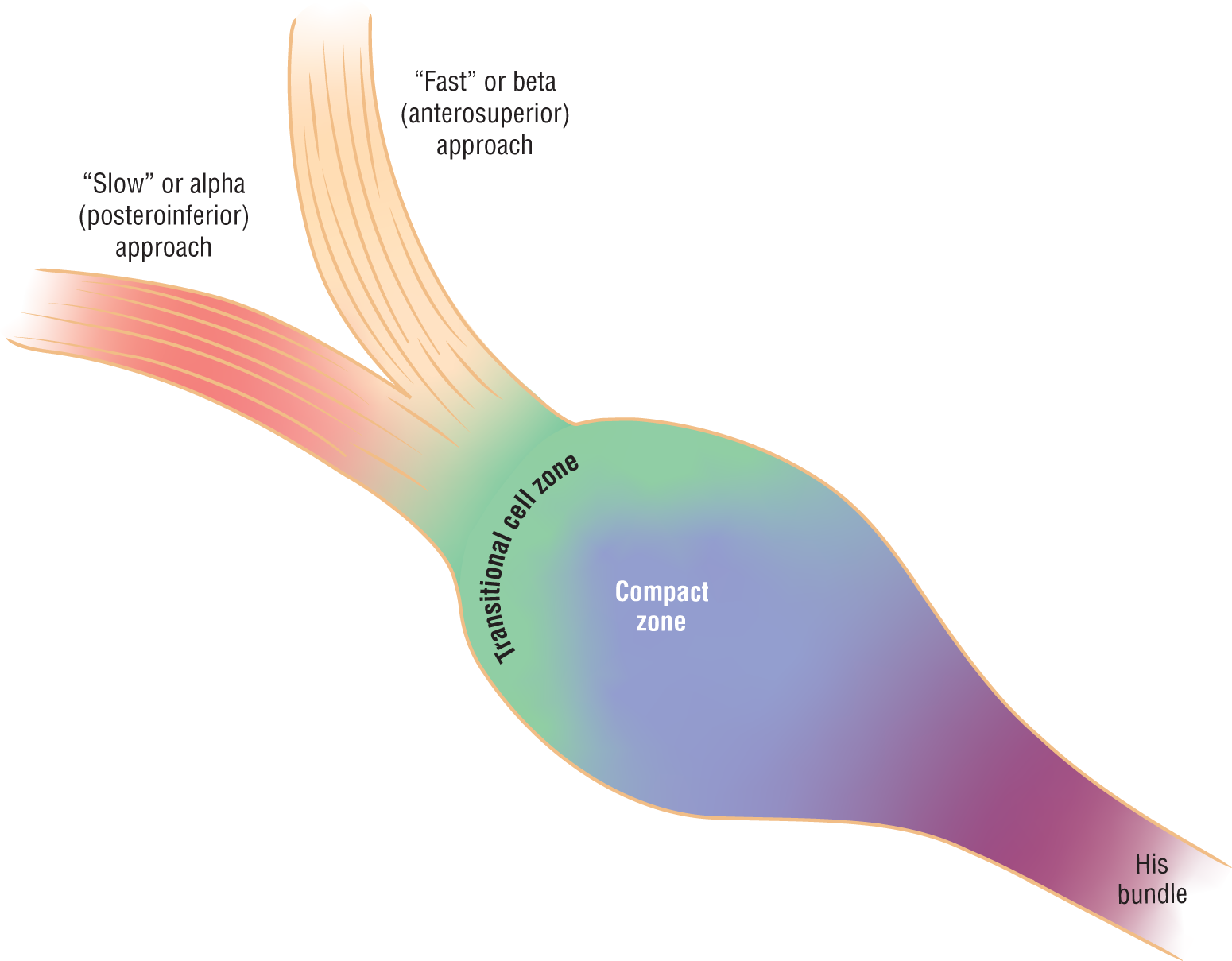
In Chapter 21, Introduction to Junctional Rhythms, and in the previous section, we talked about the anatomy of the AV node. We saw that most people have a single area of nonspecialized tissue that approaches the AV node. But sometimes people have two separate approaches instead of one. These approaches are surrounded by nonconductive tissue and are, therefore, isolated from each other and the rest of the myocardium. Figure 25-10 is a graphic representation of the AV junction accentuating the two approaches or tracts leading up to the AV node.
Figure 25-10 The AV junction is composed of one or two approaching tracts separated by fibrous, nonconductive tissue and three separate zones in the AV node. For our discussion, the graphic represents the two approaches or tracts that can create arrhythmias.
Instead of allowing the two tracts to depolarize the AV node from two different impulses, the two tracts unite to form a single common pathway immediately before reaching the AV node. Note that the fusion of these two tracts takes place immediately before the AV node.
So, why are we emphasizing that the fusion of the tracts occurs before the AV node? Because it is in this short area of fusion where the circus movement that creates AVNRT is born. In essence, this small area, where the two tracts fuse together to form the final common pathway, becomes the battleground that decides which tract’s impulse will be transmitted to the AV node. Which one will win? That honor lies with the tract that wins the race: either the fast tract or the slow tract.
Now, let’s look at all the events that occur in this area in a very short time. First, the impulse reaches the “semicircular battleground” and causes the final pathway to depolarize and fire, transmitting that impulse forward to the AV node. In Chapter 8, Normal Sinus Rhythm, we discussed the principle of absolute refractoriness and the absolute refractory period. There, we mentioned that all cardiac cells enter a state of absolute refractoriness immediately after they depolarize, preventing them from transmitting any subsequent impulses until the cells recover (signaling the end of the absolute refractory period). So, what happens to the impulses that arrive to an area in the absolute refractory period? Well, they would simply fizzle out. That is exactly what happens to the impulse that arrives in second place in a two-tract system; the impulse simply fizzles out.
As you will see later in this chapter, understanding this concept is critical to understanding how circus movements are created, including the ones that trigger an AVNRT.
Some people with the two tracts develop not only an anatomic separation, but a clinically relevant separation that can lead to reentry arrhythmias, specifically AVNRT. The two approaches are located at the base of the right atrium and are known as the fast or beta (anterosuperior) pathway and the slow or alpha (posteroinferior) pathway.
The pathways are functionally, as well as anatomically, different from each other, each with its own respective properties. The fast tract has very rapid conduction times but very slow refractory times. Simply, that means that the fast tract conducts impulses through the pathway very, very quickly but, once it fires, it takes a long time before it is ready to fire again. Think of a sprinter in a track race, giving his all for a short burst of speed and then needing time to recoup strength.
The slow tract has very slow conduction times but very fast refractory times. In other words, it conducts the forward impulse slowly but can conduct another one shortly afterward. This is more like a long-distance runner who can run for long distances with a short recovery time between the various bursts of speed in a race.
Now that we have covered some of the basics, can you predict what would happen when an atrial depolarization wave approaches the two tracts (Figure 25-11)? (Think back on the water model presented earlier in this chapter.)
Figure 25-11 An atrial depolarization wave is approaching the AV junctional tracts. Can you predict what would happen?
The impulse would hit the two approaches simultaneously. The two approaches would then start transmitting the impulse at the same time, but the fast tract would transmit it faster (Figure 25-12). The result is that the fast tract stimulates the AV node and causes the depolarization wave to proceed normally down the bundle of His and on to the ventricular electrical conduction system, causing a nice tight QRS complex. The depolarization wave will also retrogradely travel back up the slow tract. Eventually, the two opposing waves (the normally conducted wave along the slow tract and the retrograde wave) would crash into each other and cancel each other out. The cancellation of the two wavefronts in the slow tract is exactly what occurs 99.99999%+ of the time during a regular sinus or atrial rhythm.
Figure 25-12 The depolarization wave travels down the fast channel faster. The result is that the AV node is depolarized by the impulse from the fast channel. The impulse then begins to spread backward from the AV node to the slow channel. Eventually, the two wavefronts traveling through the slow channel would meet and cancel each other out. Note that only one of the impulses was transmitted to the ventricles.
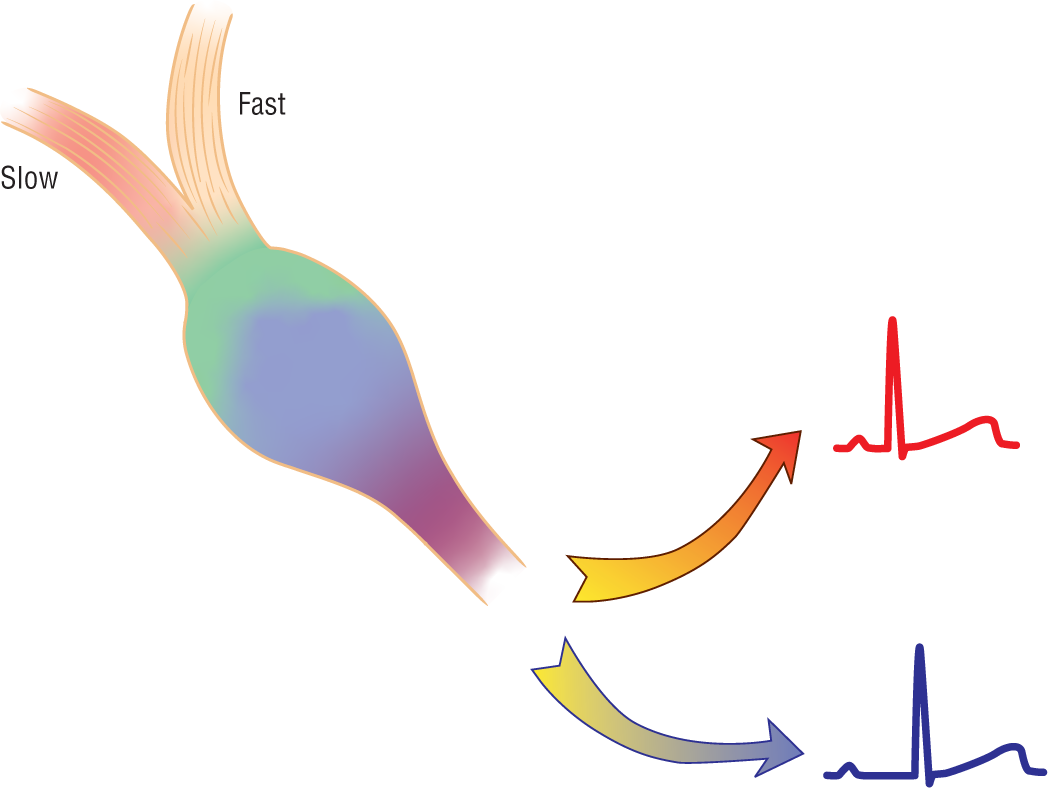
What would happen if, for any reason, the fast tract could not transmit the impulse? To understand what would happen, think about what happened when the tree blocked the fast channel in the water analogy. When the fast tract was obstructed, the water traveled down the slow tract to reach the pond. Likewise, if the fast tract were refractory for any reason, the impulse would be propagated down the slow tract. Would the two complexes look the same? The answer is that the complexes would be identical, except for the PR intervals (Figure 25-13). The PR intervals of the impulses that traveled down the slow tract would be longer than ones that used the fast tract. This is exactly what we see in many patients with a functional two-tract system. They have identical complexes with two different PR intervals present on the same strip. (Note that these two types of complexes are still both sinus complexes, as the variations in the PR intervals are not due to ectopic foci firing but rather to conduction alternating intermittently between the two different tracts.)
Figure 25-13 Depending on which tract transmits the impulse, the PR intervals will vary. This variation can occur beat-to-beat in many circumstances.
AVNRT is formed when a reentry loop is created along the two approaches and the AV node. Here is how the loop is created. Assume that the heart is clipping along at a nice regular pace (Figure 25-14). The impulses are being transmitted “normally” along the two pathways. Immediately after being depolarized, the two tracts would be refractory to any further impulse propagation for a short time.
Figure 25-14 A normal sinus depolarization wave arrives at the two tracts. The fast tract transmits the impulse through as expected and as shown in the graphic. The premature impulse would then arrive, and this sequence is shown in Figure 25-15.
Now let’s suppose that an ectopic atrial focus fires prematurely, causing a premature atrial contraction (PAC; see Figure 25-14). Will the fast tract be ready to handle the PAC? Will the slow tract be able to handle the PAC?
When the PAC hits the two tracts (Figure 25-15), it would find the slow tract ready to accept it because of its faster recovery time, but the fast tract would still be refractory to any new impulse due to its intrinsically slow recovery time. In other words, the PAC reached the fast tract when it was refractory and functioning exactly as the log did in our water model. Due to the obstruction to flow in the fast tract, the impulse would have to be conducted to the AV node through the only way possible—the slow tract. (Note that the PR interval found in this PAC would be wider than normal, reflecting the additional time needed for the impulse to be conducted through the slow tract.)
Figure 25-15 By the time the PAC arrives at the two tracts, the fast tract is refractory and the impulse must proceed through the slow tract. When the impulse reaches the AV node, it begins to fire retrogradely through the now nonrefractory fast tract.
As we saw before, once the depolarization wave stimulates the AV node, it would begin to return retrogradely up the fast tract (see Figure 25-15). The reason that the fast tract would now be able to handle the new impulse is because it took additional time for the wave to travel through the slow tract. The extra time allowed the fast tract to work through its slower refractory period, allowing it to be ready to receive the new retrograde impulse.
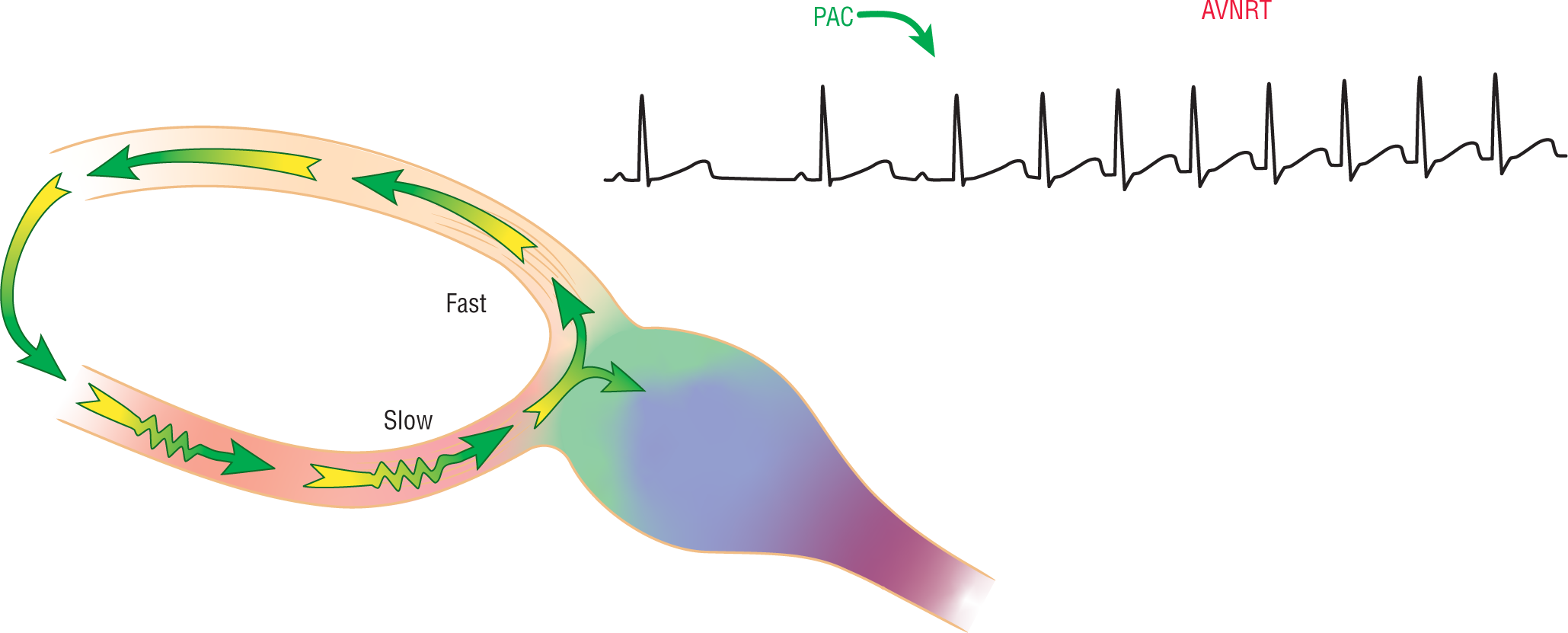
At this point, the retrograde wave can traverse the entire fast tract retrogradely without meeting any obstruction. When the retrogradely spread impulse reaches the other end of the fast tract, it spreads quickly over to the slow tract (Figure 25-16). Remember, electricity, like water, spreads whenever it can and wherever it can. At this point, we have completed a complete loop. What do you think happens at this point?
Figure 25-16 The PAC triggers a circus movement involving both tracts and the AV node. The resulting reentry circuit leads to the formation of a rhythm known as AVNRT. Note the pseudo-S pattern at the end of the AVNRT complexes representing the retrogradely conducted P wave.
The slow tract, with its short refractory period, receives the retrograde impulse and transmits it back toward the AV node, which then retrogradely spreads the impulse to the fast tract, which spreads it back to the slow tract . . . and so on, and so on (see Figure 25-16). It is now a reentry circuit or circus movement within the AV junction and the rhythm that is produced electrocardiographically is an AV nodal reentry tachycardia. The PAC was the trigger that started this.