Trauma to the Genitourinary Tract
Jack S. Elder
Etiology
Most injuries to the genitourinary tract in children result from blunt trauma during falls, athletic activities, or motor vehicle crashes (see Chapter 82 ). Children are at greater risk of blunt renal injury than are adults, because they have less body fat and because the kidneys are not located directly behind the ribs. Children with a preexisting renal anomaly, such as hydronephrosis secondary to a ureteropelvic junction obstruction, horseshoe kidney, or renal ectopia, also are at increased risk for renal injury. Blunt abdominal or flank trauma often causes a renal injury. Falling can cause a deceleration injury that results in an injury to the renal pedicle, interrupting blood flow to the kidney. If the bladder is full, blunt lower abdominal trauma can cause a bladder rupture. Rupture of the membranous urethra occurs in 5% of pelvic fractures. Straddle injuries usually are associated with trauma to the bulbous urethra.
Symptoms and signs of urinary tract injury include gross or microscopic hematuria, bleeding from the urethral meatus, abdominal or flank pain, a flank mass, fractured lower ribs or lumbar transverse processes, and a perineal or scrotal hematoma.
In more than 50% of cases, there also are major injuries to the brain, spinal cord, skeleton, lungs, or abdominal organs.
Diagnosis
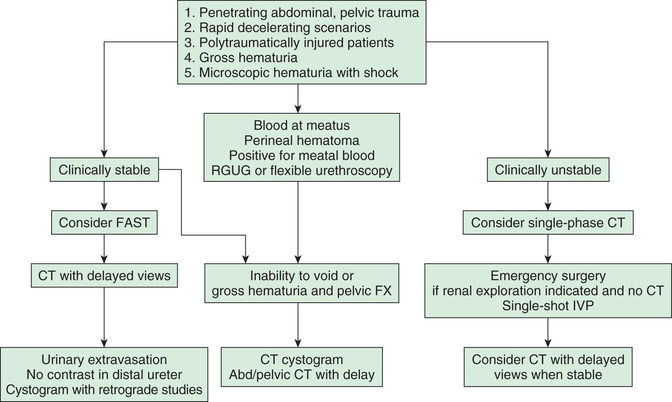
Evaluation of the patient begins after an adequate airway has been established and the patient is hemodynamically stable (see Chapters 80 and 81 ). With significant abdominal injury, gross hematuria or >50 red blood cells per high-power field, or suspicion of renal injury (deceleration injury, flank pain or bruise), renal imaging is indicated (Fig. 561.1 ). The bladder should be catheterized unless blood is dripping from the urethral meatus, which is an indication of potential urethral injury. Passing the catheter in the presence of a urethral injury can increase the extent of the damage and convert a partial membranous urethral tear into a total disruption. In these patients, a retrograde urethrogram should be performed by injecting radiopaque contrast medium into the urethral meatus under fluoroscopy. Oblique radiographs demonstrate the extent of the injury and whether urethral continuity is preserved or has been disrupted.
A 3-phase spiral CT scan should be performed to evaluate the kidneys, ureters, and bladder. The delayed images are important to detect renal extravasation of blood or urine. Prompt function of both kidneys without extravasation usually excludes significant renal injury. Renal injuries are classified according to the grading scale presented in Table 561.1 . Minor renal injuries are most common; these include contusion of the renal parenchyma and shallow cortical lacerations not involving the collecting system. Major renal injuries include deep lacerations involving the collecting system, the shattered kidney, and renal pedicle injuries (Fig. 561.2 ). Complete absence of function of one kidney without contralateral compensatory hypertrophy (indicating congenital absence) should be regarded as an indication of major injury to the renal pedicle. Renal angiography, once used for further evaluation of renal injuries, particularly if a renal pedicle injury is suspected, now is rarely used because such patients are often hemodynamically unstable, and management is not significantly affected by the findings. In some cases, a preexisting renal anomaly is demonstrated on the study. A ruptured ureteropelvic junction obstruction may be apparent if the kidney is intact but the distal ureter is not visualized.
Table 561.1

If there is a pelvic fracture, a urethral transection injury should be suspected, particularly in males. The risk is directly related to the number of broken pubic rami and whether there is separation of the pubic symphysis or displacement of the posterior pubic arch. Radiographic evaluation with retrograde urethrography should be performed if there is blood at the urethral or vaginal meatus, inability to void, and a perineal or penile hematoma.
Treatment
Minor renal injuries such as contusions are managed by bed rest and monitoring of vital signs until abdominal or flank discomfort and gross hematuria have resolved. Children with a major renal injury usually are admitted to an intensive care unit for continuous monitoring of vital signs and urine output. Intravenous antibiotics are also administered. These injuries also are managed nonoperatively, because Gerota's fascia often causes tamponade of bleeding from the kidney, and dramatic healing of the injured parenchyma can occur even with significant urinary extravasation.
Approximately 10% of children with a major renal injury undergo surgical exploration because of associated abdominal injuries, hemodynamic instability, persistent extravasation, or persistent hematuria or to correct a congenital renal deformity. It can be difficult to identify normal and devitalized parenchyma, and the likelihood of having to remove the kidney is significant. If the child is undergoing exploration for other abdominal injuries, the injured kidney is examined. If there is persistent extravasation because of intermittent ureteral obstruction from a blood clot, passage of a temporary double-J stent endoscopically between the bladder and kidney might allow resolution. If the renal pedicle is injured, nephrectomy is necessary. The kidney can be salvaged by emergency renal revascularization only if the kidney is explored within 2-3 hr of the injury. Virtually all penetrating injuries of the kidneys should be explored.
In addition to loss of renal function, the main long-term complication of renal injury is renin-mediated hypertension. Children who sustain significant renal injuries should have periodic measurement of blood pressure if they have any residual renal abnormality.
Ureteral injuries usually are iatrogenic. Injuries of the ureter by blunt or penetrating trauma require immediate surgical attention.
When the bladder can be catheterized, a static cystogram is obtained, infusing a contrast solution through the catheter by gravity, ideally using fluoroscopy. Flat and oblique views are often obtained; a postvoid film also should be obtained because, in some cases, extravasation may be hidden by the full bladder. An alternative is a CT cystogram, which is highly accurate in demonstrating a bladder injury.
Bladder ruptures can be intraperitoneal or extraperitoneal. All intraperitoneal ruptures require surgical repair. Minor extraperitoneal near-ruptures might be treated by catheter drainage but generally require surgical treatment.
Treatment of a membranous urethral injury is controversial. Erectile dysfunction, urethral stricture, and urinary incontinence are the major late complications of rupture of the membranous urethra, and therapy is directed at minimizing the risk of these problems. A large pelvic hematoma with tamponade often is present, and an immediate attempt to repair the injury can be technically difficult and result in significant hemorrhage. Many such injuries are managed initially by temporary suprapubic cystostomy, with continuous bladder drainage for 3-6 mo. Subsequently, open or endoscopic urethroplasty can be performed. Alternatively, some try to achieve urethral continuity under anesthesia and leave a urethral catheter for several months. These patients typically require subsequent open urethroplasty.
Penile injury is uncommon. Partial or complete glans amputation is a risk of newborn circumcision with a Mogen clamp. With immediate surgical repair, often the excised glans tissue can be replaced as a free graft. Some males who are in the process of toilet training sustain an injury to the glans penis if the lid of the toilet falls while they are urinating. These males often have a hematoma covering the distal half of the glans. Typically, they have no difficulty urinating and do not need extensive evaluation. Some male infants develop an inadvertent hair coil tourniquet or strangulation injury. Typically, a very narrow constriction is noted with severe distal penile swelling and pain. Identification and incision of the hair allows prompt resolution of the edema. The urethra and penile vascularity should be assessed after release of the hair coil. Adolescent males who indulge in extremely vigorous sexual intercourse may sustain rupture of one of the corporal bodies. These males have severe swelling of the penile shaft and require emergency exploration and repair. Males with penetrating injuries of the penis also require emergency debridement and repair.
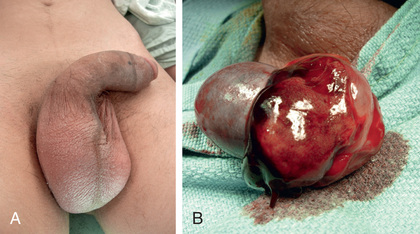
Testicular injuries are relatively uncommon in children because of the small size of the testes and their mobility within the scrotum. Such injuries usually result from blunt trauma during athletic activity. Typically, these males have significant scrotal swelling, testicular pain, and tenderness (Fig. 561.3A ). Ultrasonography demonstrates rupture of the tunica albuginea, which is the capsule of the testis, and surrounding hemorrhage. Prompt surgical treatment of testicular injuries increases the salvage rate (see Fig. 561.3B ). An uncommon injury is the zipper injury, which can affect either the scrotum or foreskin. This problem generally occurs in males who do not wear underwear. The zipper can be cut with bone cutters or metal cutters. Sedation generally is unnecessary.