
Most parents-to-be expect their babies to arrive right around their due date, give or take a couple of days or weeks. And the majority of babies do arrive pretty much on schedule, allowing them plenty of time to prepare for life outside the womb and their parents plenty of time to prepare for life with a baby.
But in about 12 percent of births in the United States, that vital preparation time is cut unexpectedly—and sometimes dangerously—short when baby is born prematurely and/or too small. Some of these babies weigh in at just a few ounces under the low-birthweight (5-pound, 8-ounce) cutoff, and are able to quickly and easily catch up with their full-term peers. But others, deprived of many weeks of vital uterine development, arrive so small that they can fit in the palm of a hand. It can take months of intensive medical care to help them do the growing they were supposed to have done in the cozy, nurturing confines of the womb.
Though the low-birthweight baby (whether born early or born small for gestational age) is still at higher risk than larger babies, rapid advances in medical care for tiny infants have made it possible for the great majority of them to grow into normal, healthy children. But before they are carried proudly home from the hospital—and sometimes even after they’re home—a long road often lies ahead for these babies and their parents.
If your baby has arrived too soon and/or too small, you’ll find the information and support you’ll need to navigate that road in the pages that follow.
Learning to eat outside the womb isn’t easy at first, even for a full-term baby who must master the basics of nursing from a breast or a bottle. For preterm or low-birthweight babies, the challenges may multiply. Those who are born just 3 or 4 weeks early are usually able to breastfeed or take the bottle right after birth—again, after mastering the basics. Ditto for babies who were born close to term but at a low birthweight. But babies born before 34 to 36 weeks usually (but not always) have special nutritional needs that traditional feeding can’t satisfy—not only because they’re born smaller, but because they grow at a faster rate than full-term babies do, may not be able to suck effectively, and/or may have digestive systems that are less mature. These littlest babies also need a diet that mirrors the nutrition they would be receiving if they were still growing in utero and that helps them gain weight quickly. And those vital nutrients need to be served up in the most concentrated form possible, because preemies and low-birthweight babies can take only tiny amounts of food at a time—partly because their stomachs are so small, and partly because their immature digestive systems are sluggish, making the passage of food a very slow process. And since they can’t always suck well or even suck at all, they can’t take their meals from a bottle or a breast—at least not right away. Luckily, breast milk, fortified breast milk, or specially designed formulas can usually provide all the nutrients preemies and low-birthweight babies need to grow and thrive.
As a parent of a premature or very-low-birthweight infant, you will find that feeding and monitoring weight gain become two of the most consuming aspects of caring for your baby in the hospital—in terms of both time and emotion. The neonatologists and nurses will do everything they can to ensure that your preemie receives the nutrition needed to gain weight. Just how your baby receives that nutrition depends on how early he or she was born:
IV feeding. When a very small newborn is rushed to the intensive care nursery, an intravenous solution of water, sugar, and certain electrolytes is often given to prevent dehydration and electrolyte depletion. Very sick or small babies (usually those who arrive before 28 weeks gestation) continue to receive nutrition through their IV. Called total parenteral nutrition (TPN) or parenteral hyperalimentation, this balanced blend of protein, fat, sugar, vitamins, minerals, and IV fluids is given until the baby can tolerate milk feedings. Once your baby is able to begin milk feedings by gavage, TPN will decrease.
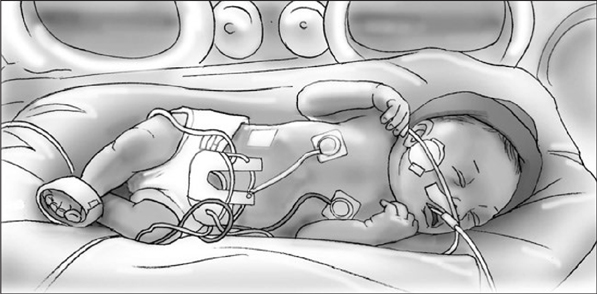
Gavage feeding. Babies who arrive between 28 and 34 weeks gestation and who don’t need IV nutrition (or babies who started out on TPN but have progressed to the point where they can tolerate milk feedings) are fed by gavage—a method not dependent on sucking, since babies this young usually have not yet developed this reflex. A small flexible tube (gavage tube; see illustration) is placed into the baby’s mouth or nose and passed down to the stomach. Prescribed amounts of pumped breast milk, fortified breast milk, or formula are fed through the tube every few hours. Gavage tubes are either left in place between feedings or removed and reinserted for each feeding. (The tube won’t bother your preemie because the gag reflex doesn’t develop until about 35 weeks.)
It may be a relatively long time before you’ll be able to feed your baby as you’d always imagined you would, through breast or bottle. Until then, you can still take part in feedings by holding the tube and measuring how much your baby takes, cuddling skin-to-skin during tube feedings, or giving your baby your finger to practice sucking on while he or she is being fed (this helps strengthen the sucking reflex and may also help your baby associate sucking with getting a full tummy).
Babies who can’t yet feed from a nipple are fed through a small, flexible gavage that is placed through the baby’s mouth or nose into the stomach.
Nipple feeding. One of the most momentous milestones of your preemie’s stay in the hospital will be the switch from gavage feeding to nipple feeding. When it comes to readiness for this milestone, there can be some big differences among little babies. Some are ready to tackle the breast or bottle as early as 30 to 32 weeks gestational age. Others won’t be ready to take on the nipple until 34 weeks, still others, not until 36 weeks gestational age.
The neonatologist will consider several factors before giving you the green light to begin breastfeeding or bottle-feeding: Is your baby’s condition stable? Can he or she handle being fed in your arms? Have all the other physical requirements of readiness been met—for instance, can baby suck rhythmically on a pacifier or feeding tube and coordinate breathing and sucking? Is baby awake for longer periods? Are there active bowel sounds and no sign of abdominal distension or infection, and has meconium stool been passed?
Since nipple feedings are tiring for a small baby, they’ll be started slowly—one or two a day, alternated with tube feedings. Infants with respiratory problems may have an even harder time, requiring extra oxygen while feeding or experiencing short episodes of apnea (breathing cessation) while sucking (they might concentrate too hard on sucking and forget to breathe). For babies who have trouble mastering the suck, a specially designed pacifier may be used to help them practice and perfect their technique before graduating to breast or bottle.
What are preemies and low-birthweight babies nourished with? Whether fed through gavage or nipple, your tiny baby will get either breast milk, fortified breast milk, or formula:
• Breast milk. Breast is best not only when it comes to full-term infants, but also (or especially) when it comes to preemies, and for a number of reasons: First, it’s custom designed for a preemie’s special nutritional needs. Milk from moms who deliver early is different from milk from those who deliver at term. It contains more protein, sodium, calcium, and other nutrients than full-term breast milk does. This preemie-perfect balance prevents tiny babies from losing too much fluid, which helps them maintain a stable body temperature. It’s also easier to digest and helps babies grow faster.
Second, breast milk has important substances not found in formula. Colostrum (early breast milk) is extremely rich in antibodies and cells that help fight infection. This is especially important when babies are sick or premature and may have a higher chance of developing an infection.
Third, research has shown that breastfed preemies have a lower risk of developing necrotizing enterocolitis, an intestinal infection unique to preemies (click here). They also tolerate feedings better, have a lower risk of allergies, and receive all the benefits that a full-term baby gets from breast milk (click here). Even if you don’t plan to breastfeed long-term or full-time, providing breast milk for your baby while he or she is in the hospital—either by nursing or pumping or both—gives your baby the best possible start at a time when that start has begun too soon. Moms who can’t produce milk (or enough milk) can feed their preemies the best, too, since donated milk is often available through the hospital or a recognized and licensed milk bank.
To ensure your baby is still getting enough nutrition in the early stages of breastfeeding (when baby’s suck may still be weak or your breasts are not producing sufficient amounts of milk), talk to the doctor about the following supplemental feeding methods that don’t interfere with nursing.
If you’re nursing, you can:
• Nurse with the gavage still in place
• Use a supplemental nutrition system (click here)
If you’re pumping you can:
• Bottle-feed with the gavage still in place
• Use a feeding system taped to your finger (finger feeding)
• Feed the milk through a syringe
• Use slower-flow bottle nipples
For more on breastfeeding your premature baby, click here.
• Fortified breast milk. Sometimes, even the milk of a preemie’s mother isn’t enough for a preemie. Since some babies, particularly very tiny ones, need even more concentrated nutrition—including more fat, proteins, sugars, calcium, and phosphorus, and possibly, more of such other nutrients as zinc, magnesium, copper, and vitamin B6—the breast milk being fed through a tube or a bottle may be fortified with human milk fortifier (HMF) as needed. HMF comes in a powdered form that can be blended with breast milk, or in a liquid form for use when adequate amounts of breast milk are not available.
• Formula. Babies can do well, too, when they’re fed formula specially designed for preemies. Even if you are breastfeeding, your baby may get additional feedings with a bottle or supplemental nursing system. Preemies are fed using small plastic bottles marked in cubic centimeters (cc) or milliliters (ml). The nipples are specially designed and require less sucking strength from your baby. Ask a nurse to show you the correct position for bottle-feeding your preemie—it may differ slightly from that for a full-term infant.
Feeding a newborn often comes with challenges. Feeding a preemie or low-birthweight baby multiplies those challenges:
Sleepiness. Many preemies get tired easily—and sometimes sleeping can win out over eating. But frequent feeds are needed so a small baby can start catching up on growth—and it’s up to you to make sure your extra-little one doesn’t sleep through the feeds he or she needs. For tips on how to wake a sleepy baby, click here.
Breath holding. Some preemies, especially those who were born without good sucking-breathing coordination, will forget to breathe when feeding. This can be tiring for baby and anxiety producing for you. If you notice your baby hasn’t taken a breath after a number of sucks or looks pale while feeding, remove the nipple from baby’s mouth and let him or her take a breath. If your baby seems to be holding his or her breath all the time during feedings, regularly remove the nipple after every three to four sucks.
Oral aversion. Babies who have spent a lot of time in the NICU may come to associate their mouths with feeding tubes, ventilator tubes, suctioning, and other unpleasant sensations and experiences. As a result, some preemies develop a strong aversion to having anything in or around their mouths. To combat this, try to replace the unpleasant oral associations with more pleasant ones. Gently stroke your baby around the mouth, give your baby a pacifier or your finger to suck, or encourage your baby to touch his or her own mouth or suck on his or her thumb or fist.
Reflux. Many preemies are prone to gastroesophageal reflux disease (GERD) because of their immature digestive systems. Click for tips on coping with spitting up and GERD.
If by the time you get home together you’re breastfeeding your preemie exclusively, you’ll be all set—your breast milk supply will continue to grow with your baby. If you’re formula feeding (or doing a combo), you may or may not need to continue using formula specifically designed for preemies once you’re home with your little one. It’ll depend on your baby’s progress, and your doctor will be able to steer you to the right formula. You might decide to continue to use the same small bottles that were used in the hospital, especially because preemies need to be fed smaller amounts and need to be fed more often than full-termers. But keep in mind that what worked in the hospital might not work as well once you’re home and your baby continues to grow in both size and maturity.
Wondering about when to start solids? Like full-term babies, preemies should start receiving solids at about 6 months. But for preemies, that date is based on adjusted age rather than chronological age (which means a preemie who was born 2 months early might not be ready for solids until 8 chronological months). Because some preemies experience delays in development, solid feedings should not be started until there are signs of readiness (click here), even if the corrected age says it’s time to bring on solids. Some preemies have a more difficult adjustment to solids—especially once they graduate to chunkier foods—often because of negative oral associations picked up earlier. Working with a speech or occupational therapist can help a baby overcome oral aversions and move on to a lifetime of healthy eating.
“How will I ever bond with my preemie if she’s spending the first few months of her life in the NICU?”
Your baby was whisked away moments after birth and before you even got a good look at her, she’s too fragile to breastfeed, and she spends more time being poked and prodded by the hospital staff than snuggling in your arms. It’s no wonder you’re feeling as if bonding with your new baby—something that may seem so easy and natural to parents of full-termers—is an impossible goal to reach. But here’s the real truth about bonding: The love and attachment between mom, dad, and baby develop over many months and years, blossoming over a lifetime rather than bursting into full bloom during the first few moments of life. So if you didn’t get the chance to bond with your preemie newborn the way you had dreamed of, all is not lost—in fact, nothing at all is lost. Plus, there are plenty of ways to start the lifelong process now—even while your baby is still in the hospital. Here’s how:
Ask for a picture, along with a thousand words. Baby’s not with you? Sometimes preemies have to be moved to another hospital for upgraded intensive care while mom’s still stuck in the hospital postdelivery. If that’s the case with you and your new bundle, have your spouse (or the hospital staff) email or text you some pictures and videos of your baby so you can enjoy looking at them until you’re able to look at the real thing. Even if more tubing and gadgets are visible than baby, what you see will likely be less frightening and more reassuring than what you might have imagined. As helpful as a picture may be, you’ll still want those thousand words—from your spouse, and later the medical staff—describing every detail of what your baby is like and how she’s doing.
Be hands-on. You may be afraid to touch your tiny, fragile baby—and you may even feel that he or she is better off not being touched—but studies have shown that premature infants who are stroked and lightly massaged while they are in intensive care grow better and are more alert, active, and behaviorally mature than babies who are handled very little. So, assuming the neonatologist gives the okay (some very early preemies can’t tolerate touch and find any kind of handling stressful), let your hands do the bonding. Start by gently touching those arms and legs, since they are less sensitive at first than the trunk. Try to work up to at least 20 minutes of stroking a day.
Care like the kangaroos do. Skin-to-skin contact can not only help you get close to your baby, it can help with her growth and development. In fact, studies have shown that babies who receive so-called kangaroo care are likely to leave the NICU sooner. To cuddle your baby marsupial-style, place her on your chest under your shirt so that she’s resting directly on your skin (she’ll probably be wearing only a diaper and a hat, which prevents heat loss via the head). Loosely place your shirt over her to keep her even warmer, or cover her with a blanket. See box for more.
It turns out kangaroos are more than just cute—when it comes to caring for their new babies, research shows they’re smart, too. Snuggling a baby (particularly a preemie) skin-to-skin is a marsupial-inspired parenting practice that comes with many substantial benefits, right from the start and continuing throughout the NICU stay and beyond. For your baby, and for you.
You can start skin-to-skin contact, known as kangaroo care, as soon as the neonatologist determines that your baby is stable enough—even if she is very sick or very small, and hooked up to machines. Not only can’t the snuggling hurt your baby, it can help in so many ways. Your baby will be comforted by your heartbeat, your scent, and the rhythm of your voice and your breathing. Kangaroo care will help maintain your baby’s body warmth, regulate his or her heart and breathing rates, and speed weight gain and development. It’ll also encourage deeper sleep, and help your baby spend more of his or her awake time quiet and alert instead of stressed and crying—all of which help boost development.
The benefits of kangaroo care extend to you, too. Being close to your baby (even when you’re not feeding) can help improve a mom’s milk supply and your chances of breastfeeding success. It’ll also, not surprisingly, help nurture bonding between you and your baby while building your confidence as a new parent. (It will be something you can do for your baby, in a NICU where most of baby’s care is provided by strangers.)
What’s more, both you and your baby will collect on the benefits of skin-to-skin contact even if it’s only for short periods of time each day. Have the time, and protocol and treatment permit? The more kangaroo care—ideally at least an hour at a time—the better.
Moms and dads can both offer kangaroo care—there’s no special equipment required (and dad’s hairy chest definitely doesn’t disqualify him). Simply hold your diapered baby upright on your bare chest (between your breasts if you’re the mom), positioned tummy to tummy with a blanket or your clothes draped over your baby’s back. Then breathe in your baby’s scent, close your eyes, and relax. You’re doing a world of good for your tiny bundle of joy, and for yourself.

Carry on a conversation. Sure, it’ll be a one-way conversation at first—your baby won’t be doing any talking, or even much crying, while she’s in the NICU. She may not even appear to be listening. But she’ll recognize your voice (and your spouse’s) from when she was in utero—and she’ll be comforted by the familiar sound. Can’t be with your baby as often as you’d like? Leave a recording of your voice, talking, singing, or reading, that the nurses can play for your baby when you’re not around. Just keep the volume down whenever you’re near your little one, since her ears are still very sound-sensitive. In fact, for some very small preemies, any extra sounds can be extremely disturbing, so check with your baby’s doctor about how much sound is just right for her and how much is too much.
See eye-to-eye. If your baby’s eyes are shielded because she’s getting phototherapy for the treatment of jaundice, ask to have the bili lights turned off and her eyes uncovered for at least a few minutes during your visit so that you can make eye-to-eye contact while you’re doing your kangaroo cuddling or through the isolette (click here) walls.
Take over for the nurses. As soon as your baby’s out of immediate danger, the NICU nurse will show you how to diaper, feed, and bathe her. You may even be able to perform some simple medical procedures for her. Caring for your tiny baby will help make you more comfortable in your new parent skin, offer a sense of normalcy, and give you some valuable experience for the months that lie ahead (particularly those first few weeks at home). If staff doesn’t offer to show you these basics or give you the opportunity to get some hands-on experience, ask.
“My baby is in the NICU, and it’s scary seeing all that medical equipment he’s hooked up to … all those tubes and wires.”
A first look at a NICU can be frightening, especially if your baby is one of the tiny patients in it. Knowing what you’re looking at can keep your fears from overwhelming you. Here’s what you can expect in most NICUs:
A main nursery area comprising a large room or a series of rooms. There may also be a couple of isolation rooms in an area separate from the main nursery. Adjoining may be several small family rooms where moms can express milk (breast pumps are usually provided), and where families can spend cuddling time with their babies as they get stronger.
An often busy atmosphere. Depending on the size and occupancy of the NICU, there may be many nurses and doctors bustling about, treating and monitoring babies. Other parents may also be caring for or feeding their own infants.
Relative quiet. Though it’s one of the busiest places in the hospital, it’s typically also one of the quietest. That’s because very loud noises can be stressful for tiny babies or even harmful to their ears. To help keep the sound level down, you should talk quietly, close doors and isolette portholes gently, and take care not to drop things or place items loudly on the tops of incubators. (One sound that is important for your preemie, however, is the sound of your voice; click here.)
Dim lights. Since still-sensitive eyes need protection, too (after all, they’d be exposed to no light at all if they were still in the womb), NICU staff usually tries to control the brightness in the nursery. While bright lights are often necessary so that the doctors and nurses can do what they need to do (and see what they’re doing) to keep your baby healthy and thriving, most NICUs do their best to keep the lights down to simulate life in the womb. Putting a blanket over your baby’s isolette when the lights are bright may help somewhat as well—though ask the staff first, because it’s also important that your baby not be kept in the dark all the time. Research shows that constant dim light can disturb body rhythms and slow the development of normal sleep-wake cycles. In fact, preemies who are exposed to natural cycles of light and dark that mimic day-night rhythms gain weight faster than those kept around-the-clock in either bright light or low light.
Strict hygiene standards. Keeping germs that can spread infection (and make sick babies sicker) out of the nursery is a major priority in the NICU. Each time you visit, you’ll need to wash your hands with antibacterial soap or sanitizer (there’s usually a sink or dispenser for this purpose right outside the nursery doors). You may be asked to put on a hospital gown, too. If your baby is in isolation, you may also need to wear gloves and a mask.
Tiny babies. Some will be in clear incubators or isolettes (bassinets that are totally closed except for four portholelike doors that allow you and the staff to reach in and care for your baby) or in open bassinets. Some may be on warming tables under overhead heat lamps. Some very small babies may be wrapped in a plastic (polyethylene) skin wrap to minimize the loss of fluids and body heat through the skin, particularly in the few hours right after birth. This helps preemies keep warm—particularly those less than 4 pounds, who lack the fat necessary to regulate body temperature, even when they’re swaddled in blankets.
An array of apparatus. You’ll notice an abundance of technology near each bed. Monitors that record vital signs (and will warn, by setting off an alarm, of any changes that need prompt attention) are hooked up to babies via leads that are either held on the skin with gel or inserted by needle just under the skin. In addition to a monitor, your baby may be linked to a feeding tube, an IV (via arm, leg, hand, foot, or head), a catheter in his umbilical stump, temperature probes (attached to the skin with a patch), and a pulse oximeter that measures the oxygen level in his blood using a small light attached to the hand or foot. A mechanical ventilator (breathing machine) may be used to help your baby breathe normally if he is less than 30 to 33 weeks gestation. Otherwise, your baby may receive oxygen through a mask or delivered into his nose through soft plastic prongs attached to tubing. There will also be suction setups that are used periodically for removing excess respiratory secretions, as well as lights for phototherapy (bili lights), used to treat babies with excess jaundice. (Babies undergoing this treatment will be naked except for eye patches, which protect their eyes from the bili lights.)
A place for parents to cuddle (and kangaroo) their babies. In the midst of all this high-tech equipment, there will likely be rocking chairs or gliders where you can feed or hold your baby.
A large team of highly trained medical specialists. The staff caring for your baby in the NICU might include a neonatologist (a pediatrician who has had special training in newborn intensive care), pediatric residents and neonatal fellows (doctors undergoing training), a physician assistant or nurse practitioner, a clinical nurse specialist, a primary nurse (who will be your baby’s primary caregiver as well as your primary go-to), a nutritionist, a respiratory therapist, other physician specialists (depending on your baby’s particular needs), social workers, physical and occupational therapists, x-ray and lab technicians, and lactation specialists.
The parents of full-term newborns may be surprised when they first see their babies. The parents of preterm infants are often shocked. The average preemie weighs between 1,600 grams (about 3½ pounds) and 1,900 grams (about 4 pounds, 3 ounces) at birth, and some weigh considerably less. The smallest can fit in the palm of an adult hand and have wrists and hands so tiny that a wedding band could be slipped over them. The preemie’s skin is translucent, leaving veins and arteries visible. It seems to fit loosely because it lacks a fat layer beneath it (making it impossible for baby’s temperature to self-regulate), and often it is covered with a fine layer of prenatal body hair, or lanugo, that has usually been shed by full-term infants. Because of an immature circulatory system, you may notice some skin coloring changes when you touch or feed your baby. Your little one’s ears may be flat, folded, or floppy because the cartilage that will give them shape has yet to develop. Preemies often lie with arms and legs straight rather than classic newborn style—curled or tucked in—not only because their muscles still lack strength, but because they never had to fold to fit in a cramped uterus as full-term babies do.
Sexual characteristics are usually not fully developed—testicles may be undescended, the foreskin in boys and the inner folds of the labia in girls may be immature, and there may be no areola around the nipples. Because muscular and nerve development are not complete, many reflexes (such as grasping, sucking, startle, rooting) may be absent. Unlike term babies, a preemie may cry little or not at all. He or she may also be subject to periods of breathing cessation, known as apnea of prematurity.
But the physical characteristics of preemies that make up this portrait are only temporary. Once preterm newborns reach 40 weeks of gestation, the time when, according to the calendar, they should have been born, they very much resemble the typical newborn in size and development.
“The doctors say my preemie will have to spend many weeks in the hospital. How long is it likely to be—and how will I be able to handle her long stay?”
Chances are, you’ll be able to bring your baby home from the hospital at about the same time you would have if she had arrived at term—about 37 to 40 weeks gestational age—though if your preemie faces other medical challenges besides being small, the stay may be extended. But no matter how long your baby’s hospitalization ends up being, it will likely feel even longer. To make the most of that time and to even help it pass somewhat faster, try:
Striking up a partnership. Parents of a preemie often begin to feel that their baby belongs less to them and more to the doctors and nurses, who seem so competent and do so much for him. But instead of worrying that you can’t measure up to the staff, try teaming up with them. Get to know the nurses (easier if your baby has a primary nurse in charge of care at each shift, which is likely), the neonatologist, and the residents. Let them know you’d like to do as much of the baby care as possible—diapering, swaddling, bathing—which can save them time, help you pass yours, and help you feel less like a bystander and more like an involved participant in your little one’s care.
Getting a medical education. Learn the jargon and terminology used in the NICU. Ask the in-charge nurse to show you how to read your baby’s chart. Ask the neonatologist for details about your baby’s condition and for clarification when you don’t understand. Parents of preemies often become experts in neonatal medicine very quickly, throwing around terms like RDS and intubation as easily as a neonatologist. See box for some frequently used terms.
Being a fixture at your baby’s side. Some hospitals may let you move in, but even if you can’t, you should spend as much time as possible with your baby, alternating shifts with your spouse as needed. This way you will get to know not only your baby’s condition but your baby as well. (If you have other children at home, however, they’ll also need you now. Click here for more on siblings).
Making your baby feel at home. Even though the isolette’s only a temporary stop for your baby, try to make it as much like home as possible. Ask permission to put friendly-looking stuffed animals around your baby and tape pictures (perhaps including stimulating black-and-white enlargements of snapshots of mommy and daddy) to the sides of the isolette for her viewing pleasure. Ask if you can pipe in a recording of your voice for when you’re not there, or soft music. Remember, however, that anything you put in the baby’s isolette will have to be sterilized and obviously can’t interfere with life-sustaining equipment.
Readying your milk supply. Your milk is the perfect food for your premature baby. Until she’s able to nurse, pump milk for indirect feedings and to keep up your supply. Pumping will also give you a welcome feeling that you’re “doing something.”
Hitting the shops. Since your baby arrived ahead of schedule, you may not have had time to order furniture, layette items, and other necessities. If so, now’s the time to get online and get that shopping done. If you feel superstitious about filling your home with baby things before she is discharged from the hospital, fill up the cart but don’t complete the order until you’re closer to the homecoming (especially because you won’t know what size to buy those diapers or baby clothes in just yet). You’ll not only have taken care of some necessary chores, but will also have filled some of the long hours of baby’s hospitalization and made a statement (at least to yourself) that you’re confident you’ll be bringing your new bundle home soon.
“I’m trying to be strong for my son while he’s in the NICU, but I’m scared, overwhelmed, and feeling out of control.”
Most parents whose babies are in the NICU experience a wide spectrum of ever-changing emotions, which can range from shock to anger to frustration, stress to fear to numbness, disappointment to confusion, intense sadness to equally intense hope—all of which are valid, understandable, and normal. You may feel overwhelmed by all the medical equipment attached to your baby and the constant activity of nurses and doctors. You may be frightened of the procedures your baby is undergoing or frustrated by feelings of helplessness. You may feel disappointed that your little one isn’t the dimpled, adorable full-term baby you’d been expecting (and envisioning) throughout your pregnancy, frustrated that you can’t take him home to begin your life together, and guilty about both sets of emotions. You may also feel guilty for not feeling happy about your baby’s birth or guilty about not being able to keep the pregnancy going longer (even if there was absolutely nothing you could have done to prevent your baby’s prematurity, which most often, there isn’t). You may feel unsettled at the uncertainty of your baby’s future, particularly if he is very small or sick. You may even unconsciously distance yourself from your preemie for fear of becoming too attached or because you find bonding difficult to accomplish through the portholes of an isolette. Or, you may feel unexpectedly strong feelings of love and attachment—deepened, instead of challenged, by the ordeal you’re both enduring. You may be angry at yourself for your reactions, at your partner for not reacting the same way you are, at your family and friends for not understanding what you’re going through or for acting as if nothing has happened, at your ob for not preventing this. Confusing these emotions further may be the fact that they may often conflict or fluctuate wildly—for instance, leaving you feeling hopeful one minute, hopeless the next, deeply in love with your baby one day, afraid to love him the next. Compounding them may be the physical exhaustion that comes from keeping a round-the-clock vigil at your baby’s bedside, which may be more debilitating still if you haven’t yourself recovered from delivery or are suffering from nipples painfully cracked from pumping.
Coping with these emotions may be extremely difficult, but keeping the following in mind may help:
• What you’re feeling, saying, and doing is perfectly normal. Such extreme and sometimes contradictory emotions are experienced by nearly every parent of a premature baby at some time or another (though you may often believe that no one else has ever felt the way you do).
• There is no one right way to feel. Your emotions may differ from those of your partner, the parents of the baby in the next isolette, or from other parents of preemies you’ve talked to. Everyone will react to it a little differently—and that’s normal, too. Remember, too, as you speak to other parents of preemies (and you should) that they may be feeling all of the same unsettling emotions on the inside, but those feelings may not show on the outside. Deep emotions often stay deep inside.
• Emotions need expressing. Keeping your feelings inside will only compound them—and make you feel more isolated. Let the NICU staff know what your feelings and fears are. Not only will they understand what you’re going through (since helping parents is almost as important a part of their job as helping babies), but they may offer insights that can help you cope.
• You and your partner need each other. You can each gain strength by leaning on the other—and can be more effective as a team than individually. Open communication can also help keep the stress inherent in parenting a preemie (or having a sick baby) from hurting your relationship.
• Support best comes from those who know. Try talking with other parents in the NICU. You’ll find that they also feel alone, unsure, and scared. Friendships are easily formed in the NICU because other parents need you as much as you need them. Many hospitals make support available through groups run by the NICU social worker, or can hook you up with support families whose babies have left the NICU—especially through online groups. No one can relate better to what you’re experiencing—and share more wisdom and empathy—than parents who’ve experienced it themselves. Also be sure to tap into the message boards at WhatToExpect.com to look for support from those who know. A mobile source of support will be especially invaluable during those long days and nights of waiting at the NICU.
• It will take time. You probably won’t be on an even emotional keel at least until your baby’s on an even physical one. Until then, you’ll have good days and bad days (usually corresponding to your baby’s ups and downs). If you’re a brand new mom of a preemie, your physical recovery and normal hormonal fluctuations can intensify feelings of all kinds. Reminding yourself that your feelings are normal—that all parents of preemies ride an emotional roller coaster at least until their babies are safely home and completely well (and sometimes even longer than that)—won’t make the feelings go away, but it will help give you the perspective you need to cope with them. Of course, if you (or your partner) are feeling sadness, hopelessness, anxiety, or an inability to function that’s too significant to attribute to the very normal stresses of being the parent of a preemie, it could be that you’re also dealing with postpartum depression. Click here and What to Expect When You’re Expecting for more on recognizing the symptoms of PPD, and be sure to seek the help you need to get better fast. Remember: To take the best care possible of your little baby, you’ll also need to take the best care possible of yourself.
“I’ve always been determined to breastfeed my baby, and since she was born at 28 weeks, I’ve been pumping milk to be fed to her through a tube. Will she have trouble switching to nursing later?”
So far, so good. From birth your baby has been provided with the best possible food for a premature newborn—her mommy’s milk—in the only way such a tiny baby is able to take nourishment, through a tube. Naturally, you’re concerned that she be able to continue to get this perfect food once she graduates to suckling. But you have little to worry about. Research finds that premature infants weighing as little as 1,300 grams, or nearly 3 pounds, and as young as 30 gestational weeks may be able to suckle at the breast and are more successful at it than they are with the bottle.
Once you do put your baby to the breast, you’ll want to make conditions as conducive to success as possible. Here’s how:
• Read all about breastfeeding, beginning here, before getting started. Also enlist the help of a lactation consultant (hopefully there will be one on staff to help you out).
• Be patient if the neonatologist or nurse wants your baby monitored for temperature and/or oxygen changes during breastfeeding. This won’t interfere with the breastfeeding process itself, and it will protect your baby by sounding an alarm in case she is not responding well to the feeding.
• Be sure you’re relaxed and that your baby is awake and alert.
• Ask the staff if there is a special nursing area for preemie moms, a private corner with an armchair or glider for you and your baby, or a privacy screen that can be put up to shield you—especially because it’s best if you cuddle and nurse your baby skin-to-skin.
• Get comfortable, propping your baby on pillows, supporting her head. Many new moms find a football hold (click here) comfortable as well as easy on the nipples.
• If your baby doesn’t yet have a rooting reflex (she probably doesn’t), help her get started by placing your nipple, with the areola, into her mouth. Compress your breast lightly with your fingers to make it easier for her to latch on (click here), and keep trying until she succeeds.
• Watch to be sure your baby is getting milk. Your breasts are used to mechanical pumping and will take a while to adjust to the different motions generated by your baby’s mouth. At first, your baby’s suckling will be rapid—an attempt to stimulate let-down. Then, as the milk is let down, your baby will slow down her suck and switch to a suckle-swallow pattern.
• If your baby doesn’t seem interested in your breast, try expressing a few drops of milk into her mouth to give her a taste of what’s in store.
• Nurse your baby for as long as she’s willing to stay at the breast. Keep her on your breast until she’s stopped active suckling for at least 2 minutes. Small preemies may nurse for close to an hour before being satisfied.
• Don’t be discouraged if the first session or first several sessions seem unproductive. Many full-term babies take a while to catch on, and preemies deserve at least the same chance. Still having trouble? Ask for help.
• Ask that any feedings at which you can’t nurse be given by gavage (through the nose) rather than by bottle. If human milk fortifier or other fortification is given to your baby to supplement the breast milk, ask that it, too, be given by gavage or by the supplementary nutrition system (click here).
You’ll be able to tell how well your baby is doing on the breast by following her daily weigh-in. If she continues gaining about 1 to 2 percent of her body weight daily, or about 3½ to 7½ ounces a week, she’ll be doing fine. By the time she reaches her original due date, she should be approaching the weight of a full-termer—somewhere around 6 to 8 pounds. Do keep in mind that breastfed preemies (as with term infants) will gain a little more slowly than formula-fed ones.
“So far I’ve handled our baby only through the portholes of his isolette. But I’m worried about how well I’ll be able to handle him when he finally comes home. He’s so tiny and fragile.”
When your baby finally makes that long-anticipated trip home, he’ll probably seem pudgy and sturdy to you, rather than tiny and fragile. After all, depending on how small he was when he arrived, he may have doubled his birthweight when he hits 4 or 5 pounds—the average weight at discharge for preemies. And chances are, you won’t have any more trouble caring for him than most new parents have caring for their full-term babies. In fact, if you have a chance to do some baby care at the hospital (something you should be encouraged to do, especially when it comes to his specialized care) in the weeks before your baby’s homecoming, you’ll actually be ahead of the new parent curve. Which is not to say it will be easy—it rarely is for new parents, whether the bundle they’re bringing home is preemie or full term.
If you’re wondering how well you and your baby will do without a nurse or neonatologist looking over your shoulder, be assured that hospitals don’t send home babies who are still in need of full-time professional care. Any care that you’ll need to provide at home (beyond the baby basics), the staff will prepare you for—and if they don’t give you the instructions and preparation you need, ask for them. Also ask about getting infant CPR training before you take baby home, an important skill for any new parent, but especially one of a preemie (click here. To help parents feel more confident before discharge, most NICUs offer parents the opportunity to spend a night with their baby in a family room close to the nursery but without any nursery staff supervision—on their own, but with backup a call light away.
If you’re still feeling overwhelmed at the thought of going it alone by the time your baby’s getting ready for discharge (especially if he’s being sent home with an assortment of medical apparatus, such as breathing monitors and oxygen hoods), consider hiring a baby nurse who has experience with preemies and their care to help out for the first week or two, finances permitting.
“Though the doctor says our baby is doing well, I’m still afraid that she’ll come through this with some kind of permanent problems.”
One of the greatest miracles of modern medicine is the rapidly increasing survival rate for premature infants. At one time, a baby weighing in at 1,000 grams (about 2 pounds, 3 ounces) had no chance of making it. Now, thanks to the advances in neonatology, many babies who are born even smaller than that can be expected to survive (see box). Which means the odds of your baby coming home well from her hospital stay are very much in her favor.
Overall, better than two out of three babies born prematurely will turn out to be perfectly normal, and most of the others will have only mild to moderate disabilities. Most often the baby’s IQ will be normal, though preterm infants do have an increased risk of learning challenges. The risks of permanent development issues are much greater for those who are born at 23 to 25 weeks and/or weigh less than 25 ounces. Still, of the 40 percent of these infants who survive, more than half do well.
As your baby grows, it will be important to keep in mind that she will have some catching up to do before her development reaches the normal range for her birth age. Her progress is likely to follow more closely that of babies of her adjusted age (see next question). If she was very small, or had serious complications during the neonatal period, she is very likely to lag behind her corrected age mates, too, particularly in motor development.
It may also be slower going in the neuromuscular department. Some preemies may not lose those telltale newborn reflexes such as the Moro, tonic neck, or grasp reflexes (click here) as early as term infants do, even taking adjusted age into account. Or their muscle tone may be weak, in some cases causing the head to be floppy, in other cases causing the legs to be stiffer than normal and the toes to point. Though such signs may signal something’s wrong in full-term babies, they’re usually nothing to worry about in pretermers (but do have them evaluated by the doctor).
Slow developmental progress is definitely to be expected in a preemie, and is not usually a cause for concern. If, however, your baby seems not to be making any progress week to week, month to month, or if she seems unresponsive (when she’s not ill), speak to her doctor. If a problem is discovered, the early diagnosis could lead to early treatment, which may make a tremendous difference in the long term.
“Our son, who was born nearly 2 months early, seems very far behind compared with other 4-month-olds. Will he ever catch up?”
Your little guy’s probably not “behind” at all. In fact, he’s probably just where a baby conceived when he was should be. Traditionally, a baby’s age is calculated from the day he was born. But this system is misleading when assessing the growth and development of premature infants, since it fails to take into account that at birth they have not yet reached term. Your baby, for example, was just a little more than minus 2 months old at birth. At 2 months of age he was, in terms of gestational age (calculated according to his original due date), equivalent to a newborn. At 4 months, he’s more like a 2-month-old. Keep this in mind when you compare him with other children his age or with averages on development charts. For example, though the average baby may sit well at 7 months, your child may not do so until he’s 9 months old, when he reaches his seventh-month corrected age. If he was very small or very ill in the newborn period, he’s likely to sit even later. In general, you can expect motor development to lag more than the development of the senses (vision and hearing, for example).
Experts use the gestational age, usually called adjusted or corrected age, in evaluating a premature child’s developmental progress until he’s 2 to 2½ years old. After that point, the 2 months or so differential tends to lose its significance—there isn’t, after all, much developmental difference between a child who is 4 years old and one who is 2 months shy of 4. As your baby gets older, the gap between his adjusted age and his birth age will likely diminish and finally disappear, as will any developmental differences between him and his peers (though occasionally, extra nurturing may be needed to bring a preemie to that point). In the meantime, if you feel more comfortable using his adjusted age with strangers, go ahead (they’ll never know the difference). Certainly do so when looking at your baby’s developmental progress.
You can encourage motor development by placing your baby on his tummy, facing outward toward the room rather than toward the wall, as often and for as long as he’ll put up with it (but only when he is carefully supervised). Since preemies and low-birthweight babies spend most of their early weeks, sometimes months, on their backs in isolettes, they often resist this “tummy-to-play” position, but it’s a necessary one for building arm and neck strength. Tummy time on your tummy or chest may be more fun for both of you … plus you’ll both reap the benefits that come from such kangaroo care if you do it skin-to-skin.
“My baby seems way too small for the infant car seat. Wouldn’t she be safer in my arms?”
It’s not only unsafe but illegal for a baby (premature or full-term) to ride in somebody’s arms rather than in a car seat. Every baby, no matter how tiny, must be buckled up safely, securely, and snugly each and every time she’s in a moving vehicle. But parents of low-birthweight babies often find that their especially little babies seem lost in a standard rear-facing infant car seat. The AAP recommends the following when choosing and using a car seat for your preemie:
• Select a car seat that will fit your baby. Choose an infant car seat, not a convertible seat, and look for one that has less than 5½ inches from the crotch strap to the seat back. This will help keep your baby from slouching. Also, look for one that measures less than 10 inches from the lowest harness strap position to the seat bottom so that the harness won’t cross over your baby’s ears.
• Make it fit even better. Use the newborn insert that comes with the car seat (most infant seats include one) to cocoon your baby. If baby still seems too small to fit, roll a towel or small blanket and arrange it so that it pads the seat at the sides of her head. And if there’s still a big gap between your baby’s body and the harness, use a folded towel or blanket to fill it in (but don’t place one under baby).
Also consider having a certified car seat installation technician check how your preemie fits into her car seat—to make sure she’s getting the support she needs and is seated safely, as well as to show you how to make any necessary adjustments. (Search on nhtsa.gov/apps/cps/index.htm for a location near you.)
Some premature babies have trouble breathing in the semipropped position the seat requires. One study has shown that these infants may show a decreased oxygen supply while riding in a car seat, and that this deficit may last for as long as 30 minutes or more afterward. Some may also experience short periods of apnea (breathing cessation) in car seats. Make sure your baby is observed and monitored in the car seat by the hospital staff before going home. If she does experience breathing problems in a car seat, it’s best to limit the amount of auto travel you do with her for the first month or two at home (or use an approved car bed), especially if she has had spells of apnea previously. Ask her doctor about monitoring her breathing when she’s in an ordinary car seat, at least for a while, to see if she is experiencing any problems.
The same breathing problems may occur in young premature babies in infant seats and baby swings, so don’t use either without the doctor’s approval.
Prematurity is risky business. Tiny bodies are not fully mature, many systems (heat regulatory, respiratory, and digestive, for example) aren’t yet fully operative, and not surprisingly, the risk of neonatal illness is increased. As the technology for keeping such babies alive improves, more attention is being given to these common preemie conditions, and completely successful treatment is becoming more and more the norm for many of them. (New treatments are being developed almost daily and so may not be detailed here, so be sure to ask your neonatologist or pediatrician about recent advances.) The medical problems that most frequently complicate the lives of preterm infants include:
Respiratory distress syndrome (RDS). Because of immaturity, the premature lung often lacks pulmonary surfactant, a liquid that coats the inside of the lungs and helps keep the air sacs (alveoli) in the lungs from collapsing. Without surfactant the tiny air sacs collapse like deflating balloons each time baby breathes out, forcing him or her to work harder and harder to breathe. This is called RDS. Interestingly, babies who have undergone severe stress before birth, usually during labor and delivery, are more likely to have surfactant, since the stress appears to speed lung maturation.
RDS, the most common lung disease of premature infants, was once frequently fatal, but more than 80 percent of babies who develop RDS today survive, thanks to an increased understanding of the syndrome and new ways of treatment. Extra oxygen is given via a plastic oxygen hood, or via continuous positive airway pressure (CPAP), which is administered through tubes that fit into the nose or mouth. The continuous pressure keeps the lungs from collapsing until the body begins producing sufficient surfactant, usually in 3 to 5 days. With severe RDS, a breathing tube is placed in the mouth and the baby is put on a respirator. Artificial surfactant is then administered directly to the baby’s lungs via the breathing tube. Sometimes, when lung immaturity is detected in utero, RDS can be prevented entirely by the prenatal administration of a hormone to the mother, to speed lung maturation and production of surfactant.
A mild case of RDS usually lasts for the first week of life, though if the baby must be placed on a respirator, the recovery may be much slower. Babies with severe cases of RDS may be at an increased risk of colds or respiratory illnesses during their first 2 years of life, and may be more likely to experience childhood wheezing or asthma-like illnesses and be hospitalized in their first 2 years.
Bronchopulmonary dysplasia (BPD). In some babies, particularly those born very small, long-term oxygen administration and mechanical ventilation used to help treat RDS appear to combine with lung immaturity to cause BPD, or chronic lung disease. The condition, which results from lung injury, is usually diagnosed when a newborn still requires increased oxygen after reaching 36 weeks gestation and lung changes (such as scarring) are seen on x-rays. Babies with BPD have to work harder than other babies to breathe, and breastfeeding or bottle-feeding makes them work especially hard. Because they end up using so many calories when they exert themselves to breathe, and because they have a harder time eating, babies with BPD often have nutritional challenges such as poor weight gain.
BPD is a chronic condition, and the only cure is giving it time, since over time, new healthy lung tissue will grow and the symptoms will ease. That’s why treatment is only to lessen the symptoms of the condition while the lungs grow and mature. Treatment can include extra oxygen, continued mechanical ventilation, medications such as bronchodilators (to help open the airways) or steroids (to reduce inflammation), and medication to prevent RSV (respiratory syncytial virus; click here) prevention medication. Some babies will require oxygen at home, and all require a high caloric intake to improve growth. Happily, most babies with BPD outgrow their symptoms and lead healthy lives.
Apnea of prematurity. Though apnea (periods when breathing stops) can occur in any newborn, the problem is much more common among premature infants. Apnea of prematurity occurs when immature respiratory and nervous systems cause preterm babies to stop breathing for short periods. It is diagnosed when a baby has such periods that last more than 20 seconds or shorter ones that are associated with bradycardia, a slowing of the heart rate. It is also considered apnea if the cessation of breathing is associated with the baby’s color changing to pale, purplish, or blue. Almost all babies born at 30 weeks or less will experience apnea.
Apnea is treated by stimulating the infant to start rebreathing by rubbing or patting the baby’s skin, administering medication (such as caffeine or theophylline), or using continuous positive airway pressure (CPAP), in which oxygen is delivered under pressure through little tubes into the baby’s nose. Apnea of prematurity is not associated with SIDS (Sudden Infant Death Syndrome), and many babies will outgrow it by the time they reach 36 weeks gestation. If a baby has breathing pauses after apnea has been outgrown, it is not considered apnea of prematurity and is more likely caused by some other problem.
Patent ductus arteriosus. While baby is still in the uterus, a duct called the ductus arteriosus connects the aorta (the artery through which blood from the heart is sent to the rest of the body) and the main pulmonary artery (the one leading to the lungs). This duct shunts blood away from the nonfunctioning lungs and is kept open during pregnancy by high levels of prostaglandin E (one of a group of fatty acids produced by the body) in the blood. Normally, levels of prostaglandin E fall at delivery, and the duct begins to close within a few hours. But in about half of very small premature babies (those weighing less than 3 pounds, 5 ounces), and in some larger babies, levels of prostaglandin E don’t drop, and the duct remains open or “patent.” In many cases there are no symptoms, except a heart murmur and a little shortness of breath on exertion and/or blueness of the lips, and the duct closes by itself soon after birth. Occasionally, however, severe complications occur. Treatment with an antiprostaglandin drug (indomethacin) is often successful in closing the duct. When it isn’t, surgery will do the job.
Retinopathy of prematurity (ROP). The blood vessels in the eyes are not fully developed until about 34 weeks gestation. When babies are born too early, the immature blood vessels in the retinas sometimes begin to grow too quickly, damaging the retina. Retinopathy of prematurity (ROP) is the name for the improper growth of the blood vessels on the retina and the damage caused by that growth. In most preemies, the growth of the retinal blood vessels will slow down on its own, and vision will develop normally. The incidence of ROP increases as birthweight decreases. More than half of babies born weighing less than 2 pounds, 12 ounces (1,250 grams) will develop ROP, most often mild. Severe retinopathy of prematurity is largely a problem of those babies born before 28 weeks.
Most cases of ROP will get better on their own, requiring no treatment, and the babies will recover with no lasting visual problems. But since ROP can sometimes lead to scarring and distortion of the retina, increased risk of nearsightedness, wandering eye, involuntary rhythmic movements of the eye, and even blindness, a newborn with ROP will be seen by a pediatric ophthalmologist. Infants with severe ROP may require treatment (laser therapy, cryotherapy, or surgery) to stop the progression of the abnormal vessels.
Intraventricular hemorrhage (IVH). IVH, or bleeding in the brain, is extremely common among premature infants because the vessels in their developing brains are very fragile and can bleed easily. Intraventricular hemorrhage most often affects preemies weighing less than 3 pounds, 5 ounces, usually within the first 72 hours of life. The most severe hemorrhages (which affect only 5 to 10 percent of extremely premature babies) require close observation to correct any further problems that develop—for example, hydrocephalus (blockage of spinal fluid). Regular follow-up ultrasounds are usually ordered for such hemorrhages until they are resolved. Unfortunately, there is no way to stop an intraventricular hemorrhage once it has begun. In mild cases (and most cases are), the blood is absorbed by the body. In a less mild case, the treatment targets symptoms of the bleed instead of the bleed itself. The good news is that in most mild cases the follow-up ultrasound of the head is normal and the baby’s development is normal for a preterm baby.
Necrotizing enterocolitis (NEC). NEC is a condition where the intestines become infected and can begin to die. If the disease is not treated promptly, a hole can form through the bowel wall, spilling the bowel’s contents into the abdominal cavity. No one knows for sure what causes NEC, but because the more premature a baby is, the greater the risk of NEC, doctors speculate that the intestines of very premature babies are not developed enough to completely handle digestion. Delaying feedings doesn’t seem to prevent the condition, but babies fed breast milk usually are at less risk of NEC (breast milk has protective factors that encourage good intestinal development and reduce the amount of harmful bacteria in the intestines). The symptoms of this serious bowel disease include abdominal distension, vomiting, apnea, and blood in the stool. A baby with necrotizing enterocolitis is usually put on intravenous feedings (to let the bowels rest) and antibiotics (to treat the infection). If there is serious deterioration of the intestine, surgery is usually performed to remove the damaged portion. Unfortunately, preemies who are medically or surgically treated for NEC may have growth delays, trouble absorbing nutrients, and trouble with their livers and gall bladders. NEC also seems to increase the risk of developmental delays.
Anemia. Many premature infants develop anemia (too few red blood cells) because their red blood cells (like those of all babies) have a shorter life than red blood cells of adults, they make few new red blood cells in the first few weeks of life (like all infants), and the frequent blood samples that must be taken from the baby to do necessary laboratory tests make it difficult for red blood cells to replenish. Anemia is also more common in preemies because they missed out on the transfer of iron from their moms that happens during the last weeks of pregnancy and because the bone marrow process that makes new red blood cells is immature in preemies.
Mild anemia may not need treatment if the number of red blood cells is enough to carry oxygen to meet the baby’s needs. More serious anemia is usually treated by blood transfusions, iron supplementation, and limiting the amount of blood drawn to only what is necessary. Since preemies, whether they’re anemic or not, are born with low levels of iron, they are usually given iron supplements to help build up the reserves necessary to produce red blood cells.
Infection. Premature infants are most vulnerable to a variety of infections because they are born before the transfer of disease-fighting antibodies from the mother that normally occurs toward the end of pregnancy. Preemies also have an immature immune system, making it more difficult to fight germs, including those that are inadvertently introduced via feeding tubes, IV lines, and blood tests. Among the infections preemies are more likely to come down with are pneumonia, urinary tract infections, sepsis (infection of the body or bloodstream), and meningitis. Babies whose blood, urine, or spinal fluid cultures come back positive for signs of infection are treated with a full course of IV antibiotics, which usually helps resolve the infection and puts baby on the right track back to health again.
Jaundice. Premature babies are much more likely to develop jaundice than are full-term infants. Also, their bilirubin levels (the measure of jaundice) are likely to be higher and the jaundice longer lasting. Read about the condition here.
Hypoglycemia. Premature and low-birthweight babies often have low blood sugar or hypoglycemia. But since the brain depends on blood glucose as its main source of fuel, it’s crucial that a baby’s blood sugar gets regulated as soon as possible so that it doesn’t lead to serious (and rare) complications such as brain damage. Problem is, hypoglycemia may not be obvious in newborn babies because the symptoms are hard to pinpoint. Luckily a simple blood test for blood glucose levels can diagnose hypoglycemia, and treatment is straightforward and works well. Treatment includes a rapid-acting source of glucose, which may be as simple as giving baby a glucose/water mixture intravenously or early feedings of formula or breast milk, if baby is well enough to feed. Breast milk is considered as beneficial as formula in treating hypoglycemia. Blood glucose levels are closely monitored after treatment to see if the hypoglycemia occurs again, and if it does, treatment will resolve the issue once again with no long-lasting negative results.