CHAPTER 11
FATIGUE AND WEAKNESS IN PATIENTS WITH INFLAMMATORY MYOPATHIES: DERMATOMYOSITIS, POLYMYOSITIS AND INCLUSION BODY MYOSITIS
Jane H.Park, Brittany C.Lee and Nancy J.Olsen
OBJECTIVES
The objectives of this chapter are to:
• characterise fatigue and weakness in myositis patients with dermatomyositis, polymyositis or inclusion body myositis;
• consider the aetiology of muscle dysfunction and abnormalities in patients with myositis;
• suggest methods for alleviation of fatigue and weakness in order to improve muscle strength, endurance and overall quality of life.
INTRODUCTION
Idiopathic inflammatory myopathies, including dermatomyositis (DM), polymyositis (PM) and inclusion body myositis (IBM), are chronic, debilitating diseases which are primarily characterised by weakness, fatigue and myalgia (Dalakas, 1991). The underlying reasons for these disabilities are not clearly understood. Symptoms can be partially alleviated by treatment with prednisone and immunosuppressive medications like methotrexate and/or azathioprine. However, most adult patients retain some disability and do not return to their original state of strength and endurance (Harris-Love, 2003). Thus, inflammatory myopathies have long-term effects on patients’ lifestyles and employment possibilities. Since muscle strength and fatigue are the clinical features most readily followed during treatment, extensive investigations have provided applicable clinical tests and basic physiological insights into these aspects of inflammatory myopathies. Weakness or strength is evaluated with the ability to lift weights, and fatigue or endurance is measured by patient self-assessments such as the health assessment questionnaire (HAQ), or by testing the effects of prolonged exercise (Dastmalchi et al., 2007).
CLINICAL EVALUATION
Dermatomyositis and polymyositis show symmetrical proximal muscle weakness in the thighs, shoulders and neck, whereas inclusion body myositis demonstrates weakness and atrophy in both proximal and distal muscles. These three diseases are diagnosed by clinical examination and laboratory tests. Elevated levels of serum enzymes, namely creatine phosphokinase (CK), aldolase, lactic dehydrogenase (LDH) and aspartate and alanine aminotransferases (AST and ALT), suggest muscle degeneration and fragmentation. However, serum enzyme levels, particularly CK, can be normal or elevated by non-myopathic factors such as CK inhibitors in the serum, intense exercise, gender and race. In addition, muscle enzyme levels from biopsies have documented defects in respiratory chain enzyme activities and increased succinic dehydrogenase (Rifai et al., 1995; Chariot et al., 1996). Muscle damage is further verified by abnormal EMG and biopsy. Distinguishing histological features of the diseases as demonstrated by biopsy are well-recognised. DM shows immune processes of perivascular distributions of inflammatory cells, primarily B-lymphocytes and T4+ cells, against capillaries and secondarily against muscle necrosis. PM involves a cell-mediated cytotoxicity by T-lymphocytes, especially T8+ cytotoxic cells and macrophages. IBM myotoxicity is mediated by T-cells producing intranuclear tubular inclusions (Wortmann, 2005). Biopsy has an advantage over magnetic resonance imaging (MRI) in that it can distinguish the type of inflammatory infiltration and the features of the vascular system.
MAGNETIC RESONANCE IMAGING OF MUSCLE MORPHOLOGY
Since biopsy and EMG are painful and not suitable for long-term evaluation of chronic muscle diseases, MRI is now used to evaluate muscle morphology as related to weakness and fatigue (Park et al., 1990; Dalakas, 1991). MRI provides an image of the entire thigh or shoulder, and thereby avoids the error of a negative biopsy within a small, restricted area. As a non-invasive technique, longitudinal MRI examinations are utilised for therapeutic evaluations of individual thigh muscles (Park et al., 1994). Examples of T1- and T2-weighted images are shown in Figure 11.1 to illustrate inflammation and progressing stages of fat infiltration in affected patients.
T1-weighted images (left-hand column) are rapidly acquired images and do not show inflammation. This can be seen in the similarity of the signal intensity in the thigh of a normal control (A) and a DM patient (C). By contrast, T2-weighted images (right-hand column) are acquired four times more slowly and demonstrate high signal intensity (brightness) in the DM vastus muscles (D), presumably the mobile water of inflammation. For the PM patient (E), T1-weighted images show infiltrated fat with rapidly rotating methyl protons, as illustrated in the vastus muscles of quadriceps and also in the superficial fat of all subjects. T2-weighted images (F) show fat as somewhat darkened, but the vastus muscle itself is lightened by overlying inflammation. This can be definitively observed in the STIR images (Figure 11.2), which were acquired with a sequence that suppresses (blackens) the fat signal and thereby enhances the bright signal of the inflammation (Dalakas, 1991). The chronic PM patient (G) shows total fat replacement in the quadriceps, but preservation of the rectus femoris, biceps femoris, semimembranosus, gracillus and sartorius. This 70-year-old patient went to the gym five times per week and was able to walk and exercise with his preserved muscles at an unexpectedly high level of function. IBM patients were not included in our discussion as they represent only 15% of this myositis group and are a different clinical phenotype (Alexanderson et al., 2007).
MRI quantification with T1 and T2 relaxation times
Signal intensity differences between the patients can be quantitatively evaluated by calculation of T1 and T2 relaxation times within a defined region of a given muscle. Inflammation within a muscle produces high T1 and T2 values (Table 11.1) (Park et al., 1990, 1994). By contrast, fat infiltration shows a substantially lower T1 value and a high T2 value. These calculations are not only useful for characterising the severity and extent of inflammation or fat infiltration, but also for evaluating responses to
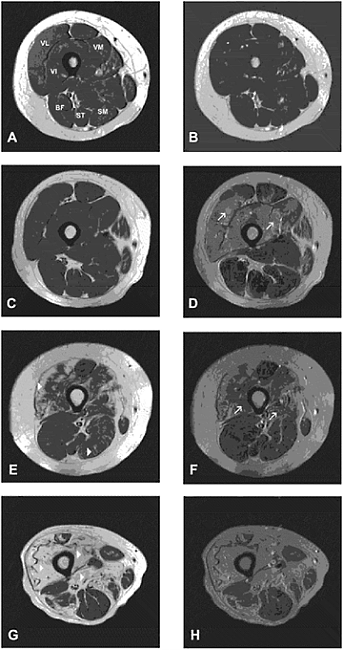
Figure 11.1 T1- and T2-weighted images of the thigh of control, DM and PM patients. T1-and T2-weighted images of a control subject (A, B) and DM (C, D), and PM (E, F) and chronic PM patients (G, H). The left column illustrates T1-weighted images (A, C, E,G), and the right column shows corresponding T2-weighted images (B, D, F, H). Arrowheads on T1-weighted images indicate fat, and arrows on T2-weighted images indicate inflammation. VL: vastus lateralis; VI: vastus intermedius; VM: vastus medialis; BF: biceps femoris; ST: semitendinosus; SM: semimembranosus; MRI: T1-weighted images; TR/TE=500/20, 80; T2-weighted images, TR/TE=2000/20, 80

Figure 11.2 STIR images of DM and PM thighs. The STIR image of DM patient (A) shows inflammation in the quadriceps muscles. For the PM patient (B), both suppression of the fat signal and the enhancement of the inflammation in the vastus lateralis and adductor magnus
ongoing therapies. When T1 and T2 calculations are confounded with infiltrated fat in the presence of inflammation, a STIR image can be quantitatively measured by increased signal intensity to show selected areas of inflammation (Figure 11.2) (Dalakas, 1991). Self-assessment measurements of fatigue and weakness on a 10cm visual analogue scale (VAS) indicate severe problems with functional activities (Table 11.1). Although the perception of fatigue and weakness varies among patients, longitudinal evaluation by an individual patient may be particularly revealing.
The focal characteristics of inflammation and/or fat infiltration are strikingly demonstrated in MRI images (Figure 11.1). In general, the anterior quadriceps muscles are more affected than the posterior hamstring muscles, which may have normal relaxation values (Figure 11.1: D, F). This accounts for the proximal weakness observed in rising from a chair or getting out of a car. Although the pattern seems well-defined in the muscles of these three patients, selection of different muscles and distribution of inflammation has been noted. DM cases have been described in which
inflammation has been suppressed by immune therapy, but the patient still reported weakness and fatigue (Newman and Kurland, 1992; Park et al., 1994). These findings demonstrate that functional ability does not always correspond with image abnormalities; therefore, investigations with magnetic resonance spectroscopy (31P MRS) have been conducted to evaluate metabolic abnormalities.
METABOLIC ABNORMALITIES RELATED TO WEAKNESS AND FATIGUE
Non-invasive 31P MRS is useful for characterisation of metabolic abnormalities in the muscles of patients with inflammatory myopathies. 31P MRS monitors metabolic status by determining levels of the high-energy phosphate compounds, ATP and phosphocreatine (PCr), which are required for muscle contraction (Park et al., 1990, 1994; Lodi et al., 1998; Cea et al., 2002; Pfleiderer et al., 2004). Figure 11.3 shows 31P spectra from a myositis patient and control subject at rest. Patients have lower Pi, PCr and ATP peaks compared to control subjects. The concentration of substrates is calculated from the determination of the area under the curve and the application of appropriate correction constants (Park et al., 1990, 1994).
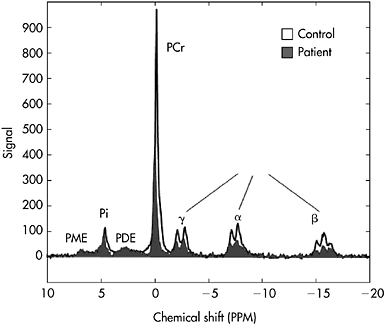
Figure 11.3 Comparison of 31P MRS spectra of the quadriceps muscles of a normal control and an inflammatory myopathy patient at rest. The positions of the Pi and PCr peaks, along with the α-, β- and γ-phosphate peaks of ATP, PDE and PME are shown. The muscles of the patient had lower peaks for PCr and ATP than did those of the control subject
Studies have shown that at rest, PCr and ATP are approximately 38% lower in both DM (Park et al., 1995, 2008) and PM (Park et al., 2008) patients compared to controls.
During the course of exercise, PCr levels in patients decrease in order to maintain constant ATP levels (Figure 11.4). During exercise at 25% MVC, Pi/PCr ratios are 56% greater in DM patients compared to controls, and 52% greater at 50% MVC. Elevated Pi/PCr ratios indicate a deficiency in DM muscles for generation and maintenance of ATP. PM patients and controls have similar ratios at 25% MVC exercise, and at 50% MVC, PM patients’ ratios are 20% less than controls. The similar ratios between controls and PM patients do not mean that the two groups are equally efficient. The fact that PM patients lifted less than half the weight by controls (8lbs versus 21.5lbs) means that diseased muscles required less PCr for contraction. The calculations of ratios may be misleading unless the quantitative values for the metabolites are determined. The work/energy cost ratios (weight lifted/[Pi/PCr]) of DM and PM patients are lower than those of normal controls, but ratios between patient groups are not different. Though DM patients have higher Pi/PCr ratios, they lifted more weight than PM patients (15lbs versus 8lbs), thus making the work/energy cost ratios approximately the same. These MRS findings suggest that, with regard to muscle function, DM patients are more metabolically active than PM patients.
31P MRS can also determine magnesium (Mg2+) levels in muscle. Mg2+ is important because it is a required cofactor for all enzymatic reactions involving ATP, and for mitochondrial membrane stability. Also, Mg deficiency can lead to muscle weakness (Cronin and Knochel, 1983). 31P MRS measurements of Mg levels in muscles are determined by the chemical shift of the β-phosphate peak of ATP when it binds to free Mg2+ and forms the enzymatically active MgATP complex (Figure 11.5). Free Mg2+ levels represent the biologically active form of Mg in vivo.
In previous studies, MgATP levels in DM and PM patients were found to be approximately 40% below control values at rest (Figure 11.6) (Niermann et al., 2002; Qi et al., 2007, 2008a). During exercise, DM patients lose about 15% of their MgATP, while PM patients with a very low workload were able to maintain their levels throughout the exercise protocol. Loss of MgATP during exercise represents a serious defect in metabolism. ATP is degraded to ADP and then to AMP, which can leave the muscle cell as adenosine. To subsequently rebuild ATP without the adenine starting blocks can require 2–3 hours, resulting in a prolonged period of significant fatigue. Juvenile DM (JDM) patients have MgATP levels that are 32% below juvenile controls at rest, but, unlike the adult DM patients, exercise does not decrease levels of this compound in children (Niermann et al., 2002).
Levels of free Mg2+ in resting DM or PM muscles were not significantly different from control muscles. During exercise, free Mg2+ in the muscles
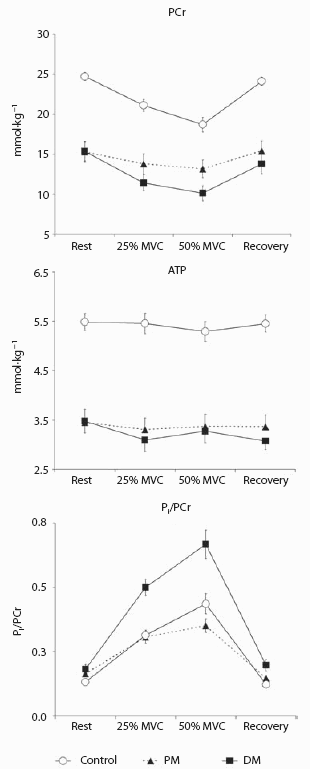
Figure 11.4 PCr and ATP concentrations and Pi/PCr ratios in control subjects and DM and PM patients during rest, exercise and recovery. Values are mean ± SEM mmol·kg−1 wet weight muscle. DM and PM patients had less PCr and ATP compared to control subjects throughout the exercise protocol. DM patients had higher Pi/PCr ratios compared to controls, indicating problems with oxidative phosphorylation. PM patients had similar or lower Pi/PCr ratios compared to controls because they lifted substantially less weight and therefore had less PCr utilisation
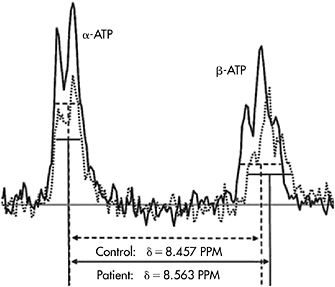
Figure 11.5 Chemical shift of the β-ATP peak in the spectrum of the quadriceps muscles of an inflammatory myopathy patient. The β-ATP peak in the spectrum for the control subject (solid line) exhibits a symmetrical triplicate shape, indicative of MgATP complex. In the patient’s spectrum (dotted line), the β-ATP peak is less symmetrical and shifted to the right, indicating decreased Mg binding. The distance (δ) from the half-height midpoint of the α-peak to the quarter-height midpoint of the β-peak was utilised for the calculations of Mg
of adult and juvenile controls rose by 17% or 30%, respectively. In contrast, free Mg2+ in DM and JDM patients decreased significantly to approximately 40% of their respective control values and remained low, even during recovery. These low levels of free Mg2+ may be related to weakness and fatigue since this cation is the biologically active magnesium in muscle (Welch and Ramadan, 1995). It is required for optimisation of enzyme reactions, maintenance of membrane integrity, stabilisation of mitochondria, regulation of ATP-dependent ion channels of K+, Na+, and Ca2+ transport (Welch and Ramadan, 1995; Irish et al., 1997; Blazev and Lamb, 1999). Low levels of Mg2+ may result in hypercontractility of smooth muscle and arteriolar vasoconstriction, which may produce hypoperfusion of oxygen and substrates (Blazev and Lamb, 1999). Thus, muscle dysfunction could be induced by magnesium deficiencies through multiple mechanisms.
Treatment of myositis patients with prednisone and immunosuppressive drugs results in increases in levels of MgATP and free Mg2+ in muscle tissue. Increases in magnesium are concordant with improved strength and endurance (Niermann et al., 2002). Therefore, MgATP and free Mg2+ may be significant factors in the pathophysiology of myositic diseases.
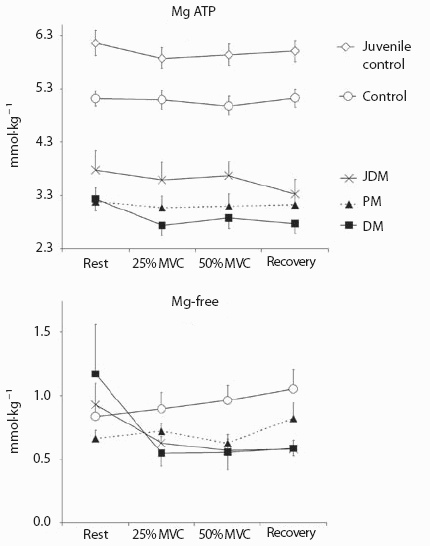
Figure 11.6 Differences in MgATP and free Mg2+ concentrations in control subjects and DM, JDM and PM patients during rest, exercise and recovery. Values are mean±SEM mmol·kg wet weight muscle. Control subjects have higher concentrations of MgATP than DM, JDM and PM patients throughout the exercise protocol. Juvenile controls also had greater concentrations of MgATP compared to their adult control counterparts. Free Mg2+ concentrations increased over the course of exercise in control subjects, but decreased in DM, JDM and PM patients
ADDITIONAL FACTORS RELATED TO FATIGUE AND WEAKNESS
Lung involvement
In dermatomyositis and polymyositis, extramuscular organ involvement is common, such as a typical erythematous skin rash in dermatomyositis, as well as involvement with the lungs, heart, and joints. Lung involvement has been found in two separate studies to affect approximately 75% DM/ PM population, primarily as interstitial lung disease (ILD) (Fathi et al., 2007, 2008). The high frequency of ILD in this population suggest that chest X-ray, high resolution computed tomography and lung function tests be performed in DM/PM patients. ILD responds to treatment with prednisone and adjunct immunosuppressive drugs such as methotrexate and azathioprine. The hypoventilation associated with ILD and weakness of respiratory muscles will clearly decrease oxidative phosphorylation in the mitochondria of muscles. In extreme cases, progressive lung disease may result in atrophy and fibrosis of diseased muscles. Lung disorders may lead to decreased patient activity which, in turn, may result in muscle dysfunction. However, cardiac involvement is rare in this group of patients, and its effects on exercise are therefore not discussed.
Relationships between carbohydrate and fat metabolism
Regulation of carbohydrate and fat utilisation in muscle was studied in 1963 by Randle et al., who introduced glucose-fatty acid cycle relationships in metabolism (Randle et al., 1963). They proposed that an increase in fatty acid would result in increased fat metabolism and inhibition of glucose utilisation. The detailed enzymatic pathways and relationships of these data to insulin sensitivity has resulted in extensive present day studies of the glucose-fatty acid cycle in type 2 diabetes, and also in muscle exercises at various intensities. With 31P MRS experiments, mitochondrial oxidative phosphorylation in the skeletal muscle of diabetic patients was shown to be substantially decreased (Phielix and Mensink, 2008). Although it was difficult to determine whether mitochondria were impaired by insulin resistance or were a primary point of pathogenesis, the data suggest a starting point for myopathies with fat infiltration. Mitochondrial damage and fat infiltration in polymyositis patients have been observed, but the disease mechanisms were not determined (Schroder and Molnar, 1997). Damaged mitochondria may, in part, explain the more severe weakness and exercise abnormalities in polymyositis patients compared to dermatomyositis patients (Figures 11.4 and 11.5).
Hypoperfusion as a contributor to muscle deficiency
Numerous histological studies have documented abnormalities in the arteries and capillaries of DM/PM muscles (Emslie-Smith and Engel, 1990; Grundtman et al., 2008). The pathological findings include reduced capillary lumen, disrupted capillary membrane and reduced capillary density. These abnormalities may represent the known hypoperfusion in muscle, resulting in reduced substrate concentration and oxygen metabolism. The elegant 31P MRS kinetic studies with DM and PM patients placed hypoperfusion as the primary factor in defective oxidative phosphorylation in mitochondria (Cea et al., 2002). Abnormalities in perfusion and diffusion in DM/PM patients were demonstrated with MRI methods of diffusion-weighted imaging (DWI), and diffusion tensor imaging (DTI) which provide a microscopic picture of water movement required for delivery of substrates and oxygenation (Qi et al., 2008b; Park et al., 2009). DTI fibre tracking shows fibre fragmentation and spatial displacement that affect diffusion. Clearly, many factors could contribute to the reduced metabolism which produces fatigue and weakness. There are real difficulties in prioritising these factors as the interplay between parameters is substantial.
TREATMENTS FOR ALLEVIATION OF WEAKNESS AND FATIGUE
Exercise therapy to improve strength and fatigue
Patients with inflammatory myositis show improvement in muscle function with prednisone treatment and adjunct immunosuppressive agents, such as methotrexate and azathioprine. However, most adult patients are left with residual weakness and fatigue, which requires continued medication (Harris-Love, 2003). Despite the early objections to exercise for dermatomyositis and polymyositis patients, it has now been shown that moderate exercise programmes improve both muscle strength and endurance (Hicks et al., 1993; Wiesinger et al., 1998; Alexanderson et al., 2007; Dastmalchi et al., 2007). The reasons for improvements are revealed in the well-documented study of biopsy data which show that fibre type is altered (Dastmalchi et al., 2007). After 12 weeks of exercise, nine patients (four DM and five PM) showed fibre type changes. Type I fibres, which contain mitochondria for oxidative phosphorylation and slow myosin heavy chains, increased from 32% to 42% of the total fibre count. This increase was due to a change in type IIC fibres to type I fibres. The relative proportion of fast fibres, type IIA and IIB, was unchanged after training. Moreover, the mean cross-sectional area of type II fibres increased by 25%, whereas type I fibre cross-sectional area did not change. In addition to increased strength and decreased fatigue, the health assessment scores for lifestyle characteristics (SF-36) indicate substantial improvements which correlate with fibre type change and increased muscle fibre area. This is the first study to show changes in fibre types in inflammatory muscle diseases.
Creatine supplementation for improved energy metabolism
Creatine supplements are known to have modest effects on highly trained athletes during periods of training (Kreider, 2003). Muscular dystrophies are also improved with creatine supplementation (Tarnopolsky et al., 2004). However, creatine did not improve all exercise tasks equally. Benefits of creatine are thought to be due to changes in the muscle bioenergetics through increased PCr levels.
For inflammatory diseases, an excellent double-blind, randomised, placebo-controlled trial was conducted for dermatomyositis and polymyositis patients (Chung et al., 2007). The purpose of this creatine trial was to determine whether improvements with regular exercise could be further promoted by creatine supplementation over a period of six months. In this investigation, 37 DM or PM patients were assigned to an exercise programme. Of these, 19 patients received creatine and 18 received a placebo. Statistical analyses showed, as stated in the previous paragraph, that both groups demonstrated increased muscle endurance. Creatine-treated patients demonstrated further improvement in endurance and the ability to undertake high-intensity exercise. 31P MRS studies showed that the additional exercise improvements in the creatine group correlated with increased PCr/β-NTP ratios, as demonstrated in other studies of myositis patients (Rico-Sanz et al., 1999; Schunk et al., 1999; Park et al., 2000; Scott and Kingsley, 2004). Thus, the improvements are, in part, due to metabolic changes associated with increased PCr. There were no changes in measures such as serum CK levels and health status. The authors conclude that exercise provides a key to rehabilitation, and oral creatine supplements could enhance exercise benefits at a reasonable cost to patients. Creatine does not, however, substitute for the immunosuppressive drugs that treat the basic myositic diseases.
Creatine and magnesium supplementations
Since DM and PM patients have decreased levels of PCr, ATP and Mg2+, a preliminary study was proposed to determine whether creatine and Mg2+ would be tolerated and enhance muscle performance. Five patients (one DM and four PM) were enrolled in a six-month open-label trial. Creatine was given for 30 days, and, for the following five months, a daily dose of either 200 mg or 400 mg per day of Mg2+ as magnesium aspartate was added. All five patients adhered to the therapeutic regimes from their physicians and completed the trial. PCr, ATP and Mg2+ levels, strength and function improved significantly during the trial. Four out of five patients had decreased fatigue and pain, as measured on the VAS (P=NS) and by HAQs (P=0.04). Patients showed functional improvement by their physician’s global assessment. Due to technical difficulties, only three of the patients completed follow-up MRI exams. In these patients, T2 values decreased from 38.2 to 34.6ms (P=0.04), suggesting partial resolution of inflammation. Creatine and Mg2+ supplementation may be a safe and effective treatment for DM and PM patients. Therefore, a larger double-blind trial should be considered. The above results are consistent with the data from the larger creatine trial discussed above (Park et al., 2005; Qi et al., 2005; Chung et al., 2007).
CASE HISTORIES SHOWING CLINICAL ASPECTS
Case histories of 11 dermatomyositis patients were studied longitudinally at the request of the physicians (Park et al., 1994). The progression and/or regression of disease indicated a wide variety of clinical results. Therefore, two cases were selected to illustrate the excellent recovery of a juvenile dermatomyositis patient with all clinical factors improving, and an adult woman with a disease flare followed by clinical improvement.
Patient 1: A 14-year-old Caucasian boy had a sudden onset of weakness, pain and typical erythematous rash. He was examined with MRI and MRS prior to the initiation of prednisone treatment, three weeks after a dosage of 60mg·d−1 prednisone was started, and at five and seven months, when the dosage had been reduced to 35mg·d−1. During this course of treatment, he showed decreases in serum CK levels and increases in strength (MVC) (Table 11.2). Initial T2-weighted images showed abnormal regions of high signal intensity in the quadriceps muscles, indicative of inflammation, whereas the posterior hamstring muscles appeared normal with a dark homogeneous signal (Figure 11.7B). T2 images taken in the seventh month of treatment show the resolution of inflammation with both the quadriceps and hamstring muscles having dark homogeneous signal intensity. These results were verified by the calculation of elevated T1 values in the initial images of the quadriceps muscle (1,890ms) and a return to normal T1 levels in the seven-month evaluation period (1,265ms). Biochemical abnormalities in the initial 31P MRS were detected as an approximately 40% decrease in both ATP and PCr. The Pi/PCr ratio was initially elevated, indicating inefficient generation and/or utilisation of ATP and PCr. Over the 5–7-month period, the Pi/PCr ratio decreased. This metabolic improvement was consistent with the increase in MVC from 15lbs to 40lbs. During exercise at 25% MVC, normalisation of Pi/PCr ratios, despite the higher workload, demonstrated improvement in bioenergetic status (work/energy-cost ratios increased from 7.1 to 32.3).
These data corresponded with the physician’s global evaluation of improved status. However, mild residual fatigue persisted, as evaluated in the activity questionnaire, and a restriction on excessive exercise in physical education classes was suggested.
Patient 2: A 67-year-old woman presented with mild weakness and was examined with MRI and 31P MRS prior to receiving medication. She was treated with a low dose of prednisone and showed considerable improvement. Hence, medication was terminated. A flare in disease activity occurred at 15.5 months, and she was sent for re-evaluation with MRI/ MRS. Treatment was restarted with daily doses of 60 mg prednisone, and considerable improvement was noted. Initial PCr values of 20mmol·kg−1 muscle dropped to 11mmol·kg−1 at 15.5 months, but with the resumption of prednisone treatment, returned at 33 months to 18mmol·kg−1.
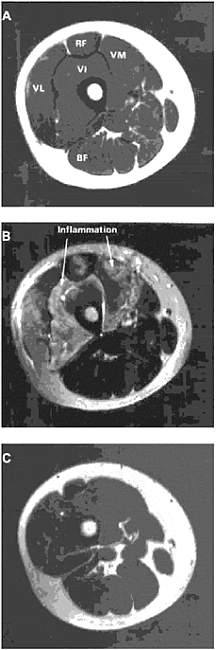
Figure 11.7 T1- and T2-weighted MRI images of the thigh of Patient 1. (A) Initial T1-weighted image, showing homogeneous signal intensity in major muscle groups. VL: vastus lateralis; VI: vastus intermedius; VM: vastus medialis; RF: rectus femoris; BF: biceps femoris. (B) Initial T2-weighted image, showing inflammation, as indicated by increased signal intensity (brightness), in RF, VL, VI, and VM muscles. (C) T2-weighted image after five months of prednisone treatment shows homogeneous signal intensity, indicating inflammation has resolved
When Pi/PCr ratios were considered, the initial ratio at rest was comparable to normal values at 0.15, but with exercise, increased to an abnormally high level of 0.6 (Figure 11.8). During the disease flare at 15.5 months, all ratios at rest, exercise and recovery were elevated, indicating a severe deterioration of the bioenergetic status in the muscles. When prednisone treatment was restarted, all metabolic parameters were improved. However, her T1 values did not return to normal levels. Her slightly elevated T1 values (1,439ms) were essentially unchanged over 33 months.
This patient’s history is interesting because the morphology of the MR images did not correlate with clinical tests, and in this case, the biochemical abnormalities of the MRS evaluations provided the most sensitive indicators of disease activity.
CONCLUSION
The major symptoms of inflammatory myositis, weakness and fatigue are closely intertwined. Pharmacological treatment depresses the immune
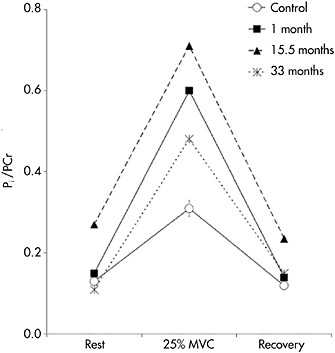
Figure 11.8 Pi/PCr ratios for Patient 2 during relapse and remission. Initially, patient ratios are similar to control values at rest and recovery and only elevated with exercise. During disease relapse at 15.5 months, ratios are elevated at all stages of the protocol. After treatment at 33 months, a trend toward normalization of Pi/PCr ratios is observed
responses and improves both strength and persistence during tasks. Over time and with exercise through physical therapy, greater muscle fibre size and increased numbers of type I oxidative fibres improve strength and, concordantly, endurance for selected exercise tasks. Creatine, or a combination of creatine and Mg supplements, demonstrate that biochemical intervention, which increases high energy compounds, PCr and ATP, and also Mg, will enhance strength, endurance and the lifestyles of patients with DM and PM. Substantial advances in clinical treatment and understanding of basic aetiology promise to evoke substantial opportunities for future investigations of idiopathic inflammatory myopathy (IIM).
FIVE KEY PAPERS THAT SHAPED THE TOPIC AREA
Study 1. Park, J.H., Vital, T.L., Ryder, N.M., Hernanz-Schulman, M., Partain, C.L., Price, R.R. and Olsen, N.J. (1994). Magnetic resonance imaging and 31P magnetic resonance spectroscopy provide unique quantitative data useful in the longitudinal management of patients with dermatomyositis. Arthritis and Rheumatism, 37, 736–746.
This paper explored the utility of using MRI and 31P MRS to evaluate disease progression/improvements in DM patients over an extended period of time. Monitoring of DM activity level is commonly performed with a strength evaluation or physical exam, and by measuring serum levels of muscle enzymes such as CPK. However, increased CPK is not directly indicative of disease status, as not all patients show an elevation in this enzyme. Invasive tests such as EMG and muscle biopsy are also not desirable for long-term monitoring. MRI and MRS are non-invasive and can be repeated multiple times. This paper presents long-term evaluations of 11 DM patients, both with and without useful laboratory findings. T1 and T2 relaxation times were calculated from MRI images, and concentrations of metabolites such as Pi, PCr and ATP were determined from resonance areas of the 31P MRS spectra. Of the 11 DM patients, seven had consistently normal CPK levels, nine showed statistical changes in T1 and T2 relaxation values following the clinical course of the disease, and nine exhibited changes in biochemical parameters that were also consistent with clinical evaluation. However, these MRI and MRS changes were not temporally concordant, indicating that inflammation and metabolic abnormalities are not necessarily resolved at the same rate. Overall, this study shows the absence or resolution of inflammation does not appear sufficient for some patients to return to normal metabolic status. Conversely, metabolic changes can also be an early indication of muscles abnormalities. MRI and MRS examinations proved very useful for initial diagnosis of the extent and severity of DM and subsequent evaluation of therapy.
Study 2. Harris-Love, M.O. (2003). Physical activity and disablement in the idiopathic inflammatory myopathies. Current Opinions of Rheumatology, 15, 679–690.
This review focuses on the enablement-disablement model of disability applied to idiopathic inflammatory myopathies and discusses the role of physical activity in the enablement process. First proposed in 1965, the model has been revised and expanded by the Institute of Medicine to better convey the multidirectional and dynamic relationship between the domains of disablement. Their Enabling-Disabling Process focuses on the role of the enabling process, separation of disability from the individual and emphasis on person-environment interaction. Pathological factors such as estimates of disease activity and damage may be used to guide exercise intervention and lend insight into the potential for muscle to exhibit adaptive response to strength training. Impairments of IIM are muscle weakness, excessive fatigue and diminished aerobic capacity that can be targeted by exercise therapy. Disability is the consequence of functional limitations in a social context and often measured by self-report. Cardiovascular fitness and muscle strength can be improved with various modes of physical activity and are a valuable adjunct therapy to pharmacological treatment in PM/DM patients. These aspects can decrease functional limitations and disability as part of the enablement process. Conversely, decreased physical activity as a result of IIM can cause a decline in health and independent functioning. Overall, the Enablement-Disablement model takes into account the continuum of health and functioning instead of exclusively focusing on disability, and provides a better conceptual framework to understand the effectiveness of exercise interventions in the treatment of IIM. A comprehensive description of clinical activities in future trials will help discern how much exercise helps with physiological adaptations, the appropriate timing and the type of exercise done to promote clinical guidelines.
Study 3. Dastmalchi, M., Alexanderson, H., Loell, I., Stahlberg, M., Borg, K., Lundberg, I.E. and Esbjornsson, M. (2007). Effect of physical training on the proportion of slow-twitch type I muscle fibres, a novel nonimmune-mediated mechanism for muscle impairment in polymyositis or dermatomyositis. Arthritis and Rheumatism, 57, 1303–1310.
This paper compared fibre type composition and fibre area in healthy controls and patients with chronic PM and DM and sought to determine if 12 weeks of physical training changes these muscle characteristics. The relative frequency of fast (type II) and slow (type I) twitch fibres in the muscle determines the muscle’s endurance capacity. Muscle fibre type, cross-sectional area and amount of regenerating fibres were determined from biopsies. The Functional Index (FI) in myositis was used to evaluate muscle strength and endurance. The Swedish version of the Medical Outcomes Study Short Form 36 (SF-36) was used to evaluate subject’s perceived health-related quality of life. Initially, patients had fewer type I fibres and more type IIB and IIC fibres compared to controls. After 12 weeks of physical training, the patients had increased type I fibres with training and increased type II muscle fibre cross-sectional area, thus making trained muscles more similar to those of controls. Muscle endurance and quality of life scores also increased after training. Positive correlations were found between the increase in type I fibres and physical function (subset of SF-36), as well as function and type II fibre cross-sectional area. The low percentage of oxygen-dependent type I fibres found in patients before the exercise programme was hypothesised to be due to adaptation to muscle tissue hypoxia. The exact mechanism(s) still needs to be determined, but the authors proposed it could be due to improved microcirculation, lowered total peripheral resistance, and reduced skeletal muscle ischemia. The increase in cross-sectional area of type II fibres was attributed to the type of weight training performed, which is known to increase muscle protein synthesis preferably in type II muscles fibres. The clinical relevance of the changes in fibre type composition and fibre area were supported by the improvement of physical capacity measured by both the FI test and the reported improvement of physical functioning in the SF-36 questionnaire.
Study 4. Chung, Y.L., Alexanderson, H., Pipitone, N., Morrison, C., Dastmalchi M., Stahl-Hallengren, C., Richards, S., Thomas, E.L., Hamilton, G., Bell, J.D., Lundberg, I.E. and Scott, D.L. (2007). Creatine supplements in patients with idiopathic inflammatory myopathies who are clinically weak after conventional pharmacologic treatment: six-month, double-blind, randomized, placebo-controlled trial. Arthritis and Rheumatism, 57, 694–702.
This paper presents one of the largest reported randomised, placebocontrolled trials in IIM. Oral creatine is generally considered to improve athletic and sporting performance. This study was designed to test the hypothesis that patients with established, treated IIM and persisting weakness would have additional benefits from exercise combined with oral creatine therapy. In a six-month, two-centre, double-blind, randomised, controlled trial, a total of 29 patients were randomised to receive oral creatine supplements (eight days, 20mg·d−1 then 3mg·d−1 patients followed a home exercise programme which consisted of resistive, range of motion and stretching exercises, as well as a 15min daily walk. The primary outcome measure was aggregate functional performance time (AFPT), which was a functional assessment measured in times to complete four simple tasks involving walking and stair climbing. 31PMR spectroscopy was used to evaluate muscle bioenergetics as determined by the PCr/ β-NTP ratio. Assessments were taken before and at the third and sixth months of the trial. AFPT showed a median decrease of 11.4% in the creatine group versus 3.7% decrease with placebo from initial performance. PCr/β-NTP ratios increased in the creatine group, but remained unchanged in the placebo group. Creatine increased the benefits of exercise on endurance and improved ability to undertake high-intensity exercise, an effect maintained over five months. Therefore, creatine could be a useful adjunct therapy to extend the benefits of exercise on muscle weakness and fatigue.
Study 5. Niermann, K.J., Olsen, N.J. and Park, J.H. (2002). Magnesium abnormalities of skeletal muscle in dermatomyositis and juvenile dermatomyositis. Arthritis and Rheumatism, 46, 475–488.
This study utilised 31P MRS to characterise muscle magnesium (Mg) levels in DM and JDM patients and to evaluate how effective immunosuppressive therapy was in increasing free and ATP-bound Mg (Mg2+ and MgATP). Spectra were obtained during rest, two graded levels of exercise and recovery. Levels of free ATP, biologically active free Mg2+ and enzymatically active MgATP were calculated from these spectra at each of the four stages of the exercise protocol. MgATP levels in DM and JDM myopathic muscles were at least 37% lower than those in normal muscles during rest, exercise and recovery (P<0.0005). Free Mg2+ levels were normal in DM and JDM myopathic muscles at rest, but were significantly lower than control values during exercise and recovery (P< 0.029 and P<0.005 for DM and JDM, respectively). Prednisone and immunosuppressive therapy partially reversed the magnesium abnormalities, as evidenced by elevation of the levels of MgATP and free Mg2+. Increased levels of MgATP and free Mg2+ were concordant with decreased weakness and fatigue.
GLOSSARY OF TERMS
31P MRS | phosphorus magnetic resonance spectroscopy |
ADP | adenosine diphosphate |
ALT | alanine aminotransferase |
AMP | adenosine monophosphate |
AST | aspartate aminotransferase |
ATP | adenosine triphosphate |
BF | biceps femoris |
CK | creatine phosphokinase |
CTL | adult control subject |
DM | dermatomyositis |
EMG | electromyography |
HAQ | health assessment questionnaire |
IBM | inclusion body myositis |
IIM | idiopathic inflammatory myopathy |
JCTL | juvenile control subject |
JDM | juvenile dermatomyositis |
LDH | lactate dehydrogenase |
Mg | magnesium |
MgATP | magnesium adenosine triphosphate |
MRI | magnetic resonance imaging |
MVC | maximum voluntary contraction |
PCr | phosphocreatine |
PDE | phosphodiester |
Pi | inorganic phosphate |
PM | polymyositis |
PME | phosphomonoester |
SM | semimembranosus |
ST | semitendinosus |
TE | echo time |
TR | repetition time |
VAS | visual analogue scale |
VI | vastus intermedius |
VL | vastus lateralis |
VM | vastus medialis |
REFERENCES
Alexanderson, H., Dastmalchi, M., Esbjornsson-Liljedahl, M., Opava, C.H. and Lundberg, I.E. (2007). Benefits of intensive resistance training in patients with chronic polymyositis or dermatomyositis. Arthritis and Rheumatism, 57, 768–777.
Blazev, R. and Lamb, G.D. (1999). Low [ATP] and elevated [Mg2+] reduce depolarized-induced Ca2+ release in rat skinned skeletal muscle fibres. Journal of Physiology (London), 520, 203–215.
Cea, G., Bendahan, D., Manners, D., Hilton-Jones, D., Lodi, R., Styles, P. and Taylor, D.J. (2002). Reduced oxidative phosphorylation and proton efflux suggest reduced capillary blood supply in skeletal muscle of patients with dermatomyositis and polymyositis: a quantitative 31P-magnetic resonance spectroscopy and MRI study. Brain, 125, 1635–1645.
Chariot, P., Ruet, E., Authier, F.J., Labes, D., Poron, F. and Gherardi, R. (1996). Cytochrome c oxidase deficiencies in the muscle of patients with inflammatory myopathies. Acta Neuropathology, 91, 530–536.
Chung Y.L., Alexanderson, H., Pipitone, N., Morrison, C., Dastmalchi, M., StahlHallengren, C., Richards, S., Thomas, E.L., Hamilton, G., Bell, J.D., Lundberg, I.E. and Scott, D.L. (2007). Creatine supplements in patients with idiopathic inflammatory myopathies who are clinically weak after conventional pharmacologic treatment: six-month, double-blind, randomized, placebo-controlled trial. Arthritis and Rheumatism, 57, 694–702.
Cronin, R.E. and Knochel, J.P. (1983). Magnesium deficiency. Advances in Internal Medicine, 28, 509–533.
Dalakas, M.C. (1991). Polymyositis, dermatomyositis and inclusion-body myositis. The New England Journal of Medicine, 325, 1487–1498.
Dastmalchi, M., Alexanderson, H., Loell, I., Stahlberg, M., Borg, K., Lundberg, I.E. and Esbjornsson, M. (2007). Effect of physical training on the proportion of slow-twitch type I muscle fibres, a novel nonimmune-mediated mechanism for muscle impairment in polymyositis or dermatomyositis. Arthritis and Rheumatism, 57, 1303–1310.
Emslie-Smith, A.M. and Engel, A.G. (1990). Microvascular changes in early and advanced dermatomyositis: a quantitative study. Annals of Neurology, 27, 343–356.
Fathi, M., Lundberg, I.E. and Tornling, G. (2007). Pulmonary complications of polymyositis and dermatomyositis. Seminars in Respiratory and Critical Care in Medicine, 28, 451–458.
Fathi, M., Vikgren, J., Boijsen, M., Tylen, U., Jorfeldt, L., Tornling, G. and Lundberg, I.E. (2008). Interstitial lung disease in polymyositis and dermatomyositis: longitudinal evaluation by pulmonary function and radiology. Arthritis and Rheumatism, 59, 677–685.
Grundtman, C., Tham, E., Ulfgren, A. and Lundberg, I.E. (2008). Vascular endothelial growth factor is highly expressed in muscle tissue of patients with polymyositis and patients with dermatomyositis. Arthritis and Rheumatism, 58, 3224–3238.
Harris-Love, M.O. (2003). Physical activity and disablement in the idiopathic inflammatory myopathies. Current Opinions of Rheumatology, 15, 679–690.
Hicks, J.E., Miller, F., Plotz, P., Chen, T.H. and Gerber, L. (1993). Isometric exercise increases strength and does not produce sustained creatine phosphokinase increases in a patient with polymyositis. Journal of Rheumatology, 20, 1399–1401.
Irish, A.B., Thompson, C.H., Kemp, G.J, Taylor, D.J. and Radda, G.K. (1997). Intracellular free magnesium concentrations in skeletal muscle in chronic uraemia. Nephron, 76, 20–25.
Kreider, R.B. (2003). Effects of creatine supplementation on performance and training adaptations. Molecular and Cellular Biochemistry, 244, 89–94.
Lodi, R., Taylor, D.J., Tabrizi, S.J., Hilton-Jones, D., Squier, M.V., Seller, A., Styles, P. and Schapira, A.H. (1998). Normal in vivo skeletal muscle oxidative metabolism in sporadic inclusion body myositis assessed by 31P-magnetic resonance spectroscopy. Brain, 121 (11), 2119–2126.
Newman, E.D. and Kurland, R.J. (1992). P-31 magnetic resonance spectroscopy in polymyositis and dermatomyositis: altered energy utilization during exercise. Arthritis and Rheumatism, 35, 199–203.
Niermann, K.J., Olsen, N.J. and Park, J.H. (2002). Magnesium abnormalities of skeletal muscle in dermatomyositis and juvenile dermatomyositis. Arthritis and Rheumatism, 46, 475–488.
Park, J.H., Lee, B.C. and Qi, J. (2009). Magnetic resonance imaging (DTI) of abnormalities in the thigh muscles of polymyositis patients. Proceedings of the International Society of Magnetic Resonance in Medicine, 17, 1903.
Park, J.H., Niermann, K.J., Ryder, N.M., Nelson, A.E., Das, A., Lawton, A.R., Hernanz-Schulman, M. and Olsen, N.J. (2000). Muscle abnormalities in juvenile dermatomyositis patients: P-31 magnetic resonance spectroscopy studies. Arthritis and Rheumatism, 43, 2359–2367.
Park, J.H., Olsen, N.J., King Jr, L., Vital, T., Buse, R., Kari, S., Hernanz-Schulman, M. and Price, R.R. (1995). Use of magnetic resonance imaging and P-31 magnetic resonance spectroscopy to detect and quantify muscle dysfunction in the amyopathic and myopathic variants of dermatomyositis. Arthritis and Rheumatism, 38, 68–77.
Park, J.H., Qi, J., Kroop, S.F. and Olsen, N.J. (2005). Preliminary trial of creatine and magnesium supplementation in myositis patients. Arthritis and Rheumatism, 52, S316.
Park, J.H., Qi, J., Lee, B.C. and Olsen, N.J. (2008). Comparisons of metabolic defects in exercising muscles of patients with polymyositis and dermatomyositis. Arthritis and Rheumatism, 58, S230.
Park, J.H., Vansant, J.P., Kumar, N.G., Gibbs, S.J., Curvin, M.S., Price, R.R., Partain, C.L. and James Jr, A.E. (1990). Dermatomyositis: correlative MR imaging and P-31 MR spectroscopy for quantitative characterization of inflammatory disease. Radiology, 177, 473–479.
Park, J.H., Vital, T.L., Ryder, N.M., Hernanz-Schulman, M., Partain, C.L., Price, R.R. and Olsen, N.J. (1994). Magnetic resonance imaging and P-31 magnetic resonance spectroscopy provide unique quantitative data useful in the longitudinal management of patients with dermatomyositis. Arthritis and Rheumatism, 37, 736–746.
Pfleiderer, B., Lange, J., Loske, K.D. and Sunderkotter, C. (2004). Metabolic disturbances during short exercises in dermatomyositis revealed by real-time functional 31P magnetic resonance spectroscopy. Rheumatology, 43, 696–703.
Phielix, E. and Mensink, M. (2008). Type 2 diabetes mellitus and skeletal muscle metabolic function. Physiology and Behaviour, 84, 252–258.
Qi, J., Lee, B.C., Olsen, N.J. and Park, J.H. (2007). Abnormalities in magnesium (Mg) and ATP levels correlate with muscle dysfunction in polymyositis. Proceedings of the International Society of Magnetic Resonance in Medicine, 15, 2606.
Qi, J., Park, J.H., Kroop, S.F. and Olsen, N.J. (2005). P-31 MRS measures the metabolic changes in a creatine and magnesium supplementation trial for myositis patients. Radiological Society of North America, Radiology, Supplement 237, 400.
Qi, J., Niermann, K.J., Lee, B.C., Olsen, N.J. and Park, J.H. (2008a). Metabolic deficiency in skeletal muscle of dermatolyositis (DM) and polymyositis (PM) patients detected with quantitative P-31 MRS. Radiological Society of North America, Radiology, Supplement 249, 628.
Qi, J., Olsen, N.J., Price, R.R., Winston, J.A. and Park, P.H. (2008b). Diffusion-weighted imaging of inflammatory myopathies: polymyositis and dermatomyositis. Journal of Magnetic Resonance Imaging, 27, 212–217.
Randle, P.J., Hales, C.N., Garland, P.B. and Newsholme, E.A. (1963). The glucose-fatty acid cycle: its role in insulin sensitivity and the metabolic disturbances of diabetes mellitus. Lancet, 1, 785–789.
Rico-Sanz, J., Zehnder, M., Buchli, R., Kuhne, G. and Boutellier, U. (1999). Non-invasive measurement of muscle high-energy phosphates and glycogen concentrations in elite soccer players by 31P- and 13C-MRS. Medicine and Science in Sports and Exercise, 31, 1580–1586.
Rifai, Z., Welle, S., Kamp, C. and Thornton, C.A. (1995). Ragged red fibres in normal aging and inflammatory myopathy. Annals of Neurology, 37, 24–29.
Schroder, J.M. and Molnar, M. (1997). Mitochondrial abnormalities and peripheral neuropathy in inflammatory myopathy, especially inclusion body myositis. Molecular and Cellular Biochemistry, 174, 277–281.
Schunk, K., Pitton, M., Duber, C., Kersjes, W., Schadmand-Fischer, S. and Thelen, M. (1999). Dynamic phosphorus-31 magnetic resonance spectroscopy of the quadriceps muscle: effects of age and sex on spectroscopic results. Investigations in Radiology, 34, 116–125.
Scott, D.L. and Kingsley, G.H. (2004). Use of imaging to assess patients with muscle disease. Current Opinions in Rheumatology, 16, 678–683.
Tarnopolsky, M.A., Mahoney, D.J., Vajsar, J., Rodriguez, C., Doherty, T.J., Roy, B.D. and Biggar, D. (2004). Creatine monohydrate enhances strength and body composition in Duchenne muscular dystrophy. Neurology, 62, 1771–1777.
Welch, K.M.A. and Ramadan, N.M. (1995). Mitochondria, magnesium and migraine. Journal of Neurological Sciences, 134, 9–14.
Wiesinger, G.F., Quittan, M., Graninger, M., Seeber, A., Ebenbichler, G., Sturm, B., Kerschan, K., Smolen, J. and Graninger, W. (1998). Benefit of 6 months long-term physical training in polymyositis/dermatomyositis patients. British Journal of Rheumatology, 37, 1338–1342.
Wortmann, R.L. (2005). Inflammatory Diseases of muscle and other myopathies. In E.D.Harris Jr., R.C.Budd, M.C.Genovese, G.S.Firestein, J.S.Sargent and C.B.Sledge (eds), Kelley’s Textbook of Rheumatology, 7th edn, Vol. 2. Philadelphia: Elsevier Saunders.