

I don’t like the word ‘plan’. Any plans you make in life – weddings, job interviews, holidays – almost never go exactly the way you thought they would. You have to expect the unexpected. So rather than ‘planning’, think of it more as ‘preparing’. This is why I use the term ‘birth preferences’. A birth preference is a much more positive way of looking at labour and birth. We’d all prefer sunny skies on our wedding day but you can’t let rain ruin the day.
The aim of a birth plan is to communicate your wishes to the people who will care for you in labour. It’s a nice way for us midwives to get an idea of what a couple is like, especially if we haven’t met them before. We’re pretty good at getting to know couples fairly quickly in a short space of time! There are no hard-and-fast rules for how to do it, but below are some good starting points. Remember, though, that births can be unpredictable, and if you’ve not experienced it before, then you may well feel differently on the day. So allow for flexibility. The best way of ensuring things go to plan is by acknowledging that they may not always go to plan.
• Do your research: find out what’s likely and what’s possible where you have chosen to give birth (see chapter 3).
• Gather information but fight the fear: understand the process and reality of birth but don’t get bogged down in labour stories from hell. This is your baby’s birth! Fear is your enemy; kick it to the kerb now.
• Talk to your birth partner: explore what both your priorities are, and if there’s anything you’re worrying about, address it together.
Discuss and write your birth plan with your birth partner, so you are on board together. For example, you need them to know and understand why you may not want to be lying on your back for the pushing stage, or why pethidine isn’t a great option if you’re hoping to stay active and use the pool. During labour you want someone to be your advocate and voice. Labour is hard work and requires all your energy and focus. You don’t want to have to answer the midwife’s questions mid-contraction. And always allow for a change in your preferences, i.e. ‘I’d like to use the pool for labour but if it is recommended that I need to be continuously monitored I would like to stand/use the ball/use the mat/sit on a chair so I’m not on the bed.’ Keep your options open. Now jot some things down – some key things to consider:
• Who is your birth partner? Where do you want them to be, when?
• What positions do you want to consider for labour/birth? (see here)
• Pain relief and what order you’d like it in: include here any specifics like hypnobirthing techniques or massage (see here and here).
• What you want to do in the event that labour has slowed?
• Do you want to use a pool or any other equipment, e.g. birthing ball?
• Do you want baby monitoring? If so how are you happy for this to happen?
• Do you want a Managed or Natural Third Stage (placenta delivery)? See: www.nice.org.uk/guidance/cg190/ifp/chapter/delivering-the-placenta
• Who do you want to cut the cord?
• Do you want skin-to-skin when the baby is born, if possible?
• Vitamin K for your baby – oral drops or injection? (Talk to your midwife.)
• What are your hopes and requests for feeding your baby?
• What do you want to happen in unexpected situations? For example, if your baby needs to go to SCBU do you want your birth partner to go with them or stay with you?
• Any particular requirements, e.g. religious needs or language difficulties?
Pop a copy of your birth preferences in your maternity notes and make sure your partner shows it to your midwife when you’re in labour. As the big day approaches, go back and review your choices to make sure it’s still what you want. Remember, you can always change your mind. And don’t put too much pressure on yourself: if you need an epidural because you’ve been in early labour a long time and had no sleep, then that’s what’s right for you at that point. Never feel guilty or beat yourself up about the choices you’ve made, because they will always be the right choice at the time.
I think it’s really important to know and understand the stages of labour, what will happen and when key things will happen. This will help you to know when to go into hospital/phone for a taxi/call the community midwives (if you’re planning a home birth). But like anything, biology doesn’t always follow the rules and if this isn’t your first baby, times and lengths of labour may differ. Remember that we are all made up differently and don’t perform in exactly the same way.
First stage or early/latent phase
This is usually the longest stage of labour so it’s probably the stage that you should understand the most. However it’s usually the stage that the majority of first-time mums overlook. I always like to tell women that labour is like running a marathon (I’ve never run a marathon myself but I have gone through three, well, four labours if you count both of the twins). You never start a marathon using up all your resources and energy; you start slowly, pacing yourself as best you can. Labour is no different.
So let’s start with a carrot, because your cervix is like a small carrot. It’s not orange but it’s long and firm, and by the time you’re in established or active labour (5cm dilated) it’s completely changed shape. It’s moved forward, shortened, opened, dilated and softened. Imagine your cervix is now like the opening of a sock. So that’s quite a bit of change it’s got to make and this is why it can take several days of early labour to do so. During the first stage of labour you may experience:
• Backache, period-type pains.
• A vaginal bloody show (the mucus plug that sits in the neck/opening of the cervix).
• Short irregular contractions.
• Your waters might break (but these can break at any stage of labour, even as the baby is being born).
• Diarrhoea, nausea or you may even actually vomit.
A contraction can feel like a stronger version of a period pain, but everyone feels them differently.
It felt like griping pains, like when you have a bad stomach bug. It came and went and built in intensity and my tummy went really hard, like a big rock!
Louise, mum of one
Women often get really excited when they think they’re going into labour, and why not? Of course it’s exciting – but remember the marathon analogy: take it slowly. If your contractions are short and far apart you are not going to push a baby out any time soon.
When thinking of the best positions for labour, remember UFO: U for Upright, F for Forward and O for Open. Any position where you are upright, forward and open is great. When upright you obviously have gravity on your side, and by leaning forward you’re encouraging the baby into the optimum position for birth, as the weight of the back of the baby’s head will be round to the front of you as opposed to resting against your back. By open I mean your legs are apart and you are creating room in your pelvis rather than restricting the space. This will make life, or at least labour, easier for you.
Some really useful things to do to help you through this stage include:
• SLEEP/REST: The number of women I know who charge around the park or walk up and down the stairs from the first twinge baffles me. Doing that, you will without doubt completely exhaust yourself. If it’s early labour, rest while you can. If the contractions slow down and stop altogether go to bed or make a nest on the sofa, draw the curtains, switch off your phone, and smell some lavender. You will be so grateful for any snippets of sleep you can grab now and your body will thank you for it when it really needs the energy later on.
• DISTRACTION: If your partner is at home with you, stick on your favourite box set. Why not stand and do some cooking? (Remember UFO – Up, Forward, Open.) This will help the baby to get into a good position in your pelvis. Plus a home-made lasagne in the fridge will be very much welcomed when you come home from hospital and are starving hungry!
• EAT/DRINK: When you’re in established labour, you’re less likely to feel hungry, so eating and staying hydrated in early labour is vital. You need food that is jam-packed with slow-releasing energy: porridge with fruit and honey, a big bowl of pasta, and peanut butter on toast are great. Coconut water is full of antioxidants and great for when you need hydrating. (Make sure you pack some in your hospital bag, see here.)
• RELAX: Get in the deepest bath possible, light a candle, put on your hypnobirthing tracks and stick a pair of headphones in your ears. Switch off from the world and focus on your baby and body. It’s doing an amazing thing but it takes time, so don’t try to rush it. Practising your breathing exercises at this stage is a fantastic way to find your rhythm so that you find it much easier to use later on, when labour is established.
• MASSAGE: Now is the perfect time to get your partner to show off their massage techniques. Remember to focus on your shoulders, lower back and feet. (See pregnancy massage, here.)
You may begin to notice a rhythm or pattern with the contractions, so you could start to time them using an online app or just getting your partner to jot them down. As a rough guide, contractions in early labour are usually more than 5 minutes apart and only last between 20 and 30 seconds. Remember, if they are short and irregular it’s probably too soon to be thinking about calling your midwife or going to the hospital. You’ll only be disappointed if you go in too soon and are sent home again.
So when should you to go to the hospital/call your midwife if you’re planning a home birth?
• First baby: your contractions are every 3 minutes, lasting at least 40 seconds and are strong and regular.
• Second baby: your contractions are every 5–7 minutes but are strong and regular.
Remember you should always call your midwife if:
• You have a heavy ‘show’ of bright-red blood (heavier than a period).
• You feel your waters breaking (this is when the amniotic fluid leaks out through your vagina), especially if they are brown, green or smelly.
• Your baby’s movements slow down.
• You are worried about anything.
Active phase
This is when you’re in business and hopefully labour won’t stall or stop if you’ve remained as rested as possible in the early/latent phase. You may already be in the hospital at this point, or your midwife will have come to your home if you’re planning a home birth. You will be offered a vaginal examination to assess how dilated (open) your cervix is at this point. Try not to focus too much on this, though: it’s just a number and doesn’t necessarily determine how long your labour will be. Remember, your body is amazing and your cervix is now dilated at least 5cm. Your contractions are strong and regular, coming about every 3–4 minutes and lasting at least 45 seconds. You may feel these contractions in your back or across your uterus and won’t be able to talk through them; up-breathing (see hypnobirthing, here) is brilliant for getting through these contractions. It’s important to remain (if possible) upright for this stage, rather than lying on your back, as you want your baby’s head to be well applied to your cervix to encourage dilation.
If you have had an epidural by this point, ask your midwife and partner to encourage you to change position on the bed; lying on your left side and even going on your knees and leaning over the back of the bed is really beneficial. If you’re mobile (which may not be the case if you’ve had an epidural) ask to use a birthing ball, mats and bean bags – in hospital they may not be visible but are often kept in storage cupboards.
As the contractions are now closer together a few useful tips on how to manage the gaps in between include:
• Small sips of water or coconut water via a sports bottle or cup with a straw.
• Try to empty your bladder every hour as a full bladder can make it harder for your baby to get into a good position (sitting on the loo is a good position to try for a bit).
• Keep lighting low and noises minimal – you want to feel safe and calm.
• Wiggle your hips and pelvis to keep everything loose and open.
• If you’re in the pool ask your partner to pour warm water over your neck and shoulders.
Contractions in the active phase tend to maintain their momentum and open your cervix more rapidly, but it may still be many hours before your cervix is fully dilated. Take it one step at a time and remember that each contraction is bringing you closer to meeting your baby. You can do it!
Transitional phase
This is when you move from the first stage of labour to the second stage. It usually starts when your cervix is about 8cm dilated, and ends when your cervix is fully dilated, or when you get the urge to push. Your contractions may space out a bit but are much stronger and longer-lasting. It’s common for waters to break just before, or during, transition. As your cervix becomes fully dilated, you may have another show of blood.
As women experience transition in different ways it’s hard to tell how you will be. Try to remember that it’s okay to feel scared, vulnerable, overwhelmed and emotional. You may feel zoned in to your labour and only able to make abrupt demands (I snapped at my husband many times at this stage). You may make noises that you can’t control, you may shout and feel impatient with everyone, but this is okay: your body is about to do something amazing. Your midwife will be very experienced at knowing how to support you and your partner during this stage.
If you’re planning to give birth without pain relief, this may be the most testing part of labour for you and your birth partner. You may want to tear up your birth plan or demand an epidural, even though you’d hoped to avoid one! Or if you’d planned a home birth, you may now want to go to hospital. All of these feelings are normal and with lots of support and encouragement from your midwife and partner you will get through this next stage – your baby will be born soon!
During my home birth I asked for someone to get my shoes and coat as I wanted to go to hospital. I have no idea why I wanted to go; it was just something I kept saying. Obviously there was no clinical reason why I should be transferred and before I could think about anything else, the sensation of pressure increased and my baby was born 10 minutes later!
Kate, mum of one
Pushing stage
This is it: the past 40-odd weeks are almost over and you’re about to meet your baby for the first time! If you haven’t had an epidural the only way to describe the second stage is like needing to do a massive poo. Someone once said to me it felt like she was ‘vomiting out of her bum’! What she meant was that there is no way you can hold back; your body is amazing and literally wants to expel your baby by pushing down on all your nerves in your bottom. Getting into a deep squat, on to a birthing stool or on your knees are the perfect positions to get pushing: no one can go for a poo lying on their back. With every contraction you need to work with your body and push your baby’s head down into your pelvic floor. Sometimes it takes practice, so don’t worry if you don’t get it at first – your midwife will help you. They may use a torch and mirror to see if they can see your baby’s head and help you to push in the right place. You may want to put your finger inside to feel how close your baby’s head is to being born: trust me, giving birth is not about dignity. As your baby is close to being born you may feel a hot, burning sensation as the widest part of the head stretches the skin around your vagina and perineum. This is when all that perineal massage really pays off and hopefully your baby’s head stretches that skin without causing any tearing.
So some tips for pushing include:
• Get into any upright position – gravity is your friend!
• Work with your body – this is it, you’re almost there.
• Every push brings your baby lower and closer to being born – don’t give up.
• Remember to breathe slowly as the head is being born (or crowns); it will allow the skin to stretch and not tear.
• You can ask for a warm compress, such as a flannel on your perineum, to ease the burning sensation.
Third stage
You’ve done it! All that hard work and your wet, squishy baby is out! They may not be pink straight away – that’s normal – a few good cries and all that oxygen will turn their skin to a healthy colour. They may be covered in white cream called vernix, which is the amazing moisturiser that has kept their skin in perfect condition while they’ve lived in water for the past nine months. Keeping them skin-to-skin with you (or your partner) is a lovely way to keep them warm, regulate their breathing and calm them down.
As this is all going on your midwife will keep a close eye on your bleeding. It’s now recommended that babies’ cords are left attached, to pulsate, which basically means the blood flowing from the placenta to the baby isn’t cut off with a clamp as that extra oxygenated blood is so important for your baby. Your midwife may recommend you have an injection of a hormone called syntocinon into your thigh to help contract your uterus and help your placenta come out. You may, however, decide not to have this injection and opt for a natural delivery of the placenta. It’s best to be open-minded about this and see what your midwife advises at the time.
Either way, the best news about your placenta – it’s soft! It will literally just fall out with some gentle pulling on the cord, and it’s like a large piece of liver. Don’t worry if you don’t want to see it – lots of people aren’t keen, but you may be surprised at how amazing it is – after all, it has kept your baby alive for 40 weeks! Your partner may want to look at it or photograph it, so you can look at it later when you’re feeling a bit more normal. Some people choose to keep their placenta – to eat, encapsulate (freeze-dried and made into tablets) or bury in the garden. You can pretty much do what you want with it, so discuss with your partner in advance. If you do choose to take it home it’s best to have a large plastic box with a lid to carry it in.
Preparing for the birth of your baby can be a daunting time, both physically and mentally. But it’s important to remember that you are a strong and capable woman! A quick and easy way to start thinking more positively is to start each day with some powerful affirmations.
This simple habit can have an amazing transformative effect on your mindset. Write down your favourite positivity quotes or buy a pack of cards with inspiring affirmations already written on them, and then keep them by your bed, in your handbag, anywhere within reach so that whenever you are having a wobble, you can pick a new card and read it aloud and embrace an encouraging message.
Calmness, confidence and self-belief are great for dealing with those tricky moments during pregnancy, and when you come to the actual birth, you can recall all of those positive thoughts you’ve had during your pregnancy.
Each affirmation acts like a tiny fist-pump to yourself: a reminder that YOU CAN DO THIS! So go, mama!
I had never known that a home birth was an option for us before we discussed the birth with our midwife. The thought of being in hospital gave me the willies; I have a phobia of both me and other people being sick, so a labour ward was the sort of place I wanted to give a wide berth (excuse the pun). The thought of taking that anxiety out of labour was the initial appeal, but quickly other pros mounted up, and all I kept thinking was that we could change our minds at any point and go into hospital if we wanted. Planning a home birth gave us a choice.
When I first mentioned a home birth to my husband, Guy, he was against the idea. He was worried about the possibility of something going wrong. Both our fathers are retired doctors and were sceptical, which added to his hesitancy. I kept reminding him that we could transfer to the hospital at any point – we weren’t ruling anything out. It took a few weeks of mulling it over, but eventually Guy came round to the idea, supporting my decision.
Guy and I spent a lot of time preparing for the birth: Guy looked after the logistics, working out how to set up the pool and find the right adaptor for our taps. I focused on getting myself in the right physical condition and mindset. I was doing lots of exercise, such as yoga, swimming, step and resistance training. I was also doing my pelvic-floor exercises and perineum massage. I listened to a hypnobirthing track as I went to sleep at night, and also found it really useful in helping me get back to sleep when I was struck with insomnia.
1:27 a.m.
I was five days past my due date when I felt my first contraction. I woke up at 1:27 a.m. to a strong tightening in my stomach that faded away. I lay still, wondering what would happen next, and shortly after felt the same sensation rising and falling.
I slipped out of bed, not wanting to wake up Guy, and went to lie down on the sofa. I put on my hypnobirthing track, taking the opportunity to nap between contractions, which at this point were around 8 minutes apart. After two 40-minute loops of the track, the contractions were getting stronger so I put on a DVD of Cold Feet, one of my favourite TV series, to distract me and moved on to my birthing ball. As the contractions came, I rested my head on the arm of the sofa, rolled my hips on the ball and closed my eyes. I had set myself the target of 6 a.m. to wake Guy. When 6 a.m. arrived, I still felt pretty relaxed, so I decided to hold out for another hour. Just after 7 a.m., I went into our bedroom, nudged Guy gently and whispered, ‘Guy, the baby’s coming.’ His eyes burst open and he leapt up. ‘Really? Where? Now?’
Once Guy had properly woken up, I updated him on the past hours. Together we timed a couple of contractions, had some breakfast, got showered and dressed and at 9 a.m. paged our midwife to let her know that our baby was ready.
The midwife on call called us back soon afterwards. We chatted about my progress and how I was feeling, ‘That all sounds great,’ she said reassuringly. ‘Keep doing what you’re doing – lots of walking around and moving – and give me a call again when the contractions are three minutes apart, and really strong, so strong you can’t think or talk through them.’ Before putting down the phone, she said, ‘Each time a contraction comes, say to yourself “bring it on”. The bigger and stronger, the more you’re progressing.’ It was a piece of advice that carried me through the labour.
We called our immediate families to let them know that we were on, and were brought to tears by a call with Guy’s mother, who explained that she’d secretly hoped that the baby would make an appearance today as it was the 12th anniversary of the death of her father, our baby’s great-grandfather, a very special man.
9:30 a.m.
It was a beautiful, sunny, autumnal Sunday morning, so Guy and I headed out to our local park for a walk. We picked up coffees and walked slowly around our favourite wildlife garden, talking about our baby, its names and our hopes and dreams for him or her. Guy was keeping track of the contractions and would say, ‘You should be having a contraction around n—’, and on cue I would feel one rising.
After about an hour of walking, the contractions had increased in intensity and we headed home. Along the way the contractions would stop me in my tracks and I would need to crouch down on the path or lean on a tree until it had passed. During one contraction, I remember a young family passing us, smiling and giving us the thumbs- up. Once home, we attached the TENS machine. I returned to the birthing ball and Guy started setting up the birthing pool in the back room of our flat. The contractions were coming every 3 minutes, but I could still think and talk through them so knew I just needed to keep going – Guy and I would count together (he’d call from the back of the flat) so I knew how long until it would pass; I knew when we reached 20 seconds that it was going to ease again.
11 a.m.
Around 11 a.m. the contractions reached such an intensity that we decided to call the midwife. The midwife explained to Guy that she was up at the hospital with a new mother (her first delivery of the day) and that she’d be with us within the hour. When I opened the door to her, it was a huge relief and I burst into tears.
Our midwife was fantastic. She walked in, sat me down and chatted to me about how I was feeling, watched a couple of contractions, checked the baby’s and my heart rates, and then examined me. ‘You’re 3cm dilated. I’m going to stay.’ The golden words; I was so relieved.
From this point it was all about progress, ‘bringing on’ the contractions. I’d been sitting on my birthing ball, rotating my hips, using my TENS machine and breathing to relax through the contractions (pursing my lips and breathing out ‘golden spirals’), but to get things going, I needed to move around. I got to my feet and started pacing up and down our hallway, looking for places to lean on as the contractions washed through me.
Guy had just served our midwife some lunch when her phone rang. My ears pricked up when I heard her say, ‘I’ll be with you in five minutes, I’m just around the corner.’ The midwife put down the phone and said to Guy, ‘There’s a lady round the corner pushing with her second child. I’m afraid I have to go. You’ll understand when you have a second child. I’ll be back as soon as the other midwife on call gets there.’ And she ran out the door.
There was nothing else to do but carry on as we were doing. I continued pacing while Guy started filling the pool. I remained calm for around 45 minutes before I started longing for her return. I sat myself at the front window and gazed out at the road, squinting at every car that passed, asking Guy, ‘Is that her?’
3 p.m.
Within the hour, she was back. This time, when she walked in, she was wearing a smock and carrying lots of bags of medical paraphernalia. I thought to myself, ‘This is more like it!’ Our midwife had reached the other house five minutes before the baby had arrived – her second delivery of the day. The second midwife had arrived shortly afterwards, having had to hitch-hike a lift in a police van (a story in itself). It was an extraordinary day for our midwives.
The midwife carried out more checks and suggested I get in the shower for a change of scenery. I stepped into the shower and got down on all fours, and what a relief it was. Initially, I thought that the shower was slowing down my progress as the contractions eased, but it was actually relief from the warm water. I remained there for what I thought was 30 minutes, but was actually 2 hours. Guy kept popping his head round but I just apologetically asked him to leave me. I felt very calm and just wanted to be alone and focus on the contractions. The midwife intermittently, quietly and discreetly, came in and checked our heart rates. Hearing the little heartbeat of my baby was amazing. It was a constant reminder to me that this was a team effort, I was not alone. My little baby was going through something even bigger than me and remaining calm. I was so proud.
6 p.m.
At around 6 p.m., I asked the midwife what my options were. I felt like I was having contractions that seemed to go on and on, running into each other. I was disappointed that my waters hadn’t broken and I was worried it was holding my progress back. The midwife suggested another examination and then to get into the pool. The examination confirmed I was progressing well and had reached 7cm. She described my waters as ‘bulging’.
7 p.m.
I made my way down to our back room, where Guy had created the most beautiful space around the pool with candles and music. As soon as I saw the water I virtually dived in. As I submerged, a contraction took over me, and at the same time I felt my waters pop. The midwife tucked herself discreetly to my left and Guy to my right. The midwife left Guy to do the encouraging while she wrote up my notes and calmly answered questions and monitored everything. About an hour later I started feeling the urge to push. At first I didn’t really know what I was doing but after a few attempts the midwife suggested I keep my voice low and explained that I had strong but short contractions so to really try and drag them out. Guy was incredible: encouraging me, filling up my water bottle and reminding me to drink, filling up the pool with warm water and keeping so calm. He went through waves of emotions; laughing, crying and quietly just absorbing the atmosphere. I remember it being dark and very calm – probably because I mostly had my eyes closed. I felt very safe, focused and supported.
9 p.m.
After an hour of bearing down I was tired. I had only eaten a piece of toast and my energy stores were getting low. Guy knelt beside me and said, your next push is going to be for Poppy (my niece). As the contraction rose I thought of Poppy’s little face and I found a new strength. Next up was my grandmother, followed by Guy’s grandfather (whose anniversary it was) and it carried on.
Shortly afterwards we were joined by our second midwife. This arrival was another huge help: I knew I must be getting close if back-up was arriving. I remember feeling something, like a little nose nudging; one more push and the baby crowned. My immediate reaction was to leap out the water and jump up and down, but the midwives told me to breathe and listen very carefully as I needed to do some very small pushes to avoid tearing. I followed their instruction and felt the head deliver. I remember looking down between my legs and seeing a torch light flashing around. The midwife told Guy to join her and showed him our baby’s face in a hand mirror – its little eyes blinking and head looking around.
9:28 p.m.
With the next and final contraction I pushed the rest of the body out. I reached down and lifted my baby up in front of me. The midwives spotted that the cord had got tangled around the baby’s neck, so they both quickly jumped in and unwound it. I then lifted the baby out the water. ‘It’s a girl,’ I announced, followed by, ‘and she looks like your dad, Guy.’ In the background INXS’s ‘Beautiful Girl’ was playing. It was a moment of my life that I will never forget.
I sat back into the water and the midwives placed my daughter in my arms and latched her on to feed – her body submerged in the pool to keep warm, with a little hat on her head and a towel over her shoulders. Once all the goodness had been pumped from the placenta, Guy stepped forward and cut the cord, separating my little baby and me for the first time. We sat for 20 minutes while the midwives filled out the paperwork and made a round of tea. Guy took our daughter for some skin-to-skin and I stayed in the pool while we waited for signs that the placenta had detached. After 45 minutes, the midwife stoked up an injection to speed up the process and as I stood up to have it administered, I spotted drops of blood in the water. With one final push (I really didn’t think I had it in me), I delivered it!
11:30 p.m.
By 11:30 p.m. our wonderful midwives had weighed our daughter, administered a vitamin K injection into her little leg, completed the paperwork, cleared up the placenta and were ready to go. Our daughter was the third baby they had delivered that day – they are superhumans. We thanked them for everything (how do you even start to thank people who have just done what they did?), and I took our baby to our bed, where we rested and fed. Guy emptied the birthing pool – with a whisky – and when it was all cleared joined us in bed. Just the three of us; our new, wonderful family.
Knowing about TENS, epidural and other pain-relief options ahead of the birth can help you make confident decisions. Remember to stay open-minded: you make the choices that are right for you at the time.
TENS (Transcutaneous Electrical Nerve Stimulation)
A TENS machine sends mild electrical impulses to your back via electrode pads that stick to your skin. You remain in control of the strength of the pulses, which can be varied, using the controls on the machine. The TENS machine is essentially a form of pain relief but it doesn’t involve any pharmaceuticals, so has no effect on your baby and also means you are able to be fully present and not left feeling out of control in any way. The electrical pulse it produces stimulates the body to produce endorphins, which are the body’s natural pain relief. If you use the TENS machine from early on in labour you’re essentially filling your body with endorphins, meaning you can enjoy a more comfortable labour, even when everything is established and contractions are coming thick and fast. You can buy or hire a TENS machine, so make sure if you choose to use one you allow for enough time – no one likes a last-minute online panic!
Advantages:
• Portable, so can be used while staying mobile/active.
• Works well in early labour (you can stay at home longer in the first stage).
• No effect on baby.
• You control the strength of the pulse you receive.
Disadvantages:
• You can’t use it in the pool (water and electricity don’t mix!).
Water/birth pool
A lot of women often ask me if using water in labour means you have to give birth in the pool – well, the answer is absolutely not! Using water can be anything from having a lovely bath in early labour at home, standing in the shower with the shower head onto the bottom of your back or using a birthing pool once in established labour. You can even use the pool for pain relief but deliver your baby out of the water, if that’s your preference. Remember to be open-minded. I’ve looked after women in labour who weren’t even sure they liked the idea of using the pool but once they got in they didn’t want to get out and ended up having a beautiful water birth. I’ve also cared for women who used the pool throughout their entire labour and got out at the end and birthed on dry land. Have a chat with your midwife and find out your options.
One study found that only 24 per cent of first-time mothers who had water births needed pain-relieving drugs compared to 50 per cent of those who didn’t use water.
Questions to think about include: does the hospital have birth pools available and if so how many? Most UK midwives should be trained in supporting women who wish to have a water birth, so if your midwife on the day isn’t confident, for whatever reason, it’s worth asking for another midwife to care for you. If you’re thinking about having a home birth it’s worth exploring your options for having a pool set up at home. You can hire them or buy them new online, or even purchase second-hand ones – just make sure they’re fully sterilised with disinfectant and always use a brand-new sterile liner. You need to check your tap adapters and water pressure. It’s not overly complicated, but I’ve seen some very stressed-out partners trying to fit the hose pipe to their tap via all sorts of methods (gaffer tape, a cake-piping nozzle). It’s not what you want while you’re in labour, so make sure you know what you’re doing well in advance.
The pool was amazing. The hot water made me feel relaxed and seemed to take the pressure off my back and pelvis. I never wanted to get out.
Karmel, mum of one
Advantages:
• Calms you down and reduces anxiety – which lessens your perception of pain and gives you confidence in your ability to give birth. Go, mama!
• Supports your weight and makes it easier for you to stay upright, helping your pelvis to open up so your baby can pass through. The buoyancy of the water also makes it easier to change positions to help with contractions.
• Reduces the risk of tearing. The water softens the tissues of your perineum (see here), making them more supple and able to stretch to accommodate your baby’s head as it passes through. This also means you’re less likely to need an episiotomy.
• Relaxing in warm water helps the production of pain-relieving endorphins.
• You can combine it with other forms of pain relief, including gas and air (see below), massage, acupressure and aromatherapy.
• It’s peaceful! The pool itself is a quiet, private environment, which helps you feel safe and secure. Some women want their partners in the pool with them or to stay right next to them, supporting them.
There was no way my husband was getting in the pool with me – not only had I weed in the pool, but the pool was my sacred space, which belonged to me. He was brilliant at holding my hand through the contractions, changing the music and refilling my water bottle.’
Katie, mum of two
Disadvantages:
• The water may make you too relaxed and slow your labour down (it’s recommended that you’re at least 5cm dilated and contracting regularly before you use the pool).
• If there are any reasons why your midwife recommends that your baby’s heartbeat is monitored continuously on a CTG machine (e.g. if the baby has pooed during labour). Some hospitals offer wireless monitoring of your baby called telemetry – speak to your midwife for more information.
• You can’t use a pool if you have had pethidine or an epidural, although you can have either after leaving the pool.
Gas and air is a mixture of oxygen and nitrous oxide and is breathed in via a mask or mouthpiece. It’s available in all hospitals and birth centres and if you’re planning a home birth your community midwives will bring it to your home. It won’t take away the pain/sensation of the contractions but it will relieve them by making you feel a bit like you’ve had a few too many gin and tonics. It takes about 15–20 seconds to work, so make sure you start inhaling it at the beginning of the contraction so it’s kicked in by the time you reach the peak of the contraction. It takes a few seconds to wear off, which is when you might feel a bit giddy, spaced out or even really giggly (I’ve seen women in absolute hysterics after using it!).
Advantages:
• It has no side effects for the baby during labour.
• Combined with the pool it can be all you need for pain relief.
• It’s very accessible – you can use it in the bath, pool or shower as the pipe is relatively long.
• In hospital it never runs out! (At home the midwives will have a supply of canisters but may need to get more from the hospital.)
Disadvantages:
• It may make you feel sick (however this is often the effects of labour), but you can stop using it straight away if this is the case.
• Some women don’t like the sensation of feeling ‘high’ or the tingly sensation it can give.
Opiates, e.g. pethidine, morphine, diamorphine, meptid
An opiate drug is usually given via an injection in the top of the thigh or in the bottom and takes about 20 minutes to fully take effect. As it has to be prescribed by a doctor, it’s not always available in every hospital, so it’s worth checking with your midwife beforehand. As it can make you feel nauseous, your midwife may recommend having an anti-sickness drug at the same time.
Advantages:
• If you’ve had a very long latent phase of labour (the early stage) and have not slept it can be used to help you relax and sleep – some labours are stalled due to tiredness, which means the cervix doesn’t dilate effectively.
• You can still have an active birth and don’t have to be continuously monitored.
Disadvantages:
• It can make you feel woozy, sick and sometimes forgetful and confused.
• It crosses the placenta, so if given too close to delivery it can cause breathing problems for the baby (your midwife might recommend that a neonatal doctor is present for delivery in case of this).
• It can interfere with the baby’s first feed due to making the baby sleepy and therefore difficult to feed.
Epidurals
Epidurals get a lot of negative press so it’s only fair to be honest about them and give a balanced view. Although I’ve never personally had one, I’ve looked after hundreds of women who have had one, and who have had a positive birth experience.
An epidural is the only form of pain relief available in labour that will give you full relief from the contractions. It’s administered by an anaesthetist by passing a thin tube (via a needle) into a space in your back. The needle is then taken away and the tube is held in place with lots of sticky tape so it won’t come out. It works by numbing the nerves that carry pain signals from the brain to your uterus so you can still move your legs, although they may feel heavy and numb.
As you are less likely to feel the sensation to go for a wee (emptying the bladder is really important during labour) it is recommended that you have a catheter inserted into your urethra via a small tube. This may feel a bit uncomfortable so your midwife won’t put it in until your epidural is working effectively. This then stays in for at least 12 hours after your baby has been born. As epidurals can sometimes make your blood pressure drop, it’s also recommended you have some fluids via an IV (intravenous) drip. This is usually a saline drip but you can still drink fluids as well. (Nothing too heavy, though – water, coconut water and energy drinks are good options). You will need to be continuously monitored on a CTG machine throughout labour.
I got the chance to actually get a breather after hours of back-to-back contractions. If like me you’re having a long labour, an epidural provides a lot of people with much-needed respite after no sleep. Timed right, it gives you the break to recharge, and to push at the final leg.
Nada, mum of two
Advantages:
• It can give really good long-term pain relief for labour.
• Excellent if you’re exhausted and need a rest and some sleep.
• It can be brilliant if you’re experiencing all your labour in your back and nothing else has helped relieve this.
Disadvantages:
• Epidurals can slow down labour as you’re most likely to be in one or two positions on the bed; therefore you may need a hormone drip called Syntocinon to help give those contractions a boost.
• You’re more likely to need an assisted delivery (instrumental delivery), especially if this is your first baby, as it’s harder to push with an epidural on board. This will either be by a ventouse (a small cup placed on the baby’s head) or forceps. Both are carried out by an obstetric doctor.
• If you do have an instrumental delivery (depending on if you’ve had a baby vaginally before), you are more likely to need an episiotomy to make space for the baby’s head.
• About 1 in 100 women experience a postural puncture headache with an epidural and you may need to go to theatre for a blood patch.
• The medication used with an epidural can make your skin itchy – this can be relieved by medication given by your midwife.
• You may have a sore back for a few days after your baby is born – however this can also be associated with pregnancy and labour itself.
So there you have it; all you need to know about pain relief for labour/birth. Keep an open mind about what’s right for you. Labour can be unpredictable and there are no medals for who did it with or without drugs. It’s about having a positive birth, which might be with just a whiff of gas and air.
When we’re in strange places with people we don’t know our bodies trigger our fight-or-flight response. This stimulates the production of adrenalin and means our birthing muscles stop getting the blood and oxygen they need to work comfortably and efficiently. Creating an environment that feels more private and homely will help reassure you that you are safe and that no one is observing you (we’re very primal when it comes to birth).
A few little extras, whether you’re planning a birth at home or in hospital, can really help you relax. Remember you need all the oxytocin you can get during labour. Oxytocin is the ‘love’ hormone and is needed to initiate and maintain labour. It requires a dark, quiet, familiar, non-threatening environment in order to flow. If you’re having your baby in hospital, it’s likely you’re going to encounter the smell of bleach or hand-gel, so it’s a good idea to override that with your own comforting scents. I’m a big fan of essential oils – they are easy to use and incredibly effective during pregnancy and birth, when your sense of smell is heightened. My favourites include:
• Lavender: Well known to aid relaxation and promote calm. Also a painkiller that stimulates circulation and healing and may strengthen contractions.
• Clary sage: One of the oils that you should avoid during pregnancy until 37 weeks, but fine once you’re in labour, clary sage can strengthen contractions. It’s also a great oil for lifting your spirits and reducing anxiety.
• Peppermint: A generally uplifting and refreshing oil.
• Chamomile: Soothes, calms and helps to reduce tensions and anxiety.
• Jasmine: Acts as a uterine tonic, painkiller and anti-spasmodic. Also known to strengthen contractions and can be used to aid delivery of the placenta.
During my third labour I inhaled clary sage and lavender on a cold wet flannel every time I got a contraction. It was seriously powerful and got me through the toughest parts, as lavender is a muscle relaxant and sedative and clary sage boosts contractions. Winning combo!
Creating a playlist of songs that make you feel happy and safe is a really lovely way as a couple to think about your birth (and a fun way to have a giggle at some of your old CDs collecting dust).
Music has the power to make you feel all sorts of emotions, and you certainly will go through many in labour! It doesn’t need to be whale music and pan pipes – any music you had at your wedding or remember from childhood, for instance, is likely to bring up those nostalgic, emotive memories and associations of feeling loved and at ease. Mix it up: maybe have some instrumental pieces when you want to feel focused and in your zone, and then some up-tempo stuff for moments when you want to feel more energised and alive. Basically, the more you can appeal to all of your senses with positive triggers, the better! You may want to pack some small portable speakers in your hospital bag as not every hospital/birth centre will have access to a music player.
Latent phase/first stage: The time when you’ll be mostly at home relaxing. So think chill-out tunes. You may want to consider listening to these via some headphones in the bath, snoozing in between the milder contractions. Remember, you don’t want to be using up all your energy at this stage, so get in the zone and try to stay relaxed.
Active phase: Something a little more upbeat could be really great here. I have seen (and have done it myself) women dancing to the beat of music during this stage of labour. Imagine sitting on the birthing ball, rocking your hips from side to side to a great tune with a great bass. Your partner might get involved too, and even your midwife!
I often hear women telling me their birth stories, and a common theme comes through: ‘I had to get on the bed to have monitoring’ or ‘the midwife/doctor needed to listen to the baby’s heartbeat so I got on the bed.’
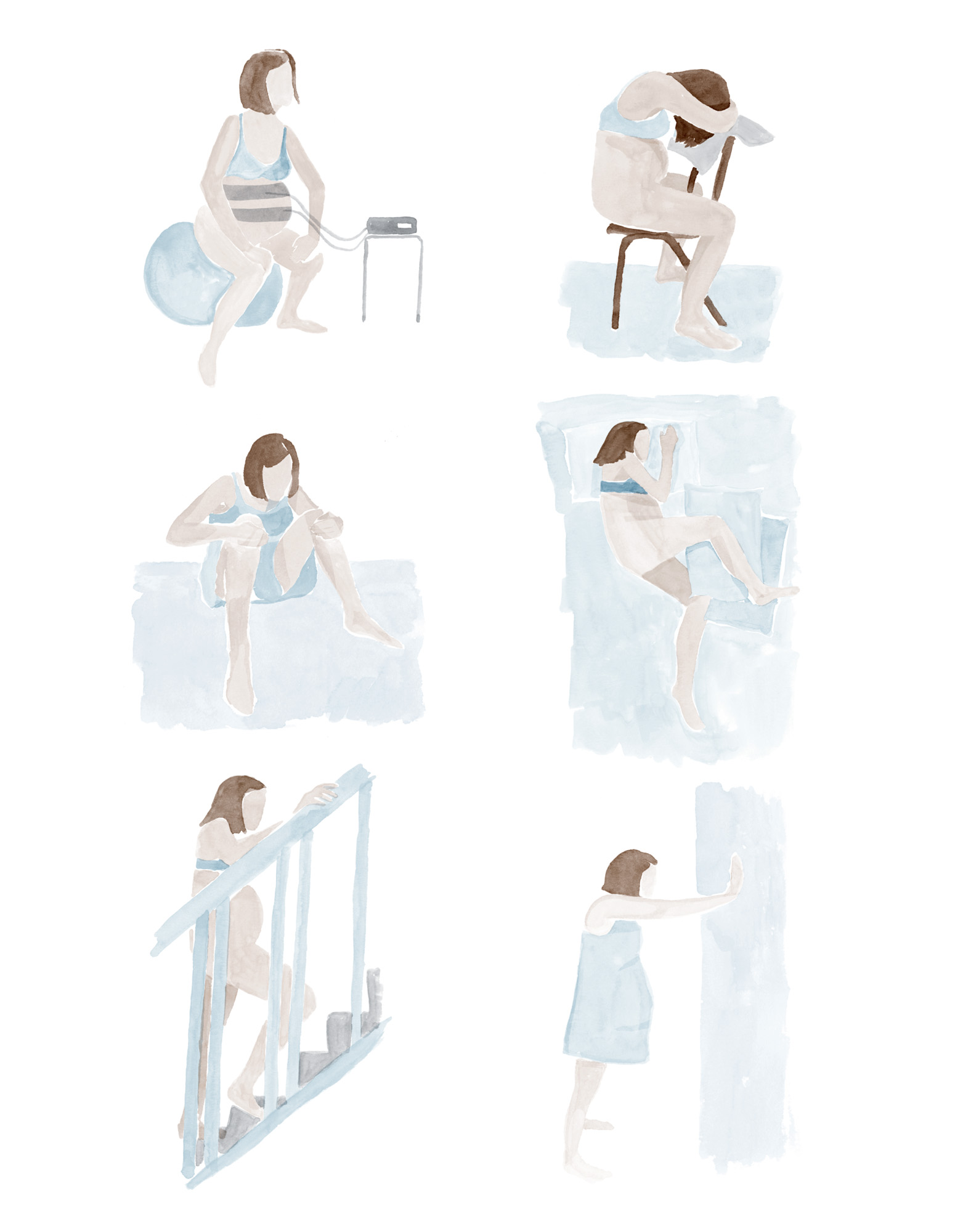
There is no rule written in any guideline/hospital policy that says a woman has to be on the bed for monitoring. If it is advised that it is safer to monitor your baby’s heartbeat during labour with a CTG machine then ask to stand, lean over the bed or sit on a ball, because this is your labour and you know the benefits of staying upright. Remember UFO! (See here). Get your birth partner to ask for the bed to be moved, for a birthing ball (or take your own in) or for birthing mats to be put down on the floor. Any unnecessary equipment can be moved out of the way to make space for you to be active.
Active birth was first introduced to me as a first-year student midwife 10 years ago. It became something I was so passionate about I even wrote my final-year dissertation on the subject: ‘Alternative Positions of the Mother in the Second Stage of Labour’. There have been hundreds of studies written about why staying upright and moving around in labour is more beneficial for the woman. So just to clarify some of the benefits:
Benefits of active birth:
• Shorter, more efficient, labour.
• Help the labouring mum to cope with the intensity of contractions.
• Less risk of fetal distress as there is better blood flow to the placenta.
• Working with gravity rather than against it.
• Partners can give physical support, helping them to get involved.
• Minimal trauma for mum and baby.
Opposite are a few great ideas for keeping active in labour.
I think it’s one of the most commonly asked questions us midwives hear: ‘Will I poo when I’m giving birth?’ In fact, 80–90 per cent of women do a poo at some point during labour. And do you know what? Us midwives get a little excited when we see a poo. Seriously, we do, because it often means the baby is getting closer to being born and that is really exciting! But we don’t scream and shout ‘Look she’s done a poo, look everyone!’ We quietly and subtly clear it away without anyone (partners included) noticing.
I have constructed a list, to dispel all myths about all things poo-related.
• Midwives don’t really mind poo. It often means the baby coming, so we get super-excited and slowly start to put our gloves on.
• Life goes on after pooing in front of your partner. You’ve already been naked, had sex, probably vomited, passed wind etc. in front of them, so a poo is really no biggie.
• As the baby pushes down in your pelvis, it pushes on all the nerves and muscles in your bottom. So if there’s some poo in there, then of course it’s going to come out. Giving birth really does feel like going for the biggest poo of your life.
• If you can, go for a poo in early labour. Women often have diarrhoea at the onset of labour, which is the body’s way of having a clear-out.
• Don’t worry about what you have eaten. Depriving yourself of food during early labour because you’re worried about pooing is a bad idea. A runner does not prepare for a marathon by starving herself and you shouldn’t either. You and your baby need energy to have the endurance for birth.
• ‘Bear down’ and ‘push like you need a poo’ are some phrases you may hear us midwives say during birth. Focus on this: get into a position as if you are going to open your bowels, such as a deep squat, all fours or on a birthing stool. No one poos lying down or with their legs in stirrups – so think about this if you’re asked to get on the bed to deliver the baby.
As we arrived at the hospital I was taken in to the assessment room. I could hear nervous whispered conversations from couples sitting quietly behind curtains waiting to see a midwife, all likely to be sent home again because they’d come in too early. I, on the other hand, was pretty far along and was wailing and MOOING like a cow. It’s happened in both my labours and it’s not even a noise I can do on demand, but it really is the exact sound of a loud and distressed cow.
The midwife was asking me to get up on the bed so she could check how dilated I was, but the contractions were getting closer and closer and I needed to be standing up. On my mum’s advice – she was a midwife – I’d hung on at home for as long as possible, which meant I was pretty much good to go on arrival at the hospital. So I kept trying to get up, and then mooing a bit, and getting back off the bed. I was making quite a scene behind my little curtained-off area.
And then it happened: the pressure all got too much and I ripped down my knickers and shat. As I was standing it was from quite a height so – much like a cow-pat, to continue the theme – it splatted all over the floor. Rather than quietly hope no one had heard, I accompanied it with yells of ‘I’m shitting, I’m shittiiiing’ while my husband patted my back and said ‘We know, darling’, then I apologised repeatedly to the wall of curtains that must have been hiding horrified couples.
But you know what? I didn’t care. I was in labour and I knew that my body was doing what it was supposed to do.
So, is birth beautiful? It is definitely incredible and mind-blowing as well as messy. An actual human being comes out of your body. It still freaks me out a little. And despite what he saw, my husband also remembers it as an awesome thing, watching me do something so incredible and with such determination. So, despite all the crapping and mooing, I suppose it was pretty beautiful.