CASE 41
A 45-year-old man presents for the evaluation of weight gain. He has noticed a 20-lb weight gain in the past few months without any change in his diet or activity level. He has started developing “stretch marks” on his abdomen as well. His wife has noted that even his face seems to be “growing fatter.” Review of systems is significant for complaints of fatigue, multiple recent upper respiratory infections, and the development of facial acne. He has no significant medical history and takes no medications. There is a family history of diabetes and hypertension. On examination, his blood pressure is elevated at 165/95 mm Hg, but his other vital signs are normal. His face is plethoric, and he has a small fatty hump developing on his upper back. His abdomen is obese but soft and nontender without masses or fluid. Skin examination is notable for moderate facial acne and multiple violaceous striae on the abdomen. Blood tests show an elevated glucose level of 150 mg/dL, normal electrolytes, and renal function. His thyroid function tests are normal. You suspect idiopathic Cushing disease and order a dexamethasone suppression test to assist with confirming the diagnosis.
 Which pituitary hormone stimulates the release of adrenocortical steroids?
Which pituitary hormone stimulates the release of adrenocortical steroids?
What is the major glucocorticoid produced in the adrenal glands?
What is the major mineralocorticoid produced in the adrenal glands?
What is the major effect of mineralocorticoids?
ANSWERS TO CASE 41:
Adrenal Cortex
Summary: A 45-year-old man has Cushing disease.
 Pituitary hormonal stimulus of adrenocortical steroid production: ACTH.
Pituitary hormonal stimulus of adrenocortical steroid production: ACTH.
Primary adrenal glucocorticoid: Cortisol.
Primary adrenal mineralocorticoid: Aldosterone.
Major mineralocorticoid effects: Regulation of salt and water balance in the kidney, promote sodium retention, and potassium loss.
CLINICAL CORRELATION
Cushing disease is caused by ACTH-secreting tumors in the pituitary gland. The continuous production of ACTH disrupts the normal circadian production of ACTH and overrides the feedback of adrenal steroids on the hypothalamus and pituitary, resulting in excessive adrenocortical steroid production. Glucocorticoids affect most organs and tissues in the body. Their effects are mediated by specific intracellular glucocorticoid receptors that modulate the transcription rates of specific genes and results in increases or decreases of specific proteins. The major glucocorticoid produced in the adrenal glands is cortisol (hydrocortisone). Glucocorticoids have numerous physiologic effects, including the stimulation of gluconeogenesis, increasing lipolysis, decreasing glucose uptake into fat cells, and redistributing body fat. These effects cause some of the symptoms and signs of Cushing disease, which include glucose intolerance or overt diabetes, weight gain, and increasing truncal obesity. Glucocorticoids also have anti-immune effects, which include decreasing circulating lymphocytes, monocytes, eosinophils, and basophils, increases in circulating neutrophils and atrophy of lymphoid tissue. The excess production of glucocorticoids can therefore lead to immune system suppression and recurrent infections. Under normal physiologic conditions, adrenocortical steroids will exert a negative feedback of ACTH release from the pituitary gland. ACTH release, and subsequent cortisol production, can be suppressed even more by the administration of synthetic steroids such as dexamethasone. ACTH, which is continuously produced by a tumor, will not be suppressed by this feedback mechanism. This formulates the basis for the dexamethasone suppression test, in which a dose of dexamethasone is administered and subsequent cortisol production is measured. Normally dexamethasone administration would cause a reduction of circulating cortisol. In Cushing disease the measurement of cortisol will remain at normal, or even elevated, levels.
APPROACH TO:
Pharmacology of the Glucocorticoids
OBJECTIVES
1. Understand the physiologic regulation of the hypothalamic-pituitary-adrenal axis.
2. List the natural and synthetic adrenocortical steroids, their actions, therapeutic uses, and adverse effects.
3. Know the effects of glucocorticoids and mineralocorticoids.
4. Understand the adrenocortical antagonists, their mechanism of action, uses, and adverse effects.
DEFINITIONS
Glucocorticoids: In humans the most important glucocorticoid is cortisol. These hormones regulate carbohydrate, protein, and lipid metabolism.
Mineralocorticoids: In humans, aldosterone is the most important mineralocorticoid.
Aldosterone: It regulates Na+ and K+ homeostasis.
DISCUSSION
Class
Control of the secretion of glucocorticoids by the adrenal gland is regulated by a classic negative feedback pathway that includes the hypothalamus, pituitary, and the adrenal cortex (see Case 39). The neuropeptide CRH is a 41-amino acid peptide produced in the hypothalamus that is secreted with a circadian rhythm. Secretion can also be increased by physiologic or psychologic stress. CRH acts on the pituitary to stimulate the release of ACTH. ACTH released from the pituitary is transported in the systemic circulation to the adrenal cortex, where it acts to stimulate the zona fasciculata and reticularis to increase the biosynthesis of cortisol and weak androgens such as androstenedione, respectively. It also acts on the zona glomerulosa to slightly stimulate the production of aldosterone. ACTH is a true trophic hormone: it is necessary for the survival of cells of the adrenal cortex, although this effect is somewhat less pronounced in the zona glomerulosa. Cortisol secreted by the adrenal cortex is bound extensively to cortisol-binding globulin (CBG) in the plasma.
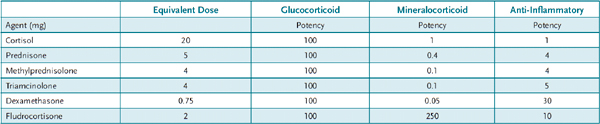
Glucocorticoids Natural and synthetic glucocorticoids play a diverse role in metabolism, catabolism, and immunity. Both cortisol, the natural glucocorticoid, and many synthetic glucocorticoids are used therapeutically (Table 41–1). The synthetic glucocorticoids have reduced mineralocorticoid activity and in general increased potency compared to cortisol. Glucocorticoids have a myriad of therapeutic uses. They are potent anti-inflammatory agents because they stimulate annexin A1. Annexin A1 has a number of anti-inflammatory actions including inhibition of cytokine production, inhibition of prostaglandin production, and inhibition of immune cells. Unlike nonsteroidal anti-inflammatory drugs (NSAIDs), they inhibit leukocytes and macrophages that contribute heavily to inflammation. Glucocorticoids are used to treat joint and bone inflammation, inflammatory bowel disease, bronchial asthma (first-line therapy), and dermatitis. Systemic inflammations such as in lupus erythematosus, rheumatoid arthritis, and acute respiratory distress syndrome are also treated with glucocorticoids. Glucocorticoids are potent immunosuppressive agents and are used either alone or in conjunction with other immunosuppressive agents to suppress organ rejection following transplant, and to reduce the severity of allergic reactions including contact dermatitis, serum sickness, and allergic rhinitis. Other uses include prevention of respiratory distress syndrome in infants (by induction of surfactant), prevention of nephrotic syndrome, and at high doses to reduce cerebral edema. Adrenal insufficiency either acute or congenital is treated with glucocorticoids. Finally glucocorticoids are useful diagnostically as in the dexamethasone suppression test described above.
Table 41–1 • COMMONLY USED ADRENOCORTICAL AGENTS
Although they are highly efficacious agents, the adverse effect profile of glucocorticoids limits their use typically to short (approximately 2 weeks) periods. Chronic use of glucocorticoids beyond this duration produces adrenal suppression and can cause iatrogenic Cushing syndrome. The metabolic sequelae of Cushing syndrome include fat redistribution (buffalo hump and moon facies), hyperglycemia, and elevations in insulin secretion leading to frank diabetes. Continued protein degradation can cause myopathy and muscle wasting, and thinning of the skin that becomes prone to bruising and striae. Immunosuppression leads to susceptibility to infection and poor wound healing. Peptic ulcers and osteoporosis are other potential consequences of glucocorticoid use. Adrenal suppression occurs with chronic glucocorticoid use as a result of continuous suppression of ACTH production by the pituitary. The absence of the trophic hormone leads to adrenal atrophy and an inability to respond to stress, which can be life-threatening. Neurological adverse effects include hypomania, acute psychosis, and depression. At sufficient doses, all glucocorticoids have some mineralocorticoid activity that can lead to electrolyte imbalances and water retention.
Mineralocorticoids Aldosterone is the naturally occurring mineralocorticoid. It is secreted by the zona glomerulosa of the adrenal cortex. Secretion of aldosterone is increased by angiotensin II and K+, especially when serum Na+ is low. The physiologic action of aldosterone is to increase Na+ reabsorption in the distal convoluted tubule and cortical collecting tubule via the amiloride-sensitive Na+ channel. As Na+ is reabsorbed, K+ or H+ is secreted into the urine and water is retained. Aldosterone also causes Na+ reabsorption in the salivary and sweat glands and the mucosa of the gastrointestinal (GI) tract. Aldosterone is not useful as an oral agent because of a nearly 100 percent first-pass effect by the liver. Fludrocortisone (see Table 41–1) has both glucocorticoid and mineralocorticoid activity. An alternative to fludrocortisone is deoxycorticosterone (DOC), which is a potent mineralocorticoid.
Structure
Synthetic glucocorticoids are all analogs of the natural occurring cortisol. Various modifications of the steroid nucleus have important pharmacokinetic effects to increase glucocorticoid potency relative to mineralocorticoid potency, to decrease first-pass effect and increase half-life, and to decrease binding to CBG. Aldosterone has a unique epoxide structure in the “D” ring that prevents its inactivation.
Mechanism of Action
Both the glucocorticoids and the mineralocorticoids bind to specific nuclear receptors within target cells. The glucocorticoid receptor is in an inactive state in the cytoplasm of target cells bound to a variety of heat-shock proteins, especially HSP 90. On binding a glucocorticoid, the heat-shock proteins dissociate, the GR forms a homodimer and translocates to the nucleus and binds to the promoter region of specific target genes. Via the process of coactivator or corepressor recruitment, transcription of specific target genes is either increased or decreased. The mineralocorticoid receptor (MR) is expressed in the kidney, salivary glands, and GI tract. It binds aldosterone with high affinity but also binds cortisol with nearly the same affinity. MR bound to cortisol is held in an inactive state by NADH produced by the enzyme 11β-HSD2.
Administration
Glucocorticoids can be administered orally, by injection, by inhalation (especially for use in asthma), rectally, and topically. Patients taking glucocorticoids for longer than 2 weeks must be slowly tapered off the drug so that adrenal function can be restored. When used for less than 10–14 days, systemic glucocorticoids cause insignificant adrenal suppression and tapering is not necessary.
Pharmacokinetics
The half-life and duration of action of glucocorticoids depend on the route of administration and the particular agent. In general, glucocorticoid effects are seen within 4–6 hours. Most corticosteroids are metabolized in the liver to sterol ketones or hydroxides and eliminated by the kidney.
Glucocorticoid and Mineralocorticoid Antagonists There are some clinical circumstances such as inoperable adrenal tumors, prior to surgery and for diagnostic use, where inhibition of glucocorticoid action is desirable. Metyrapone is a specific inhibitor of 11-hydroxylation, and can thereby inhibit the synthesis of corticosterone and cortisol. In the presence of normal pituitary function there is a compensatory increase in 11-deoxycortisol production. Metyrapone is also useful in the assessment of adrenal function. Following metyrapone administration, urinary 17-hydroxysteroids, metabolites of adrenal glucocorticoid synthesis, typically double if the adrenals are functioning normally. Chronic metyrapone can cause hirsutism, nausea, sedation, and rash.
Aminoglutheamide blocks the conversion of cholesterol to pregnenolone. This inhibits the synthesis of all hormonally active steroids. It has been used to reduce glucocorticoid levels in patients with Cushing syndrome because of adrenal tumors or excessive ectopic production of ACTH. It has also been used to treat estrogen-dependent breast cancer and prostate cancer. Adverse effects are common and include GI upset and neurologic disturbances.
Ketoconazole is an antifungal agent; at high doses it nonspecifically blocks several enzymes, especially P450 enzymes that are involved in adrenal and gonadal steroidogenesis. It is the most effective inhibitor of steroid hormone biosynthesis available in patients with Cushing disease. Adverse effects include hepatic dysfunction with increased transaminases and liver failure.
Mifepristone (RU-486) is a 19-nor steroid that is a potent antagonist of both the glucocorticoid and progesterone receptors. It has been used to reduce the activity of glucocorticoids in patients with ectopic ACTH production or adrenal carcinoma. The main use of mifepristone is as an antiprogestin (Case 40) as an abortifacient when combined with prostaglandin E1.
Two mineralocorticoid antagonists are available, spironolactone and eplerenone. Spironolactone antagonizes the mineralocorticoid and the androgen receptor (AR). It is used to treat hypertension (see Case 12) usually in combination with a thiazide or a loop diuretic. It can be used diagnostically to restore potassium levels to normal in patients with hypokalemia secondary to hyperaldosteronism. Based on its antiandrogen activity, it has been used to treat hirsutism in women. Adverse effects include hyperkalemia, sedation, cardiac arrhythmias, gynecomastia, sedation, headache, and GI upset.
Eplerenone is a new-generation, aldosterone receptor–specific antagonist. It is approved for use in congestive heart failure, post-myocardial infarction, and hypertension. It avoids the antiandrogen activity of spironolactone. Adverse effects include mild hyperkalemia, dizziness, cough, and fatigue.
COMPREHENSION QUESTIONS
41.1 Which of the following best describes appropriate protocols for withdrawal of glucocorticoids from a patient who has been taking large doses for 6 months?
A. Maintain dose of glucocorticoids and add metyrapone.
B. Maintain dose of glucocorticoids and add spironolactone.
C. An alternate-day dosage regimen of glucocorticoids should be begun.
D. Slow reduction of the glucocorticoid dose over 1–2 weeks.
41.2 A patient with severe shoulder pain resulting from inflammation is not responding to treatment with naproxen. You elect to begin a course of treatment with oral dexamethasone. What is the basis that the glucocorticoid will be more effective as an anti-inflammatory agent?
A. Glucocorticoids inhibit both prostaglandin production and inflammatory cells.
B. Glucocorticoids are more potent inhibitors of cyclooxygenase than naproxen.
C. Glucocorticoids inhibit biosynthesis of both COX-1 and COX-2.
D. Glucocorticoids will reduce the edema in the inflamed area.
41.3 A 32-year-old woman is prescribed a pill for excessive hair on her face and arms. She notes that she has been going to the bathroom at night more often. What is the most likely explanation for the nocturia?
A. Diabetes insipidus effect of the medication
B. Osmotic load to the kidney from the medication delivery system
C. Distal renal tubule effect of the medication
D. Hyperglycemic effect from the medication
ANSWERS
41.1 D. Long-term use of glucocorticoids results in adrenal suppression and atrophy. A slow “weaning” from the drug is necessary so that the adrenals can recover.
41.2 A. Glucocorticoids reduce prostaglandin production like NSAIDs and they also inhibit most of the cells that are involved in the inflammatory process.
41.3 C. The medication is probably spironolactone, which is a competitive inhibitor of androgens at the receptor level, and also an antimineralocorticoid effect at the distal tubule, inhibiting free water resorption. As such, it is a potassium-sparing diuretic agent.
REFERENCES
Tritos NA, Biller BM. Advances in medical therapies for Cushing’s syndrome. Discov Med. 2012 Feb;13(69):171–9.
Graudal N, Jürgens G. Similar effects of disease-modifying antirheumatic drugs, glucocorticoids, and biologic agents on radiographic progression in rheumatoid arthritis: meta-analysis of 70 randomized placebo-controlled or drug-controlled studies, including 112 comparisons. Arthritis Rheum. 2010;62:2852–63.