CHAPTER IX
THE HEAD AND NECK
IN the previous sections the trunk and extremities have been considered. The student must now devote his attention to the most difficult, and yet in many ways the most interesting, part of anatomy, viz. the head and neck. It will be convenient to take the neck first.
Close attention, assisted by repeated observation, is absolutely necessary, as it is by the narrowest scrutiny only that certain details can be understood.
For example, one frequently hears some such expression as “a beautiful light in the eye.” But the explanation of such an expression is beset with great difficulties. In the first place, the light is not in the eye at all, but is reflected from it. Secondly, the manner of the reflection of the light depends to a large extent upon the curvature of the reflecting surface of the eyeball itself and of the surrounding lids and prominences. Thirdly, not only the surface of the eyeball, made up of the transparent cornea and the opaque white sclerotic, but also its internal parts, and in particular the iris, reflect and modify the light which falls upon it. And again, the expression, dependent upon the movements of the facial muscles surrounding the organ, is a very important factor in modifying “the light of the eye.”
In expression one part of the face seldom acts alone; almost always there is a correlated action of other sets of facial muscles. The student has to study and to learn how to indicate the associated actions involved in such expressions, e.g. of the eye and mouth; and further, he must also learn to correlate the expression of the face generally with the movements of the limbs and trunk; to learn, in other words, to combine expression with appropriate gesture.

Fig. 67.—Lateral View of Neck. Massive trapezius.
The Neck is the narrow part of the body between the head and the trunk. It supports the head upon the trunk, and it is based upon the two shoulders, and so connected with the upper limbs. The shape of the neck varies much in different individuals: it may be long or short; it may show well-marked muscular prominences, especially in males; it may be gently rounded, especially in the female, owing to the presence of a normal quantity of healthy fat and the absence of any great muscular development. or it may present pendulous rolls of unhealthy fat.
The neck displays perhaps its most striking features in front.
If the student looks at the subject in profile (Figs. 67 and 68), he will observe that the upper part of the neck in front lies considerably behind the point of the chin.
As the profile is traced downwards towards the front of the chest, it is seen to incline a little forwards. In the natural easy position of the head the angle made by the lower jaw with the front of the neck is about ninety degrees, but of course it varies with changing positions.

Fig. 68.—The Surface Markings of the Side and Front of the Neck.
When the head is bent backwards so that the face looks up, the angle is opened out (Fig. 77); when, on the contrary, the head is bent forwards, the angle is much diminished (Fig. 75). A greater range of movement is allowed in a downward than in an upward direction.
The angle also depends upon the extent of fulness in the submaxillary and submental regions. The surface here is gently rounded in youth (Fig. 72), while later in life it may be divided into two or even more rolls by transverse furrows, giving rise to the popular expression “double-chin ” (Fig. 69).
These extra chins are the result of the presence of fat in large quantities, and of the subdivision of the fat by folds in the skin, which are primarily caused by some fibres of the platysma muscle (Fig. 25) crossing to the other side, and by the movement of the head upon the neck; but they are secondarily perpetuated by the formation of fascial, or fibrous, bands under the skin.
Note that in the case of a well-marked double chin the intervening furrow is prolonged on to the lower part of the side of the face.
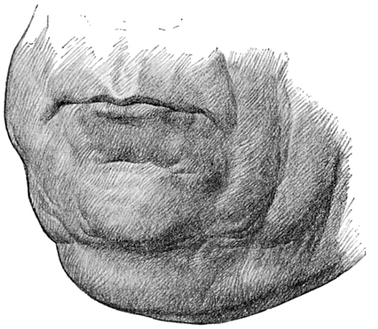
Fig. 69.—Furrows around Mouth. Thin lips. Double chin.
Immediately under cover of the lower jaw, never visible, and but very rarely even palpable until the head is bent backwards, is the slight median body of the hyoid bone. So small is this that it would hardly be worth noticing in a study of surface form were it not for the fact that from the hyoid many muscles pass to the lower jaw and tongue, and to the thyroid 182 cartilage, muscles which assist in the acts of talking mastication, swallowing, etc. (Fig. 73), and become prominent during some of these actions. Moreover, since the hyoid bone is arched just like the body of the lower jaw, and is smaller, and placed just below it in the neck, it follows that the muscles which pass between these two bones must converge upon the smaller bone from the mandible. The general sloping inwards and backwards of the skin from the lower jaw to the upper part of the neck is thus explained; its direction is backwards in the submental region, best seen in profile, and downwards and inwards in the submaxillary regions, best seen from in front (Figs. 70, 71, 72).
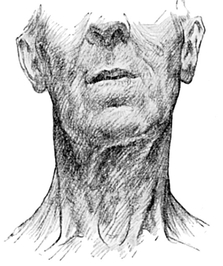
Fig. 70.—The Surface Markings upon the Neck of an Old Man. Front view.

Fig. 71.—The Surface Markings upon the Neck of an Old Man. Side view.
The first prominent landmark which makes itself apparent in the profile below the lower jaw is due to the largest cartilage of the larynx, as the voice-box or upper part of the air-tube is called (Fig. 68).
This thyroid cartilage consists of two wings or alœ, which lie in a vertical plane, one on each side of the middle line. The alæ converge and are united to form a sharp though not straight edge, which is palpable in the middle line in front in both sexes, though more easily visible, because larger, in the male; it is called the pomum Adami, or “Adam’s apple.”
The adult male, then, has a prominent thyroid cartilage, and a much deeper voice than the female; the student will rightly anticipate that the two facts may be associated with each other.
It is in the upper part of the larynx that the vocal cords lie. The vibration of these by air during expiration produces phonation. Owing to the large size of the thyroid cartilage, to which in part they are attached, the vocal cords are much longer in the male than the female—indeed the proportion is 3 to 2—and thus a deeper sound is produced when they vibrate.
There is little or no difference in size between the young girl and the boy. In the latter, however, a great increase takes place at puberty, and accounts for the “breaking ” of the voice.
The alæ are flat, and can be easily felt as they diverge backwards from the pomum Adami.
The thyroid cartilage is separated from the hyoid bone by a shallow and broad groove which is obliterated by the superficial coverings. The groove is supported by the thyro-hyoid membrane and thyro-hyoid muscle.
The Cricoid cartilage, in shape like a signet-ring, lies below the pomum Adami, and can be felt in the middle line of the neck. It is broad behind and narrow in front. It is partly by the movements of the thyroid upon the cricoid cartilage that alterations in the pitch of the voice are brought about by causing different states of tension in the vocal cords.
The thyroid and cricoid cartilages are separated by a transverse furrow, and are connected with each other in two ways: first, by a membrane which is continuous with the vocal cords, and which is known as the crico-thyroid membrane; and secondly, by a small joint on each side.
The cricoid cartilage is directly continuous below with the trachea or windpipe, which passes down behind the supra-sternal fossa into the upper part of the chest and so to the lungs.
The windpipe may generally be felt, but is only seen in very thin subjects. It would be legitimate to indicate it, or at least its first ring, as visible through the skin in a man suffering from starvation. It consists of alternate rings of fibrous tissue and cartilage. The more prominent rings are the cartilaginous, which are not quite complete, being deficient behind, where they are replaced by fibrous tissue.

Fig. 72.—The large Thyroid Gland in a Girl’s Neck.
The second, third, and fourth rings are obscured by the isthmus of the thyroid body (Fig. 72); the lower rings are not seen, because as the trachea is traced downwards towards the chest, it lies much more deeply, i.e. further away from the surface, until, in a fat adult male, it may be an inch and a half from the floor of the supra-sternal fossa. This increased depth of the trachea from the surface is partly due to the fact that the neck, as seen in profile, slopes slightly forwards again just above the sternum (Fig. 77).
The larynx and trachea can be seen to move upwards during the act of swallowing, and downwards when the action is completed.
Just above the sternum lies the supra-sternal fossa, which has already been alluded to in the description of the trunk. Occasionally a small blue vein may be seen passing across this fossa in a transverse direction; it connects the lower parts of two veins which lie close to the middle line. They are the anterior jugular veins, and pass from the region beneath the chin to the lower part of the neck. There they diverge outwards on each side, under cover of the sterno-mastoid muscle. These veins are only obvious when enlarged in cases of asphyxia.
If the neck of a young female is thrown forcibly backwards a distinct bulging will be noticed in its lower part—in a very thin subject the bulging may reveal the shape of an H. The swelling, which is quite distinct in this position, and often obvious in any position, is due to the presence of an important structure known as the thyroid gland. This gland is very frequently enlarged, giving rise to a “goitre,” a comparatively common condition amongst the inhabitants of some of the Swiss and Tyrolese valleys. In England the condition sometimes bears the name of “Derbyshire neck.”
There are fashions in appreciation and portrayal of beauty, and the neck has in two very different periods been the part selected for exaggeration. Rossetti and Burne-Jones often endowed the lower part of the side and back of the neck with extraordinary muscular development (Fig. 67), while in the Renaissance women the thyroid was often depicted as verging on a goitre (Fig. 72, p. 185).
Some of the landmarks hitherto referred to in the neck can only be demonstrated with difficulty, and all are of little importance when compared with that to which the student’s attention will now be called. This is the most marked muscular feature of the neck, in either sex, an oblique ridge formed by the sterno-mastoid on each side (Figs. 68, 70, 71, 73, 74).
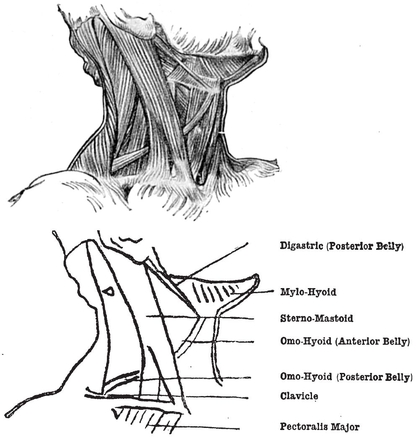
Fig. 73.—The Muscles of the Side and Front of the Neck.
This muscle is very thick and strong, and passes downwards from the mastoid process of the skull, which is situated behind the external ear or auricle, as well as from a part of the occipital bone continued backwards from it (Fig. 73).
From this origin, where the ridge it forms is hardly so pronounced as elsewhere, the muscle passes downwards, forwards, and inwards, becoming progressively more prominent. It is attached below to the inner two inches of the upper surface of the collar-bone, and, by an independent tendon, to the front of the upper part or manubrium of the sternum. The clavicular portion is broad, flat, and fleshy; the sternal portion round, cord-like, and tendinous. The two parts of the muscle become separated from each other at only a short distance above the clavicle; in this way a small and variable triangular interval is left between them.
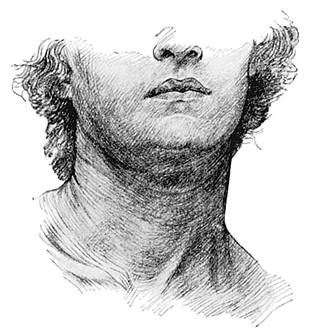
Fig. 74.—Necklace-like Creases in Front of Neck of Youth.
Although the sterno-mastoid muscle runs obliquely when the head is directed forwards, its position is very different when the head is turned on one side. Then the sterno-mastoid of the side opposite to that towards which the face is turned assumes a vertical position, and stands out well, because it is in action, while the sterno-mastoid of the other side becomes more oblique and less prominent, because it is not in action.
Whatever position the head may occupy the prominence formed by the sterno-mastoid is always obvious, although naturally it is more pronounced when the muscle is in forcible action.
This large and important muscle has a complicated action. When the muscles of the two sides act together and the thorax is fixed, they bend the head forward. But when the head is fixed, they raise the chest, and can thus be used as accessory muscles of respiration. This happens when there is difficulty in breathing, as in a case of asphyxiation, or in a man suffering from asthma.
When one muscle acts alone the face is rotated to the opposite side, and the head is depressed on the shoulder of the side of the acting muscle. This composite movement results in a slight elevation of the chin, and a corresponding upward inclination of the face. The exercise of rowing displays it in vigorous action.
The sterno-mastoid muscle forms the boundary of certain regions of the neck, viz. the slightly hollow areas known as the triangles of the neck (Figs. 68, 73).
There are two chief triangles, anterior and posterior, so called from their position relative to the sterno-mastoid. They are of course bi-lateral. and in the “attention” position of the head are symmetrical.
The anterior triangles are immediately adjacent to each other, the boundary being the anterior middle line of the neck, the various points of which have just been described.

Fig. 75.—Head and Face of an Old Man.
The apex of each anterior triangle points downwards, and is formed by the convergence upon the middle line at the lower part of the neck of the sterno-mastoid muscle as it passes to its sternal attachment.
The base of the anterior triangle is directed upwards, and is formed on each side by the lower margin of the jaw, and by a line drawn backwards from this to the tip of the mastoid process.
The sides of the triangle are formed by the middle line of the neck and the anterior border of the sterno-mastoid muscle.
During the act of coughing, in a well-developed muscular subject who has very little fat, three ridges, or perhaps furrows, may occasionally be observed converging upon the hyoid bone. These indicate the presence of small subjacent muscles.
One of the ridges or furrows is more obscure than the others, and passes from the hyoid bone downwards, outwards, and backwards, beneath the sterno-mastoid. This is the anterior portion of a slender, long, tape-like muscle, the omo-hyoid, which passes downwards across the anterior triangle in its lower part, and subsequently across the base of the posterior triangle, to find attachment on the scapula (Fig. 73).
The other two ridges are due to the two portions of one muscle, the digastric, the anterior part of which passes to the hyoid bone from the chin, while the posterior part passes to the same bone from the mastoid process, in company with a small muscle, the stylo-hyoid, which cannot be separately distinguished without dissection (Fig. 73).
These three ridges divide the anterior triangle into three smaller ones, of which the upper, or digastric triangle, is the most obvious. It lies beneath the lower margin of the jaw, and contains the submaxillary salivary gland, which produces a fulness in this region, and a part of the parotid gland, which, except in the glutton, forms no prominence, but merely fills up what would otherwise be a hollow between the ramus of the lower jaw and the ear.
The posterior triangle lies behind the posterior border of the sterno-mastoid.
This is a much smaller area than the anterior triangle, and differs from it in having its base directed downwards and its apex upwards.
The base of the posterior triangle is formed by the middle third of the upper border of the clavicle. The sides are formed in front by the posterior border of the sterno-mastoid, and behind by the anterior border of the upper or cervical portion of the trapezius. The apex of the triangle is at the point where these muscles meet, or nearly meet, at the middle third of the superior curved line of the occipital bone. That is, the apex is about the mid-point of a line drawn between the tip of the mastoid process and the external occipital protuberance.
Occasionally the base of this triangle may be narrowed by the attachments of the sterno-mastoid and trapezius muscles to the clavicle approaching each other more nearly than usual.
Such decreased breadth is not necessarily due to excessive muscular development. Such development would merely cause the boundaries to be more prominent and the triangle to be deeper, and therefore more pronounced.
The apex of the triangle may, on the other hand, be replaced by a short line in those subjects in whom the attachments of the same two muscles to the occipital bone fail to meet.
The basal part of the area behind the sterno-mastoid may show pulsation, owing to the presence of the subclavian artery which lies deeply in this region just above the clavicle.
The neck, as it reaches the trunk, becomes rather thicker. The increased thickness is due to certain deep muscles which pass from the neck to the upper ribs, but they will not repay the artist for an attempt at differentiation.
In persons who have not much superficial fat the external jugular vein is easily discerned, but it is seldom as striking an object in nature as in art (Fig. 68, p. 181). It is one of the largest of the superficial veins in the whole body. Its course is indicated by a line drawn from the mid-point between the angle of the lower jaw and the tip of the mastoid process to the middle of the upper border of the clavicle. Just above the clavicle it disappears from view by passing deeply under the outer margin of the sterno-mastoid, to join the subclavian vein. There is no such thing as a “jugular artery.” The main artery in the neck is the carotid, and the vein which runs with it, too deep to be seen, is the internal jugular.
Expiratory effort, as in singing, makes the external jugular vein full and prominent, and then it may show one or two dilatations in its course, the result of valves within its lumen.
There is a very interesting thin, but wide, muscle on each side of the neck, called the platysma myoides (Fig. 25), the best example in the human being of the superficial sheets of muscular fibres similar to those which cover a great part of the body of some of the lower animals, e.g. the horse. A very good representation of this is to be found in the hall of the Royal College of Surgeons. The platysma lies in the superficial fascia of the neck and upper part of the chest. Sweeping downwards from the face, it covers both anterior and posterior triangles, and obtains a weak attachment to the margin of the lower jaw and of the clavicle as it passes with a slight inclination back wards over the latter bone, to terminate in the skin of the upper part of the chest and shoulder. When the platysma acts, it pulls the skin of the chest upwards and the angle of the mouth downwards and outwards. Some of the muscles of the face are derived from the same subcutaneous muscular sheet, but have become specially developed in connection with the expression of the emotions. The platysma is sometimes very strongly marked, and the individual bundles of muscle fibres which form the sheet may even be seen through the skin. Being concerned in expression, it is innervated to a large extent by the facial nerve (Plates XXIV., XXV.).
Notice the double destiny of this subcutaneous muscle sheet, so useful to certain animals for startling away, by the sudden movements it can give to the skin, any irritating insects which are out of reach of the tail. Over the greater part of the human body the muscle has degenerated; it has, in other words, undergone involution. The facial part of it, however, has become evoluted and differentiated, and is of great importance in the expression of the emotions.
Notice also that it is the anterior borders of the two platysma muscles which account for those two vertical cord-like folds of baggy skin in the pre-hyoid and pre-thyroid region of the aged and withered neck. Here, and about the apex of the posterior triangle of the neck, are the two places where are earliest shown the effect of age in withering the subcutaneous structures and rendering the skin baggy (Fig. 70).
The superficial fat of the neck, as of the rest of the subject, is relatively more abundant in the female than the male, and fills up the hollows and rounds off the prominences, so that in the female the muscles, and especially the sterno-mastoids, are not nearly so conspicuous as in the male.
We must now concentrate our attention upon the trapezius muscle, which forms a flat sheet situated on each side of the cervical and dorsal vertebræ.
The trapezius (Fig. 62, p. 158) has the most extensive attachment of any muscle in the body. Its origin lies in and near the middle line, and embraces attachments above to the external occipital protuberance, and to an inch or more of the superior curved line of the occipital bone; below this to the ligamentum nuchæ, a strong, deep, elastic ligament which bridges the backward concavity formed by the cervical spine as seen in the profile view of the skeleton; and below this again to all the dorsal spinous processes.
The ligamentum nuchœ, from which this muscle arises in the neck, is a broad band of fibrous material containing some elastic tissue, and extending from the external occipital protuberance to the spine of the seventh cervical vertebra. It is attached to all the cervical spines, and gives origin to several layers of muscles situated on the back of the neck. It helps to keep the head erect, and so diminishes, but does not abolish, the need for continued muscular activity in order to maintain the poise of the head; in quadrupeds it is enormously hypertrophied, because, their spine being disposed horizontally, its task is increased. But for the ligamentum nuchæ, any quadruped with a heavy head would have to hang it vertically from the shoulder as in the position of grazing, or to., develop some stronger muscles in the back of the neck; muscular tissue becomes tired, while ligaments do not.
If the student will now examine that border of the trapezius which bounds the posterior triangle (Fig. 62, p. 158), he will observe that it is not nearly so vertical as the lower border which lies upon the back. The cervical outer border is curved somewhat forwards, so that the back part of the side of the neck is gently rounded. The shape and bulk of the trapezius will be better realised if the model shrugs his shoulders, while the student examines the part just above the scapula (Figs. 67, 77).
In a muscular subject it can be appreciated that in the greater part of the dorsal region, and in the upper part of the cervical region, the muscular fibres of the trapezius extend right up to the middle line; but in the lower cervical and upper dorsal regions a short flat tendon of origin, or aponeurosis, is developed on each side, which produces a slight flattening or depression on either side of the vertebra prominens (Fig. 62, p. 158).
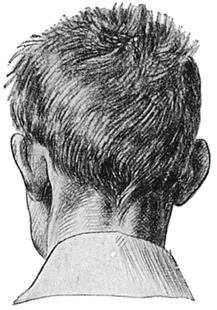
Fig. 76.—Back of Boy’s Neck, showing Median Furrow.
In the middle line of the neck between the two tra-pezii there is a deep furrow, frequently obscured by fat, and best seen perhaps in the boy’s neck (Fig. 76), continuous with that already described in the account of the trunk. At the bottom of this nuchal furrow lie the ligamentum nuchæ and the spines of the vertebræ. Although the trapezius makes the longitudinal elevation on each side of this furrow, it is by no means entirely responsible for its prominence, the thick complexus muscle contributing largely though its outline is obscured by the trapezius.
The complexus lies under the trapezius and pushes it up. The ridge it forms is narrower and more prominent above than below (Fig. 76).
If the student now adds to what he can see that which he can feel by pressing his finger down this furrow, he will make acquaintance with the spine of the axis, or second vertebra.
The axis forms a massive, though not prominent, eminence below the occipital protuberance. The spines of the first, third, fourth, and fifth vertebræ cannot be felt, but the sixth and seventh are quite distinct. The spine of the vertebra prominens is, however, hardly more conspicuous than that of the first dorsal vertebra, which lies below it and is almost if not quite as obvious.
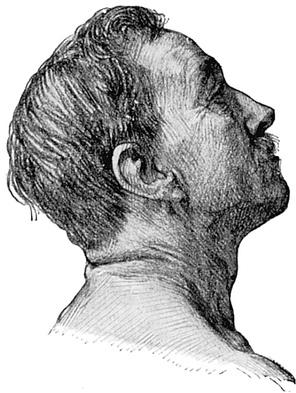
Fig. 77.—Creases seen on Back of Extended Neck.
These spinous processes of the vertebræ are best observed when the skeleton spine is bent forwards. In this position they are also separated by wider intervals than when the head is erect (Plate XXII.).
When the head is bent backwards (Fig. 77), transverse superficial folds may be seen running across the back of the neck. Hair is found in the upper part of the neck, and especially in the median nuchal furrow (Fig. 76, p. 196). In the muscular subject the back of the head is often nearly, but seldom quite, flush with the back of the neck (Figs. 65, 67), a very different condition from that seen and described in the front part of the same region.
The Head and Face.
The skull, or skeleton of the head, is divided by anatomists into (a) the Cranial Bones, concerned chiefly with the protection of the brain, and therefore dense and strong; and (b) the Facial Bones, designed for the accommodation of the organs of special sense and of mastication and expression, and therefore comparatively light.
The Scalp, as the soft parts covering the cranium are collectively called, is, with the exception of the forehead, covered with hair. The scalp is very dense and tough and mobile, but quite thin, so that the shape of the cranium is dependent upon the bones, which vary much in different skulls, and are rarely exactly similar even on the two sides of any individual—in fact, no human being is in any part strictly symmetrical. Two main types of skull may be mentioned—the “dolichocephalic” or long head, and the “brachycephalic” or broad head. Between these two main types is an intermediate one, to which belong the higher races of mankind.
The various relations of length and breadth of the skull in its different parts are dealt with in the science of anthropology.
We will study first the skull with its coverings, and later the face.
The Hairy Scalp.—The hair throughout the body varies in many qualities—e.g. colour, texture, thickness, and moisture—but it never varies in the direction of its slope, which as a general rule is such that if one goes down on all-fours, rain falling on one’s back would be directed to the ground by the hairs. The hair of the scalp slopes downwards from a point situated rather behind the vertex of the skull. Possibly the direction of the slope of the hair may be to some limited extent determined, or even altered, by habitual brushing in a definite direction. The frequent early disappearance of hair at the upper part and sides of the forehead is in all probability due partly at least to the wearing of some form of hard head-gear. Readers of Scott will recall his description of Marmion.
Hair also often disappears and produces baldness in the mid-line of the head, behind and around the vertex. From this “tonsure” the area of disappearing hair spreads forward, laterally, and backwards, until finally only the sides of the head are left covered. In the majority of persons becoming bald the area immediately surrounding the patch of baldness is poor not only in quantity, but also in the size of the individual hairs.
The scalp has no definite boundaries except in front, where it is separated from the face by the curved upper margin of the bony orbit, a line corresponding with the eyebrows. Laterally the boundary is that arch of bone, the zygomatic arch, which forms a flying buttress on each side of the head, and is composed of a slender process of the temporal bone, called the zygomatic process, at the back of the arch, and of the malar bone at the front.
Behind this arch the mastoid process, the superior curved line, and the external occipital protuberance mark the boundary between head and neck.
The auricle, or ear, ought properly to be considered as a part of the cranium. For various reasons, and especially for the art student, it will be more conveniently considered with the anatomy of the face.
The part of the Cranium which is not covered with hair, and which is known as the forehead, is as liable to show variety of shape as any part of the skeleton. Any eminences which may be present upon it are due chiefly to the surface form of the underlying frontal bone. On each side of the middle line the student will notice the frontal eminence. This is situated some two inches above the orbit, and as a rule is smooth and rounded, and only slightly elevated.
The frontal eminences are said to be well marked in high types of intellect, as the intellectual nerve centres are specially developed in the frontal lobes of the brain. But it is only right to state that these eminences are also particularly well developed in feeble children suffering from rickets.
It is necessary to distinguish the frontal eminences from those others which are situated much nearer to the middle line, just above the root of the nose. These superciliary ridges, which, owing to the absence of any intervening furrow, occasionally run into one another, are due to the development of air spaces within the frontal bone connected with the nasal cavity, and are probably useful as resonating chambers for the modulation of certain qualities of voice. They are hardly developed at all until after the age of seven years, and afford little, if any, indication of the intellectual power of the individual.
They lie above and parallel to the supra-orbital margins, being separated from them by a distance of one-third of an inch. These ridges can always be felt, but not always seen.
The root of the nose, where the forehead becomes continuous with the face, will be described with the latter.
The skin of the forehead is usually smooth and frequently shiny; it is liable, as in the act of raising the forehead to express surprise, to be thrown into a series of slightly curved folds, or furrows, some of which, to a varying extent in different individuals, are permanent.
Three or four such frontal furrows are demonstrable. The upper ones run across the middle line, but the lower are interrupted there. They are concavo-convex, the convexity lying on each side of the middle line and the concavity lying across it, and both ends being directed downwards (Fig. 75).
The upper furrows, as well as being larger and more complete, are deeper. All the furrows are prolonged outwards on each side to the margin of the hairy portion of the scalp. They occupy usually only the lower half of the forehead.
The furrows are due to the contractions of the underlying frontalis muscle, which is the anterior muscular portion of a musculo-membranous sheet called the occipito-frontalis. The muscle is connected above with the aponeurosis, while below it is inserted into the skin of the forehead, and passes down into the nose. It also blends with the muscle chiefly concerned in the opening and shutting of the eye, viz. the orbicularis palpebrarum.
In the act of frowning, additional grooves are to be noticed placed vertically or obliquely near the middle line just above the nose. These important grooves are formed by the contraction of a tiny muscle known as the corrugator supercilii..
The upper border of the frontalis muscle corresponds to the limit of the transverse furrows on the forehead.
The two frontales muscles lie immediately adjacent to one another in the middle line, and their upper edges, where they blend with the aponeurosis, are sharply convex. The outline of these muscles is particularly well seen in young subjects.
On the side of the forehead a tortuous, pulsating ridge may be seen in the old, or even in those who are prematurely old; and, be it remembered, a man’s age is rarely so correctly ascertained at Somerset House as by an examination of his blood-vessels. The condition of this heaving and pulsating ridge, due to the presence of the subjacent superficial temporal artery, is a far better indication of senility than the records of a registrar (Fig. 75).
Its conspicuousness in old persons is a consequence partly of that wasting of the superficial tissues which occurs with age, but chiefly of the deposit of a lime salt within the walls of the artery. The deposit renders the artery more rigid, so that it stands out much more distinctly than it would do other. wise. The artery is at the same time lengthened, which causes it to become tortuous.
The forehead varies very much in expanse and shape. The low forehead, which is considered by some to be a point of beauty in the female, to others suggests chiefly the criminal taint with which it is often associated in the male.
The high forehead is thought to be a characteristic feature of intellect; notice, for instance, the busts of Shakespeare, or the portraits of Walter Scott. Certainly the height of forehead may be due to actual expanse of cranium, but beware of the false impression conveyed by baldness or the brushing back of the hair.
The forehead may bulge forwards, or it may be decidedly “retreating.”
The prominences noticeable upon that part of the head which is covered with hair are symmetrically placed, like those of the forehead.
The parietal eminences are seen at the broadest part of the head on each side, above and behind the ear. They indicate the spots at which the ossification of those bones originally started.
Immediately behind the ear is the nipple-shaped mastoid process (Figs. 15, 16, and 18, pp. 55, 56, 58), a bony eminence which is better developed, actually as well as relatively, in the adult than in the child. The reason for this difference is, that after the age of seven years air spaces are developed in the substance of the temporal bone in connection with the middle ear, a part of the organ of hearing buried deep in that bone. The air spaces are in direct continuity with the middle ear, as the box which has the drum of the ear in its outer wall is called. All vibrations entering through the passage of the external ear disturb the drum which lies at the bottom of it. The drum transmits the disturbance or vibration by means of three small bones, advantageously placed for this special purpose, to the internal ear, which is the actual organ of hearing.
The external occipital protuberance can be more easily felt than seen, but its position should be observed, as it forms an important landmark. It lies just above the nuchal furrow in the middle line of the back. The superior curved line, and therefore the boundary between the head and the back of the neck, is continued outwards on each side from this protuberance.
In young children who have not yet obtained a covering of hair, and to a less extent in older persons who may have lost it, the posterior muscular part of the epicranial musculo-aponeurotic sheet will be noticed, forming a flat, slightly raised eminence of thin muscle called the occipitalis. This corresponds behind to the frontalis already described as a landmark of the forehead.
The whole sheet is called the occipito-frontalis muscle. The posterior part is known as the occipitalis muscle, and arises from the superior curved line of the occipital bone. The origins of the two occipital muscles are separated, unlike the frontales, by a distinct interval, measuring at least an inch.
The occipito-frontalis muscle (Fig. 78) is not capable of throwing the skin of the scalp into folds except in the forehead, where it accounts for the transverse grooves so obvious in the expression of surprise. The extent to which these folds can be voluntarily produced varies much in different individuals, and in a few, especially after youth is past, the grooves are permanently impressed upon the skin. Similar differences are found in the degree of voluntary control possessed by individuals over the movement of the scalp and of the external ear.
On the side of the skull, but chiefly in front of the ear, a fan-shaped, slightly elevated region, broad with convex border above, and narrow below, is due to the subjacent temporal muscle (Figs. 79, 80). This is one of the immensely powerful closers, or elevators, of the lower jaw. It arises from the temporal fossa of the skull, and is inserted into the coronoid process of the mandible. When vigorously contracted, as in grinding the teeth, the belly of the muscle can be felt as a rounded eminence above the zygomatic arch. The muscle descends deep to this arch (which has been cut away in Fig. 79 to show the tendon) as it passes to its destination. The facility with which this muscle may be felt, or even seen, to contract when the jaw is clenched has been utilised by fraudulent thought-readers as a means of communicating with the confederate by a sort of Morse code.
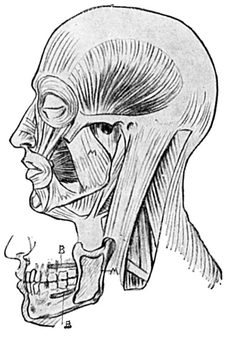
Fig. 78.—Muscles of side of Head, Face, and Neck.
M=Masseter. Inset of Jaws showing;—B. Origin of Buccinator.M. Insertion of Masseter.
The Superficial Anatomy of the Face.—Even in the more vacant countenance, which has been said to bespeak the empty mind, there are variations in expression from moment to moment. When the subject of our study is an active-minded and intelligent person, the difficulties which confront us are complex and varying in the extreme.
The Face, for the purposes of convenient description, includes the chin, cheek, mouth, nose, eyes, and ears.
The ordinary anatomist is content to consider all faces to be as much alike as a row of pins, yet in reality there is as much difference between any two faces as there is between any two finger-prints; no two faces are exactly alike, and no face is strictly symmetrical. Even as a doctor must be a student all his life, so a portrait-painter finds that the longest life is too short to fathom all the depths and difficulties presented by facial expression.
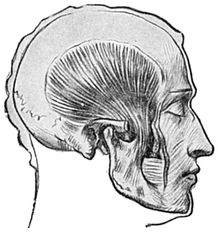
Fig. 79.—Temporal Muscle. Zygoma cut away.
Let us attempt a brief account of the anatomy of the face and its component parts, in order that the student may begin to understand something of its various movements and resultant expressions.
When the face is viewed from the front (Fig. 81), the outline of the forehead (as high as the vertex) and face may be seen to resemble that of an egg, the broad part of the head being situated above and the narrow part below.
Let the ovoid be quartered or divided by a vertical median line and by a horizontal line through the middle of the vertical one (Fig. 81).
The eyeballs lie on a level with the line drawn horizontally through the middle of the ovoid, or even slightly below this level. This is a most important point to realise, for if the eyes are placed too high, it becomes at once manifest that the head belongs to that microcephalic type which is usually associated with the criminal class.
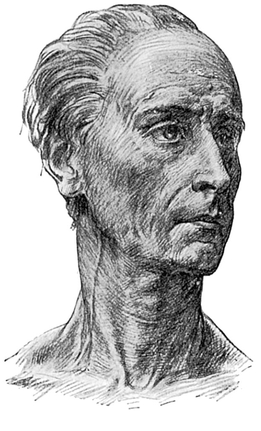
Fig. 80.—Surface Markings upon a Thin Face and Neck.
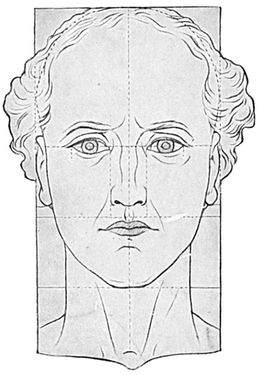
Fig. 81.—Figure to show Proportions of Face and Neck.
Most of the face therefore lies in the lower half of the ovoid; only a small part, indeed, passes into its upper half, which is chiefly occupied by the forehead.
If the lower half of the vertical median line be bisected by another horizontal line so as to subdivide the lower half of the ovoid, the mouth and chin will be found to lie in the lowest quarter of the face, and the nose in the quarter above this.
If the horizontal line through the eyeballs be continued outwards it will pass a little below the highest points of the ears.
If a horizontal line be drawn between the tips of the ears, and the face be still viewed from the front and considered as if it were flat, and this line be divided into fifths, the middle fifth corresponds to the root of the nose, and the fifths on each side of the middle, to the eyes; and the fifths to the side of this again correspond to the foreshortened temples.
The eyeballs are the organs of vision by which light waves are received and transmitted to the brain. They are well protected from injury by surrounding bony ridges, orbital margins, which bound the anterior part of the bony cavities in the skull, known as the orbits.
Above the eyeball is the particularly well-marked ridge formed by the supra-orbital margin (Fig. 82, p. 210) of the frontal bone. This is sharp and concave downwards, and terminates externally in the well-marked external angular process to which the temporal muscle nearly reaches, and internally in the less noticeable internal angular process on the side of the root of the nose.
Externally to the eyeball, the antero-internal part of the malar bone forms a protecting ridge. Below the eye the infra-orbital margin of the malar and superior maxilla forms a ridge which, though less prominent than the supra-orbital, yet projects enough to bring this margin also in front of the eyeball.
Internally, the boundary of the orbit is formed by the nasal process of the superior maxilla and part of the frontal bone.
It is the prominence of the nose, however, that is responsible in the main for the protection of the eyeball from blows directed on its inner side. Owing also to this same prominence, vision is more obscured on the inner or nasal side of the eye than on the outer or temporal side; so that when the eyes are directed to an object situated on the left side, the left eye sees much more of the object than does the right eye.
The supra-orbital margin is covered by closely set and rather coarse hairs, forming the eyebrows. The line of the eyebrows, in the inner half of its length, lies on a nearly horizontal plane, but in the outer half it is prolonged somewhat downwards.
The inner ends of the two eyebrows sometimes meet in the middle line of the root of the nose, running somewhat downwards to do so, and producing a “beetling brow.”
The individual hairs of the eyebrows are directed for the most part upwards and outwards, but externally the outward or even a downward direction may be more apparent (Fig. 82, p. 210).
In some people the eyebrows project directly forwards, and are very long; in some the outer part may be almost wanting, or may be directed upwards and outwards.
The upper and lower soft fleshy curtains or eyelids form an additional protection to the delicate organ of vision, upon which they move almost without friction because of the sac of the conjunctiva, which is lubricated by tears.
The conjunctiva covers the apposed surfaces of the lids and eyes. It is a transparent sheet of mucous membrane, and allows the colour of the tissues lying beneath it to show through; so that the inner surface of each lid is ruddy, while the fibrous coat of the eyeball, or sclerotic, shines white through the ocular conjunctiva. The transparency of this membrane is further proved by the fact that, although it covers the cornea, or clear part of the eyeball, it does not obstruct vision.
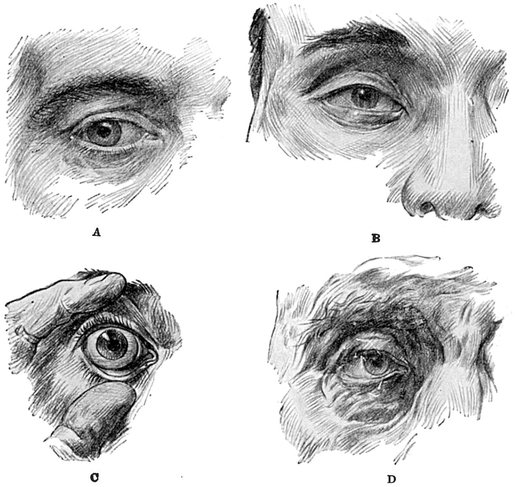
Fig. 82.—The Palpebral Aperture, Eyelids, and Eyebrows.
The chink between the two lids is known as the palpebral fissure (Fig. 82). When the eyelids are separated from each other and the eye open, this fissure is oval or almond-shaped, with the outer corner sharp and angular, and the inner corner rounded or punched out. At this inner corner the edges of the lids run for a space parallel with each other, and thus a little bay is formed, in which is to be seen the caruncle, a small pink fleshy structure.
In certain races, e.g. in the Chinese, the inner end of the upper eyelid is prolonged on the face, over the inner end of the lower eyelid (Fig. 82 B).
Naturally the shape and appearance of the palpebral fissure vary according as the eye is open or shut; and the fissure, when the eyelids are approximated, is generally transverse, with a slight convexity downwards and forwards. When the eye is open, the edge of the upper lid is convex forwards and concave downwards. The edge of the lower eyelid is convex forwards and slightly concave upwards. Both these edges become straighter when the eye is closed.
Near the entrance of the punched-out bay at the inner angle of the fissure, a black spot will be noticed on each eyelid at the summit of a very small eminence. This is the punctum, and is the entrance to the lachrymal canaliculus. It is by the apposition of the lids to the globe of the eyeball that the tears are enabled to enter these puncta, and to be thence transmitted along the canaliculi to the lachrymal duct, and so to the nose.
The lids act not only as curtains, but also as brushes; they move the tears along, and they also sweep away the particles of dust which constantly enter the conjunctival sac.
Increased formation of tears, in certain emotional states, leads to their accumulation in the conjunctival sac till they overflow the lower eyelids and run down the face, the canaliculi being too small to deal with. such an increased flow.
As age advances, the lids, which are normally kept in close apposition with the eyeball, fall away a little (Fig. 82 D, p. 210), owing to loss of tone in the muscle controlling the movements of the lids. As a consequence the tears are very apt to flow over the face, and the eyes to become “blear”—i.e. the ruddy inner surface, especially of the lower lid, becomes visible as in most hounds and some other dogs.
The free edge of each eyelid is thicker than the rest of the lid, and is very slightly everted. Each free edge also carries a row of short, coarse, curved hairs, the eyelashes, which are not very numerous, vary greatly in thickness, in length, and in curve, and are directed forwards. They afford protection against small foreign bodies, which otherwise would enter the eye more frequently.
The Movements of the Eyelids.—Both lids are capable of an upward and downward movement, but the upper lid moves much more freely and extensively than the lower. For this reason the palpebral fissure, when closed, lies below the level of the pupil of the eye.
Within each lid there is a crescentic plate of cartilage, which gives rigidity to the curtain without impairing its mobility.
Two muscles bring about the movements of the lids, viz. the orbicularis palpebrarum and the levator palpebræ superioris. The former is a flat sheet of muscular fibres, arranged in parallel and concentric circles around the margin of the palpebral fissure. This muscle is not visible through the skin, but when the skin has been dissected away it may be seen to spread outwards in the temporal and malar regions; inwards, upon the nose; and downwards, upon the face.
A part of the orbicularis palpebrarum lying actually upon the eyelids may be distinguished from the main part, which lies wide of these curtains. The nerve supply, as is the case with all the muscles of expression, comes from the seventh cranial, i.e. the facial, nerve.
The upper eyelid is distinguished from the lower by having an additional muscle which assists in performing and controlling its movements. This is the levator palpebralis superioris. It runs forwards in the cavity of the orbit, as do most of the muscles which move the eyeball. By the contraction of this muscle the upper eyelid is raised, and owing to it the upper eyelid has more active movements than the lower.
Forcible closure of the lids is brought about by the contraction of the orbicularis palpebrarum, and the eye is opened by the relaxation of this muscle, together with the contraction of the levator.
Blinking is a quick forcible action of the orbicularis, resulting in momentary closing of the eye. It occurs at periodic intervals, and assists in the moistening of the surface of the eyeball itself, as well as in the circulation of the tears and the removal of small foreign bodies from the conjunctiva. Blinking also occurs with any sudden shock, especially one of a visual nature.
Winking is a slower movement, is purely voluntary, and is dependent upon the action of the orbicularis, especially in connection with the lower lid, which is raised in the process. Winking does not take place without the will and knowledge of the subject, and it is not given to everybody to have the necessary amount of voluntary control over each orbicularis independently of the other; blinking, on the contrary, is usually as much an involuntary act as breathing, and the agent is not conscious of either unless it is performed under the influence of some unusual stimulus. Another essential distinction between these two actions is that in winking only one eye is involved at a time, while it is usual for both eyes to blink together—in the human being, at least, though the closing of a single eye in cats and other animals is probably of the nature of an unconscious blink rather than a conscious wink.
Ptosis, or drooping, is a condition of the upper eyelid which the art student should notice. It is sometimes due to paralysis of the facial nerve, which of course supplies the orbicularis; and sometimes to paralysis of the third cranial nerve, which supplies the levator. In either of these cases it is generally unilateral. It may, however, be congenital, and is then more frequently bilateral. Ptosis is an exaggerated degree of the condition known as drooping of the eyelids, which is of considerable interest as indicative of certain emotional states (vide infra).
Some of the various means by which very efficient protection is afforded to the eyeball have now been considered, and the student should direct his attention next to the organ itself.
The eyeball is the organ of vision, and is connected with the brain by means of the optic or second cranial nerve. It is contained in the orbit, which is a cavity developed in the skull in special adaptation to the important structures which it contains.
The expression “globe of the eye” almost exactly describes its shape. It is a little over one inch in diameter, almost as large in the infant as in the adult, and about the same size in all adults. When we say that “the eye is large,” we really mean “the palpebral fissure is large.”
Only that part of the eyeball which lies in front can be seen without the aid of dissection, or the use of the ophthalmoscope, an instrument devised by Helmholtz, by means of which the interior of the eyeball can be illuminated and examined.
The wall of the eyeball consists of three coats. The inner coat, or retina, contains the terminals of the optic nerve, or rods and cones, which are the only structures in the body capable of receiving and transmitting to the brain for interpretation the vibrations of light; the middle, or choroid, is remarkably rich in blood-vessels for the supply of the component parts of the eyeball; and the outer coat, or sclerotic, is protective.
The sclerotic is fibrous and firm, and to it are attached the various small muscles which bring about the movements of the eyeball. It is white in colour, with a faint tinge of blue, and forms the “white of the eye.”
The front part of the sclerotic presents a nearly circular window, filled in by a thick membrane, as transparent as glass and bulging slightly more than the sclerotic. This is the cornea, and through it rays of light pass to the interior of the eye. In addition to its transparency, the cornea differs in certain other respects from the sclerotic. It is, in the first place, thinner; in the second place, it bulges from the surface of the sclerotic because it is a segment of a smaller globe. It would not be quite correct to say that the cornea is circular, for it is slightly longer horizontally than it is vertically.
The colour of the eye, which varies in different individuals, depends upon the presence of a pigmented circular membrane behind the cornea, known as the iris.
The iris might properly be described as a circular disc perforated in its centre. The perforation, however, presents a most remarkable peculiarity; it is capable of alterations in size. If the student brings a light suddenly in front of the eye he will notice that the aperture becomes smaller. If, on the contrary, he places his hand partially over the eye so as to cut off some light, he will observe that the perforation becomes larger.
The perforation or aperture is known as the pupil of the eye. The iris, in addition to being responsible for the colour of the eye, produces also alterations in the size of the pupil, which are of supreme importance to the subject.
The iris contains muscular fibres which are so disposed, in both a radiating and a circular manner, as to cause increase or decrease of the size of the pupil by their action. There are certain definite conditions which cause dilatation—e.g. when the surrounding light is obscured, when a distant object is being observed, and when the subject is under the influence of certain drugs. Belladonna is one of these, and no doubt it received its name from the dark large pupils it produces, which are commonly considered beautiful, and which result from the contraction of the radiating fibres in the iris or the paralysis of the circular fibres.
The pupil is contracted and small during sleep; also, when an object close at hand is being observed, and when the subject is under the influence of certain other drugs, of which opium is one.
The iris contains pigment, which is variable in quantity and not in quality. If there is little pigment the eyes are lighter and bluer; if there is much pigment the eyes are dark. Occasionally there is no pigment at all, in which case the red colouring matter of the blood alone colours the iris. This condition of pink eyes, occurring in albinos, is associated with an absence of pigment elsewhere. The hair of such individuals is white, and the skin has a pinkish tinge. Owing to the absence of pigment their irides are too transparent, so that they do not like a bright light, and hide from it as far as they can.
A large pupil will make the whole eye appear larger than usual.
There is another cause, though a less important one, for the varying colour of eyes, namely, that the iris being thrown into folds radiating from the pupil the rays of light which strike it are reflected and refracted from it. Refraction implies the splitting up of white light into the various primary colours, and it will be clear that this must be responsible for much of the variation in the colour of irides and for some factors in that interesting and obscure subject “light in the eye.”
The student, if he make a close observation, will observe that the iris is not a flat surface, but is slightly curved forwards.
Behind the iris, and filling up the pupil, is the lens of the eye, a transparent structure shaped like an ordinary magnifying glass. It is capable of alteration in its convexity, by means of the action of the small ciliary muscle situated within the eye.
By alteration in the shape of the lens distant as well as near objects can be focussed upon the retina without the necessity for any change in the other parts of the eyeball. The power of thus altering the shape of the lens lessens with advancing years, so that old persons find they can read print more readily when it is held well away from the eyes. The explanation of this phenomenon is as follows: In the old, the lens tends to become set for distant vision only, i.e. for parallel rays of light. Only parallel rays fall upon the lens in such a manner as to be accurately focussed on the retina; and it is in the effort to produce as much parallelism as possible that the old man holds his paper as far off as the length of his arm will allow, and sometimes increases the distance yet more by the backward bending of his head and spine.
Between the lens and the cornea is the anterior chamber, filled with transparent aqueous humour.
Behind the lens lies a second and larger chamber, which contains the transparent vitreous humour.
All these parts, which go to make up the internal structure of the eye, would be useless if the eyeballs could not be moved. Their movement is brought about by six tiny muscles in each orbit. They all, with the exception of the smallest, arise from the back part of the orbit, and pass forwards to their destinations in the white sclerotic coat.
The four recti. muscles, superior, inferior, external, and internal, are attached to these aspects of the eyeball a little beyond its centre of rotation. The smallest, or inferior oblique muscle, passes from the inner side of the front of the floor of the orbit, and is attached behind the centre of rotation. The fifth, or superior oblique muscle, passes from the back of the orbit to a little sling or pulley situated at the junction of the inner wall and roof of the orbit in front. The tendon of this muscle passes round the pulley, and is attached to the upper surface of the eye behind its centre of rotation.
The individual actions of the internal and external rectus are simple. The internal rectus rotates the eyeball inwards, while the external rectus turns it outwards. When the eyeballs move together to one side, the external rectus of the same side and the internal rectus of the opposite eye are acting together. Such a system of interaction between two muscles of different sides is called “co-ordination.” This particular co-ordinated movement is controlled by a special collection of nerve cells in the brain.
The other muscles have a more complicated action, but it will be sufficient to state here that the eyeball is rotated upwards by the simultaneous action of the superior rectus and the inferior oblique, and is rotated downwards by the inferior rectus and the superior oblique acting together.
The co-ordination of these groups of muscles acting on each eyeball must be a very complicated matter. How much more complicated, then, the familiar and well-known action of making limbs and eyes act together in games or other actions of precision, e.g. shooting, cricket, and golf. The popular phrase, “a good eye,” implies almost perfect co-ordination 219 between, and cerebral control of, the movements of very many muscles in the limbs, trunk, and eyes.
Squinting is a consequence of independent action of the muscles of the eye, their proper co-ordination being temporarily or permanently suspended. Many persons are incapable of turning both eyeballs simultaneously outwards, though most persons can turn them both inwards, and indeed do so frequently.
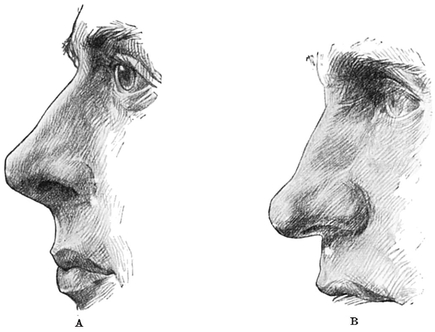
Fig. 83.—Compare these two drawings. The angle formed by the Columna nasi with the upper lip is very different.
When the eyes are accommodated for very near vision, they look decidedly inwards, as in reading small print held close to the eyes.
It may be added that in sleep the eyeball is rotated on a transverse axis upwards; the eyelids are slightly separated from each other, and only a small lower part of the cornea can be seen through the palpebral fissure.
In death the eyelids are widely separated, the cornea becomes dull, and the pupil semi-dilated.
The Nose is the most prominent part of the face. Its root is situated between the two eyes and is continuous with the forehead. Its varying shape in different individuals is due to several factors, which will be described later (Figs. 83 to 88).
The nose is narrower and depressed at its root, and more prominent at its lower end, the front part of which is named the tip, while the lateral parts are called the alœ.


Fig. 85. Various Types of Nose.

The broadening at the lower end is due to the opening of the nostrils, or anterior nares, bilateral orifices through which air passes into the nasal cavity and thence to the windpipe.
The nose is supported by both bone and cartilage—or rather by either bone or cartilage, for where the bone supports the nose there is no cartilage, and vice versa. The bony framework lies chiefly at the root of the nose, the cartilaginous nearer the tip.
Thus the support of the bridge is formed by the nasal bones and the nasal process of the superior maxilla, assisted by the spine of the frontal bone. This part of the nose, being fixed to the skull, is immovable.
The lower part of the nose is supported by cartilages, and is movable, and in the skeleton it is absent. The cartilages, just under the skin, are four in number, two on each side. They lie in apposition with each other in the mid-line, and the median groove between them can often be seen on the front of the tip.
In addition to these cartilages, the nasal septum, which divides the cavity of the nose into two parts, is also partly cartilaginous. It is cartilaginous where it forms the substance of the columna nasi, separating the two nostrils, and is covered by superficial fat and skin. By the presence of these stiffenings of cartilages the nostrils are kept open. The lateral cartilages are attached only by fibrous tissue to the adjacent superior maxillary bone, and are responsible for the slight bulge at the lower part of the lateral aspects of the nose.
The orifices of the nasal chamber, known as the nostrils or anterior nares, look almost directly downwards.
Sometimes the nostrils are much narrower than is usual or natural; in such cases the subject will be found to breathe almost entirely through his mouth, which he keeps constantly open.
The nostrils produce a bulging on each side of the lower part of the nose, and owing to the action of some tiny muscles these bulgings become more prominent during the action of respiration, especially if at all forced, as in distress of beathing.
There is always a slight depression, or fossa, to be felt at the junction of the root of the nose with the forehead. Below this fossa the nasal bones may descend almost vertically from the frontal bone; or they may be inclined more obliquely forwards, when the result is a prominent bridge (Figs. 84, 85, p. 221); or the nasal bone may be sunk in, either as a congenital defect or following upon accident or disease, in which case the bridge is very much depressed and the nose is said to be “snub.”
The nostrils are separated by a median partition or columna, which is the anterior end of the septum dividing the right and left nasal chambers from each other. It is also continuous with the central part of the upper lip, which may by its means communicate slight movement to the tip of the nose.
Hairs project from each nostril, especially, it is said, in the very strong. Those in front are directed backwards as well as downwards; those behind have a forward as well as downward direction. This arrangement produces a very efficient filter, which guards against the entrance of some gross impurities from the air.
The tip of the nose is sometimes red, rough, and blotchy, owing to cold, indigestion, or other causes. It varies much in shape—pointed, flattened, bulbous, and almost bifid varieties frequently running in families (Figs. 83 to 88). Age often has much to do with the shape of the nose ; a prominent bridge is rare in childhood, but a cunning tip-tilt is common. Note also another characteristic which runs in families, and that is the extent to which the columna nasi is visible in profile (Fig. 83 A and B, p. 220).
The Mouth is as important an object in the study of expression as the eye. Just as the anterior nares form the entrance to the large nasal cavities, so the mouth, surrounded by the lips, is the entrance to the large buccal cavity which contains the tongue and teeth (Figs. 87 to 92).
There is a great distinction between the shapes of the upper and lower lips.
The lips of a well-formed mouth that is unspoiled by bad usage exhibit curves which are certainly among the most beautiful features of the face, and as certainly they are among the most difficult to describe adequately. It is not too much to say that a child’s mouth, which has not been pulled out of shape, is that part of the face which best repays close inspection (Fig. 88).

Fig. 87.—Nostrils and Mouth.
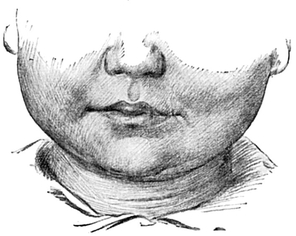
Fig. 88.—Dimpled Face of Smiling Child.
The two lips occupy rather different planes, the upper one, as a rule, projecting farther forwards than the lower (Figs. 89, 90).
The lips consist of muscle and a little fat, with a covering of skin and red mucous membrane.
The cutaneous surface of the upper lip shows a central vertical depression, beginning above at the septum of the nose, and terminating, after expanding a little, below, immediately above the middle of the red margin of the lip, which here is rather prominent (Fig. 87).
On each side of the depression is a ridge passing vertically downwards from the inner side of each nostril towards the upper lip.
The curved line of demarcation between the skin and the mucous membrane of the upper lip may be traced on each side from the middle line, where it is slightly depressed. It then turns upwards, and with a magnificent sweep downwards, nearly reaches the corner of the mouth, before it again passes somewhat upwards for a brief space. This lateral part is well seen in profile to lie below and behind the central part (Figs. 89 to 91).
The edge of the red margin, which actually bounds the oral fissure or chink between the closed lips, begins in the mid-line at the papilla, and passes outwards and upwards, then slightly downwards, and then upwards again, to reach the angle; but the curves here are not so pronounced as in the upper line of demarcation between skin and mucous membrane. The visible red area of the lightly closed lips is broadest in the middle, and dwindles away to nothing at the angle.
The line of demarcation between the skin and red mucous membrane in the lower lip lies in a nearly horizontal plane, but as it projects forwards in profile it is directed slightly downwards (Fig. 90). The edge which bounds the chink between the closed lips is concave upwards, and consequently the oral fissure is convex downwards in the middle third, and concave downwards on each side of this (Fig. 88) Lips vary very greatly in different races, and even in different ages and sexes, and are valuable exponents of character. We expect more fulness in youth, and are not surprised if in old age vertical wrinkles occur from wasting and withdrawal of support by loss of teeth (cf. Figs. 89, 90, and 75, 91).
The Chin.—The face terminates below in the chin, which is peculiar to the human being, but varies much in shape.
The chin is supported by the front part of the lower jaw, or mental protuberance, and like it may be pointed or square, prominent or retreating; occa-sionally, especially in broad chins, it may be surmounted by a central small pit of varying depth.


Mouth and Chin.
A deep transverse furrow separates the chin from the mouth (Fig. 90).
Very often, although not by any means always, the chin is a good indication of character.
Many men lack a good development of chin, and grow a beard to cover this deficiency. With their beard on they may have a strong face; without it, a weak one.
It may interest the student to consider the association of a small chin and weak character. If he will take the trouble to notice a man who has recently passed through a great physical struggle, he will find that the jaw is dropped, as if even the facial muscles, and the muscles of mastication, were tired. He is so tired and breathless that he cannot even keep his mouth shut. He is not in a position now to force home arguments, even to a child. His appearance of strength has gone. Depression of the jaw, then, is associated with great physical exertion and fatigue, so that the man is no longer quite himself. Depression of the jaw leads to an apparent retraction of the chin. The small chin is, therefore, associated in our minds with the man who is wanting in decision and in strength of character, because the depressed jaw is seen in the man who has not the physical force to make his will prevail.

Fig. 91.—Furrows around Mouth, Chin, and Neck.
The hair of the face deserves more than the passing consideration which can be given in these pages. First, be it observed, the man who can grow a good beard cannot necessarily grow a good moustache. The moustache varies very much. Sometimes it curves downwards, sometimes forwards, sometimes upwards. Sometimes it may appear asymmetrical. Sometimes, even in a young person, it may be different in colour from the beard.
Below the eyes, that part of the face known as the Cheek bulges a little forward in the average well-nourished adult. In the infant the bulging is more pronounced, owing to the presence of a mass of fat called the “sucking pad” (Figs. 92 and 93).
The emaciated may actually become “hollow-cheeked,” and then the zygomatici and other facial muscles may be identified when in action.

Fig. 92.—Head and Neck of Baby.
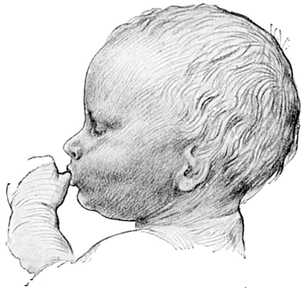
Fig. 93.—Child Sucking Thumb.
In edentulous or toothless persons the alveolar margins of the jawbones, which formerly contained the teeth, waste and the cheeks fall in (Fig. 75). The changes which the face undergoes with advancing age will be dealt with more fully in a succeeding chapter (p. 264).
The ear, the organ of hearing, consists of special sense as well as transmitting parts. The former or inner ear, and half the transmitting part or middle ear, lie deeply buried in the bones at the base of the skull, and fortunately the study of these is not expected of the art student, for they are extremely complicated.
The remaining half of the transmitting part, namely, the auricle and meatus, together constituting the external ear, forms a prominent object on the side of the head, and claims the attention of the art student (Fig. 94).
It should be noticed how well adapted the auricle is for collecting the waves of vibration which, when transmitted to, and interpreted by, the end organs of the auditory nerve in the inner ear, constitute sound. In respect of this function, however, the human auricle falls below that of certain of the lower animals, to whom hearing is of even greater importance than it is to man. They have not only larger but also more mobile auricles.
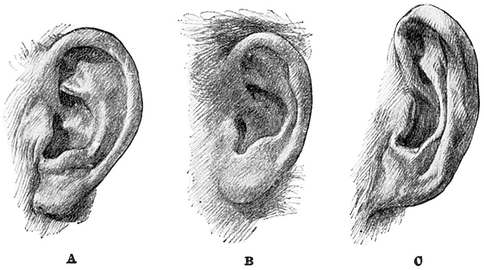
Fig. 94.—Different Types of Ear.
There is a little eminence on the curled-over edge of the auricle which is known as Darwin’s tubercle (Fig. 94 B), after the great naturalist who was the first to explain its significance. It is said to be more marked in members of the criminal classes. It is held to represent the extreme point of the auricle in the long-eared horse and ass, and thus to form one of the indications of the descent of man and beast from a common ancestor.
If the student will further observe the auricle of such an animal—for example, the horse—he will notice that it is capable of extensive movement. Owing to this great range of mobility, the open orifice of the funnel can be directed towards the back, side, or front of the animal, and thereby sounds can be collected from all quarters much more efficiently than by the fixed human organ. These movements are brought about by muscles which, in man, having undergone involution, are very tiny, and indeed quite rudimentary. Upon only a few members of the human species is the power of moving the auricle bestowed. Yet small muscles can be found by dissection of any auricle in exactly the situations to be expected.
One lies above the auricle, another behind it, and another in front of it. There are also some minute muscles lying on the auricle itself. All of them are, as one would expect, supplied by the seventh or facial nerve, because that is the nerve specially destined for the supply of all the muscles of expression. The student will quickly call to mind the very obvious influence produced by the movements of its ears upon the expression of a horse or a donkey.
The rigidity of the auricle, and the fact that when it is forcibly bent down it will recover its shape as soon as the pressure is released, indicate that it has some form of strong framework which is not bony. The support is afforded by a strip of cartilage folded upon itself and fixed within a bony orifice upon the outer surface of the temporal bone, known as the external auditory meatus.
The cartilaginous support of the ear is immediately under the skin, which is very thin in this region, there being no fat except in the lower extremity or lobule. For this reason, and because it is apt to get compressed against the hard skull, bruising is peculiarly frequent upon the ear. An unsightly swelling results, and has been depicted in ancient statues of boxers.
The external ear varies very much in size, in degree of prominence, in shape, in quality of skin, and even in colour.
Maltreatment during development is prejudicial to the beauty of any feature, and the auricle suffers perhaps as often and as much as any.
The bony parts in immediate relation to the external ear are as follows:—
Behind it is the mastoid process; in front of it is the ramus of the mandible, while below there is a deep hollow, which is to some extent filled up by the upper part of the sterno-mastoid muscle.
The auricle has various named parts. Thus the part hanging downwards, which is thicker and softer than the rest of the ear, is known as the lobe or lobule. Its substance is fatty, and it contains no cartilage. The lobule usually hangs free at its posterior and inferior edges, but is attached in front to the cheek and above to the auricle. It may be very large (Fig. 94 A and B), and may then have a free anterior edge as well; or it may be very small (Fig. 94 c), and hardly separable from the rest of the auricle.
This is the part of the ear which is perforated for ear-rings, and certain races specially cultivate it for supposed aesthetic reasons, hanging weights upon it for the purpose of increasing its length. Ear-rings have been considered a relic of this barbarous practice.
Above the lobule is the concha, a wide open depression which leads to the external auditory meatus. The incurved margin of the ear, which begins below and behind at the lobule and curves round the ear to the middle of its anterior border, is the helix. “Darwin’s tubercle” is situated in the upper and back part of this margin.
The concha is bounded at its upper and back part by a ridge known as the antihelix. The ridge bifurcates at its upper extremity, and is separated from the helix by a depression, somewhat in the shape of an elongated pear bent upon itself, called the scaphoid fossa.
The concha is prolonged downwards into a little bay, whose boundaries are the tragus anteriorly, and the antitragus situated at the back. The little bay has the name of the incisura intertragica.
Just above the tragus, and slightly in front of it, the crus helicis forms a prominence directed backwards into the fossa of the concha. There is no cartilage between this part of the helix and the tragus.
The auricle is apt to become red in cold weather, and it takes a part in the general reddening of the face known as blushing.
Large ears are often prominent. Ears may be nearly triangular in shape, broad above and narrow below. There may be hardly any lobule developed at all, and it may be closely attached to the side of the head.
Upon the back part of the side of the face a massive quadrate swelling is formed by the masseter muscle (Fig. 95), lying on the angle of the jaw. Its promin ence is much more noticeable when the jaws are clenched, and it can then be seen passing between the mandible near its angle and the zygomatic arch.
The outline of the contracted muscle may be sometimes obscured in the glutton by the over-development of a tongue-like lobe of the parotid gland, which lies horizontally upon the surface of the masseter.
In a face which has clearly cut and well - marked features, the following points should be noted by the student. There is a well-marked furrow, running from a point just below the inner angle of the eye, downwards and outwards, well on to the cheek. There is a second furrow below, and nearly parallel, continuous above with the fossa above the ala of the nose, and curved downwards below to pass just outside the angle of the mouth. Between these two furrows is the naso-labial fold. There is a third furrow passing in a curved direction downwards and outwards from the angle of the mouth. The furrows, or wrinkles, best seen in old people at the sides of the eyes, lie at right angles to the fibres of the orbicularis palpebrarum, and thus are disposed in a radiating manner.
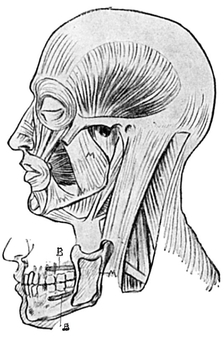
Fig. 95.—Muscles of side of Head, Face, and Neck.
M=Masseter. Inset of Jaws showing:—B. Origin of Buccinator. M. Insertion of Masseter.