISE
The musculoskeletal system also undergoes several different physiological responses during acute exercise to allow it to produce mechanical work. Such responses to acute exercise include an increase in motor unit and muscle fibre recruitment, muscle temperature and muscle enzyme activity.
Motor unit
A motor neuron (nerve cell) and the skeletal muscle fibres that it innervates (services).
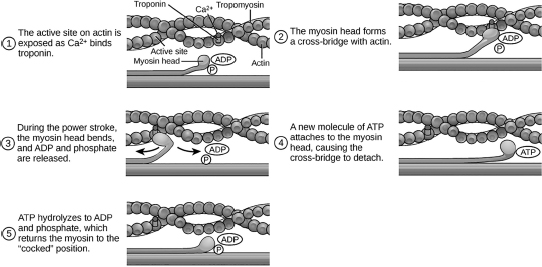
Acute cardiorespiratory and/or resistance exercise requires repeated skeletal muscle action to complete the desired physical task. Skeletal muscle actions rely on the actions of smaller fibres (called myofilaments) consisting of myosin (a thick myofilament) and actin (a thin myofilament). Myosin and actin slide past each other during skeletal muscle actions; hence, the process underlying skeletal muscle action is known as the sliding filament theory.
When the external resistance is low, such as during low-intensity cardiorespiratory or resistance exercise, the body recruits predominantly slow-twitch (type I) skeletal muscle fibres, which are highly fatigue resistant but have low force-generation characteristics. In contrast, high external loads, such as those encountered during maximal strength training, activate fast-twitch (type II) skeletal muscle fibres, which are more susceptible to fatigue but are able to generate higher forces (see Table 1.7 for a comparison between the physiological characteristics of the different skeletal muscle fibre types). Collectively, slow- and fast-twitch skeletal muscle fibres produce the movements required during an acute exercise bout.
Figure 1.4. The sliding filament theory of skeletal muscle contraction
Source: Retrieved from www.oercommons.org/courseware/module/15136/overview.
In addition, acute exercise may involve three different types of skeletal muscle actions; concentric, eccentric and isometric. Concentric muscle actions involve the shortening of skeletal muscle fibres and occur when the contractile force of the muscle is greater than the resistance force, whereas eccentric muscle actions involve the lengthening of skeletal muscle fibres and occur when the contractile force is less than the resistive force. The skeletal muscle length remains constant during an isometric muscle action, which occurs when the contractile and resistive forces are equal.
PRESCRIBING PHYSICAL ACTIVITY AND EXERCISE
Due to the strong association between physical activity and health outcomes such as chronic disease and obesity, the Australian Department of Health has developed age-specific guidelines for physical activity (Table 1.8). These guidelines are intended to help facilitate positive health outcomes for all Australians.
Whether you are undertaking exercise for general health, or to improve your competitive performance, when exercise sessions are repeated over multiple weeks and months chronic adaptations to exercise begin to occur. These chronic adaptations occur as a result of the specific loading and progression of exercise sessions and can be specific aerobic, anaerobic or strength adaptations, depending on the goals of the individual. One of the simplest and most common methods to monitor and progress your training program is by using the FITT (frequency, intensity, time, and type) Principle. An example of how you may target different exercise goals using the FITT Principle is provided in Table 1.9. By changing one or more of the elements within the FITT Principle, you can continue to overload the body to promote adaptations.
Table 1.7. A comparison of the physiological, neurological and biomechanical properties of different skeletal muscle fibre types
| Characteristic | Type I | Type IIa | Type IIx |
| Colour | Red | Red | White |
| Fibre size | Small | Medium | Large |
| Motor neuron size | Small | Large | Very large |
| Twitch velocity | Slow | Medium | Fast |
| Force production | Low | Medium | High |
| Phosphate resynthesis rate | Fast | Medium | Slow |
| Oxidative enzyme concentration | High | Medium | Low |
| Glycolytic enzyme concentration | Low | Medium | High |
| Major metabolic fuel source | Triacylglycerols | Phosphocreatine/ glycogen | Phosphocreatine/ glycogen |
| Mitochondrial density | High | High | Low |
| Capillary density | High | Medium | Low |
| Myoglobin content | High | Medium | Low |
It is important to adjust training loads as an individual progresses through an exercise program to ensure adequate training stress is applied; this is termed progressive overload. Following an initial exercise stimulus, the body is transiently fatigued due to acute changes, and subsequently recovers and adapts to that initial stimulus. This results in the body having a new baseline level of performance, which therefore requires a greater exercise stimulus to promote the next adaptation. Figure 1.5 outlines the effect of subsequent exercise sessions on improving the performance level of the individual. If exercise is not followed by sufficient rest, it may result in the individual becoming over-trained. Conversely, if too much time follows between exercise bouts, the adaptations return to the initial baseline levels without further adaptation occurring. In this sense, the periodisation of training becomes important to ensure a sufficient balance between exercise stimulus and recovery.
Progressive overload
The continued incremental increase in training demand (duration or intensity) required to elicit an adaptive response.
Table 1.8. Australia’s Physical Activity Guidelines
| Age Range | Guideline |
| Birth–5 years | Infants (Birth–1 Year): 30 minutes of ‘tummy time’ per day Toddlers (1–2 Years): At least 180 minutes of activity including energetic play Pre-schoolers (3–5 Years): At least 180 minutes of activity with at least 60 minutes of energetic play |
| 5–12 Years | At least 60 minutes of moderate-to-vigorous physical activity per day |
| 13–17 Years | At least 60 minutes of moderate-to-vigorous physical activity per day |
| 18–64 Years | 150 to 300 minutes of moderate physical activity or 75 to 150 minutes of vigorous physical activity per week |
| Older Adults | At least 30 minutes of moderate physical activity per day |
Source: Adapted from Department of Health 2017.
Table 1.9. Example application of the FITT principle for targeted physiological adaptation
| Cardiovascular Endurance | Muscular Endurance | Muscular Strength | |
Frequency (How often the exercise is performed) |
3–5 times per week | 3–5 times per week | 3 times per week |
Intensity (How hard the exercise is) |
60–90% max heart rate | 12+ repetitions, 2–4 sets | 3–7 repetitions, 3–5 sets |
Time (The duration of each individual exercise session) |
>30 min | 30–60 min | 15–60 min |
Type (The kind of activity completed) |
Running Swimming Bicycling Walking | Free weights Circuit training Body-weight exercises | Free weights Resistance machines |
Source: Adapted from ThePhysicalEducator.com.
The timing of exercise bouts to ensure sufficient exercise stimulus and recovery is provided to elicit the greatest response and adaptation.
CHRONIC ADAPTATIONS TO EXERCISE
Adaptations that occur as a response to exercise are specific to the training stimulus applied and include changes to the cardiovascular, metabolic, respiratory and muscular systems. Regular aerobic exercise, for example, enhances the ability of the body to use fat as fuel during exercise through increased transport of free fatty acids, fat oxidation and mitochondrial biogenesis (increase in the number and mass of mitochondria), to name a few, and elicits the development of type I muscle fibres. All of these adaptations lead to an improved capacity to complete longer duration or higher intensity exercise while remaining within an aerobic state. Exercise and prolonged training also stimulate the release of a number of hormones, including testosterone and growth hormone, which promote an anabolic effect on the body. These hormones increase protein synthesis and cell growth, leading to an increase in lean muscle mass and decreased fat mass. This chronic adaptation of an individual’s body composition, which increases the amount of active tissue in the body, also leads to an increased metabolic rate for the individual. Growth hormone also stimulates cartilage formation and skeletal growth, which encourages bone formation. The mechanical loading of exercise, such as during foot strike while running, also elicits the remodelling of bone to adapt to the load under which it is placed; this is known as Wolff ’s Law. As is the case with all chronic adaptations to training, when the exercise stimulus is removed these adaptations revert back to original baseline levels.
Oxidation
Part of a chemical reaction that results in the loss of electrons. During fat oxidation, triglycerides are broken down into three fatty acid chains and glycerol.
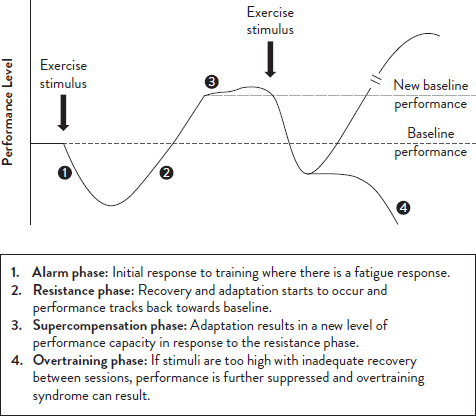
Figure 1.5. The general adaptive syndrome and its application to periodisation
Source: Adapted from National Strength and Conditioning Association 2011.
An anabolic effect refers to the ‘building up’ and repair of tissues through increased protein synthesis and cell growth. It is the opposite of ‘catabolism’, which refers to the breakdown of molecules.
Wolff’s Law
Bone in a healthy person will adapt to the loads under which it is placed. In this sense, an exercise stimulus results in bone remodelling that makes the bone stronger to resist that sort of loading.
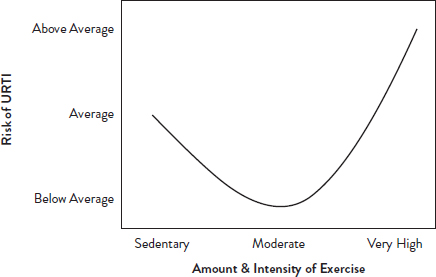
Along with the more commonly discussed changes to our cardiovascular, metabolic and muscular systems, exercise also affects our immune system. Following acute exercise, there is a reduction in white blood cell numbers and activity due to circulating hormones (catecholamines, growth hormone, cortisol, testosterone) and as a result of local inflammation. This acute-phase response can last from two to 72 hours post-exercise. The extent of these changes is influenced by the intensity and duration of exercise, with longer duration and higher intensity exercise eliciting a greater immunosuppressive response. The immune system can also be affected by travel and when in a team sport environment. Specific hygiene practices should be in place to reduce the duration and severity of illness, as well as to limit the spread of infection during periods of exercise. Over a period of time, there appears to be a J-shaped relationship between exercise and immune function (Figure 1.6). While sedentary behaviour or excessive/strenuous exercise can result in immune dysfunction and greater risk of illness, moderate amounts of exercise exert a protective effect on our immune system. Nutrition is also thought to play a role in maintaining immune function, through the adequate intake of specific micronutrients (for example, iron, zinc, vitamins A, E and B12) and sufficient carbohydrate availability during exercise bouts to help limit the rise in the stress hormone cortisol.
RECOVERING FROM EXERCISE
In order for the body to adapt to the exercise stimulus, sufficient recovery is required following each bout of exercise (short-term recovery) and training block (long-term recovery). It is during this recovery period that the body is able to replenish energy stores and repair damaged tissue to allow the body to develop and adapt in response to the stimulus. The simplest ways to recover from exercise are to have a rest day from training and to get good-quality sleep. Other common recovery methods include cold or contrast water immersion, compression garments, foam rolling and massage. Nutrition plays a big part in the recovery process through the sufficient intake and timing of key macro- and micronutrients. The nutritional recovery requirements are dependent on the demands of the activity and so will vary between endurance and power-based sports.
Source: Adapted from Neiman 1994.
Amino acids
The building blocks of protein, composed of a central carbon to which is attached a hydrogen (H), an amino group (NH2), a carboxylic acid group (COOH), and a side chain group.
As an example, endurance sports such as a marathon or game of Australian football will have key recovery strategies focusing on rehydration and the replenishment of carbohydrates, whereas power-based sports such as weightlifting have a greater focus on increasing protein-building amino acids to assist in muscle repair and growth following training. You can read more about these requirements in Chapters 15 and 16.
SUMMARY AND KEY MESSAGES
After reading this chapter, you should understand the importance of physical activity for human health. You will have an understanding of the types of sport played in Australia and New Zealand, and be familiar with physiological adaptations to sport and exercise. You will understand how exercise is measured and monitored, and be familiar with the principles of exercise prescription.
Key messages
• Physical activity is vital for our health and wellbeing, and our daily physical activity levels can be maximised through participation in intentional exercise and recreational or competitive sport.
• Exercise can be classed as endurance or power, aerobic or anaerobic, and cardiorespiratory or musculoskeletal.
• METs are used to describe the amount of work performed during exercise based on the amount of oxygen consumed relative to rest. The energy expended can be expressed using kilojoules or kilocalories.
• The intensity of exercise is often estimated using heart rate or perceived exertion.
• The body responds to cardiorespiratory exercise by increasing the blood flow to the muscle, increasing the volume of air inhaled, and increasing the amount of oxygen delivered from the blood to the working muscles.
• There are three types of muscle fibres, each with different properties that enable them to perform best in different types of activities.
• The body responds to musculoskeletal exercise by increasing the temperature and enzyme activity within the muscle, and by recruiting more muscle fibres.
• Exercise prescription involves the manipulation of frequency, intensity, time and type of exercise.
• Chronic adaptations that occur as a response to exercise are specific to the training stimulus applied and include changes to the cardiovascular, metabolic, respiratory and muscular systems.
• Rest is important to avoid overtraining, promote recovery and minimise risk of injury and illness.
REFERENCES
American College of Sports Medicine, 2010, American College of Sports Medicine’s Resource Manual for Guidelines for Exercise Testing and Prescription, Philadelphia, PA: Lippincott Williams & Wilkins.
Australian Sports Commission, 2018, ASC recognition, ASC, retrieved from <www.ausport.gov.au/supporting/nso/asc_recognition>.
Borg, G.A., 1982, ‘Psychophysical bases of perceived exertion’, Medicine & Science in Sports & Exercise, vol. 14, no. 5, pp. 377–81.
Department of Health, 2017, Australia’s physical activity and sedentary behaviour guidelines, retrieved from <www.health.gov.au/internet/main/publishing.nsf/content/health-pubhlth-strateg-phys-act-guidelines>.
Exercise and Sports Science Australia, 2018, Accredited exercise scientist scope of practice, retrieved from <www.essa.org.au/wp-content/uploads/2018/05/Accredited-Exercise-ScientistScope-of-Practice_2018.pdf>.
Foster, C., Florhaug, J.A., Franklin, J. et al., 2001, ‘A new approach to monitoring exercise training’, Journal of Strength & Conditioning Research, vol. 15, no. 1, pp. 109–15.
Gellish, R.L., Goslin, B.R., Olson, R.E. et al., 2007, ‘Longitudinal modeling of the relationship between age and maximal heart rate’, Medicine & Science in Sports & Exercise, vol. 39, no. 5, pp. 822–9.
Global Association of International Sports Federations, 2012, Definition of sport, retrieved from <https://web.archive.org/web/20121205004927/http://www.sportaccord.com/en/members/definition-of-sport>.
Karvonen, M.J., 1957, ‘The effects of training on heart rate: A longitudinal study’, Annales Medicinae Experimentalis et Biologiae Fenniae, vol. 35, no. 3, pp. 307–15.
Neiman, D., 1994, ‘Exercise, upper respiratory tract infection, and the immune system’, Medicine & Science in Sports & Exercise, vol. 26, no. 2, pp. 128–39.
National Strength and Conditioning Association, 2011, NSCA’s Guide to Program Design: Understand the general principles of periodization, Champaign, IL: Human Kinetics.