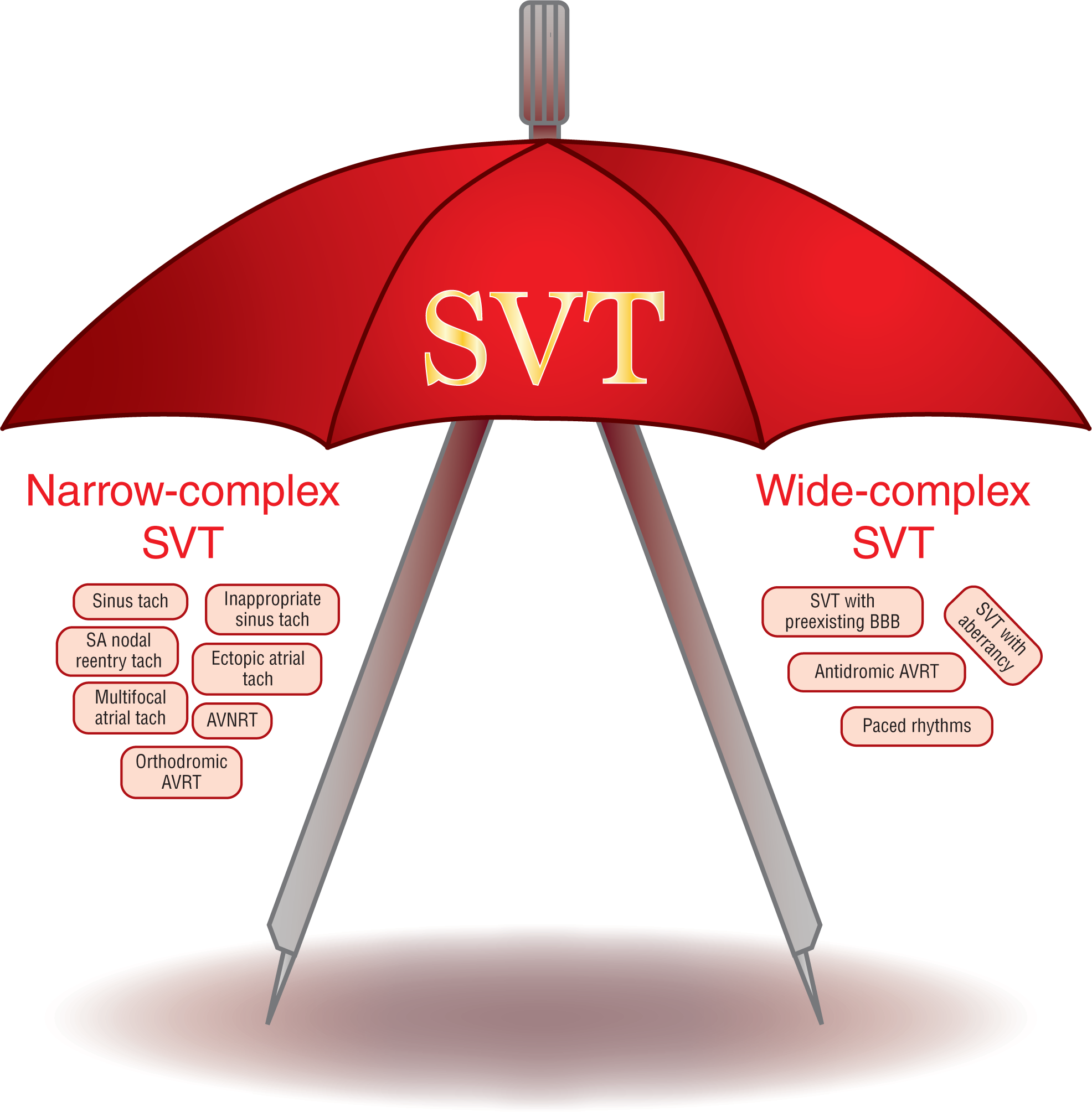
Figure 27-1 Supraventricular tachycardia (SVT) is an umbrella term encompassing both the narrow-complex SVTs and the wide-complex SVTs.
© Jones & Bartlett Learning.
DescriptionWhen we conceptualized this text, we felt that the flow of learning would progress more efficiently if we analyzed the individual rhythms by regions. In that light, we examine the various rhythms that originate above the ventricles individually. For the sake of simplicity, however, practitioners love the concept of encompassing all of those rhythms and grouping them together under one umbrella term, the supraventricular tachycardias (Figure 27-1). In the past, the term paroxysmal SVT was also in favor and reflected the fact that many of these rhythms had rapid onsets and terminations. Since then, the term paroxysmal has fallen out of favor and has been laid to rest. However, the term SVT continues to gain in popularity.
Figure 27-1 Supraventricular tachycardia (SVT) is an umbrella term encompassing both the narrow-complex SVTs and the wide-complex SVTs.
© Jones & Bartlett Learning.
DescriptionFor the past decade or so, focused therapy has been the rage due to the onset of newer, more focused pharmaceutical agents and techniques, along with the establishment of cardiac electrophysiology as a new subspecialty of cardiology. The interest in focused therapy has made sense, since having the ability to target the pathologic mechanism of an arrhythmia means more efficient treatment strategies with less chance of complications. Though it is true that electrophysiologic studies (EPS) and focused treatment protocols have revolutionized the way we understand and treat arrhythmias, these developments have in no way diminished the popularity of the term SVT.
What is the importance of this umbrella term? The various governing and certifying committees have adopted an “If you can’t beat them, join them!” attitude and created new treatment strategies that can safely be used to treat the SVTs as a whole. These simplifications provide a greater safety margin for patients and afford clinicians at all levels of training and experience a more unified approach to emergent treatment that does not require a level of absolute certainty in an exact diagnosis.
If you look at the 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia,1 you quickly see that these authorities have, in essence, created a two-tier level of treatment: (1) treatment of SVTs as a whole in the emergent and acute phase, and (2) focused treatment of the individual rhythm once the patient is more stable. Clinically, this approach makes sense, mainly because it is often difficult (if not impossible) to differentiate between the SVTs in an emergent situation when seconds count. In those cases, treatment can be rapidly started and the patient stabilized. Then, after the patient is hemodynamically stable, further evaluation and study can be instituted to isolate the true arrhythmia and focused therapy can be safely started. As you will see, this is not a perfect system, but it is an elegant compromise.
However, even in well-thought-out systems, things are not as rosy as they seem. To improve our sensitivity to the nuances within these various categories, more and more criteria are surfacing every day. As these criteria are published in the literature, the burden falls on clinicians to learn and use these very cut-and-dried facts. The act of committing these criteria to memory is becoming quite a challenge. Adding to the difficulty of remembering all of these details, many of these rhythms are seldom encountered and “what we don’t use, we lose.”
In the past, many introductory and intermediate books simply gave two paragraphs on this topic and called it a day. Those days are over, and we face a dilemma: Do we look at the individual rhythms, or do we look at the whole group as a single entity? Ethically, we decided to do both—conform to the guidelines and incorporate the additional information on the criteria and algorithms into our chapters. This change has caused us to rethink and restructure these sections. Now, let’s take a look at our solution.
Time is a valuable and, unfortunately, rare commodity in our present society. As such, many medically related texts in use today apply the concept of high-yield learning. The focus is on providing the maximum information in the smallest amount of space. High-yield books are great at familiarizing readers with the material in a concise way without a lot of fluff, or they can be quite useful for review of previously known material. In the olden days, this type of material was simply known as an outline or notes. For the purposes of this chapter and the wide-complex tachycardias section, this approach is quite useful since we have covered much of the material in the prior chapters focusing on the individual arrhythmias. However, to truly learn the material for the first time, you need a little fluff.
The bottom line is that there are many types of readers, and many reasons for reading. Some readers like to cut to the heart of the matter fast and simple; others enjoy a more traditional explanation of the material with analogies, tips, and so forth. Either way, we have your back. Within the context of this text, we’ll provide you with the traditional way to cover the material. If you feel you already have a firm grasp on the material and want to access the basic information quickly or you just need a quick review, we will provide you with that version of the same information in the digital offering that comes with the purchase of this text. Feel free to start off with the system that you feel works best for you, then check out the other one for fun.
To add another level of personalization, we have divided the material in this chapter even further by isolating the basic, intermediate, and more advanced information. If you are familiar with our companion publication, 12-Lead ECG: The Art of Interpretation, you are already familiar with the level system we like to use. In this text, we have broken down this chapter and Chapter 34, Wide-Complex Tachycardia: The Basics, through Chapter 37, Wide-Complex Tachycardia: Putting It All Together, into three levels, as follows:
INTERMEDIATE
ADVANCED
The object is to read the information up to your level of training and understanding, then go back and challenge the next highest level when you are ready. Suppose you are a beginner: Read the information that appears with a white background. Then, after you feel comfortable with that material, try your hand at the intermediate (green) level, and then again at the more advanced (red) level as your command of the material advances. In addition, to make things as easy as possible, we have provided you with some memory techniques (mnemonics) to help you in retaining the material. Though these may appear childish or bizarre, the importance of mnemonics in adult education should not be overlooked.
We would like to point out that as a clinician, you are responsible for following the criteria and the guidelines. All of them. Thus, knowing that the rhythm is an SVT is acceptable for the unstable or urgent patient. However, for the nonurgent period in a stable patient, you should try to focus on a more tailored approach. Otherwise you may get a knock on your door from your licensing board or the firm of Iwillown, Yourhouse, and Carr, Inc.