Now that you understand the basic principles of a wandering atrial pacemaker (WAP), let’s turn our attention to its closely related family member: multifocal atrial tachycardia (MAT). Remember when we were discussing normal sinus rhythm and sinus tachycardia, we mentioned that these were basically the same rhythm but at different points along a heart rate or beats-per-minute (BPM) spectrum. The same is true of WAP and MAT. They are basically the same rhythm but with different ranges of rates: WAP is at or below 100 BPM, and MAT is over 100 BPM.
Basically, MAT is a rapid tachycardia usually with heart rates between > 100 and 150 BPM (but can be as high as 250 BPM) that is caused by the chaotic firing of at least three different ectopic atrial pacemaking sites (Figure 18-1). The result is an irregularly irregular or chaotic rhythm with varying P-wave morphology, PR intervals, and P-P or R-R intervals (Figure 18-2). Due to the increased rate of firing of the pacemakers in this tachycardic rhythm, fusions and aberrancy are much more common than in WAP.
Figure 18-1 At least three individual pacemaker sites are at work in creating a completely chaotic and tachycardic rhythm. Each site is associated with an individual P-wave morphology and PR interval just as in WAP.
Figure 18-2 The ECG strip in MAT shows multiple P-wave morphologies, PR, P-P, and R-R intervals throughout the strip. There are more fusions of the P waves with the previous T waves and an increase in aberrantly conducted QRS complexes because of the tachycardia.
While we are on the topic of heart rates in the irregularly irregular rhythms, since WAP and MAT are both chaotic rhythms, their rates may momentarily cross from the normal to the tachycardic ranges and vice versa. For example, a strip that contains mostly P-P intervals in the 60- to 80-BPM range may have one or two complexes that are being transmitted at a rate of 120 BPM. This strip would still be considered WAP and not MAT just because of the few variations noted. Likewise, a strip with the majority of the complexes occurring in the 100- to 120-BPM range but that has a momentary slowdown should not be called WAP.
When you are considering WAP or MAT, you need to consider the overall rate of the rhythm strip and the presentation of the majority of the complexes. If the overall rate of the strip (as discussed in Chapter 3, Paper, Tools, and Calculating Rates), obtained by multiplying the number of complexes in a 6-second strip by 10 is over 100 BPM, then the rhythm is MAT. If the overall rate is below 100 BPM, then the rhythm is WAP.
Fusion of the complexes, mostly the P and T waves, is very common in MAT. As you can imagine, three or more pacemakers firing chaotically and rapidly causes a lot of overlap between the cycles. The net result is an increased number of buried P waves, P waves occurring on T waves, P waves occurring on QRS complexes, and even blocked P waves (Figure 18-3).
Figure 18-3 ECG strip A is an example of a wandering atrial pacemaker. The slight area of tachycardia is not enough to bring the overall rate above 100 BPM, nor are the majority of the complexes in the tachycardic range. ECG strip B is an example of MAT. Note that the majority of the strip is tachycardic and that the overall rate of the strip is above 100 BPM.
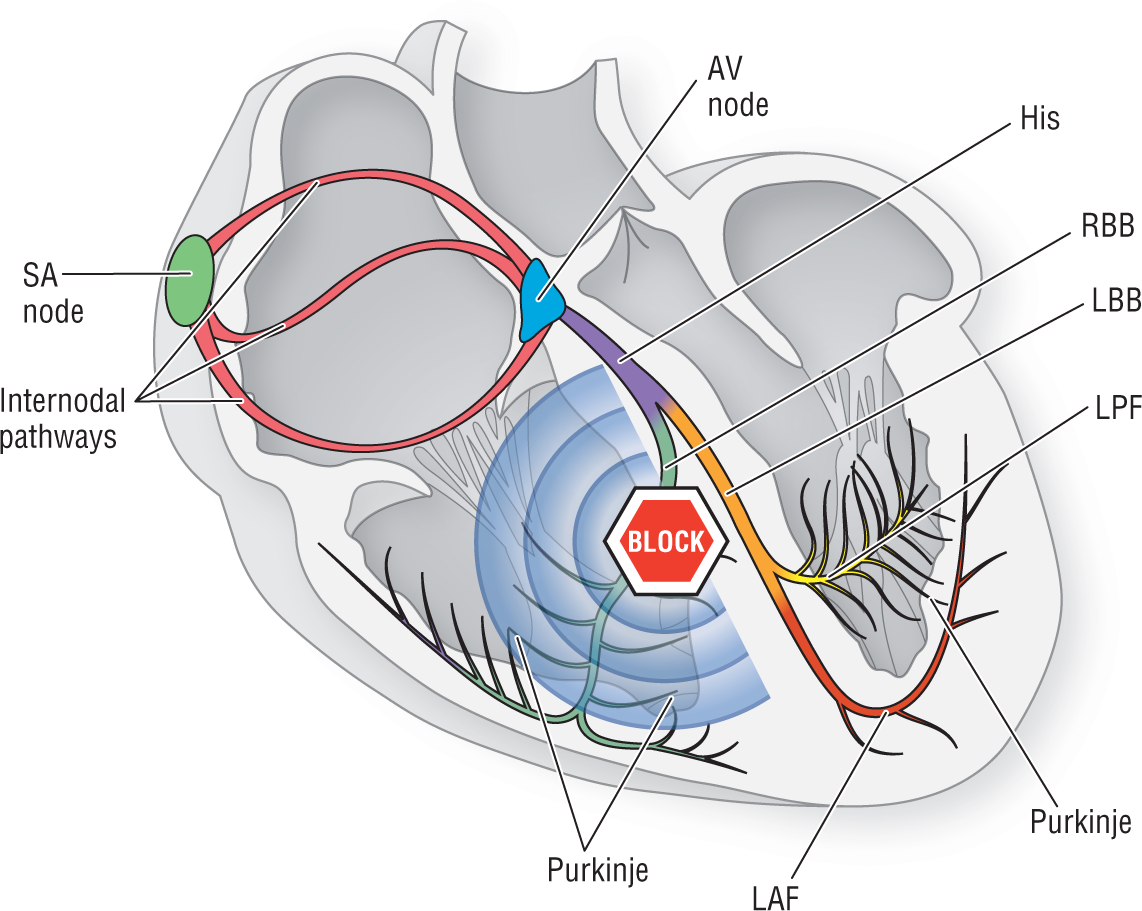
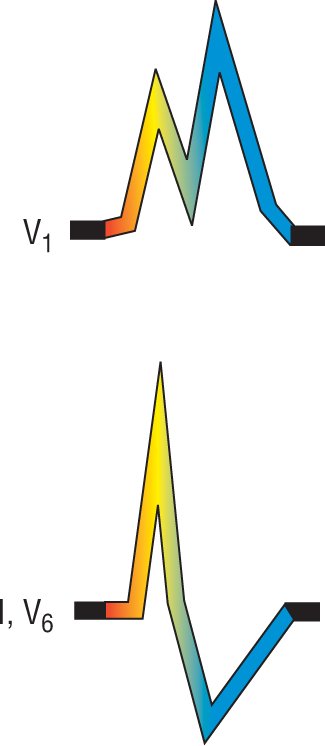
In addition to these fusions, aberrancy in the morphology of the QRS complex is also very commonly encountered in MAT. This occurs because the chaotic tachycardia causes many impulses to fall on the absolute and relative refractory period of the conduction system. As we mentioned, the right bundle branch block (RBBB) has an especially long refractory period and is very susceptible to block the impulse from being transmitted normally down to the ventricles (Figures 18-4 and 18-5). The net result is a wide QRS complex with a morphology consistent with a right bundle branch block pattern. Left bundle branch block pattern can also occur in aberrancy, but it is less common than RBBB.
Figure 18-4 When the impulse hits a refractory area in the right bundle branch, the impulse is forced to continue by direct cell-to-cell transmission throughout the rest of the right ventricle.