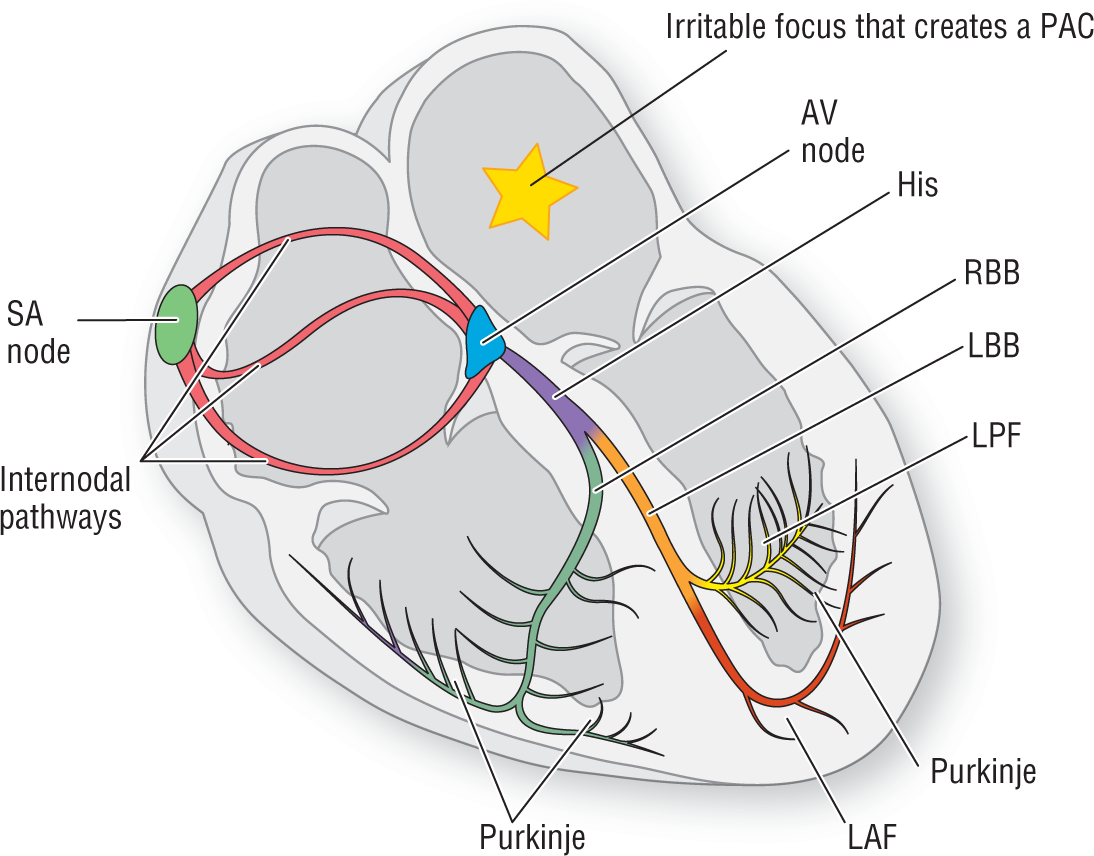
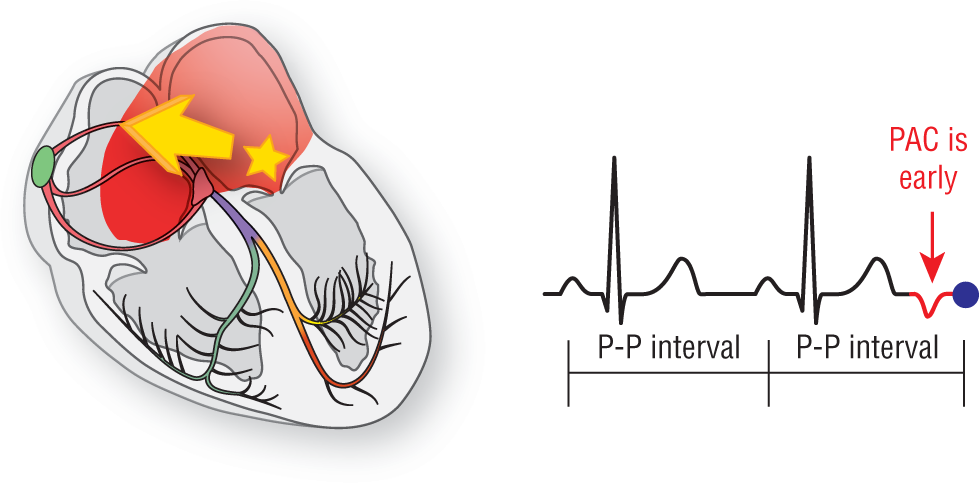
A premature atrial contraction (PAC) refers to an impulse or complex that occurs earlier than expected and originates in an atrial focus, not in the sinoatrial (SA) node (Figure 13-1). PACs typically occur when a small area of the atria is more irritable than the rest of the atrial tissue (Figure 13-2). The irritability increases the intrinsic pacing rate for the potential ectopic focus in the area, and, eventually, one fires off earlier than the sinus node.
Figure 13-1 An irritable focus, represented by the yellow star, acts as a pacemaker and causes an impulse to occur sooner than would ordinarily be expected. This creates the typical characteristics of a PAC as represented in Figure 13-2.
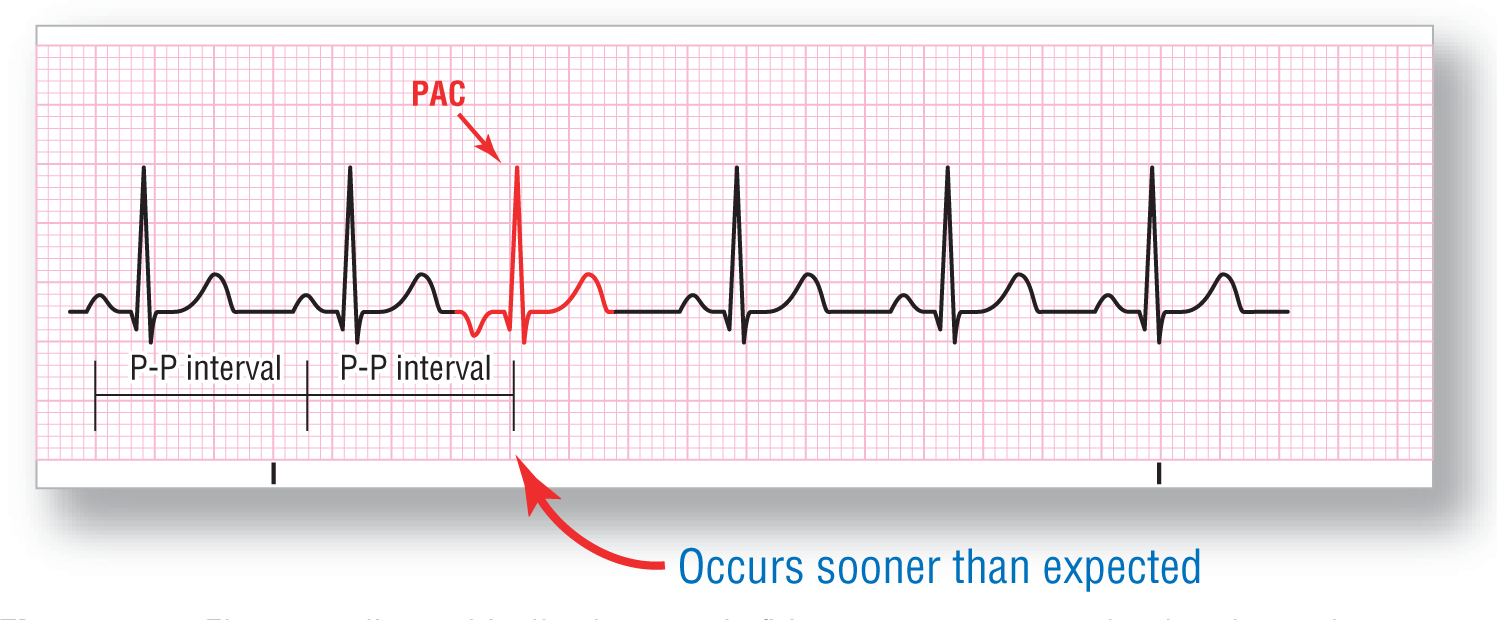
Figure 13-2 Electrocardiographically, the ectopic firing causes an event that breaks up the underlying regular rhythm. The PAC has a P-P interval that is shorter than expected and a different P-wave morphology and PR interval because it does not originate in the SA node. Let’s see why this occurs.
PACs are normally clinically insignificant. Since they occur intermittently, the slight alterations in the timing of the mechanical contractions of the heart that are produced are usually not enough to affect hemodynamics to any great degree. However, under certain circumstances (frequent PACs, valvular disorders, heart failure), the inappropriate filling of the ventricles caused by the early complexes can cause slight, but clinically significant, alterations in the cardiac output and blood pressure. These hemodynamic changes are typically not life threatening but can lead to light-headedness, palpitations, and a feeling of fluttering in the chest.
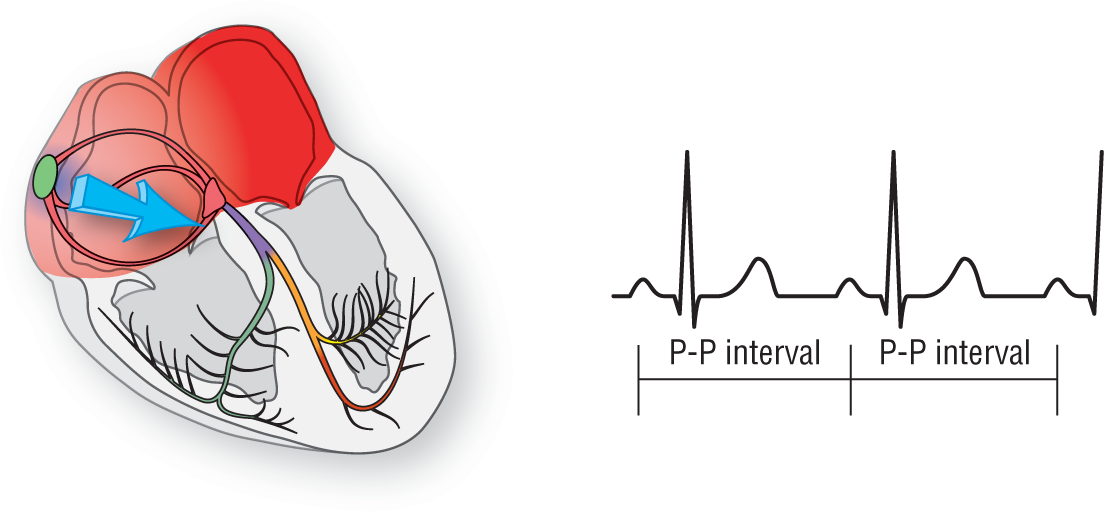
Earlier, in Chapter 8, Normal Sinus Rhythm, we saw how normal sinus rhythm (NSR) was formed. The regularity of the rhythm was set by the fastest pacemaker, the SA node (Figure 13-3). The stability of a sinus nodal origin of the impulse creates a consistency in the P-P interval on the ECG. In addition, since the P wave always originates in the sinus node, the P waves in NSR all have the same morphology and are upright in leads II, III, and aVF.
Figure 13-3 The SA node normally sets the rhythm, creating consistent P-P intervals.
Normally, the pacemaking function of the atrial tissue is set at a slower rate than that of the SA node (usually around 55–60 BPM). The result is that, as the more frequent sinus impulses wash over the focus represented by the yellow star, the pacemaking function of the focus is continuously reset and it, therefore, never fires (Figure 13-4).
Figure 13-4 The faster SA node usually fires before an ectopic focus gets the chance.
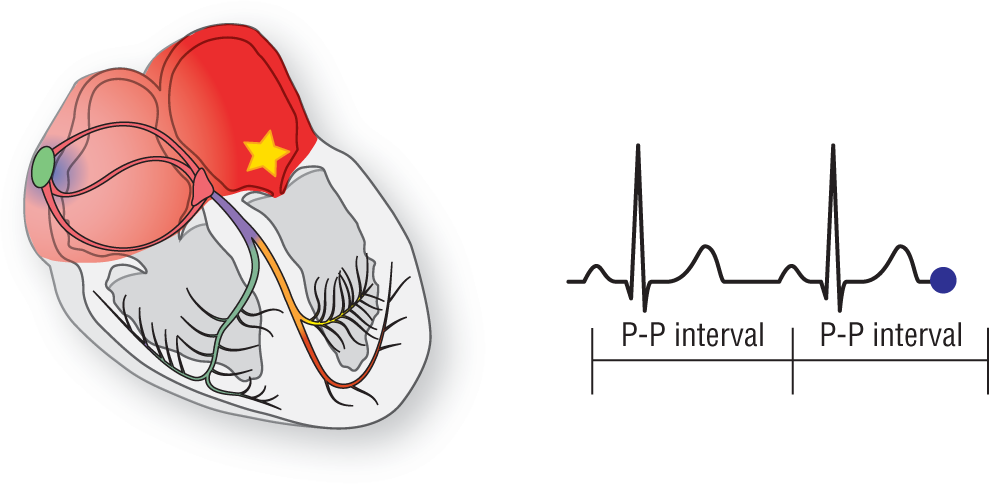
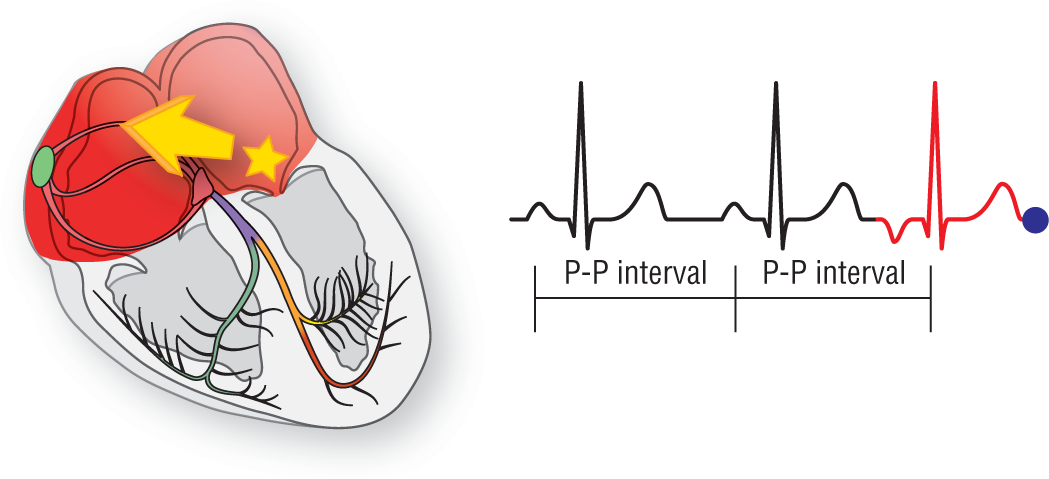
Every once in awhile, however, an ectopic focus in the atria becomes irritable and fires early. This premature impulse leads to an early contraction of the heart and, hence, a PAC (Figure 13-5). Note that the impulse of the PAC moves in a different direction and route than that taken by a sinus impulse. In this case, the depolarization wave travels upward and to the left.
Figure 13-5 When an ectopic focus fires early, the heart contracts early and a PAC results.
The abnormal vector caused by the depolarization wave from an ectopic focus causes a different P-wave morphology to be formed (Figure 13-6). In addition to the P wave, the PR interval also has to be different because of the different route taken by the wave. After the PAC, the SA node should once again take over its primary role as the main pacemaker.
Figure 13-6 The ectopic focus creates a PAC and a different P-wave morphology.
The ventricular portion of the impulse proceeds normally along the electrical conduction system of the heart once it reaches and leaves the atrioventricular (AV) node. This gives rise to a normal, narrow QRS complex that is identical to the ones seen in NSR. The only exceptions to the rule occur when there is a preexisting bundle branch block, some electrolyte abnormality, or some aberrancy in conduction because the premature impulse could not get through an area of the conduction system that is still refractory. We will discuss this a bit further when we get to the rhythm strips themselves. For now, just remember that in PACs, the QRS complexes are usually narrow.
In addition to the information discussed earlier, the formation of a PAC allows us to examine some basic concepts of arrhythmia recognition in greater detail. These include the P-wave axis, the PR interval, the pauses, and aberrancy. These are critical concepts in the analysis of any arrhythmia, and a thorough understanding of these principles is vital to your continued success.
NOTE
We need to clear up a problem with the nomenclature. In today’s literature, many terms are used to describe an atrial complex that arrives prematurely. These include premature atrial contractions, premature atrial complexes, atrial premature contractions, and atrial premature depolarizations, just to name a few. Presently, there is no consensus on which is the best label to place on these events. We are going to stick to the old tried and true term premature atrial contraction (PAC). Be aware that all of these terms refer to the same electrocardiographic event. This same nomenclature issue will also apply to premature junctional contractions (PJCs) and premature ventricular contractions (PVCs).