Table 2.1 Effectiveness of Selected Drug Prevention Programs

We believe that the possession offense [for marijuana] is of little functional benefit to the discouragement policy and carries heavy social costs, not the least of which is disrespect and cynicism among some of the young. Accordingly, even under our policy of discouraging marihuana use, the better method is persuasion rather than prosecution. Additionally, with the sale and use of more hazardous drugs on the increase, and crimes of violence escalating, we do not believe that the criminal justice system can afford the time and the costs of implementing the marihuana possession laws. Since these laws are not mandatory in terms of achieving the discouragement policy, law enforcement should be allowed to do the job it is best able to do: handling supply and distribution. (National Commission on Marihuana and Drug Abuse 1971)
As noted in Chapter 1, the use of psychoactive substances has been the subject of considerable dispute for much of human history in many parts of the world. These disputes are not based on the question as to whether or not individuals should use alcohol, tobacco, marijuana, cocaine, heroin, and other psychoactive substances to the point where they become addicted or where their physical and/or mental health begins to deteriorate significantly. Almost no one would dispute that these consequences of substance use are undesirable, and they should be prevented or treated. In the vast majority of instances, the real debate over the use and abuse of psychoactive substances concerns the extent to which they should be legal, if at all. The paragraph with which this chapter opens, for example, comes from a report issued to President Richard M. Nixon in 1971 on the legal status of marijuana. Marijuana had been illegal or closely taxed for almost half a century before this report was issued. Continued aggressive action against drugs such as marijuana, cocaine, and heroin was a key element in President Nixon’s domestic program. But the committee reporting to him, the National Commission on Marihuana and Drug Abuse, suggested a new approach to the problem of marijuana use in the United States: decriminalization for possession of small amounts of the drug, and a more vigorous program of prevention to reduce its use. Nixon rejected this and other recommendations made by the committee. As a Schedule I drug, marijuana use continues to be illegal today.
This chapter reviews the ongoing debate about the legal status of alcohol, tobacco, marijuana, and other substances abused by some individuals. First, however, the chapter reviews a discussion of the alternatives posed by the National Commission on Marihuana and Drug Abuse, and by many other expert committees and commissions, professionals in the field of substance abuse, and interested citizens and organizations: the role of prevention and treatment in reducing substance abuse.
No matter how one feels about the legality of alcohol, tobacco, marijuana, and other drugs as substances available for use by the general public, nearly everyone agrees that efforts should be made to prevent people from using these products to a point where their lives are disrupted and to provide treatment for such individuals for the worst effects of substance abuse and addiction. Individuals and agencies at every level—from the federal government to state government to local government to small groups and individuals—have been and are involved in programs of drug prevention. Some groups focus on one part of the problem of substance abuse, targeting alcohol, tobacco, or other drugs for their efforts, while others think that drug prevention programs must include some reference to all substances of abuse.
Literally hundreds of drug abuse prevention programs (also called simply drug education programs) are in existence in the United States today. No brief summary can do justice to the variety of goals, activities, and accomplishments of these programs, but many subscribe to a few general principles. One of the best statements of those principles can be found in a 2003 publication of the National Institute on Drug Abuse (NIDA), Preventing Drug Use among Children and Adolescents: A Research-Based Guide for Parents, Educators, and Community Leaders (Robertson, David, and Rao 2003). The authors of that report list 16 general principles that should guide prevention programs, such as the following:
One of the lead federal agencies dealing with drug prevention education is the Center for Substance Abuse Prevention (CSAP) of the Substance Abuse and Mental Health Services Administration (SAMHSA). The mission of CSAP is to work with local communities to develop programs of substance abuse prevention that are appropriate for that community and its specific problems in this area. CSAP uses a five-step approach in achieving this mission, beginning with an assessment of the specific substance abuse issues faced by a community; an analysis of the resources available within that community to develop a program of prevention, planning, and development of such a program; implementation of the program; and an evaluation of its successes and failures (SAMHSA’s Center for Substance Abuse Prevention 2016).
A number of for-profit and non-profit organizations have also been established to assist schools and communities in the development and implementation of substance abuse prevention programs. Perhaps one of the best known of these organizations is D.A.R.E. (Drug Abuse Resistance Education). D.A.R.E. was established in 1983 by Los Angeles police chief Darryl Gates and one of his deputy chiefs, Glenn Levant, as a way of trying to deal with the problem of substance abuse, especially among teenagers, in Los Angeles. D.A.R.E.’s drug prevention program consists of a series of classes run by police officers who have had at least 80 hours of training in drug prevention programs. The organization claims to have a presence in 75 percent of all American school districts and in 43 foreign countries (D.A.R.E. 2016).
An important question about D.A.R.E.—and all other drug prevention programs—is how effective they are. Does participation in a D.A.R.E. class, or any other drug prevention program, actually reduce the likelihood that individuals will become involved in substance abuse? A number of studies have been conducted to answer this question. One of the best known of these studies was prepared by the Office of the Surgeon General of the United States in 2000. Among its many objectives, that report attempted to identify substance abuse programs that were and were not effective. It classified a number of programs as “model programs,” because there was sound scientific evidence that the programs significantly reduced the likelihood that participants would become involved in substance abuse: as “promising,” because they showed evidence of achieving this goal; and as “does not work,” because available evidence did not support the goal of reducing substance abuse and, in some cases, actually increased the likelihood that participants would become involved in substance abuse (Youth Violence: A Report of the Surgeon General 2001, 102–109). Table 2.1 shows some of the programs that fell into each of the three categories.
It is interesting that D.A.R.E. was one of only two programs classified as Does Not Work in the report (the other being a program called “Scared Straight”). Authors of the report acknowledged the widespread popularity of D.A.R.E. but explained that it was classified as Does Not Work because “numerous well designed evaluations and meta-analyses … consistently show little or no deterrent effects on substance use. Overall, evidence on the effects of the traditional DARE curriculum … shows that children who participate are as likely to use drugs as those who do not participate” (Youth Violence: A Report of the Surgeon General 2001, 110).
The D.A.R.E. program has been subjected to a number of similar criticisms over the years and has focused on improving its work with young people to reduce substance abuse. In 2014 it announced a new program that it claimed actually worked and attempted to recover some of the good will that it had earned many years earlier (The New D.A.R.E. Program—This One Works 2014).
The question remains, however, how an ordinary person can determine the effectiveness of a drug prevention program. There certainly is no shortage of such programs, many of which are advertised on the Internet. But scientific evidence for the quality of such programs is in short supply, and the average consumer has little to base a decision in the selection of prevention programs to recommend to friends and loved ones. (One modest exception is a review of a small number of such programs provided by SAMHSA on its website at http://nrepp.samhsa.gov/AdvancedSearch.aspx.)
A position on which the vast majority of substance abuse experts can now agree is that people who abuse drugs or become dependent upon or addicted to them require some form of treatment to help them deal with their problem. That treatment is often not available, however, or those who need it do not get the treatment that is available. According to the 2014 National Survey on Drug Use and Health survey, an estimated 22,478,000 Americans over the age of 12 needed some form of treatment for substance abuse in 2014, of whom about 2,606,000 actually received treatment. Corresponding numbers for those in the age group 12 to 17 were 1,284,000 requiring treatment and 109,000 receiving it; 5,845,000 needing treatment in the age group 18 to 25 and 470,000 receiving it; and 15,349,000 in the 26 years and older group needing and 2,028,000 receiving treatment (Results from the 2014 National Survey on Drug Use and Health: Detailed Tables 2015, Table 5.51A).
As is the case with substance abuse prevention programs, a number of organizations and agencies have developed principles upon which programs of substance abuse treatment should be based. The NIDA has provided one such set of guidelines in one of the newsletters in its InfoFacts newsletters. Among the general principles the NIDA suggests are the following:
(quoted from DrugFacts: Treatment Approaches for Drug Addiction 2016)
As these guidelines suggest, treatment for substance abuse and addiction usually makes use of two approaches: medication and behavioral therapies. Medications are sometimes the first line of attack for individuals who have actually become addicted to a substance. Such is most often the case with opiate addictions, in which case three medications are generally available for use: methadone, naltrexone, and buprenorphine. A fourth drug, levo-alpha-acetylmethadol (LAAM), is also approved for use, but, because of risky side effects, not as commonly prescribed. Three medications have also been approved by the U.S. Food and Drug Administration (FDA) for the treatment of alcohol dependence and addiction: naltrexone, acamprosate (Campral), and disulfiram (Antabuse). Nicotine dependence and addiction can be treated by a variety of over-the-counter patches, sprays, gums, and lozenges that reduce the need for nicotine, as well as by two FDA-approved drugs: bupropion (Zyban) and varenicline (Chantix)). For some types of substances, such as cocaine and marijuana, no medications are available for assisting a person with withdrawal and treatment of a dependence or addiction. After a person has gone through the worst stage of recovery—withdrawal from use of a substance—then personal and group counseling is often helpful in weaning him or her entirely from the substance.
One might reasonably ask which types of treatment work best for each type of substance abuse and addiction for which individuals and under what circumstances. In fact, researchers have conducted many studies on just such issues. Because of the many variables involved, it is not possible to make simple assessments as to any one part of this complex equation. There is, however, an abundance of information about specific types of treatment for specific situations. One of the best resources for that information is a website operated jointly by the NIDA, the National Development and Research Institutes, Inc., the University of California at Los Angeles Integrated Substance Abuse Program, and the Texas Institute of Behavioral Research at Texas Christian University. The website is called Drug Abuse Treatment Outcome Studies (DATOS). Readers interested in learning more about the effectiveness of various types of treatments for individuals of various ages dealing with specific types of substance abuse under specific types of conditions should refer to this website at http://www.datos.org/.
More recent suggestions for successful treatment programs are also available. One book that deals specifically with this issue is Inside Rehab: The Surprising Truth about Addiction Treatment—and How to Get Help That Works, by medical writer Anne M. Fletcher (Viking 2013). Fletcher reports on her visits to 15 treatment programs and interviews with more than 200 clients to explain why most programs work much less effectively than they claim to or could work (see also Brody 2013).
As the preceding sections suggest, many specialists in the field of substance abuse are looking for ways for dealing with the problem that goes beyond traditional prevention and treatment options. Two such ideas that have shown promise are drug courts and recovery schools.
Drug courts are facilities that offer modified forms of traditional criminal courts consisting of prosecution, defense, and a judge or jury that meet to hear evidence in a criminal case and then decide on a person’s guilt or innocence and any punishment that may be appropriate. In drug courts, all of these elements, along with counselors, social workers, psychologists, mental health experts, and others with specialized knowledge and skills, meet to decide the best response to individuals and cases not well treated in traditional courts. Specialized drug courts have been developed for dealing with adult and young adult substance abusers, veterans, family dependency problems, tribal issues, and DWI (driving while intoxicated).
In general, the goal of drug courts is to find alternatives to sentencing and imprisonment for individuals arrested for substance-related crimes. In most cases, the court team meets to consider an individual’s background and involvement in substance abuse and to decide the most appropriate treatment before developing a treatment plan, which may consist of various forms of monitored treatment (counseling, medication, etc.) and preparation for post-release guidance and assistance. Individuals who successfully complete the prescribed course of action may have their records expunged, along with the chance to have a fresh beginning in dealing with their substance abuse issues.
The first drug court was created in Miami-Dade County, Florida, in 1989, in response to the epidemic of crack cocaine abuse then occurring in the area. Over time, the number of drug courts has increased until, at the end of 2014, there were 3,057 such courts in all 50 states, the District of Columbia, Guam, and Puerto Rico (Drug Courts 2016).
Another fairly new approach to substance abuse treatment is recovery schools. A recovery school is an educational program designed for young adults who are recovering from substance abuse. They have been developed because of the high rate of recidivism among such students who leave a (usually successful) treatment program and then return to the educational setting from which they came in the first place. This series of events has a tendency to result in an individual’s falling back into old habits and reverting once more to the substance abuse for which he or she had been treated.
The first recovery school was Sobriety High, established in Burnsville, Minnesota, in 1987, with just two students. The school later reached an enrollment of more than 100 before closing down in 2013. As of 2016, there were 25 recovery schools located in eight states, with plans to expand their presence over the next few years (Are Recovery High Schools Really Working? 2016).
Recovery schools may take a number of forms. Some, for example, are located in traditional schools, with some form of physical separation available for recovery students. Others may be housed in free-standing structures separate from traditional schools. Recovery students are expected to complete the state-mandated curriculum required of non-recovery students, but are provided with a variety of support options, such as specialized counseling, guidance, and health services (Vimont 2011). The parent association for recovery schools is the Association of Recovery Schools (https://recoveryschools.org/), from which more detailed information about the topic may be obtained. For an important evaluative study of recovery schools, see Moberg and Finch (2008).
As noted at the beginning of this chapter, the abuse of psychoactive substances, such as alcohol, tobacco, marijuana, and other drugs, has been a matter of concern in the United States for at least a century. Individuals, private organizations, and government agencies have searched for ways of dealing with this problem, with prevention and treatment programs being viewed as two possible solutions. A number of other ways of dealing with substance abuse have also been developed. One of these methods is drug testing. The 1960s and 1970s saw a dramatic increase in substance abuse in the United States. In some cases, as discussed for the use of marijuana in Chapter 1 of this book, that increase may have represented a general rejection of moral standards by some younger members of society. But increased substance abuse was also directly linked to the Vietnam conflict of the early 1960s to 1975. Many men and women who served in Vietnam sought relief from the horrible conditions they faced there by turning to alcohol and other drugs. By the end of the war, very large numbers of personnel had either used drugs from time to time or had become addicted to them. To track the severity of this problem, the Department of Defense ordered that returning veterans be randomly tested for drug use before being discharged from the service, a program that eventually earned the sobriquet of Operation Golden Flow (Holland 2015).
For a variety of reasons, President Richard M. Nixon soon overturned the Pentagon’s drug testing plan. But the idea of identifying substance abusers in the society as a whole, but especially in the workplace, had already begun to set in. Many studies have been done on the prevalence of drug testing in the workplace over the past four decades, but most seem to suggest that businesses began to see value in screening job applicants (and, less commonly, current employees) for illegal drug use as early as the 1970s. During the 1980s, however, the number of businesses that had adopted such programs increased dramatically, from about 20 percent at the beginning of the decade to more than twice that number at the end of the decade. The longest continuous series of studies on drug testing in the workplace is one conducted by the American Management Association (AMA), which collected data on the topic for more than two decades. AMA surveys show that the percentage of businesses contacted that require preemployment drug testing rose to a peak of 81 percent in 1996. It then began to fall off fairly rapidly until it reached a new low of 62.6 percent in 2004, the last year in which AMA conducted the survey (DePillis 2015). Throughout this period, the number of companies that tested current employees in addition to new hires was consistently much less, usually by a factor of one-half, than those who screened for preemployment purposes.
Proponents of drug testing in the workplace offer a number of arguments in support of their position. First, they point out that workers who are under the influence of illegal substances are more likely to have or cause accidents in the workplace, causing injuries and deaths to coworkers, innocent bystanders, and themselves, and costing the company significant amounts of money in property loss. A number of studies appear to confirm this position. For example:
Proponents of workplace drug testing also pose a number of other arguments in favor of the practice. For example, they point to data that suggest that workers who are drug-free tend to be more productive at their jobs. They also suggest also that the use of illegal substances in the workplace may affect general morale and reduce the ability of coworkers to do their own jobs efficiently. Finally, they believe that testing programs may be an important factor in helping to reduce the problem of substance abuse overall, since workers will have to reduce or discontinue use of illegal substances if they are to be hired for or retain a job (Newton 1999, 31–38).
Opponents of drug testing have their own counterarguments. They point out, in the first place, that drug testing can be a significant intrusion on a person’s privacy, which is protected in the United States by the Fourth Amendment to the U.S. Constitution’s ban on “unreasonable searches and seizures.” Since the vast majority of drug tests are conducted randomly and are not based on some illegal or improper act on the part of the testee, they would appear to violate this constitutional protection. Second, opponents note that drug tests tend to be notoriously unreliable with high percentages of false positives (a positive test when a person has not actually used a drug) and false negatives (a negative test when a person has been using a drug). The authority most often cited in defense of this position is a study conducted by the National Research Council in 1994, which concluded that “[d]espite beliefs to the contrary, the preventive effects of drug-testing programs have never been adequately demonstrated” (Normand, Lempert, and O’Brien 1994, 11).
The debate over the effectiveness of workplace drug testing continues well into the second decade of the twenty-first century. A meta-analysis of 23 studies on the question conducted in 2014 produced mixed results on the question. Researchers concluded that “the effectiveness of testing in improving workplace safety is at best tenuous,” but that the quality of the research that had been conducted was, in general, so poor that making firm conclusions was difficult (Pidd and Roche 2014, 154). Still, by the end of 2016, there seemed to be a strong consensus in the general literature that workplace drug testing has not, in its 40-year history, proved its value to industry, to workers, or to the country at large (Engber 2015).
Opponents of workplace drug testing also argue that such programs are not cost-effective. In a 1991 study of the use of drug testing in federal agencies, for example, the cost of identifying a single substance abuser was estimated to be about $77,000 (cited in Zimmer 1999, 14). That number may be a gross underestimate, however, if one assumes (probably correctly) that only one out of ten individuals who tests positive is a serious substance abuser. In such a case, the actual cost of identifying a single individual likely to be a risk in the workplace may range from $700,000 to $1.5 million (Donohoe 2005, 72). Given a number of options for locating potential substance abuser risks in the workplace, some critics say, other options to drug testing should be considered. (An excellent review of the issues involved in workplace drug testing on the Internet is this pair of websites: Olson 2004a and Olson 2004b.)
Finally, opponents of drug testing in the workplace sometimes point to the fact that most testing programs ignore the one drug—alcohol—responsible for by far the greatest proportion of accidents in the workplace.
Arguably the most serious issue about workplace drug testing has arisen because of the actions by some states to legalize the use of marijuana for medical and recreational purposes. Until the early twenty-first century, debates over the pre- and post-hiring testing for marijuana were moderated to some degree because of the fact that the drug was, after all, illegal. It was listed as a Schedule I drug by the federal government. Now, the drug is legal in nearly half of the states, and the question arises as to whether a job candidate or employee can or should be refused employment or fired because of testing positive for marijuana.
For some observers, the answer to that question is simple: Marijuana is an illegal drug; employers can test for it and act on test results. This position was taken perhaps most prominently by the Colorado Supreme Court in 2015 when it ruled in Coats v. Dish Network that Brandon Coats, a quadriplegic employee of Dish Network, was fired because he failed a workplace test for marijuana, a drug he takes for the pain associated with his medical condition. The court ruled that the company was within its rights to fire an employee who used an illegal drug (by federal standards), no matter what state law said (Coats v. Dish 2015).
Other stakeholders have taken a very different view of the problem. They argue that it is now legal to use marijuana for medical and/or recreational purposes in some states, so actions such as those taken by Dish are simply penalizing private citizens for conducting legal actions in the privacy of their own homes. Dish’s action, and that of the vast majority of employers, was not based on a worker’s performance on his or her job, but on some behavior conducted away from the workplace that may or may not have influenced the quality of his or her work. Since positive results for marijuana smoking can be collected up to ten days following the actual act, it is not clear the extent to which the act of smoking may or may not have affected a person’s job performance (Wallace 2015).
As of late 2016, no clear trend had developed as to how this new issue will be resolved. Attendees at an annual conference of the Society for Human Resource Management in 2015 packed a session on the nature of the problem companies were facing, possible actions by employees, and ways in which employers could or should react to those actions (Pratt 2015). Meanwhile, the state of Vermont was holding high-level meetings to determine how the state’s new medical marijuana law would affect workplace drug testing policies in the states. A period of controversy and debate can only be expected on this question over the near future (Bielawski 2015; for an excellent overview of this issue, see DuPont 2015).
Businesses are by no means the only place where drug testing has become somewhat routine and, at the same time, controversial. The practice is also carried out now in many schools, colleges, and universities, and in professional sports. In fact, the debate over the use of drug testing in schools began just at the nexus of these two issues when a number of school districts in the late 1980s and early 1990s decided to institute mandatory drug tests for students who wished to participate in sports at the schools. Drug testing in schools was initiated among athletic teams for a number of reasons, one being that illicit drug use was sometimes thought to be (correctly or not) especially common among student athletes. In addition, participation in athletics is a voluntary activity, unlike school attendance itself, and so boys and girls can choose whether or not to submit to drug tests. Finally, some school districts felt that student athletes should be presentable as desirable role models for the rest of the student body.
In any case, mandatory drug testing for student athletes was met in some instances by objections from individuals who objected to the practice for one reason or another. The case that eventually drew the most attention nationwide involved a decision by the Vernonia School District in Oregon in 1991 to require student athletes to be tested for a number of illicit drugs. One student, James Acton, objected to the policy and filed suit to have the district’s policy declared unconstitutional. That case worked its way through the courts and was eventually decided four years later by the U.S. Supreme Court, which ruled in favor of the school district by a vote of 6 to 3 (Vernonia School Dist. 47J v. Acton 515 U.S. 646 1995; an excerpt from that decision also appears in Chapter 5 of this book). That decision served as an important precedent for lower courts, which eventually issued decisions allowing drug testing of students who participate in any extracurricular activity and even of students who drive to school.
Another Supreme Court decision on school drug testing came in 2002 in the case of Board of Education of Independent School District No. 92 of Pottawatomie County v. Earls (536 U.S. 822), when the Court ruled by a 5 to 4 vote that schools could require drug tests from students who participate in any extracurricular activity. Writing for the majority, Justice Clarence Thomas made the point that “[g]iven the nationwide epidemic of drug use, and the evidence of increased drug use in Tecumseh schools, it was entirely reasonable for the School District to enact this particular drug testing policy” (Board of Education of Independent School District No. 92 of Pottawatomie County v. Earls 2002).
Today, drug testing in schools may take a number of different forms. It may involve student athletes only, participants in other types of extracurricular activities, a random sample of the student body, or all members of the student body on either a voluntary or a required basis. A frequently cited study on this variety of programs found that about 20 percent of all schools (containing about 20% of all students in the country) had one or another of these programs (Yamaguchi, Johnston, and O’Malley 2003, 22–23, Table 2). The most popular program was one in which testing was required only when there was specific cause or reason to suspect illicit drug use, with about 13 percent of all schools (and 13.4% of all students) involved in this type of program. The pattern of drug testing programs in about 170 schools from 1998 to 2002 is shown in Table 2.2 (for more recent, but limited, data, see Ringwalt et al. 2008).
As with workplace drug testing, arguments both in support of and in opposition to drug testing in schools have been presented, and, in many cases, the arguments are similar to those used in the workplace controversy. Most importantly, proponents of testing say, schools should do something to stem the tide of substance abuse in the nation, and carefully controlled testing of all or certain groups of students is one way to do that. Besides, students who do not use drugs have nothing to fear from substance testing. Opponents disagree, pointing out that less invasive methods of drug prevention are available, and students should not have to give up their right of privacy for the purposes of drug testing (see, for example, Anderson 2012).
Research on the effectiveness of school drug testing has produced somewhat conflicting results. A study of seven school districts with 36 high schools that had received grants from the U.S. Department of Education for drug prevention programs found that “students subject to MRSDT [the trial program: mandatory-random student drug testing] reported less substance use than comparable students in high schools without MRSDT.” The study found no other effects on students in the trial program or any “spillover” effects to students not enrolled in the program (James-Burdumy et al. 2010, xvii). More commonly, research appears to find fewer or no effects on drug use as a result of drug testing programs. At least two large-scale reviews of studies on the effectiveness of school drug testing (Stuart 2010; Sznitman and Romer 2014) have found little or no evidence that those programs changed drug use patterns among students required to take those tests. Perhaps the most significant reflection of this trend was a position paper released by the American Academy of Pediatrics in 2015. That document noted that the organization “opposes widespread implementation of these programs because of the lack of solid evidence for their effectiveness” (Levy, Schizer, and Committee on Substance Abuse 2015, 782). Although the fervor for school testing appears to have cooled to some degree since the late twenty-first century, the debate continues at a reduced level over the practice.
While interest in drug testing in the workplace and schools appears to have diminished somewhat (in the first instance) or remained about constant (in the second), it has increased quite significantly in one other situation: professional sports. Some modest efforts to limit the use of illegal substances by athletes go as far back as 1970, when the National Collegiate Athletic Association (NCAA) first established a Drug Education Committee to provide information about drug use among college athletes. It took more than 10 years, however, for the NCAA to authorize a study of the use of drugs by college athletes and 16 years before the association actually began testing athletes. That program was initiated for championship and bowl games in the fall of 1986, based on a list of banned substances adopted a year earlier by the NCAA. Today the NCAA bans thousands of drugs that fall into eight major categories: stimulants, anabolic agents, alcohol and beta-blockers, diuretics and other masking agents, street drugs, peptide hormones and analogues, anti-estrogens, and beta-2 agonists (2016–2017 NCAA Banned Drugs 2016). Most of these substances have short-term effects and must be taken just prior to an activity or in an effort to mask the use of an illegal substance (masking agents). They are, therefore, relatively easy to detect by standard drug tests.
The exception to that statement is the anabolic agents, also known as anabolic-androgenic steroids (AAS), substances that are chemically similar to the male sex hormone testosterone. AAS are popular among athletes because they produce weight gain, which occurs almost entirely in the form of muscle mass, increasing an individual’s strength, speed, and endurance. AAS compounds also have a number of troubling side effects, however, which provide an important argument against their use. These side effects include increased blood pressure and blood cholesterol levels along with increased risk for cardiovascular disease, acne, and liver damage. A number of mental conditions have also been associated with steroid use, including aggression and violence (sometimes called “roid rage”), mania, and psychosis.
Anabolic agents are the primary cause of concern among both amateur and professional sports associations because athletes value their effects so highly and they are more difficult to detect than are stimulants, masking agents, and other drugs. In many cases, it is difficult to know if an athlete is bigger, stronger, and faster as the result of training or because he or she has been taking AAS drugs. Probably the most dramatic example of this dilemma has been the revelation that many of the best-known and most successful professional baseball players achieved their physical superiority not just by training, but by the use of substances that have long been banned in most sports, although not in professional baseball until 2004 (Newton 2014; Quinn 2015).
Today, nearly all amateur and professional sports organizations have drug testing programs for a number of illegal substances. National Football League regulations, for example, call for a four-game suspension after a first positive test, a six-game suspension after a second positive test, and a one-year suspension after a third positive test. A policy adopted by Major League Baseball in 2005 calls for counseling of a player who tests positive for an illegal substance the first time; a 15-day suspension and maximum fine of $10,000 after a second positive test; a 25-day suspension and a maximum fine of $25,000 after a third positive test; a 50-day suspension and a maximum fine of $50,000 after a fourth positive test; and a one-year suspension and maximum fine of $100,000 after a fifth positive test. Both the National Basketball Association and the National Hockey League have roughly similar drug testing programs (Professional Sports and Their Drug Policies 2016).
As discussed in Chapter 1, many countries have, at one time or another in their histories, struggled with the question of how to control the use of one psychoactive substance or another within their boundaries. Three approaches have frequently been used in such efforts: education, taxation, and outright prohibition.
Educational efforts are based on the assumption that the more people know about the deleterious effects of a substance, the less likely they are to use those substances for recreational purposes. One of the classic examples of this approach to dealing with a psychoactive substance in the United States has been the Women’s Christian Temperance Union (WCTU). The WCTU was founded in Cleveland, Ohio, in November 1874 as the outgrowth of an 1873–1874 campaign known as the Woman’s Crusade. During this campaign, a number of ordinary housewives decided to rebel against what they saw as the evils of drinking alcohol that they had experienced in their communities firsthand. They organized “sit-ins” and “pray-ins” at local taverns, demanding that the sale of liquor be discontinued. Within the first three months of their campaign, these women had driven more than 250 establishments out of business (Early History 2016).
One of the WCTU’s earliest programs was an effort to introduce anti-alcohol education into public schools. In 1879, the organization created a permanent committee, a year later to become the WCTU Department of Scientific Temperance Instruction in Schools and Colleges, for this purpose. WCTU members were encouraged to appear before their local school boards of education to demand that anti-alcohol classes be included in the regular curriculum, and the organization itself began to produce materials to be used in such classes, including a textbook called Alcohol and Hygiene. When these efforts proved to be only moderately successful, the organization aimed its sights higher: at state legislatures. It lobbied for the introduction of bills that would require local districts to adopt anti-alcohol curricula, an effort that was first successful in the state of Vermont in 1882. The pressure from WCTU members was so great that Vermont legislators passed the bill by large majorities in both houses (Hanson 2009). This success was replicated elsewhere in the country, and by the end of the century, some form of anti-alcohol education law had been adopted by almost every state, the District of Columbia, and all U.S. possessions (Hanson 2009).
The success of educational efforts like those of the WCTU is difficult to determine. On the one hand, the average annual consumption of alcohol in the United States actually increased in the years in which the WCTU was most successful in passing legislation on anti-alcohol education. That number increased from 1.72 gallons of alcohol per person per year in the decade of 1871–1880 to 2.06 gallons in 1896–1900 to 2.56 in 1911–1915, a 49 percent increase in consumption in about 40 years (Nephew et al. 2002, 18, Table 1). Average alcohol consumption among Americans was not to reach that level again until the 1970s. On the other hand, the efforts of the WCTU have generally been credited with providing the momentum that eventually culminated in the great “noble experiment” to ban alcohol completely in the United States with the Eighteenth Amendment to the U.S. Constitution in 1919. That amendment did not actually ban the consumption of alcoholic beverages; it prohibited the manufacture, sale, and transportation of such beverages within the United States. The educational efforts originally promoted by the WCTU and other temperance organizations thus evolved over time into a very different type of effort to restrict the consumption of alcohol: legal remedies, the strongest of which, of course, was an amendment to the U.S. Constitution.
Many books and untold numbers of scholarly papers have been written about the American prohibition movement, the name given to the effort to stamp out the drinking of alcoholic beverages in the United States between 1919 and 1933 (the year in which the Twenty-First Amendment to the Constitution, rescinding the Eighteenth Amendment, was adopted). Experts in the area have drawn conclusions from across the board, from the experiment having been a great success in terms of reducing the consumption of alcohol among Americans to its having been a nearly total failure, on the basis not only of no change in drinking habits, but also in terms of the explosion of crime engendered by the need to supply drinkers with alcoholic beverages illegally. Of course, statistical data about alcohol consumption during the period of 1919–1933 is unavailable, since alcoholic beverages were illegal at the time. A number of studies suggest, however, that the Eighteenth Amendment had, at best, only limited success in reducing the consumption of alcohol. These studies show that the number of deaths from alcohol-related problems, the age at which males and females began drinking, and the number of arrests for drunkenness and other alcohol-related problems all suggest a significant increase in the amount of alcohol consumption during the period (Schaffer 2016).
World history is replete with examples of efforts to control the use of psychoactive substances by means of taxation or methods that fall short of actual, total prohibition. Probably the earliest example in American history of such an effort was the whiskey tax of 1791, imposed by the federal government on the producers of that beverage. The tax was imposed by the young U.S. government for a number of reasons, perhaps the most important of which was the dire financial status of the government. Under provisions under which the federal government was established, that government was required to assume all of the debts accumulated by the states in association with the Revolutionary War. The government began operation, then, with a huge debt. The first secretary of the Treasury, Alexander Hamilton, envisioned a modest tax on alcoholic spirits (whiskey, in particular) as being a possible lucrative source of income for paying down this debt. Even before the new government had formed, Hamilton presaged this idea in his earlier writings. In the Federalist Papers, for example, he had written that “[t]he single article of ardent spirits, under federal regulation, might be made to furnish a considerable revenue” (Hamilton 1904, 280). Interestingly, Hamilton’s interest in a tax on spirits was motivated by more than just a concern about revenue. He concluded the paragraph from which the previous quotation is taken with the observation that “[t]hat article [spirits] would well bear this rate of duty; and if it should tend to diminish the consumption of it, such an effect would be equally favorable to the agriculture, to the economy, to the morals, and to the health of the society. There is, perhaps, nothing so much a subject of national extravagance as these spirits” (Hamilton 1904, 280).
In 1791, then, Hamilton was able to convince the Congress to impose a tax on alcohol, based in part on the size of the manufacturing operation: large companies paid six cents a gallon in tax, while small companies paid nine cents a gallon, a system that was almost guaranteed to produce strong opposition from the latter, most of whom were then located on the western frontier. That opposition eventually boiled over into the so-called Whiskey Rebellion of 1794, with armed uprising breaking out in many of the colonies. That rebellion continued for more than five years and was met with considerable force by federal troops, whose action was necessitated at least in part by the government’s desire to establish a strong central government within the new nation. Even though the federal troops prevailed in armed conflict on the field, opposition to the tax was so strong that it was eventually repealed in 1802.
The U.S. government has sometimes taken somewhat circuitous routes—short of outright bans—to the control of psychoactive substances other than alcohol. Such was long the case with cocaine and opiates. During the second half of the nineteenth century, these substances were generally available to the public and unregulated by the government. The Sears, Roebuck catalogs of the late nineteenth century, for example, carried advertisements for “coca wine” that was recommended for the treatment of neuralgia, sleeplessness, and despondency (Pearce 2016). Some catalogs also listed small quantities of cocaine accompanied by a syringe with which to inject the drug, sold for $1.50 (Buxton 2006, 16–17). Perhaps the best-known everyday use of cocaine, however, was as an ingredient in a popular new soft drink invented by Atlanta pharmacist John Pemberton in 1885, Coca-Cola. Originally sold as a patent medicine, the drink soon became widely popular as a refreshing soft drink. As its name clearly announces, the drink originally contained cocaine. By 1903, however, the drug was removed, largely in response to growing concerns about its harmful and addictive effects.
By the turn of the century, pressures for some kind of control over the use of cocaine and opiates began to grow from both national and international sources. The first factor of importance was the annexation by the United States of the Philippine Islands, one of the penalties paid by Spain following its defeat in the Spanish-American War of 1898. Along with the many natural resources provided by the Philippines, the United States inherited a very large population of residents of the island who had become addicted to cocaine. The federal government was forced to develop some program for dealing with these individuals. The decision was finally reached that addiction to cocaine and other drugs, such as opiates, was really an international problem, rather than one restricted to the Philippines. As a consequence, President Theodore Roosevelt called for an international conference, called the International Opium Commission, to be held in Shanghai in February 1909. That meeting was followed by a second international conference, held at The Hague, the Netherlands, in May 1911. The Hague conference adopted the first international treaty for the control of psychoactive substances, calling for all signatories to do whatever they could to “control, or to cause to be controlled, all persons manufacturing, importing, selling, distributing, and exporting morphine, cocaine, and their respective salts, as well as the buildings in which these persons carry such an industry or trade” (International Opium Convention Signed at The Hague January 23, 1912 1912, Article 10, page 197). The treaty provided a powerful impetus for the U.S. government to adopt measures for the control of cocaine and opiates within its own borders.
Domestic issues also contributed to the increasing pressures for regulation of psychoactive substances. By the first decade of the twentieth century, medical studies began to show possible health issues associated with the use of these substances, for example, an increase in respiratory diseases in connection with the use of cocaine. Law enforcement officers also pointed to the legal problems created by addicts needing the money required to support their drug habits. And a number of religious and social leaders grew increasingly concerned about the moral effects of the apparent spread of cocaine and heroin use among Americans. As perhaps to be expected, much of the blame for the nation’s growing substance abuse problem fell on minority groups. A committee appointed to study this problem in 1902, for example, singled out Chinese immigrants as a major factor in the substance abuse problem faced by Americans. In its report, the Committee on Acquirement of the Drug Habit noted that opium use was rife among Chinese immigrants and concluded somewhat ominously that “[i]f the Chinaman cannot get along without his dope we can get along without him” (Report of Committee on Acquirement of the Drug Habit 1902, 572). Criticism increasingly fell on the African American community also. A number of legislators, law enforcement personnel, and experts in the field of substance abuse pointed out that cocaine and heroin use was especially common among blacks, often with terrible social consequences. A leading advocate for stricter controls on drugs, Hamilton Wright, the first opium commissioner of the United States, said at the Shanghai convention in 1909 that “cocaine is often the direct incentive to the crime of rape by the Negroes of the South and other sections of the country” (Musto 1987, 43–44). (Somewhat ironically, no credible evidence existed for Wright’s claim, or for any of the other similar warnings raised about the special problems that blacks created by their abuse of illegal substances [Courtwright 1995, Chapter 10].)
The confluence of international and domestic pressures led in 1914 to the adoption of the Harrison Act, the first federal legislation designed specifically to control the consumption of cocaine and opiates in the United States. (The act was actually written by Wright, although introduced by Rep. Francis Burton Harrison of New York.) The main provision of the act was the requirement that all individuals who “produce, import, manufacture, compound, deal in, dispense, sell, distribute, or give away opium or coca leaves, their salts, derivatives, or preparations, and for other purposes” register with federal officials and pay a tax on all their proceedings (Harrison Narcotics Tax Act, 1914). The practical effect of the Harrison Act was to make the possession and consumption of cocaine and opiates illegal for any use other than medical applications. As an attempt to solve the nation’s substance abuse problems, however, it was a failure, producing almost the opposite result. Individuals who had become dependent on cocaine or an opiate could no longer obtain their drug of choice legally and found it necessary to find ways of getting it on the black market and, in many cases, to commit crimes to get the money they needed for the increasingly expensive product.
Recognizing this disturbing trend, the secretary of the Treasury, William Gibbs McAdoo, appointed a committee to evaluate the effects of the Harrison Act. The committee reported a number of trends as a result of the act’s passage, perhaps most significant of which was that (1) the use of cocaine and opiate had actually increased since the adoption of the act and (2) a thriving new community of “dope peddlers” had arisen, bringing drugs illegally into the country from Canada and Mexico (Brecher 1972, Chapter 8). To remedy this situation, the committee recommended more of the same, that is, amendments to the Harrison Act that would increase penalties for illegal use of cocaine and opiates. Within a year of adoption of the new amendments in 1924, signs appeared that stricter enforcement of the Harrison Act was not working either. An editorialist for The Illinois Medical Journal wrote in 1926 that “[t]he Harrison Narcotic law should never have been placed upon the Statute books of the United States … instead of stopping the [drug] traffic, those who deal in dope now make double their money from the poor unfortunates upon whom they prey” (Brecher 1972, Chapter 8).
The “tax and regulate” approach to controlling cocaine and opiates has also been used with other psychoactive substances. The 1937 Marihuana Tax Act is an example. (Note that the modern spelling of the substance, marijuana, is of relatively recent origin, with an “h” instead of a “j” being more common historically.) Marijuana is obtained from the cannabis plant, of which three species are of commercial significance: Cannabis sativa, C. indica, and (less commonly) C. ruderalis. The plant is an annual dioecious (one type of gamete per plant) flowering herb that grows to a height of about 3 meters (10 feet). It has historically been utilized primarily for two purposes. First, the soft, flexible fibers obtained from its stalk—known as hemp—are used in the manufacture of more than 25,000 industrial products, including paper, cloth, construction materials, medicines, and biofuels (Hemp Facts 1997). Second, the dried flowers and leaves of the plant are smoked to produce a “high” for recreational and religious purposes.
For the first 300 years of American history, hemp was a very popular commercial crop. As early as 1619, the Virginia Assembly passed a law requiring every farmer to grow at least some hemp to be used both for domestic purposes and for exportation and foreign trade. Hemp was also used as legal tender at the time in Maryland, Pennsylvania, and Virginia. The fiber became especially popular during the Civil War when it was used as a substitute for cotton and other natural materials by both sides in the war (Abel 1980, Chapter 8). Largely because of its association with marijuana, hemp largely disappeared as a commercial crop in the United States for many years. Recently, however, a number of states have passed laws allowing the farming of cannabis plants for the production of industrial hemp or the conduct of research on industrial hemp (State Industrial Hemp Statutes 2016).
The use of cannabis products for purely recreational purposes appears to have had its beginning in the United States in the 1910s, when immigrants fleeing the Mexican Revolution arrived in this country, often bringing with them a long-standing recreational habit: the smoking of marijuana. The marijuana used for this purpose comes from cannabis plants botanically different from those used for the production of hemp. The latter have been developed to contain the lowest possible amount of Δ9-tetrahydrocannabinol (THC), the chemical responsible for the psychoactive effects of ingesting marijuana plant products. By contrast, other types of cannabis plants have been developed with relatively high concentrations of THC which, in general, have stalks that yield poor-quality hemp unsuitable for commercial use. By the early 1930s, the use of marijuana for recreational purposes had become relatively widespread in some parts of the United States, producing a reaction among law enforcement officials, governmental officials, and many private organizations and individuals. In many cases, the objections to the use of marijuana appear to have had their basis in a general fear and dislike of the immigrants who first brought the product to the United States (Abel 1980, Chapter 11). In any case, by 1931, 29 states had outlawed the use of marijuana, and the federal government had begun to consider ways of banning its use nationwide (Abel 1980, Chapter 11).
The first step in this direction occurred in 1937 when the U.S. Congress passed and President Franklin Delano Roosevelt signed the Marihuana Tax Act. Justification for the legislation was based to a considerable extent on some questionable statements about the effects of marijuana on the human personality. In his testimony before Congress as it considered the marijuana bill, for example, Commissioner of Narcotics Harry J. Anslinger said that while the drug first produces feelings of “well-being [and] a happy, jovial mood,” that euphoria is soon replaced by much less salubrious emotions, including:
a more-or-less delirious state … during which [users] are temporarily, at least, irresponsible and liable to commit violent crimes … [and] releases inhibitions of an antisocial nature which dwell within the individual… . Then follow errors of sense, false convictions and the predominance of extravagant ideas where all sense of value seems to disappear.
The deleterious, even vicious, qualities of the drug render it highly dangerous to the mind and body upon which it operates to destroy the will, cause one to lose the power of connected thought, producing imaginary delectable situations and gradually weakening the physical powers. Its use frequently leads to insanity. (The Marihuana Tax Act of 1937 2016a)
The bill that was finally passed by Congress did not specifically outlaw the production, sale, or consumption of marijuana, but it did impose a somewhat complex system of taxes and regulations. Anyone involved in any of these activities had to register with the federal government and to pay a tax for each type of activity. For example, anyone who grew or processed a cannabis product had to pay a tax of $24 annually (equivalent to $405 in 2016 dollars). The tax for sale of a cannabis product to anyone who already held a license was $1 per transaction ($17 in 2016 dollars), but $100 ($1,700 in 2016 dollars) to anyone who did not hold such a license (The Marihuana Tax Act of 1937 2016b). Federal authorities did not take long to put the Marihuana Tax Act into effect. On October 1, 1937, they arrested two men in Denver, Colorado, for possession (Moses Baca) and sale (Samuel Caldwell) of marijuana. Judge Foster Symes sentenced Baca to 18 months in jail and Caldwell to four years at hard labor and a $1,000 fine (Uncle Mike 2008).
Assessing the effectiveness of the 1937 legislation is difficult, of course, because marijuana has been, for all practical purposes, illegal since passage of the act. However, substantial evidence is available from arrests for marijuana-related crimes and other sources to suggest that the act was somewhat less than totally successful. A 1998 study found, for example, that the percentage of individuals surveyed who reached the age of 21 in the decades following 1937 and who first used marijuana increased from 0 percent in the 1940s to 2 percent in the 1950s to 6 percent in the 1961–1966 period to 21 percent in the 1967–1971 period to 40 percent in the 1972–1976 period (Johnson and Gerstein 1998, 29, Table 2). Official government statistics available since 1965 also suggest similar trends, with a gradual increase in the number of marijuana users from that year to a peak in the late 1970s, falling off then to a fluctuating but relatively constant level from that point to the present day (Initiation of Marijuana Use: Trends, Patterns, and Implications 2002, Table 3.3, page 30).
The first federal law designed to outlaw the consumption of a psychoactive substance entirely was the Eighteenth Amendment ban on alcohol, certified in 1919 and discussed earlier in this chapter. Similar laws against other psychoactive substances had been enacted much earlier, however, by individual states and municipalities. Probably the first of these laws was the prohibition on the smoking of opium in opium dens, adopted by the city of San Francisco in 1875. That law was very limited, designed to deal almost entirely with Chinese immigrants who brought the habit of opium smoking with them when they immigrated to the United States. All other uses of opium were excluded from the law, and the substance was still widely used by the non-Chinese population for medical and recreational purposes (Gieringer 2000). (Hawaii had passed a similar law in 1856, but had not yet been admitted to the Union as a state [Forbes 1998–2003, 169, #2163].) A number of other California cities, including Oakland, Sacramento, Stockton, and Virginia City, soon followed San Francisco’s example. In 1881, the state legislature enacted a similar law applying to all parts of the state (Gieringer 2000).
The first laws prohibiting the consumption of marijuana were enacted in the Rocky Mountain and Southwestern states toward the end of World War I. At the time, a number of Mexicans were fleeing the Mexican Revolution of 1910–1920 and entering the United States. Many of them brought with them the habit of smoking marijuana, a practice largely unknown in the United States at the time. As with the San Francisco law, laws prohibiting the consumption of marijuana usually reflected the dislike and disapproval of foreigners as much as it did opposition to the use of psychoactive substances. Somewhat ironically, however, the first law banning the use of marijuana had a somewhat different motivation. By the mid-1910s, a number of Mormon missionaries returning from assignments to Mexico brought with them the practice of smoking marijuana, a practice that was quickly condemned by the church as opposed to doctrine (as was and is the use of all other kinds of psychoactive substances). In August 1915, the synod of the Mormon church banned the use of marijuana among all church members, and two months later, the Utah state legislature passed similar legislation, as was commonly the case with other church prohibitions at the time in the state (Whitebread 1995).
In the 20 years following adoption of the Utah law, a total of 27 states passed similar legislation, banning the use of marijuana. Although most of those states were west of the Mississippi, some were located in the Northeast, where there were few or no Mexicans. In these states, the justification for the laws was that individuals who had become dependent on alcohol, cocaine, and opiates and who were now deprived of those drugs because of the Eighteenth Amendment and the Harrison Act were likely to turn to marijuana as their new “drug of choice” (Whitebread 1955).
Thus, as has often been the case with the American federalist system for much of the nation’s history, individual states made their own decisions as to how they would deal with psychoactive substances, whether they would ban them outright, and, if so, which substances would be prohibited. The federal government itself took a number of piecemeal actions, many (as noted previously) that fell short of outright bans on substances. During the mid-twentieth century, some of the legislation that was adopted to deal with the nation’s substance abuse problem were the following:
For almost a century, state, local, and federal legislators have been concerned about a substance abuse problem in the United States that seems not to have been amenable to control by prevention and treatment, educational programs, or punitive legislation. Since the adoption of the Controlled Substances Act in 1970, the U.S. Congress has continued to pass law after law, attempting to deal with this issue. State and local legislative bodies have generally followed suit, often acting even more aggressively than the federal government.
On one front, the U.S. Congress has continued to pass laws increasing penalties for substance abuse and expanding the scope of such laws. In 1984, for example, the U.S. Congress changed its views on the effectiveness of harsh penalties for the control of substance abuse, reversing the stand its predecessors had taken in the CDAPCA of 1970. In the federal Sentencing Reform Act of 1984, it ordered the Federal Sentencing Reform Committee to establish new minimum mandatory sentences for convictions for various types of substance abuse. It also established new mandatory minimum sentences for drug offenses committed near schools, mandated prison sentences for serious drug felonies, and created probationary penalties for less serious offenses (Simplification Draft Paper 2016). Two years later, Congress followed up on its new, harder line against substance abuse convictions by establishing new sentences for cocaine possession. Continuing a historical trend that singles out minorities in legislation of this kind, the Anti-Drug Abuse Act of 1986 provided for a mandatory minimum sentence of 5 to 40 years for cocaine possession, a sentence that could not be suspended nor was it subject to parole. The inequity in the law was based on the fact that the mandatory minimum sentence was required for possession of 500 grams of powder cocaine (by far the drug of choice among middle- and upper-class whites), or 5 grams of crack cocaine (much more popular among blacks and lower-income men and women) (Vagins and McCurdy 2006). Two years later, Congress extended this policy in the Omnibus Drug Abuse Act of 1988 by imposing a five-year mandatory sentence for possession of 3 grams of crack cocaine for second-time offenders and for possession of 1 gram of crack cocaine for third-time offenders (Stolz 1992).
While Congress has apparently remained convinced of the effectiveness of strong penalties against substance abuse, it has also had to deal with a change in the nature of that problem, specifically with the expansion of the number of chemicals similar in chemical structure and psychoactive properties to cocaine, heroin, and other traditional drugs of abuse, now available to the general public. These chemicals are often called designer drugs.
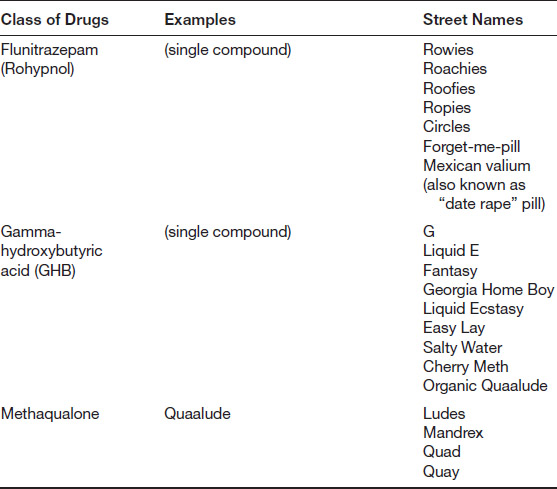
The term designer drugs has at least two meanings. First, it is used to describe new kinds of medications being developed for the treatment of a variety of specific diseases. The field of study out of which such drugs develop is called pharmacogenomics, a combination of two terms referring to the study of drugs (pharmacy) and the study of genetics (genomics). Second, the term designer drugs is used to refer to a number of synthetic chemicals that are derivatives of legal drugs developed for use in recreational settings. Chemists (usually amateur chemists) who synthesize designer drugs usually do so primarily for the purpose of avoiding legal restrictions on the production and sale of compounds that have been declared illegal by the U.S. government. Such compounds have generally been classified by the government as Schedule I or Schedule II drugs, that is, drugs that have high potential for abuse, that have some or no currently accepted medical use in treatment in the United States, and that lack any accepted safety for use under medical supervision. Table 2.3 outlines the major classes of designer drugs that have been developed over the past few decades.
The federal government first became interested in controlling the production and use of designer drugs used for recreational purposes in the early 1980s when it became apparent that existing legislation was ineffective against the many new psychoactive compounds being produced by amateur chemists. In order to deal with this issue, Congress included a provision in the Comprehensive Crime Control Act of 1984 that allowed the administrator of the Drug Enforcement Administration (DEA) to place analogs of banned substances on Schedule I or Schedule II for a period of up to one year, with a six-month extension if necessary. The law was somewhat unusual in that no evidence of a compound’s properties or possible risks was needed for such an action; the administrator’s concerns about a substance were sufficient for listing. Two years later, Congress moved to make its ban on analogs even broader and more comprehensive in the Controlled Substances Analogue Enforcement Act of 1986. It provided, first of all, that:
A controlled substance analogue shall, to the extent intended for human consumption, be treated, for the purposes of any Federal law as a controlled substance in schedule I. (Part B—Authority to Control; Standards and Schedules 2016)
It then defined a “controlled substance analog” as any substance as:
As with other illegal substances, designer drugs have been the subject of a number of other pieces of legislation since the mid-1980s. Most of these acts deal with specific substances, such as methamphetamine (Comprehensive Methamphetamine Control Act of 1996, Children’s Health Act of 2000, and Combat Methamphetamine Epidemic Act of 2005) and MDMA (ecstasy; Illicit Drug Anti-Proliferation Act of 2003).
Since the mid-1980s, the U.S. Congress has also begun to focus on other aspects of the nation’s substance abuse problem. In many cases, it has given more serious attention to other approaches to solving this problem, such as the educational, prevention, and treatment approaches discussed previously. One of the most famous of these efforts was the Just Say No program espoused during the administration of President Ronald Reagan by his wife, Nancy Reagan. After her husband’s election to the presidency in 1981, Nancy Reagan announced that her primary field of interest was going to be substance abuse. She began visiting schools around the nation with the goal of educating young people about the risks associated with using illegal drugs. At one of these visits, to the Longfellow Elementary School in Oakland, California, in 1982, she was asked by a student what she should do if she were offered drugs. Mrs. Reagan’s reply was that she should “just say no.” That brief comment soon became the theme of a nationwide campaign to encourage young people to refuse to become involved in substance abuse. In some ways reflecting the efforts of early temperance workers, Mrs. Reagan and her associates visited dozens of schools across the country, encouraging students to sign agreements not to become involved with drugs. She also appeared on many television appearances; enlisted the help of the Girl Scouts of America, the Kiwanis Club, and other service organizations; and sponsored an international conference of 30 first ladies from around the world to support her efforts (First Lady Biography: Nancy Reagan 2016). Although for many years the best-known educational program on substance abuse, this campaign was hardly the only or even necessarily the most successful of its kind (McGrath 2016).
The U.S. Congress and many state legislatures also recognized the potential value of educating young people about the dangers of substance abuse and began to commit tax dollars to such programs. In 1998, for example, the U.S. Congress passed and President Bill Clinton signed the National Youth AntiDrug Media Campaign Act. The purpose of this act was to “conduct a national media campaign in accordance with this subtitle for the purpose of reducing and preventing drug abuse among young people in the United States” (Public Law 105-277 1998, Sec. 102[A]). The Office of National Drug Control Policy, responsible for implementation of the act, was enthusiastic about its potential for reducing substance abuse among young adults (The National Youth Anti-drug Media Campaign Communication Strategy Statement [1998]), and the federal government eventually invested more than $1 billion in the program by 2003 (Eddy 2003, CRS-5). A number of studies found, however, that the program had little or no effect on substance abuse among young Americans, and the program was gradually phased out (only to be replaced by a somewhat similar program called Above the Influence; see Hornik 2008; Ingraham 2016.)
A relatively recent trend in federal drug legislation has been the focus on specific psychoactive substances or specific aspects of the campaign against drug abuse, dependence, and addiction. One of the earliest examples of this type of legislation was the Comprehensive Methamphetamine Control Act of 1996 (CMCA). That act was passed in response to what experts in substance abuse regarded as a “meth epidemic” of unparalleled magnitude in the United States at the time. One article in The North Dakota Law Review began with the somewhat sensationalistic claim that “an epidemic of methamphetamine abuse and addiction has swept across our nation and the world. Its wake has destroyed families, devastated communities, caused property crimes to surge, and caused severe neglect of children” (Bovett 2007). Although arguably a bit extreme in light of the evidence, this view was reflected in a number of similar claims by law enforcement officials, substance abuse experts, state and federal legislators, and members of the general public (Quotes about Methamphetamine 2016).
The CMCA attempted to deal with the meth epidemic from a number of angles: It made access to the raw materials used in producing methamphetamine more difficult and more expensive to obtain; it instituted rules for the preparation and transfer of such chemicals; and it increased penalties for all aspects of the illegal production of methamphetamine (Prah 2005). It also created a Methamphetamine Interagency Task Force to monitor progress of the new legislation and develop suggestions for further actions against meth abuse. One consequence of the task force’s research was the introduction of another anti-meth bill in 2000, which became the Methamphetamine Anti Proliferation Act of 2000, followed five years later by yet another piece of legislation, the Combat Methamphetamine Epidemic Act of 2005. The best available evidence suggests that meth use remained relatively constant between 2002 and 2014 among individuals between the ages of 12 and 17 and older than 26, at about 0.2 percent of the general population throughout that period, while usage rates among those between the ages of 18 and 25 dropped significantly, from 0.6 percent in 2002 to 0.2 percent in 2014 (Hedden et al. 2015, Figure 10 Table, page 9). The 106th Congress (1999–2001) also considered a number of other bills focusing on specific substances, such as the Ecstasy Anti-Proliferation Act and the Club Drug Anti-Proliferation Act, neither of which was passed in its original form, but which were absorbed into other related bills.
A particularly striking bill of special significance, the Family Smoking Prevention and Tobacco Control Act was passed in 2009. The act provided for the first time specific authority of the FDA to treat tobacco and cigarettes as a substance with health risks worthy of governmental regulation. The act imposed new label and warning standards for tobacco products, banned flavored cigarettes, placed limits on advertising of tobacco products to young people, and required tobacco companies to obtain specific approval for the introduction of new products to the marketplace (Tobacco Control Act 2016).
The most recent focus of congressional discussions has been the nation’s prescription drug abuse epidemic and related opioid abuse issues. A number of bills were introduced into the 114th Congress (2015–2017) calling for additional federal funding for research on prescription drug abuse and opioid addiction, improved programs of education for young adults about the dangers of prescription drugs, action on specific psychoactive substances (such as DMX), control and disposal of prescribed drugs, and guarantees for patients who need opioids for the treatment of pain (for examples of such bills, see Prescription Drugs 2016). As is generally the case with federal legislation, only a small handful of these bills ever received consideration by Congress as a whole. However, in an action that surprised many observers Congress passed a wide-ranging bill, the Comprehensive Addiction and Recovery Act, which was signed by President Obama on July 22, 2016. The bill provided for increased prevention, treatment, recovery, law enforcement, criminal justice reform, and overdose reversal programs and was widely hailed as “the most comprehensive effort undertaken to address the opioid epidemic” (Comprehensive Addiction and Recovery Act 2016).
The premise underlying most of this chapter has been that the consumption of certain substances is potentially harmful and dangerous for the individuals who use them. Certainly the federal government and both state and local governments appear to have taken this stance over most of the last century. And yet, a number of individuals and organizations have long taken the position that governments should not be involved in legislating the psychoactive substances individuals choose to consume for recreational purposes. Since the 1960s, there has been an ongoing debate as to whether these substances should be made legal or not. The debate has been a somewhat unusual one, with liberal Democrats and conservative Republicans—and individuals at every point between these extremes—agreeing with each other on either one or the other position.
One of the fundamental issues involved in this debate involves the decriminalization versus legalization of drugs. Although the two terms are sometimes used synonymously, they actually have very different meanings. Decriminalization refers to the removal of all jail and prison sentences for possession or use of an illegal drug. A person may still receive a fine for such an action, but it is unlikely to appear on any permanent legal record or result in confinement. In this regard, drug decriminalization is similar to traffic fines or other misdemeanors that are regarded as relatively minor legal violations (The Difference between Legalisation and Decriminalization 2014). By contrast, legalization refers to the removal of all prohibitions on possession or use of an illegal drug, within certain specific boundaries. For example, in a state where the use of illegal drugs has been decriminalized, a person might be fined $100 for having 10 grams of marijuana in his or her possession; in a state where drug use has been legalized, there would be no penalty of any kind for the possession and use of such a small amount of the drug (although larger quantities would still be subject to penalties, some quite severe).
As of late 2016, 19 states and the District of Columbia have decriminalized the possession and use of marijuana, the only drug for which such action has been taken in the United States. An example of the terms of decriminalization is the Mississippi law, in which possession of 30 grams of marijuana or less results in a fine of $250. A second conviction for the same offense results in another $250 and, for a third conviction, a fine of $500. By contrast, possession of 500 grams to 1 kilogram of marijuana results in a fine of $250,000 and a prison term of 4 to 16 years (Mississippi Laws & Penalties 2016).
The debate over decriminalization and/or legalization of drugs is based almost entirely today on a single currently illegal substance, marijuana. But arguments in favor of decriminalizing or legalizing other substances have long been, and are still being, made. Some of those arguments are as follows:
One of the fundamental principles of a democratic state is that people should be allowed to do with their own bodies whatever they want, provided they do no harm to other individuals. Having a marijuana cigarette or a Quaalude pill on a Saturday night may provide pleasure to the person who uses these substances without harming anyone else. As one blogger puts this argument:
The war on drugs is more of a war on personal choice, a war on your right to decide how you live your life. If someone wants to ingest something; put it into their own body, their own property, and they aren’t harming any other human being, animal or property, then where is the harm in that? How is the state justified in telling me that I cannot consume a natural substance? As long as your personal choice doesn’t infringe on the freedom of others, then people should be allowed to be live and act freely. (Caufield 2013)
In 1971, the year that President Richard M. Nixon first declared a “war on drugs,” the federal budget to carry on that war was about $350 million annually ($2.14 billion in 2016 dollars). Five years later, that budget had increased nearly tenfold, reaching $760 million (Goldberg 1980). Those costs continued to rise over the next four decades, reaching a total federal expenditure in 2016 of $30.6 billion (National Drug Control Budget 2016, 2). And these numbers reflect only federal spending. The cost of fighting drug abuse on state and local levels adds substantially to these totals. According to one study conducted in 2010, states and local municipalities had spent $25,684,407,000 in 2008 on drug enforcement programs, almost twice the total spent by the federal government ($13.7 billion) for that year (Miron and Waldock 2010, Table 3, page 35; National Drug Control Strategy 2008).
A number of studies conducted since 1982 suggest that many (but certainly not all) efforts to reduce substance abuse by legal means have been a failure. Some examples of those findings have been cited earlier in this chapter. In 1996, a committee of the New York Country Lawyers Association, the oldest bar association in New York City, issued a report on state and federal drug policy. It concluded that “[n]otwithstanding the vast public resources expended on the enforcement of penal statutes against users and distributors of controlled substances, contemporary drug policy appears to have failed, even on its own terms, in a number of notable respects.” It went on to suggest that that drug policy may actually have had more damaging effects on society as a whole than have the harmful effects of psychoactive substances and their abusers (Fischler et al. 1996).
That situation appears to continue today. A recent policy statement investigating the efficacy of federal “drug war” programs noted that
despite the incarceration of tens of millions of Americans and more than a trillion dollars of spending, illegal drugs remain cheap, potent, and widely available. The harms associated with them—addiction, overdose and the spread of HIV/AIDS and hepatitis B and C—continue to persist in every community. Meanwhile the war on drugs is creating problems of its own—broken families, increased poverty, racial disparities, wasted tax dollars, prison overcrowding and eroded civil liberties. (An Exit Strategy for the Failed War on Drugs 2013)
Legal prohibitions on drugs have spawned the growth of a huge crime network and provide a significant financial asset for terrorist groups. Since cocaine, heroin, marijuana, and other recreational drugs are illegal, they can be obtained only through black markets. These black markets have become an important element of organized crime in almost every country of the world. Drug organizations maintain control over their operations by means of well-organized and efficient crime groups that involve distributors and enforcers. In addition, substance abusers themselves often turn to crime to earn the dollars they need to maintain their illegal habit. If the government controlled the distribution of substances that are now illegal, the primary motivation for drug cartels would disappear, and drug-related crime rates would decrease dramatically.
In addition, profits made from the sale of illegal substances such as cocaine, heroin, and marijuana are a major source of income for terrorist groups, many of whom control the source of production for such drugs. One report on this issue concluded that “[r]efusing to address the role of prohibition [of drugs] in financing terrorism will enable terrorist groups to continue to build the resources they need to engage in even more extensive acts of terrorism than we have witnessed to date” (Oscapella 2003, 2).
Proponents of the decriminalization of illegal substances also raise a number of other points in defending their position, such as the fact that many legal substances, such as alcohol and tobacco, are far more destructive than most illegal drugs; that some illegal substances have important practical applications in research, medicine, religion, and other fields; that some substance abusers become involved with drugs simply because they are illegal and they are attracted by the adventure of becoming involved in an illegal activity; that U.S. policies on illegal substances have proved to be disastrous for domestic policies in nations where these drugs are produced (such as Afghanistan, Colombia, Bolivia, and Mexico); and that governments should treat psychoactive substances consistently, not granting approval to some (such as tobacco and alcohol) and heavily penalizing others (such as marijuana and cocaine). (For an excellent overall review of the pro-legalization argument, see Cussen and Block 2000.)
In spite of these arguments, the thought of decriminalizing or legalizing drugs is still anathema to many people. Some of the arguments for maintaining current prohibitions on illegal substances are the following:
Hardly anyone who has studied the health effects of drugs like cocaine, heroin, LSD, and MDMA would argue with the contention that the use of such drugs can have devastating short- and long-term effects on a person’s health. The argument is less clear for other drugs, marijuana perhaps being the best example. In any case, the proponents of retaining prohibitions on Schedule I and Schedule II drugs often point to mortality and morbidity statistics for these drugs. The most recent data available for mortality in the United States found that 46,471 people died in 2013 from drug-induced causes (both legal and illegal). This number represented a 5.8 percent increase over the previous year and 143 percent over the death rate for 1999 (Xu et al. 2016, 10–11 and Supplemental Tables, Table 1–3, page 6).
Numerous studies about the health effects of individual psychoactive substances have been conducted over the years. A general overview of this situation is provided on an annual basis in SAMHSA’s Substance Abuse Treatment Episode Data Set study. According to the most recent data available, the substance responsible for the greatest number of emergency department (ED) admissions for drug-related issues is alcohol, accounting for 368,007 instances out of a total of 1,739,523 total drug-related admissions in that year, or 21.2 percent of all such admissions. Admissions involving alcohol with another drug accounted for an additional 280,935 admissions (16.2%). The next most common drugs responsible for ED admissions were heroin (334,163 admissions; 19.2%), marijuana (289,379 admissions; 16.6%), other opiates (161,332 admissions; 9.3%), amphetamines (140,334 admissions; 8.1%), and cocaine (all forms; 105,474 admissions; 6.1%). (A good review of the many health and medical consequences related to substance abuse is available at Medical Consequences of Drug Abuse 2012.)
This argument is similar to the one presented earlier in support of decriminalization of drugs in that it recognizes the close relationship between substance abuse and many kinds of crimes. Instead of arguing that legalizing drugs will reduce this problem, however, proponents of drug prohibition say that strong penalties are needed to keep a rein on crime arising out of drug abuse. The DEA claims that legalizing drugs would not eliminate the crimes associated with substance abuse because individuals under some age, such as 18 or 21, would still not be allowed to purchase or use certain substances, and that portion of the population is currently and has long been a major consumer of illegal substances. Therefore, a black market for the drugs would still exist, retaining most of the violent crimes now associated with illegal drug use.
Those in favor of retaining strict penalties for the use of marijuana, cocaine, heroin, and other drugs argue that illegal drug use has decreased substantially as a result of stiff drug laws. The DEA reports that illegal drug use has dropped by a third in the last 20 years, and the use of cocaine by 70 percent during that time. The agency claims that “[s]ignificant progress has been made in fighting drug use and drug trafficking in America.” It argues that efforts to legalize drugs as being the only workable alternative to the war on drugs are wrong and that “the facts are contrary to such pessimism” (Speaking Out against Drug Legalization [2010], 13).
Individuals who have argued against the decriminalization of drugs frequently point to previous efforts in this direction, which, they say, have always failed. These commentators tend to use a common set of facts to support their view, such as the claim that decriminalization of marijuana in California in 1976 led to an increase in arrests for driving under the influence of drugs in the state by 46 percent for adults and 71 percent for juveniles. They also point to decriminalization of marijuana by the states of Alaska and Oregon in the 1970s that resulted in a doubling of the use of the substance (see, for example, Maginnis 2016).
Opponents of decriminalization resort to a number of other arguments to support their position. Perhaps the best single source for these arguments is a booklet published by the DEA in May 2003 and revised in 2010, Speaking Out against Drug Legalization. In addition to the points made previously, this booklet suggests that the war against drugs requires a balanced approach that includes both prevention and treatment, but also requires laws prohibiting their use; that the drug war, although expensive, is only a minor part of the overall federal budget, which represents an important element in dealing with an important national social issue; that alcohol abuse has already caused the nation severe social and health problems, and that the legalization of drugs will only make that situation worse; and that, in any case, most people convicted of substance abuse do not go to prison but, instead, are referred to treatment programs (Speaking Out against Drug Legalization [2010]).
Within the general realm of substance abuse issues, one topic is currently of special interest: the legal use of marijuana. A movement appears to be developing throughout the nation that calls for the legalization of the use of marijuana, either for medical purposes only or for medical and recreational uses.
Arguments over the legalization or prohibition of marijuana use are generally similar to those for other drugs, outlined in the preceding section. But proponents of legalization also point out that marijuana is probably the least dangerous of all substances listed under Schedule I of the Controlled Substances Act. If used in moderation, it almost certainly has fewer health effects than alcohol and tobacco, both of which are legal in the United States. It is also the least likely of all major drugs (tobacco, alcohol, cocaine, and opiates) to lead to addiction. In its 1999 exhaustive study, Marijuana and Medicine: The Scientific Base, the last major study on the subject, the Institute of Medicine found that about 9 percent of all individuals who had tried marijuana eventually became dependent on the drug, compared to 32 percent who became addicted to tobacco, 23 percent to heroin, 17 percent to cocaine, 15 percent to alcohol, and 9 percent to hypnotics and sedatives (Joy, Watson, and Benson 1999, 95).
Opponents of the decriminalization of marijuana often point to the possible role of the substance as a “gateway” drug. A gateway drug is a substance that, when used, leads to an increased risk of the use of other illegal substances. That is, some individuals say that a person who uses marijuana is more likely then to move on to cocaine, heroin, or other more serious drugs. For many years, the DEA has been using some form of this argument in its literature opposing the decriminalization and/or legalization of marijuana. At one point, for example, it cited a study conducted at Columbia University that “children (12 to 17 years old) who use gateway drugs—tobacco, alcohol and marijuana—are up to 266 times—and adults who use such drugs are up to 323 times—more likely to use cocaine than those who don’t use any gateway drugs” (National Study Shows “Gateway” Drugs Lead to Cocaine Use 1994; Publications 1994). Over time, the DEA cut back on the magnitude of this gateway effect (Tandy 2005), but has continued to mention it as a major reason to continue listing marijuana as a Schedule I drug (Brosious 2016).
Other authorities hold different views about the role of marijuana as a gateway drug. In its 1999 study cited previously, the Institute of Medicine concluded on this subject that “marijuana is not the most common, and is rarely the first, ‘gateway’ to illicit drug use. There is no conclusive evidence that the drug effects of marijuana are causally linked to the subsequent abuse of other illicit drugs” (Joy, Watson, and Benson 1999, 6; for further research on this question, see also Gateway Theory 2016).
One of the issues of greatest concern about marijuana at the present time is its use for medical purposes. Evidence suggests that marijuana has been used for medicinal purposes for over 2,000 years. Some of the earliest mentions of these substances for medical uses occur in Chinese herbal and medical works dating to the first century CE, if not earlier (Abel 1980). In recent years, a number of medical benefits have been claimed for these substances.
One common way of categorizing these benefits is by the confidence in which medical experts have for each effect. One such scheme classifies the medical claims for marijuana into four major categories: established effects, relatively well-confirmed effects, less confirmed effects, and basic research stage. The disorders included in each of these categories are as follows:
These claims have been sufficiently convincing, at least to some state legislators and parts of the general public that, as of 2016, 25 states and the District of Columbia have passed laws permitting the growing and sale of marijuana for medicinal purposes. The first state to pass such a law was California in 1996, later followed by Alaska (1998), Oregon (1998), Washington (1998), Maine (1999), Colorado (2000), Hawaii (2000), Nevada (2000), Montana (2004), Vermont (2004), New Mexico (2007), Rhode Island (2006), Michigan (2008), Arizona (2010), New Jersey (2010), Delaware (2011), Connecticut (2012), Massachusetts (2012), Illinois (2013), New Hampshire (2013), Maryland (2014), Minnesota (2014), New York (2014), Guam (2014), Ohio (2016), and Pennsylvania (2016) (State Medical Marijuana Laws 2016; this site is a good source for changes in and the current status of state medical marijuana laws).
There remains strong opposition to the use of marijuana, even for medical purposes. Probably the most common objection is that the substance is still listed as a Schedule I drug by the U.S. government under the provisions of the Controlled Substances Act of 1970. That means that a person in California or Maine or New Mexico (or any other state that has approved the use of medical marijuana) may be able to purchase and use the drug in his or her own state, but will still be breaking federal law in doing so. As recently as November 2015, President Barack Obama’s choice as the new chief of the DEA said that calling smoked marijuana a medicine was “a joke.” “What really bothers me,” he said, “is the notion that marijuana is also medicinal—because it’s not. We can have an intellectually honest debate about whether we should legalize something that is bad and dangerous, but don’t call it medicine—that is a joke” (Reid and Condon 2015).
Federal law enforcement officials have, of course, carried out DEA policy on the use of medical marijuana. During the administration of George W. Bush, for example, law enforcement officials raided marijuana dispensaries licensed to sell marijuana to individuals with a prescription and arrested individuals who grow marijuana for such dispensaries (see, for example, DEA’s War on California 2002). Bush’s first “drug czar,” John Walters, frequently made clear his views on medical marijuana. Not only was marijuana an invalid tool for treating any medical condition, according to Walters, but, in fact, the push for marijuana dispensaries was really a tool for obtaining complete legalization for the substance. During one television interview, for example, he said, “In California, where medical marijuana has been used as a kind of a wedge issue, or kind of phony effort to try to say, ‘It’s only going to go to people who are sick.’ It’s not going to people who are sick. In fact, in San Francisco it has been reported in the news there are now more marijuana dispensaries than there are Starbucks in downtown San Francisco” (Anderson Cooper 360 Degrees 2009).
The administration of President Barack Obama, who took office in January 2009, has had a somewhat different—and somewhat inconsistent—view of this controversy. In October 2009, Attorney General Eric H. Holder, Jr., announced that the federal government would initiate a more lenient view with regard to individuals who distribute or use marijuana for medical purposes. “It will not be a priority to use federal resources to prosecute patients with serious illnesses or their caregivers who are complying with state laws on medical marijuana,” Holder said, in a policy statement that represented a 180-degree change from that of the administrations of Presidents Bill Clinton and George W. Bush (Stout and Moore 2009). In confirming this new direction, Deputy Attorney General David W. Ogden sent out a memorandum to federal prosecutors in states with medical marijuana laws. That memorandum emphasized that the administration still held to the position that marijuana is “a dangerous drug, and the illegal distribution and sale of marijuana is a serious crime,” which it intended to prosecute. On the other hand, the memo went on, the Department of Justice had limited resources, and it had to prioritize the crimes it chose to pursue. In general, therefore, investigators were directed to concentrate on marijuana-related crimes that met certain criteria, namely, those that involved the following:
Most observers viewed the Ogden memo as a signal that federal agents would largely keep hands off legitimate use of medical marijuana in states where such use had been approved. Two years later, however, the Obama administration felt it necessary to issue a second memorandum clarifying (or, some say, reversing) its position on the issue. That memo, the so-called Cole Memorandum of 2011 (or Cole 2011), pointed out that the Ogden memo was not meant to imply that the federal government was simply going to turn its back on marijuana prosecutions. It was, Cole 2011 went on, “never intended to shield such activities from federal enforcement action and prosecution, even where those activities purport to comply with state law” (Memorandum for United States Attorneys 2011). The gates appeared to be open to more aggressive attacks by federal agents on state medical marijuana facilities, which shortly appeared to be the case as the number of such raids soon began to increase (Riggs 2011).
Fast forward two more years, and the situation appeared to change one more time. In a second memorandum by Deputy Attorney General James M. Cole (Cole 2013), the administration repeats the apparent message of the Ogden memo, namely, that the Department of Justice has decided to focus its limited resources on only certain types of marijuana-related activities, roughly corresponding with the list provided earlier (Memorandum for All United States Attorneys 2013). This most recent memo, then, appears to indicate that the Obama administration has decided essentially to ignore activities related to the use of marijuana for medical purposes in states where such use has been approved. (For a detailed background on the history of this issue, see Grim and Reilly 2013.)
Progress toward the legalization of marijuana for recreational use has occurred more slowly than it has for medical marijuana. The earliest steps in that direction took place in the 1970s when a handful of states decriminalized the use of marijuana for recreational purposes. The first such action, the Oregon Decriminalization Bill of 1973, made possession of one ounce of marijuana a violation (not a crime) punishable by a fine of $500 to $1,000 (Blachly 1976). Over the next four years, ten more states—Alaska, California, Colorado, Maine, Minnesota, Mississippi, Nebraska, New York, North Carolina, and Ohio—followed Oregon’s lead in decriminalizing the use of recreational marijuana (Scott 2010).
It took nearly 40 years, however, to take the next step: outright legalization of marijuana. Then, in the general elections of November 2012, two states, Colorado and Washington, adopted legislation legalizing the recreational use of up to one ounce of marijuana. On November 4, 2014, two more states (Alaska and Oregon) and the District of Columbia also voted to legalize the use of small amounts of marijuana for recreational purposes. The precise wording of laws in each of the four states and the District varies to some extent (State Laws 2016).
The legalization of recreational marijuana in four states has permitted the conduct of a “grand experiment” about certain long-standing and fundamental questions regarding marijuana consumption, such as the following:
None of these questions is easy to answer, and, as of early 2017, it is still too early to know what those answers might be. Nonetheless, officials in all four states are aware of the importance of such questions and the need to collect data about them. In Colorado, for example, the state legislature adopted legislation in 2013 requiring the state Division of Criminal Justice and the Department of Public Safety to collect data and prepare a report on the effects of marijuana legalization in a variety of fields. The following data are summarized from a report released in March 2016 pursuant to that charge. Among the trends noted in the report are the following (all data from Reed 2016, 5–9):
Other states have prepared reports similar to Colorado’s (see Dilley 2016; Monitoring Impacts of Recreational Marijuana Legalization: 2015 Baseline Report 2015), with results roughly similar to those from Colorado. Stronger statements about the effects on society of legalization marijuana, however, await the passage of time and more detailed studies of the issue.
As can be expected in the progress of any important social issue, the adoption of new laws or decisions by courts do not necessarily mark the end of the dispute over such issues (see, for example, the debates over abortion and same-sex marriage in the United States). Such has also been the case with the legalization of marijuana in Colorado, Washington, Alaska, Oregon, and the District of Columbia. The adoption of legislation permitting the use of marijuana for recreational purposes in these entities has not meant that opponents of legalization have ended their battle against the practice. In one instance, for example, residents of Pueblo County filed a lawsuit against the state because an adjacent crop of marijuana plants allegedly blocked their view. In another suit, a Holiday Inn hotel in Frisco, Colorado, filed a RICO (Racketeer Influenced and Corrupt Organizations Act) suit against the state because, it claimed, a marijuana dispensary scheduled to open next to the property would interfere with its normal business activities. In yet a third case, a group of sheriffs and other law enforcement officials from Colorado, Kansas, and Nebraska sued the state, claiming that the legalization of marijuana violated state law, the Colorado constitution, and the U.S. Constitution. Plaintiffs lost in all three of these cases (Warner 2016).
The case that perhaps drew the greatest attention nationally was Nebraska and Oklahoma v. Colorado (U.S. Supreme Court docket #220144), in which Nebraska and Oklahoma sued Colorado. The two states argued that the legalization of marijuana in Colorado was likely to result in an increase in drug-related crimes in their own states and that the new Colorado law was, therefore, unconstitutional. In March 2016, the Supreme Court declined to hear the case, essentially bringing to an end this type of complaint about the new Colorado marijuana law (Nebraska and Oklahoma v. Colorado 2016). While the legal history of challenges to marijuana law has universally failed thus far, it is still early days in the history of marijuana legalization, and additional challenges in other states on a variety of issues are to be expected. (See, for example, Mapes 2015.)
Abel, Ernest L. 1980. Marihuana, the First Twelve Thousand Years. New York: Plenum Press.
“Above the Influence.” 2016. http://abovetheinfluence.com/about/. Accessed on June 26, 2016.
“An Exit Strategy for the Failed War on Drugs.” 2013. Drug Policy Alliance. https://www.drugpolicy.org/sites/default/files/DPA_Exit%20Strategy_Federal%20Legislative%20Guide.pdf. Accessed on June 27, 2016.
Anderson, Jordan. 2012. “This House Supports Random Drug-Testing in Schools.” idebate.org. http://idebate.org/debatabase/debates/culture/children/house-supports-random-drug-testing-schools. Accessed on June 23, 2016.
“Anderson Cooper 360 Degrees.” 2009. CNN. http://transcripts.cnn.com/TRANSCRIPTS/0905/06/acd.02.html. Accessed on June 29, 2016.
“Are Recovery High School Really Working?” 2016. Recovery.org. http://www.recovery.org/are-recovery-high-schools-working/. Accessed on June 30, 2016.
Bielawski, Michael. 2015. “Marijuana Legalization Could Rewrite Employee Drug-Testing Rules.” VermontWatchdog.org. http://watchdog.org/256084/drug-testing-vermont-marijuana-legalization/. Accessed on June 22, 2016.
Blachly, Paul H. 1976. “Effects of Decriminalization of Marijuana in Oregon.” Annals of the New York Academy of Sciences. 282(1): 405–415.
Board of Education of Independent School District No. 92 of Pottawatomie County v. Earls. 2002. U.S. Supreme Court. http://www.supremecourt.gov/opinions/boundvolumes/536bv.pdf. Accessed on June 23, 2016.
Bonnie, Richard J., and Charles H. Whitebread. 1974. The Marihuana Conviction. Charlottesville: University of Virginia Press.
Bovett, Rob. 2007. “Meth Epidemic Solutions.” North Dakota Law Review. 82(4): 1195–1216.
Brecher, Edward M., and the editors of Consumer Reports Magazine. 1972. The Consumers Union Report on Licit and Illicit Drugs. Boston: Little, Brown and Company. http://www.druglibrary.org/Schaffer/LIBRARY/studies/cu/cumenu.htm. Accessed on June 24, 2016.
Brody, Jane E. 2013. “Effective Addiction Treatment.” The New York Times. http://well.blogs.nytimes.com/2013/02/04/effective-addiction-treatment/?_r=0. Accessed on June 22, 2016.
Brosious, Emily Gray. 2016. “White House Drug Czar Rallies against Marijuana Legalization, Argues ‘Gateway’ Theory.” Sun Times Network. http://extract.suntimes.com/news/10/153/17947/white-house-drug-czar-michael-botticelli-fights-against-marijuana-legalization-claims-gateway-theory. Accessed on June 28, 2016.
Buxton, Julia. 2006. The Political Economy of Narcotics: Production, Consumption and Global Markets. London: Zed Books.
Caufield, M. 2013. “The War on Personal Choice.” Exposing the Truth. https://www.exposingtruth.com/war-personal-choice/. Accessed on June 27, 2016.
Center for Substance Abuse Prevention. 2016. U.S. Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. http://prevention.samhsa.gov/. Accessed on June 21, 2016.
Coats v. Dish. 2015. 2015 CO 44. Colorado Supreme Court. http://extras.mnginteractive.com/live/media/site36/2015/0615/20150615_085459_coats-vs-dish.pdf. Accessed on June 22, 2016.
Comprehensive Addiction and Recovery Act. 2016. CADCA. http://www.cadca.org/comprehensive-addiction-and-recovery-act-cara. Accessed on December 23, 2016.
“Controlled Dangerous Substances Act of 1969.” 1969. Report of the Committee on the Judiciary. United States Senate. Report No. 91–613. 91st Congress, 1st Session. https://bulk.resource.org/gao.gov/91-513/000050F5.pdf. Accessed on June 25, 2016.
“Controlled Substances.” 2016. Drug Enforcement Administration. http://www.deadiversion.usdoj.gov/schedules/orangebook/e_cs_sched.pdf. Accessed on June 25, 2016.
“Controlled Substances Act.” 2009. U.S. Food and Drug Administration. http://www.fda.gov/regulatoryinformation/legislation/ucm148726.htm. Accessed on June 25, 2016.
Courtwright, David T. 1995. “The Rise and Fall of Cocaine in the United States.” In Jordan Goodman, Paul E. Lovejoy, and Andrew Sherratt, eds. Consuming Habits: Drugs in History and Anthropology. London: Routledge.
Cussen, Meaghan, and Walter Block. 2000. “Legalize Drugs Now! An Analysis of the Benefits of Legalized Drugs.” American Journal of Economics and Sociology. 59(3): 525–536.
D.A.R.E. 2016. http://www.dare.org/. Accessed on June 21, 2016.
“DEA’s War on California.” 2002. Americans for Safe Access. http://www.safeaccessnow.org/asanews172. Accessed on June 29, 2016.
DePillis, Lydia. 2015. “Companies Drug Test a Lot Less Than They Used To—Because It Doesn’t Really Work.” The Washington Post. https://www.washingtonpost.com/news/wonk/wp/2015/03/10/companies-drug-test-a-lot-less-than-they-used-to-because-it-doesnt-really-work/. Accessed on June 22, 2016.
“The Difference between Legalisation and Decriminalization.” 2014. The Economist. http://www.economist.com/blogs/economist-explains/2014/06/economist-explains-10. Accessed on June 27, 2016.
Dilley, Julia, et al. 2016. “Marijuana Report: Marijuana Use, Attitudes and Health Effects in Oregon.” Oregon Public Health Division. https://public.health.oregon.gov/PreventionWellness/marijuana/Documents/oha-8509-marijuana-report.pdf. Accessed on June 29, 2016.
Donohoe, Martin. 2005. “Urine Trouble: Practical, Legal, and Ethical Issues Surrounding Mandated Drug Testing of Physicians.” Journal of Clinical Ethics. 16(1): 69–81.
“Drug Courts.” 2016. National Institute of Justice. http://www.nij.gov/topics/courts/drug-courts/pages/welcome.aspx. Accessed on June 30, 2016.
“DrugFacts: Treatment Approaches for Drug Addiction.” 2016. National Institute on Drug Abuse. https://www.drugabuse.gov/publications/drugfacts/treatment-approaches-drug-addiction. Accessed on June 22, 2016.
DuPont, Robert L. 2015. “Workplace Drug Testing in the Era of Legal Marijuana.” Institute for Behavior and Health, Inc. http://www.drugfreebusiness.org/Media/documents/IBH_workplacetesting.pdf. Accessed on June 22, 2016.
“Early History.” 2016. Women’s Christian Temperance Union. http://www.wctu.org/history.html. Accessed on June 24, 2016.
Eddy, Mark. 2003. “War on Drugs: The National Youth Anti-Drug Media Campaign.” CRS Report for Congress. http://www.drugpolicy.org/docUploads/RS21490.pdf. Accessed on June 26, 2016.
Engber, Daniel. 2015. “Why Do Employers Still Routinely Drug Test Workers?” Slate. http://www.slate.com/articles/health_and_science/cover_story/2015/12/workplace_drug_testing_is_widespread_but_ineffective.html. Accessed on June 22, 2016.
“First Lady Biography: Nancy Reagan.” 2016. National First Ladies Library. http://www.firstladies.org/biographies/firstladies.aspx?biography=41. Accessed on June 26, 2016.
Fischler, Alan B., et al. 1996. Report and Recommendations of the Drug Policy Task Force. New York: New York Lawyers’ Association. http://www.drcnet.org/nycla.html. Accessed on June 27, 2016.
Forbes, David W., ed. 1998–2003. Hawaiian National Bibliography, 1780–1900. Honolulu: University of Hawaii Press.
“Gateway Theory.” 2016. DrugWarFacts.org. http://www.drugwarfacts.org/cms/Gateway_Theory#sthash.iIjjF7fZ.dpbs. Accessed on June 29, 2016.
Gfroerer, Joseph C., Wu Li-Tzy, and Michael A. Penne. 2002. “Initiation of Marijuana Use: Trends, Patterns, and Implications.” Office of Applied Statistics. Substance Abuse and Mental Health Services Administration. http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.187.6614&rep=rep1&type=pdf. Accessed on June 24, 2016.
Gieringer, Dale. 2000. “125th Anniversary of the First U.S. Anti-Drug Law: San Francisco’s Opium Den Ordinance (Nov. 15, 1875).” http://www.drugsense.org/dpfca/opiumlaw.html. Accessed on June 25, 2016.
Goldberg, Peter. 1980. “The Facts about Drug Abuse.” The Drug Abuse Council. http://www.druglibrary.org/schaffer/library/studies/fada/fada1.htm. Accessed on June 27, 2016.
Grim, Ryan, and Ryan J. Reilly. 2013. “Obama’s Drug War: After Medical Marijuana Mess, Feds Face Big Decision on Pot.” Huffpost Politics. http://www.huffingtonpost.com/2013/01/26/obamas-drug-war-medical-marijuana_n_2546178.html. Accessed on May 21, 2016.
Hamilton, Alexander. 1904. The Works of Alexander Hamilton (Federal Edition), 12 vols. Edited by Henry Cabot Lodge. New York; London: G. P. Putnam’s. http://oll.libertyfund.org/titles/hamilton-the-works-of-alexander-hamilton-federal-edition-vol-11. Accessed on June 24, 2016.
Hanson, David J. 2009. “National Prohibition of Alcohol in the U.S.” Alcohol Problems and Solutions. http://www.alcoholproblemsandsolutions.org/Controversies/1091124904.html. Accessed on June 24, 2016.
Harrison Narcotics Tax Act, 1914. 1914. Schaffer Library of Drug Policy. http://www.druglibrary.org/schaffer/history/e1910/harrisonact.htm. Accessed on June 24, 2016.
Hedden, Sarra L., et al. 2015. “Behavioral Health Trends in the United States: Results from the 2014 National Survey on Drug Use and Health.” HHS Publication No. SMA 154927, NSDUH Series H50. http://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf. Accessed on June 18, 2016.
“Hemp Facts.” 1997. North American Industrial Hemp Council, Inc. http://www.naihc.org/hemp_information/hemp_facts.html. Accessed on June 24, 2016.
Holland, Ellen. 2015. “Operation Golden Flow: America’s Urine Is Liquid Gold for Drug War Profiteers.” Cannabis Now. http://cannabisnowmagazine.com/current-events/legal/operation-golden-flow-americas-urine-is-liquid-gold-for-drug-war-profiteers. Accessed on June 22, 2016.
Hornik, Robert, et al. 2008. “Effects of the National Youth Anti-Drug Media Campaign on Youths.” American Journal of Public Health. 98(12): 2229–2236. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2636541/. Accessed on June 26, 2016.
Ingraham, Christopher. 2016. “A New Anti-drug Campaign Has a Wild Idea to Stop Kids from Drinking and Doing Drugs.” The Washington Post. https://www.washingtonpost.com/news/wonk/wp/2015/07/16/the-newest-anti-drug-campaign-is-written-entirely-in-emoji/. Accessed on June 26, 2016.
“International Opium Convention Signed at The Hague January 23, 1912.” 1912. Telebit. http://www.telebit.gr/press/rss/files/almanak/1872-1912/opium1912.pdf. Accessed on June 24, 2016.
James-Burdumy, Susanne, et al. 2010. “The Effectiveness of Mandatory-Random Student Drug Testing.” National Center for Education Evaluation and Regional Assistance. https://ies.ed.gov/ncee/pubs/20104025/pdf/20104025.pdf. Accessed on June 23, 2016.
Johnson, Robert A., and Dean R. Gerstein. 1998. “Initiation of Use of Alcohol, Cigarettes, Marijuana, Cocaine, and Other Substances in US Birth Cohorts since 1919.” American Journal of Public Health. 88(1): 27–33.
Joy, Janet E., Stanley J. Watson, Jr., and John A. Benson, Jr., eds. 1999. Marijuana and Medicine: Assessing the Science Base. Washington, DC: National Academies Press.
Judge, J. W. 2007. “Workplace Drug Testing’s Mixed Success.” Behavioral Healthcare. 27(4): 14, 16.
King, Rufus. 1972. The Drug Hang-Up; America’s Fifty-Year Folly. New York: Norton. http://www.druglibrary.org/special/king/dhu/dhumenu.htm. Accessed on June 25, 2016.
Levy, Sharon, Miriam Schizer, and Committee on Substance Abuse. 2015. “Adolescent Drug Testing Policies in Schools.” Pediatrics. 135(4): 782–783.
Maginnis, Robert L. 2016. “Legalization of Drugs: The Myths and the Facts.” http://www.slideshare.net/sevans-idaho/legalization-of-drugs. Accessed on June 28, 2016.
Mapes, Jeff. 2015. “Oregon Marijuana Law Could Face Legal Challenge, City and County Associations Say.” Oregon Live. http://www.oregonlive.com/mapes/index.ssf/2015/03/oregon_marijuana_law_could_fac.html. Accessed on June 29, 2016.
“Marihuana and Social Policy.” 1971. Marihuana: A Signal of Misunderstanding. National Commission on Marihuana and Drug Abuse. http://www.druglibrary.org/Schaffer/Library/studies/nc/ncrec1_9.htm. Accessed on June 21, 2016.
“The Marihuana Tax Act of 1937.” 2016a. Schaffer Library of Drug Policy. http://www.druglibrary.org/schaffer/hemp/taxact/t10a.htm. Accessed on June 24, 2016.
“The Marihuana Tax Act of 1937.” 2016b. Schaffer Library of Drug Policy. http://www.druglibrary.org/schaffer/hemp/taxact/mjtaxact.htm. Accessed on June 24, 2016.
McGrath, Michael. 2016. “Nancy Reagan and the Negative Impact of the ‘Just Say No’ Anti-drug Campaign.” The Guardian. https://www.theguardian.com/society/2016/mar/08/nancy-reagan-drugs-just-say-no-dare-program-opioid-epidemic. Accessed on June 26, 2016.
“Medical Consequences of Drug Abuse.” 2012. National Institute on Drug Abuse. https://www.drugabuse.gov/related-topics/medical-consequences-drug-abuse. Accessed on June 28, 2016.
“Memorandum for All United States Attorneys.” 2013. U.S. Department of Justice. https://www.justice.gov/iso/opa/resources/3052013829132756857467.pdf. Accessed on December 23, 2016.
“Memorandum for Selected United States Attorneys.” 2009. U.S. Department of Justice. https://www.justice.gov/sites/default/files/opa/legacy/2009/10/19/medical-marijuana.pdf. Accessed on June 29, 2016.
“Memorandum for United States Attorneys.” 2011. U.S. Department of Justice. https://www.justice.gov/sites/default/files/oip/legacy/2014/07/23/dag-guidance-2011-for-medical-marijuana-use.pdf. Accessed on June 29, 2016.
Miron, Jeffrey A., and Katherine Waldock. 2010. “The Budgetary Impact of Ending Drug Prohibition.” Washington, DC: Cato Institute. http://object.cato.org/sites/cato.org/files/pubs/pdf/DrugProhibitionWP.pdf. Accessed on June 27, 2016.
“Mississippi Laws & Penalties.” 2016. NORML. http://norml.org/laws/item/mississippi-penalties-2?category_id=868. Accessed on June 27, 2016.
Moberg, D. Paul, and Andrew J. Finch. 2008. “Recovery High Schools: A Descriptive Study of School Programs and Students.” Journal of Groups in Addiction & Recovery. 2(2–4): 128–161.
“Monitoring Impacts of Recreational Marijuana Legalization: 2015 Baseline Report.” 2015. Forecasting and Research Division. Washington State Office of Financial Management. http://www.ofm.wa.gov/reports/marijuana_impacts_2015.pdf. Accessed on June 29, 2016.
Musto, David E. 1987. The American Disease: Origins of Narcotic Control, rev. ed. New York: Oxford University Press.
“National Drug Control Budget.” 2016. Office of National Drug Control Policy. https://www.whitehouse.gov/sites/default/files/ondcp/press-releases/fy_2017_budget_highlights.pdf. Accessed on June 27, 2016.
“National Drug Control Strategy.” 2008. Office of National Drug Control Policy. https://www.whitehouse.gov/sites/default/files/ondcp/Fact_Sheets/FY2009-Budget-Summary-February-2008.pdf. Accessed on June 27, 2016.
“National Study Shows ‘Gateway’ Drugs Lead to Cocaine Use.” 1994. Columbia University Record. http://www.columbia.edu/cu/record/archives/vol20/vol20_iss10/record2010.24.html. Accessed on June 28, 2016.
Nebraska and Oklahoma v. Colorado. 2016. SCOTUSblog. http://www.scotusblog.com/case-files/cases/nebraska-and-oklahoma-v-colorado/. Accessed on June 29, 2016.
Nephew, Thomas M., et al. 2002. Surveillance Report #55: Apparent per Capita Consumption: National, State, and Regional Trends, 1977–98. Rockville, MD: National Institute on Alcohol Abuse and Alcoholism, Division of Biometry and Epidemiology: Alcohol Epidemiologic Data System. http://pubs.niaaa.nih.gov/publications/surveillanceArchive/CONS98.pdf. Accessed on June 24, 2016.
“The New D.A.R.E. Program—This One Works.” 2014. D.A.R.E. http://www.dare.org/the-new-dare-program-this-one-works/. Accessed on June 21, 2016.
Newton, David E. 1999. Drug Testing: An Issue for School, Sports, and Work. Springfield, NJ: Enslow Publishers.
Newton, David E. 2014. Steroids and Doping in Sports: A Reference Handbook. Santa Barbara, CA: ABC-CLIO.
Normand, Jacques, Richard O. Lempert, and Charles P. O’Brien, eds. 1994. Under the Influence: Drugs and the American Workforce. Washington, DC: National Academies Press.
Olson, Dave. 2004a. “Advantages and Disadvantages of Workplace Drug Testing.” Privacy, Freedom, and Security Program. Evergreen State College. http://www.uncleweed.com/words/essays/drugtesting-matrix.pdf. Accessed on June 22, 2016.
Olson, Dave. 2004b. “Privacy Issues in Workplace Drug Testing.” Privacy, Freedom, and Security Program. Evergreen State College. http://uncleweed.net/words/essays/Workplace-Drug-Testing.pdf. Accessed on June 22, 2016.
Oscapella, Eugene. 2003. “How Drug Prohibition Finances and Otherwise Enables Terrorism.” Speech given at the Lisbon International Symposium on Global Drug Policy. http://www.ukcia.org/research/ProhibitionFinancesTerrorism.pdf. Accessed on June 28, 2016.
“Part B—Authority to Control; Standards and Schedules.” 2016. U.S. Code. Title 21. Chapter 13. Subchapter 1. http://uscode.house.gov/view.xhtml?path=/prelim@title21/chapter13/subchapter1/partB&edition=prelim. Accessed on June 26, 2016.
Pearce, David. 2016. “Vintage Wine.” BLTC Research. http://cocaine.org/cocawine.htm. Accessed on June 24, 2016.
Pidd, Ken, and Ann M. Roche. 2014. “How Effective Is Drug Testing as a Workplace Safety Strategy? A Systematic Review of the Evidence.” Accident Analysis & Prevention. 71(1): 154–165.
Prah, Pamela M. 2005. “Methamphetamine.” CQ Researcher. http://library.cqpress.com/cqresearcher/document.php?id=cqresrre2005071500. Accessed on June 26, 2016.
Pratt, Timothy. 2015. “Marijuana Legalization Clashes with Drug Testing in the Workplace.” The Guardian. http://www.theguardian.com/sustainable-business/2015/apr/19/marijuana-workplace-drug-testing-employers-employees-medical-recreational. Accessed on June 22, 2016
“Prescription Drugs.” 2016. Govtrack.us. https://www.govtrack.us/congress/bills/subjects/prescription_drugs/6184. Accessed on June 27, 2016.
“Professional Sports and Their Drug Policies.” 2016. USA Today. http://usatoday30.usatoday.com/sports/graphics/sports_steroids/flash.htm. Accessed on June 23, 2016.
Public Law 105–277. 1998. http://frwebgate.access.gpo.gov/cgi-bin/getdoc.cgi?dbname=105_cong_public_laws&docid=f:publ277.pdf. Accessed on June 26, 2016.
“Publications.” 1994. National Criminal Justice Reference Service. https://www.ncjrs.gov/App/publications/abstract.aspx?ID=161247. Accessed on June 28, 2016.
Quinn, Elizabeth. 2015. “Steroids, Anabolic and Androgenic Steroids in Sports. Very Well. https://www.verywell.com/steroids-in-sports-3120518. Accessed on June 23, 2016.
“Quotes about Methamphetamine.” 2016. Quotesgram. http://quotesgram.com/quotes-about-methamphetamine/. Accessed on June 26, 2016.
Reed, Jack K. 2016. “Marijuana Legislation in Colorado: Early Findings.” Colorado Department of Public Safety. http://cdpsdocs.state.co.us/ors/docs/reports/2016-SB13-283-Rpt.pdf. Accessed on June 29, 2016.
Reid Paula, and Stephanie Condon. 2015. “DEA Chief Says Smoking Marijuana as Medicine ‘Is a Joke.’ ” CBS News. http://www.cbsnews.com/news/dea-chief-says-smoking-marijuana-as-medicine-is-a-joke/. Accessed on June 29, 2016.
“Report of Committee on Acquirement of the Drug Habit.” 1902. Proceedings of the American Pharmaceutical Society. https://books.google.com/books?id=QHICAAAAYAAJ&pg=PA572&lpg=PA572&dq=%22if+the+chinaman+cannot+get+along+without+his+dope%22&source=bl&ots=_Mp0NsjY1i&sig=EI-khMNxBLGFY770MM8m9Q137Zo&hl=en&sa=X&ved=0ahUKEwjH95SflsHNAhUT6GMKHVypC6AQ6AEIIzAB#v=onepage&q=%22if%20the%20chinaman%20cannot%20get%20along%20without%20his%20dope%22&f=false. Accessed on June 24, 2016.
“Results from the 2014 National Survey on Drug Use and Health: Detailed Tables.” 2015. Research Triangle Park, NC: RTI International. http://www.samhsa.gov/data/sites/default/files/NSDUH-DetTabs2014/NSDUH-DetTabs2014.pdf. Accessed on June 22, 2016.
Riggs, Mike. 2011. “Obama Administration Overrides 2009 Ogden Memo, Declares Open Season on Pot Shops in States Where Medical Marijuana Is Legal.” Reason.com. http://reason.com/blog/2011/06/30/white-house-overrides-2009-mem. Accessed on December 23, 2016.
Ringwalt, Chris, et al. 2008. “Random Drug Testing in US Public School Districts.” American Journal of Public Health. 98(5): 826–828.
Robertson, Elizabeth B., Susan L. David, and Suman A. Rao. 2003. Preventing Drug Use among Children and Adolescents: A Research-Based Guide for Parents, Educators, and Community Leaders. Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health: National Institute on Drug Abuse.
Russo, Ethan, and Franjo Grotenhermen. 2006. Handbook of Cannabis Therapeutics: from Bench to Bedside. New York: Haworth Press.
Schaffer, Cliff. 2016. “Did Alcohol Prohibition Reduce Alcohol Consumption and Crime?” Schaffer Library of Drug Policy. http://www.druglibrary.org/prohibitionresults.htm. Accessed on June 24, 2016.
Scott, Emilee Mooney. 2010. OLR Research Report. https://www.cga.ct.gov/2010/rpt/2010-R-0204.htm. Accessed on June 29, 2016.
“Simplification Draft Paper.” 2016. United States Sentencing Commission. http://www.ussc.gov/research/research-and-publications/simplification-draft-paper-2. Accessed on June 26, 2016.
“65170: Medical Marijuana and Other Cannabinoids.” 2016. NetCE. http://www.netce.com/coursecontent.php?courseid=1256#chap.7. Accessed on June 29, 2016.
“Speaking Out against Drug Legalization.” [2010]. U.S. Drug Enforcement Administration. https://www.dea.gov/pr/multimedia-library/publications/speaking_out.pdf. Accessed on June 28, 2016.
“State Industrial Hemp Statutes.” 2016. National Conference of State Legislatures. http://www.ncsl.org/research/agriculture-and-rural-development/state-industrial-hemp-statutes.aspx. Accessed on June 24, 2016.
“State Laws.” 2016. NORML. http://norml.org/laws/. Accessed on June 29, 2016.
“State Medical Marijuana Laws.” 2016. National Conference of State Legislatures. http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx. Accessed on June 29, 2016.
Stolz, Barbara Ann. 1992. “Congress and the War on Drugs: An Exercise in Symbolic Politics.” Journal of Crime and Justice. 15(1): 119–136.
Stout, David, and Solomon Moore. 2009. “U.S. Won’t Prosecute in States That Allow Medical Marijuana.” The New York Times. http://www.nytimes.com/2009/10/20/us/20cannabis.html. Accessed on June 29, 2016.
Stuart, Susan P. 2010. “When the Cure Is Worse Than the Disease: Student Random Drug Testing & Its Empirical Failure.” Valparaiso University Law Review. 44(4): 1055–1082.
Sznitman, S. R., and D. Romer. 2014. “Student Drug Testing and Positive School Climates: Testing the Relation between Two School Characteristics and Drug Use Behavior in a Longitudinal Study.” Journal of Studies on Alcohol and Drugs. 75(1): 65–73.
Tandy, Karen P. 2005. “Marijuana: The Myths Are Killing Us.” U.S. Drug Enforcement Administration. https://www.dea.gov/pubs/pressrel/pr042605.html. Accessed on June 28, 2016.
“Tobacco Control Act.” 2016. U.S. Food and Drug Administration. http://www.fda.gov/TobaccoProducts/GuidanceComplianceRegulatoryInformation/ucm246129.htm. Accessed on June 27, 2016.
“2016–2017 NCAA Banned Drugs.” 2016. http://www.ncaa.org/sites/default/files/2016_17_%20Banned_%20Drugs_%20Educational_%20Document_20160531.pdf. Accessed on June 23, 2016.
Uncle Mike [pseud.]. 2008. “U.S. District Court, Denver, Colorado Imposes First Federal Marihuana Law Penalties.” http://www.unclemikesresearch.com/u-s-district-court-denver-colorado-imposes-first-federal-marihuana-law-penalties/. Accessed on June 24, 2016.
Vagins, Deborah J., and Jesselyn McCurdy. 2006. “Cracks in the System: Twenty Years of the Unjust Federal Crack Cocaine Law.” American Civil Liberties Union. https://www.aclu.org/sites/default/files/field_document/cracksinsystem_20061025.pdf. Accessed on June 26, 2016.
Vernonia School Dist. 47J v. Acton 515 U.S. 646. 1995. U.S. Supreme Court. http://www.supremecourt.gov/opinions/boundvolumes/515bv.pdf. Accessed on June 23, 2016.
Vimont, Celia. 2011. “Recovery High Schools: Giving Students a Second Chance.” Partnership for Drug-Free Kids. http://www.drugfree.org/join-together/recovery-high-schools-giving-students-a-second-chance/. Accessed on June 30, 2016.
Wallace, Alicia. 2015. “Colorado Supreme Court: Employers Can Fire for Off-Duty Pot Use.” Denver Post. http://www.denverpost.com/2015/06/15/colorado-supreme-court-employers-can-fire-for-off-duty-pot-use/. Accessed on June 22, 2016.
Warner, Joel. 2016. “Marijuana Legalization Movement Just Won Multiple Courtroom Battles, But Will That Be Enough to Quash Future Legal Threats?” International Business Times. http://www.ibtimes.com/marijuana-legalization-movement-just-won-multiple-courtroom-battles-will-be-enough-2342055. Accessed on June 29, 2016.
Whitebread, Charles. 1995. “The History of the NonMedical Use of Drugs in the United States: A Speech to the California Judges Association 1995 Annual Conference.” Schaffer Library of Drug Policy. http://www.druglibrary.org/schaffer/history/whiteb1.htm. Accessed on June 25, 2016.
Xu, Jianquan, et al. 2016. “Deaths: Final Data for 2013.” National Vital Statistics Report. Volume 64, Number 2. http://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_02.pdf. Accessed on June 28, 2016. Supplemental tables are at http://www.cdc.gov/nchs/data/nvsr/nvsr64/nvsr64_02_tables.pdf. Accessed on June 28, 2016.
Yamaguchi, Ryoko, Lloyd D. Johnston, and Patrick M. O’Malley. 2003. Drug Testing in Schools: Policies, Practices, and Association with Student Drug Use. Occasional Paper No. 2. Ann Arbor: Institute for Social Research. University of Michigan. http://www.yesresearch.org/publications/occpapers/YESOccPaper2.pdf. Accessed on June 23, 2016.
Youth Violence: A Report of the Surgeon General. 2001. Public Health Service. Office of the Surgeon General. Washington, DC: Government Printing Office. http://www.ncbi.nlm.nih.gov/books/NBK44294/. Accessed on June 21, 2016.
Zimmer, Lynn. 1999. Drug Testing: A Bad Investment. New York: American Civil Liberties Union.

Young adults attend a pro-marijuana rally held in Denver in April 2013. Marijuana is now legal in Colorado. (AP Photo/Brennan Linsley)