CHAPTER 183
Obesity
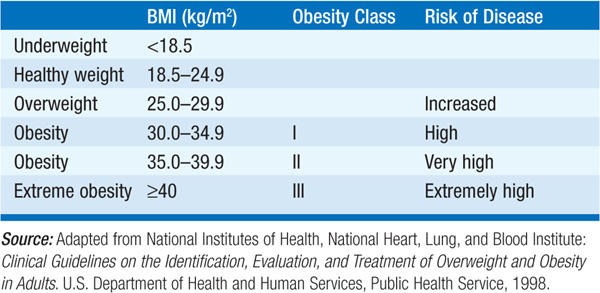
Obesity is a state of excess adipose tissue mass. Obesity should not be defined by body weight alone, as muscular individuals may be overweight by arbitrary standards without having increased adiposity. The most widely used method to classify weight status and risk of disease is the body mass index (BMI), which is equal to weight/height2 in kg/m2 (Table 183-1). At a similar BMI, women have more body fat than men. Furthermore, regional fat distribution may influence the risks associated with obesity. Central (primarily visceral) obesity [high ratio of the circumference of the waist to the circumference of the hips (waist-to-hip ratio), >0.9 in women and 1.0 in men] is independently associated with a higher risk for metabolic syndrome, diabetes mellitus, hyperandrogenism in women, and cardiovascular disease. The prevalence of obesity has increased dramatically over the past 3 decades. In the United States in 2008, 34% of adults age >20 were obese  , and another 34% were overweight (BMI 25–30). Most alarming is the same trend among children, where 17% between ages 2 and 19 were obese, and another 18% were overweight. This has led to an epidemic of type 2 diabetes in children, a condition almost never seen until recently. These trends to increased obesity are not limited to Western societies but are occurring worldwide.
, and another 34% were overweight (BMI 25–30). Most alarming is the same trend among children, where 17% between ages 2 and 19 were obese, and another 18% were overweight. This has led to an epidemic of type 2 diabetes in children, a condition almost never seen until recently. These trends to increased obesity are not limited to Western societies but are occurring worldwide.
TABLE 183-1 CLASSIFICATION OF WEIGHT STATUS AND RISK OF DISEASE
ETIOLOGY
Obesity can result from increased energy intake, decreased energy expenditure, or a combination of the two. Excess accumulation of body fat is the consequence of environmental and genetic factors; social factors and economic conditions also represent important influences. The recent increase in obesity can be attributed to a combination of excess caloric intake and decreasing physical activity. Poorly understood reasons for increased food assimilation due to dietary composition have also been postulated, as have sleep deprivation and an unfavorable gut flora. The susceptibility to obesity is polygenic in nature, and 30–50% of the variability in total fat stores is believed to be genetically determined. Among monogenic causes, mutations in the melanocortin receptor 4 are most common and account for ~1% of obesity in the general population and ~6% in severe, early-onset obesity. Syndromic obesity forms include Prader-Willi syndrome and Laurence-Moon-Biedl syndrome. Other monogenetic or syndromic causes are extremely rare. Secondary causes of obesity include hypothalamic injury, hypothyroidism, Cushing’s syndrome, and hypogonadism. Drug-induced weight gain is also common in those who use antidiabetes agents (insulin, sulfonylureas, thiazolidinediones), glucocorticoids, psychotropic agents, mood stabilizers (lithium), antidepressants (tricyclics, monoamine oxidase inhibitors, paroxetine, mirtazapine), or antiepileptic drugs (valproate, gabapentin, carbamazepine). Insulin-secreting tumors can cause overeating and weight gain.
CLINICAL FEATURES
Obesity has major adverse effects on health. Increased mortality from obesity is primarily due to cardiovascular disease, hypertension, gall bladder disease, diabetes mellitus, and several types of cancer, such as cancer of the esophagus, colon, rectum, pancreas, liver, and prostate, and gallbladder, bile ducts, breasts, endometrium, cervix, and ovaries in women. Sleep apnea in severely obese individuals poses serious health risks. Obesity is also associated with an increased incidence of steatohepatitis, gastroesophageal reflux, osteoarthritis, gout, back pain, skin infections, and depression. Hypogonadism in men and infertility in both sexes are prevalent in obesity; in women this may be associated with hyperandrogenism (polycystic ovarian syndrome).
Obesity is a chronic medical condition that requires ongoing treatment and lifestyle modifications. Treatment is important because of the associated health risks, but is made difficult by a limited repertoire of effective therapeutic options. Weight regain after weight loss is common with all forms of therapy. The urgency and selection of treatment modalities should be based on BMI and a risk assessment.
Diet, exercise, and behavior therapy are recommended for all pts with a BMI ≥25 kg/m2. Behavior modification including group counseling, diet diaries, and changes in eating patterns should be initiated. Food-related behaviors should be monitored carefully (avoid cafeteria-style settings, eat small and frequent meals, eat breakfast). A deficit of 7500 kcal will produce a weight loss of approximately 1 kg. Therefore, eating 100 kcal/d less for a year should cause a 5-kg weight loss, and a deficit of 1000 kcal/d should cause a loss of ~1 kg per week. Physical activity should be increased to a minimum of 150 min of moderate intensity physical activity per week.
Pharmacotherapy may be added to a lifestyle program for pts with a BMI ≥30 kg/m2 or ≥27 kg/m2 with concomitant obesity-related diseases. Orlistat is the only pharmacologic agent currently approved by the U.S. Food and Drug Administration for treatment of obesity; several others have been withdrawn from the market because of significant adverse effects. Orlistat, an inhibitor of intestinal lipase, causes modest weight loss (9–10% at 12 months with lifestyle measures) due to drug-induced fat malabsorption. Metformin, exenatide, and liraglutide tend to decrease body weight in pts with obesity and type 2 diabetes mellitus, but they are not indicated for pts without diabetes.
Bariatric surgery should be considered for pts with severe obesity (BMI ≥40 kg/m2) or moderate obesity (BMI ≥35 kg/m2) associated with a serious medical condition, with repeated failures of other therapeutic approaches, at eligible weight for >3 years, capable of tolerating surgery, and without addictions or major psychopathology. Weight-loss surgeries are either restrictive (limiting the amount of food the stomach can hold and slowing gastric emptying), such as laparoscopic adjustable silicone gastric banding, or restrictive-malabsorptive, such as Roux-en-Y gastric bypass (Fig. 183-1). These procedures generally produce a 30–35% weight loss that is maintained in about 40% of pts at 4 years. Complications include stomal stenosis, marginal ulcers, and dumping syndrome. Procedures with a malabsorptive component require lifelong supplementation of micronutrients (iron, folate, calcium, vitamins B12 and D) and are associated with a risk of islet cell hyperplasia and hypoglycemia.
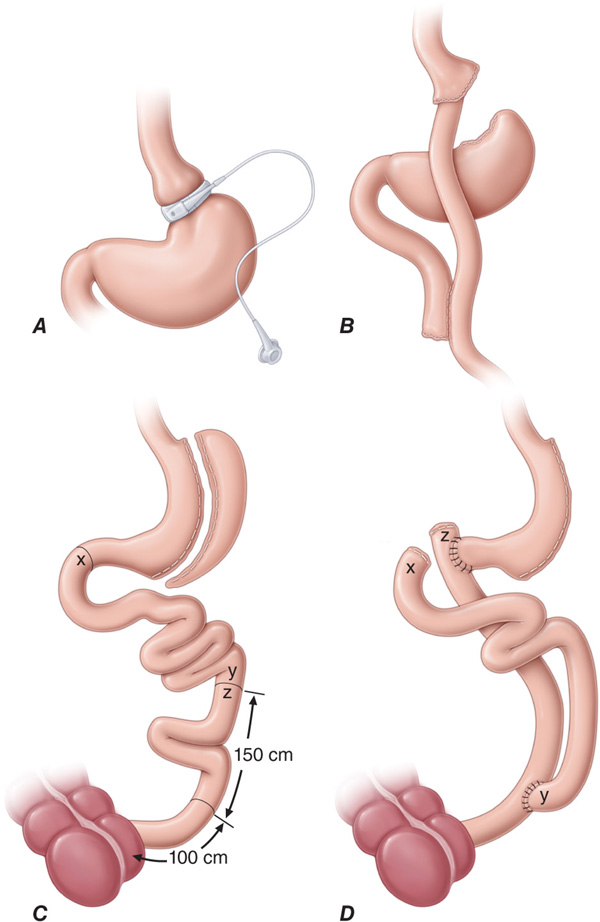
FIGURE 183-1 Bariatric surgical procedures. Examples of operative interventions used for surgical manipulation of the gastrointestinal tract. A. Laparoscopic gastric band (LAGB). B. The Roux-en-Y gastric bypass. C. Biliopancreatic diversion with duodenal switch. D. Biliopancreatic diversion. (From ML Kendrick, GF Dakin, Surgical approaches to obesity. Mayo Clinic Proc 815:518, 2006; with permission.)

For a more detailed discussion, see Flier JS, Maratos-Flier E: Biology of Obesity, Chap. 77, p. 622 and Kushner RF: Evaluation and Management of Obesity, Chap. 78, p. 629, in HPIM-18.