Looking separately at the axial and appendicular skeletons
Noting some skeletal pathologies
If you have any skeletons in your closet, now is the time to pull them out. We’re not talking about your deep, dark secrets. Seriously! Actually looking at a model of a skeleton is the best way to figure out what’s connected to what. If you don’t have any skeletons in your closet, try your refrigerator. Observantly cutting up a chicken can show you a lot about bones and joints. And you’ll get a head start on dinner!
The skeleton determines humans’ general shape and size as a species, and also humans’ very distinctive upright posture and bipedal gait. To get an overview of the skeleton, refer to the “Major Bones of the Skeleton” color plate in the center of this book.
In humans, as in all vertebrates, the skeleton is part of the musculoskeletal system. The other part, the muscular system, is the subject of Chapter 6.
The skeleton consists of all your bones, all the joints that connect your bones, and various kinds of fibrous tissue that cover, protect, and bind bones and joints together. In this chapter, we look at the special structures of these tissues and name some of the most important bones and joints. Other important functions of bone tissue, like mineral storage and blood cell production, are mentioned briefly or covered in detail in other chapters.
Reporting for Duty: The Jobs of Your Skeleton
The structural functions of the skeletal system are these:
Protection: Bones and joints are strong and resilient. The rib cage provides a protected inner space for your more delicate internal organs. The vertebral column partially encases and protects the spinal cord, and the skull completely encases the brain.
Movement: The musculoskeletal system is a motion machine: The bones anchor the skeletal muscles and act as levers, the joints act as fulcrums, and muscle contraction provides the force for movement. (See Chapter 6 for information about muscles and muscle contraction.)
This section is about how your body builds the tissues of the bones and the joints and how they all fit together to protect, move, and support the entire body.
Caring about connective tissue
The skeleton is made up mainly of three types of connective tissue: osseous (bone) tissue, cartilage, and fibrous connective tissue.
Osseous tissue
Osseous tissue is physiologically very active, constantly generating and repairing itself, and has a generous blood supply all through it. Not only that, but bone makes a huge amount of “product for export,” notably the very cells of the blood. (Yes, new blood cells are made by bones — see Chapter 9.) Bone contains four specialized types of cells: osteocytes, osteoblasts, osteoclasts, and osteogenic cells. The skeletal system’s functions depend on the functioning of these specialized cells in bone tissue.
Keep in mind the difference between bone tissue and a specific, named bone. Both the femur (thigh bone) and the humerus (arm bone) contain bone tissue, but each bone has its own specialized configuration of the components of bone tissue.
We think of our bones as being hard like rocks, and they are, but the structure of the osseous tissue is quite complex. Figure 5-1 shows the parts of osseous tissue.
The first thing you notice when looking at osseous tissue are the big holes. Then you see that everything seems to be arranged in circles around those holes. One set of these circles is called an osteon; these structures are repeated and glued together to form compact bone. The hole in the middle, the Haversian (or central) canal, creates space for the nerves and blood vessels to run throughout the bone.
Each ring encircling the central canal is called a lamella. These are formed as calcium compounds (such as calcium phosphate and calcium carbonate) are deposited into the matrix (the space between the cells). Unlike in other tissues where the matrix is fluid filled, bone cells, called osteocytes, are unable to move. They can be found in little caves called lacunae.
Also due to the rigid matrix, cells must get their nutrients from other cells. Osteocytes have armlike structures that reach through little tunnels through the matrix called canaliculi. Cells in the inner ring (lamella) have access to resources from the blood vessels in the central canal. They then pass these resources on to cells in the next ring through the canaliculi (tunnels). This continues, cell to cell, like a game of telephone.
Cartilage
Cartilage is a firm but flexible tissue made up of mostly protein fibers. If you put your finger on the end of your nose and push gently, you can get a very good idea of the rubbery texture and flexibility of cartilage. Cartilage is the main component of joints.
Cartilage is less complicated in its structure than bone tissue, having fewer cells, fewer cell types, and little or no direct blood supply. However, among the functions of cartilage tissue is the building of new bone. The two types of cartilage in the skeletal system are hyaline cartilage and fibrocartilage.
Hyaline cartilage is the type that forms the septum of your nose. It also forms a portion of the very first version of the fetal skeleton. It’s the most abundant type of cartilage in several kinds of joints — it’s a major component of the freely movable ones called synovial joints.
Fibrocartilage is a fibrous, spongy tissue that acts as a shock absorber in the vertebral column (spine) and the pelvis.
Cartilage isn’t generated and replaced as actively as bone, so cartilage gets by with fewer cells, and mature cartilage has no blood supply.
There is a third type of cartilage: elastic cartilage. Unlike the other two types, it contains numerous elastic fibers, making it much more flexible. You can find elastic cartilage in your epiglottis and your external ear.
Fibrous connective tissue
Fibrous connective tissue (FCT) can be compared to the kind of packing tape that has fibers in it. FCT contains very few living cells and is composed mainly of protein fibers, complex sugars, and water.
FCT forms a structure called the periosteum, a protective sheet that covers bones. The collagen fibers in this covering intertwine with the collagen fibers of the tendons and ligaments. These cordlike structures connect a bone to another bone (ligaments), or a bone to a muscle (tendon).
The periosteum is said to be continuous with the ligaments and tendon, because there’s no real separation between the “sheet” and the “cords.” This prevents them from letting go of the bone.
The structure of a bone
The structures called bones (the femur, the vertebrae, the finger bones) are made of bone tissue. (No surprise there, you say, but note that structures called joints are made of the tissue called cartilage.) It’s important to remember that different individual bones have different forms of bone tissue.
Long bones such as your thighbone (femur) or forearm bone (radius) are the type of bones people usually think of first. And in fact, they make a good illustration of general anatomy and physiology of bone tissue (see Figure 5-2).
In cross section, bone is structured in concentric layers, that is, an outer layer surrounds a middle layer, which in turn surrounds an inner layer. In longitudinal section, a bone has two ends, mostly similar, and a long middle area, which has cells and tissues mostly different from the ends. The following list names and briefly describes cellular and material composition of the areas of a long bone:
Compact (cortical) bone (the outer layer) is a dense layer of cells in a hard matrix of protein fibers and compounds made of calcium and other minerals. This is the layer that gives bones their amazing strength. Compact bone tissue is described in detail in the “Caring about Connective Tissue” section, earlier in this chapter.
Spongy (trabecular) bone (the middle layer) is, like compact bone, a variety of cell types within a matrix of mineralized protein fibers. But spongy bone has a more open structure than compact bone, a physiological trade-off between strength and lightness. The matrix of spongy bone is not arranged in concentric circles; instead, it appears, well, spongy. Structures called trabeculae, which follow stress lines in the bone, act like braces, providing support while leaving large pockets of space. In adults, this space contains red marrow, described in the next subsection.
The medullary cavity is the inner layer of the shaft of a long bone (the diaphysis). The medullary cavity houses bone marrow, which comes in two varieties. There’s yellow marrow, which is mostly fat (think butter), and red marrow, the site of hematopoiesis, the production of blood cells. In adults, most of the marrow in the medullary cavity is deactivated and, thus, yellow. The active, red marrow is found in spongy bone of the skull, ribs, vertebrae, pelvis, and sternum (breastbone). In infants, medullary cavities of the long bones are mostly filled with red marrow to meet the increasing demand for blood cells.
Epiphysis is the enlarged, knobby end of a long bone. It consists of an outer layer of compact bone overlying spongy bone. This is the site of bone elongation. Within the epiphysis, bone and cartilage tissue are intimately connected: As cartilage cells divide, cartilage morphs into bone tissue. This process continues from before birth until the bones reach their full adult size.
If blood cell levels drop too low — after blood loss, for instance — the yellow marrow can be reactivated and again perform hematopoiesis.
Classifying bones
Bones come in different shapes and sizes. Appropriately, many bone type names match what they look like, such as flat bones, long bones, short bones, and irregular bones. Check out Table 5-1 for the differences among the four types of bones.
Like plates of armor, flat bones protect soft tissues of the brain and organs in the thorax and pelvis.
Long
Arms and legs
Like steel beams, these weight-bearing bones provide structural support.
Short
Wrists (carpal bones) and ankles (tarsal bones)
Short bones look like blocks and allow a wider range of movement than larger bones.
Irregular
Vertebral column, kneecaps
Irregular bones have a variety of shapes and usually have projections that muscles, tendons, and ligaments can attach to.
Bone Growth and Remodeling
When long bones develop in a fetus, they’re formed from hyaline cartilage. The softer cartilage allows the fetus to bend into the poses that would make a yoga instructor beam with pride. The shape of the bone is determined by the shape of the cartilage, so it serves as a template. Calcium compounds are deposited onto the template, and the cartilage becomes calcified.
The terms calcification and ossification are often used synonymously to refer to the formation of bone. However, ossification is properly the formation of the whole tissue, whereas calcification is the actual formation and deposition of the calcium compounds.
Even at birth, the bones are not fully ossified. They continue to grow and develop well into the teenage years. This occurs via two types of ossification:
Intramembranous ossification: Intramembranous ossification occurs in all bones; it’s how short, flat, and irregular bones grow in size, and it’s how long bones increase their width. A sheet of connective tissue is formed beneath the periosteum. Specialized bone cells called osteoblasts place the calcium compounds onto the fibers of the connective tissue, creating the trabeculae of spongy bone (calcification). When they’re done building, osteoblasts become osteocytes. Later, the new spongy bone can be further developed into compact bone as new osteoblasts fill the empty space with calcium compounds until they’ve walled themselves in to a little cave — a lacuna.
Endochondral ossification: To increase their length, long bones use endochondral ossification. In Figure 5-2, you see an epiphyseal line on each end. Rather than being osseous tissue, the epiphyseal line (or plate) is made of hyaline cartilage. When stimulated by growth hormone (see Chapter 8), the chondrocytes (cartilage cells) begin to copy themselves. The cells will then enlarge, which creates more space, thus lengthening the bone. Osteoblasts will then calcify the cartilage just as they did to the connective tissue during intramembranous growth.
When the long bones increase in length, you increase in height. Eventually, around age 18, the chondrocytes stop dividing. The entire epiphyseal line is ossified (turned into bone). This is commonly referred to as the growth plates being closed.
While you’re likely done growing at this point in your life, your bones are definitely not done developing. This continues throughout life via a process called remodeling.
Because bones are constantly absorbing the forces placed on our bodies, the matrix gets damaged. The remodeling process allows the bones to retain their structural integrity by constantly replacing the weakened tissue with strong, healthy matrix. It works like road construction. The roads wear out with continued use and need to be refreshed. But you can’t do all the roads at once or else people wouldn’t be able to get places. So you do it in sections at a time, all the time. Luckily, bone remodeling doesn’t cause the headaches that road construction does!
Before we can activate osteoblasts to build new tissue, we must first clear the area. Specialized bone cells called osteoclasts are responsible for this task. Osteoclasts secrete acid to break down the weakened matrix. This releases the calcium ions from their compounds, allowing them to be absorbed into blood flow. Then osteoblasts recycle the calcium, building new compounds to deposit and reform the matrix stronger than before.
The forgotten function of bones is to store calcium, an ion essential for both muscle contraction and nervous communication (see Chapters 6 and 7). When blood calcium levels drop too low, parathyroid hormone (PTH) is released and proceeds to the bones. The PTH then stimulates osteoclasts to resorb the calcium.
The Axial Skeleton
The axial skeleton consists of the bones that lie along the midline (center) of your body, such as your vertebral column (backbone). An easy way to remember what bones make up the axial skeleton is to think of the vertebral column running down the middle of your body and then the bones that are directly attached to it — the thoracic cage (rib cage) and the skull.
The following sections give you a closer look at the main parts of the axial skeleton.
Keeping your head up: The skull
Rather than one big piece of bone, like a cap that fits over the brain, the skull comprises the cranial and the facial bones.
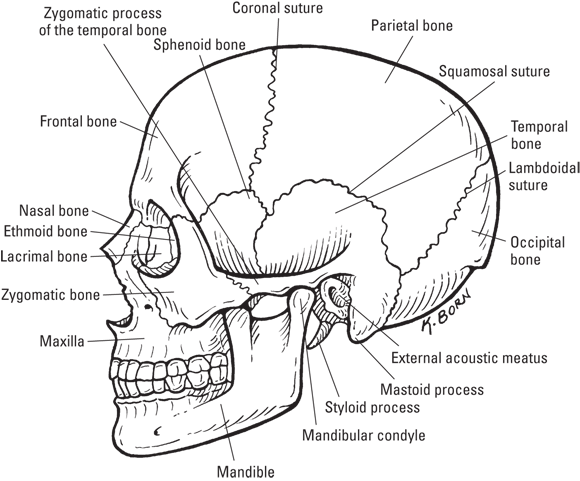
A human skull (see Figure 5-3) is made up of the cranium, which is formed of several bones, and the facial bones. The facial bones contain cavities called the sinuses, which do have a purpose other than harboring upper respiratory infections.
Illustration by Kathryn Born, MA
FIGURE 5-3: The human skull: cranium and facial bones.
Cracking the cranium
The eight bones of your cranium protect your brain and have immovable joints between them called sutures. (These look a lot like the sutures, or stitches, that you may receive to close an incision or wound.) The bones of the cranium that are joined together by sutures include the following:
Frontal bone: Gives shape to the forehead and part of the eye sockets.
Parietal bones: Two bones that form the roof and sides of the cranium.
Occipital bone: Forms the back of the skull and the base of the cranium. The foramen magnum, an opening in the occipital bone, allows the spinal cord to pass into the skull and join the brain.
Temporal bones: Form the sides of the cranium near the temples. The temporal bone on each side of your head contains the following structures:
External auditory meatus: The opening to your ear canal
Mandibular fossa: Joins with the mandible (the lower jaw)
Mastoid process: Provides a place for neck muscles to join your head
Styloid process: Serves as an attachment site for muscles of the tongue and larynx (voice box)
Ethmoid bone: Contains several sections, called plates. Forms the medial (inside) part of the eye sockets and much of the nasal cavity.
Sphenoid bone: Shaped like a butterfly or a saddle (depending on how you look at it), the sphenoid forms the floor of the cranium and the back and lateral sides of the eye sockets (orbits). A central, sunken portion of the sphenoid bone called the sella turcica shelters the pituitary gland, which is very important in controlling major functions of the body. (See Chapter 8 for more on the pituitary gland.)
Facing the facial bones
The bones that form facial structures are
Lacrimal bones: Two tiny bones on the inside walls of the orbits. A groove between the lacrimal bones in the eye sockets and the nose forms the nasolacrimal canal. Tears flow across the eyeball and through that canal into your nasal cavity, which explains why your nose “runs” when you cry.
Mandible: The lower jaw and the only movable bone of the skull.
Maxillae: Two bones that form the upper jaw, part of the hard palate (roof of your mouth), and bottom of the orbits.
Nasal bones: Two rectangular-shaped bones that form the bridge of your nose. The lower, movable portion of your nose is made of cartilage.
Palatine bones: Form the back portion of the hard palate and is the floor of the nasal cavity.
Vomer bone: Joins the ethmoid bone to form the nasal septum — that part of your nose that can be deviated by a strong left hook.
Zygomatic bones: Form the cheekbones and the lateral (outer) sides of the orbits.
Sniffing out the sinuses
The sinuses allow air into the skull, making it much lighter. The air in your sinuses also gives resonance to your voice, which means that when you talk, the sound waves reverberate in your sinuses.
Several types of sinuses are named for their location:
The frontal sinus is a hollowed-out area in the frontal bone.
Mastoid sinuses drain into the middle ear.
Maxillary sinuses are large and within the bones of the upper jaw (the maxilla).
Paranasal sinuses consist of the frontal, sphenoidal, and ethmoidal sinuses, which, along with the maxillary sinuses, drain into the nose (para means “near”; nas- means “nose”).
Setting you straight on the curved spinal column
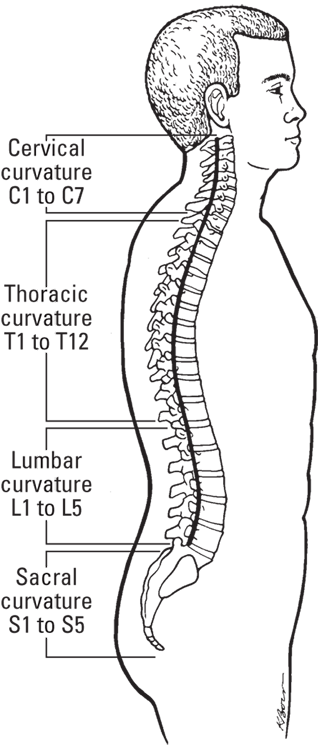
The spinal column (see Figure 5-4) begins within the skull and extends down to the pelvis. It’s made up of 33 bones in all: 24 separate bones called vertebrae (singular, vertebra), plus the fused bones of the sacrum and the coccyx. Between each vertebra is an intervertebral disc made of fibrocartilage for shock absorption.
Your spinal column is the central support for the upper body, carrying most of the weight of your head, chest, and arms. Together with the muscles and ligaments of your back, your spinal column enables you to walk upright.
An important purpose of the vertebral column is to protect your spinal cord, the big data pipe between your body and your brain. Nearly all your nerves are connected, either directly or through networked branches, to the spinal cord, which runs directly into the brain through the opening in the skull called the foramen magnum. Turn to Chapter 7 for more information about the spinal cord.
If you look at the spine from the side, you notice that it curves four times: inward, outward, inward, and outward. The curvature of the spine helps it absorb shock and pressure much better than if the spine were straight. A curved spine also affords more balance by better distributing the weight of the skull over the pelvic bones, which is needed to walk upright. A curved spine keeps you from being top-heavy. Each curvature spans a region of the spine: cervical, thoracic, lumbar, and sacral. The number of vertebrae in each region and some important vertebral features are given in Table 5-2.
The skull attaches at the top of this region to the vertebrae called the atlas.
Thoracic
12
The ribs attach to this region.
Lumbar
5
Commonly referred to as the small of the back, it takes the most stress.
Sacral
5 (fused into one; the sacrum)
The sacrum forms a joint with the hipbones and the last lumbar vertebra.
Coccygeal
4 (fused into one; the coccyx, also called the tailbone)
The coccyx absorbs the shock of sitting.
The vertebral column also provides places for other bones to attach. The skull is attached to the top of the cervical spine. The first cervical vertebra (abbreviated C-1; “C” for cervical, “1” for first) is the atlas, which supports the head and allows it to move forward and back (for example, the “yes” movement). The second cervical vertebra (C-2) is called the axis, and it allows the head to pivot and turn side to side (that is, the “no” movement).
You can differentiate these two important bones by recalling the Greek story about Atlas, who held the world on his shoulders. Your atlas holds your head on your shoulders. To remember the number of vertebrae in each region, think: breakfast, lunch, and dinner.
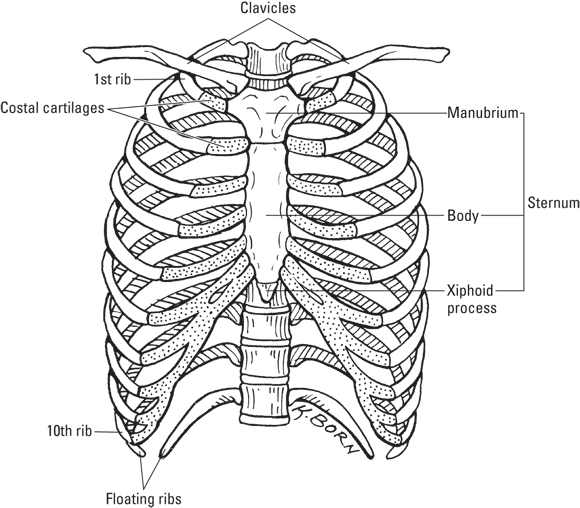
Being caged can be a good thing
The rib cage (also called the thoracic cage) consists of the thoracic vertebrae, the ribs, and the sternum (see Figure 5-5). The rib cage is essential for protecting your heart and lungs and for providing a place for the pectoral girdle (scapulae and clavicles) to attach.
You have 12 pairs of bars in your cage. Some of your ribs are true (7), some are false (3), and some are floating (2). All ribs are connected to the bones in your back (the thoracic vertebrae). In the front, true ribs are connected to the sternum (breastbone) by individual costal cartilages (cost- means “rib”); false ribs are connected to the sternum by fused costal cartilage. The last two pairs of ribs are called floating ribs because they remain unattached in the front. The floating ribs give protection to abdominal organs, such as your kidneys, without hampering the space in your abdomen for the intestines.
The sternum (breastbone) has three parts: the manubrium, the body, and the xiphoid (pronounced zi-foid) process. The notch that you can feel at the top center of your chest, in line with your collarbones (the clavicles), is the top of the manubrium. The middle part of the sternum is the body, and the lower part of the sternum is the xiphoid process.
The Appendicular Skeleton
The appendicular skeleton is made up of the bones and joints of the appendages (upper and lower limbs) and the two girdles that join the appendages to the axial skeleton. We describe each of these categories in the following sections.
Wearing girdles: Everybody has two
The word girdle is a verb than means “to encircle.” It has nothing to do with that funny undergarment all polite women wore in the early 20th century.
The body contains two girdles: the pectoral girdle, which encircles the vertebral column at the top, and the pelvic girdle, which encircles the vertebral column at the bottom. The girdles serve to attach the appendicular skeleton to the axial skeleton.
The pectoral girdle consists of the two clavicles (collarbones) and the two triangle-shaped scapulae (shoulder blades). The scapulae provide a broad surface to which arm and chest muscles attach. Refer to the “Major Bones of the Skeleton” color plate to see the individual parts of the pectoral girdle.
The clavicles are attached to the sternum’s manubrium. Significantly, this is the only point of attachment of the pectoral girdle and the axial skeleton. Because of this relatively weak attachment, the shoulders have a wide range of motion but are prone to dislocation.
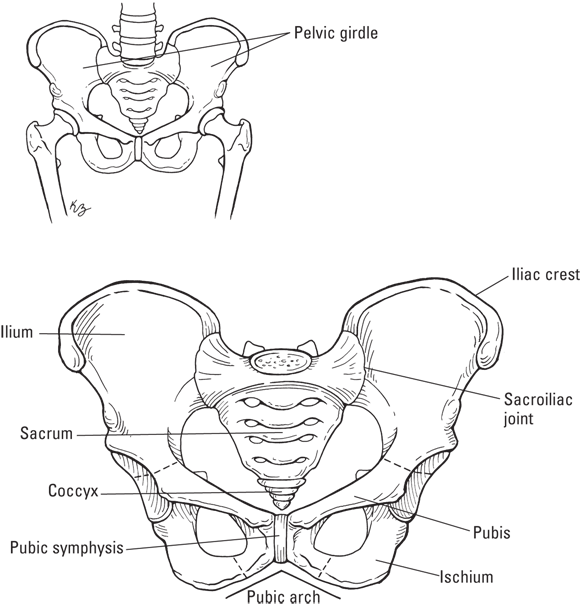
The pelvic girdle (see the pelvis in Figure 5-6) is formed by the hipbones (called coxal bones), the sacrum, and the coccyx (tailbone). The hipbones bear the weight of the body, so they must be strong.
The hipbones (coxal bones) are formed by the ilium, the ischium, and the pubis. The ilia are what you probably think of as your hipbones; they’re the large, flared parts that you can feel on your sides. The part that you can feel at the tip of the ilium is the iliac crest. In your lower back, the ilium connects with the vertebral column at the sacrum; the joint that’s formed is appropriately called the sacroiliac joint — a point of woe for many people with lower back pain.
The ischium is the bottom part of your hip. You have an ischium on each side, within each buttock. You’re most likely sitting on your ischial tuberosity right now. These parts of your hips are also called the sitz bones because they allow you to sit. The ischial tuberosity points outward and is the site where ligaments and tendons from the lower limbs attach. The ischial spine — which is around the area where the ilium and ischium join — is directed inward into the pelvic cavity. The distance between a woman’s ischial spines is key to her success in delivering an infant vaginally (see Chapters 14 and 15); the opening between the ischial spines must be large enough for a newborn’s head to pass through.
The pubis bones join the right and left hip bones together. They are joined together by a piece of fibrocartilage called the pubic symphysis. Pelvic floor muscles attach to the pelvic girdle at the pubis.
Going out on a limb: Arms and legs
Your arms and legs are limbs or appendages. The word append means to attach something to a larger body. Your appendages are attached to the axial skeleton by the girdles (see the preceding section).
Giving you a hand with hands (and arms and elbows)
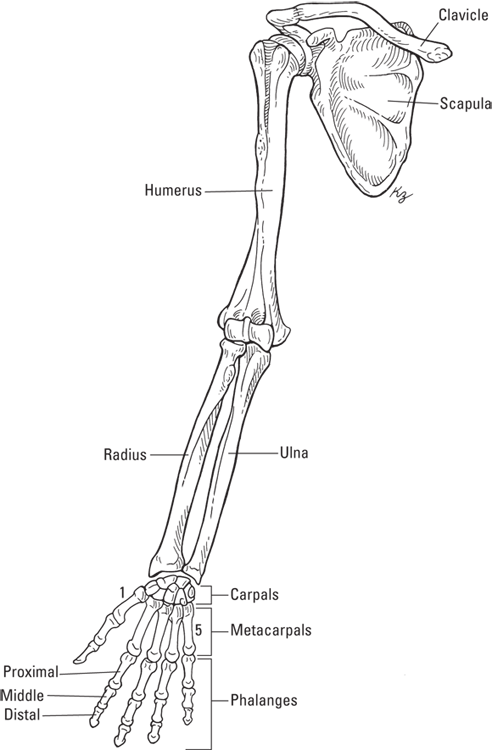
Your upper limb or arm is connected to your pectoral girdle. The bones of your upper limb include the humerus (arm), the radius and ulna (forearm), the carpals of the wrist, and the hand, which is made up of the metacarpal bones and the phalanges (refer to Figure 5-7).
The head (ball at the top) of the humerus connects to the scapula at the glenoid cavity. Muscles that move the arm and shoulder attach to the greater and lesser tubercles, two points near the head. Between the greater and lesser tubercles is the intertubercular groove, which holds the tendon of the biceps muscle to the humerus bone. The humerus also attaches to the deltoid muscle of the shoulder at a point about halfway down called the deltoid tuberosity. The muscle attached to the deltoid tuberosity allows you to raise and lower your arm.
The bones of the forearm attach at the elbow end of your humerus in four different spots:
Capitulum: Two knobs that allow the radius to articulate (join) with the humerus.
Trochlea: A pulley-like feature on the humerus that lies next to the capitulum and allows the trochlear notch of the ulna to articulate with the humerus.
Coronoid fossa: Depression in the humerus that accepts a projection of the ulna bone (called the coronoid process) when the elbow is bent.
Olecranon fossa: Depression in the humerus that accepts a projection of the ulna (called the olecranon process) when the arm is extended. Fitting, isn’t it?
The radius is the bone on the thumb side of your forearm. When you turn your forearm so that your palm is facing backward, the radius crosses over the ulna so that the radius can stay on the thumb side of your arm. The radius is shorter but thicker than the ulna. The head of the radius is flat like the head of a nail. The ulna is long and thin, and its head is at the opposite end of the bone compared with the head of the radius.
Both the radius and ulna connect with the bones of the wrist. The wrist contains eight short bones called the carpal bones. The ligaments binding the carpal bones are very tight, but the numerous bones allow the wrist to flex easily. The eight carpal bones are arranged in two rows. The proximal row (furthest from your fingertips) contain the scaphoid, lunate, triquetrum, and pisiform (from thumb to pinky — note that pisiform and pinky both start with p). The distal row (also from thumb to pinky) contain the trapezium, trapezoid, capitate, and hamate.
The palm of your hand contains five bones called the metacarpals. When you make a fist, you can see the ends of the metacarpals as your knuckles. Your fingers are made up of bones called the phalanges; each finger has three phalanges (phalanx is singular): the proximal phalanx, which joins your knuckle, the middle phalanx, and the distal phalanx, which is the bone in your fingertip. The thumb, though, only has two phalanges, so some people like to argue that it’s not considered a true finger. So you may have eight fingers and two thumbs or ten fingers depending on how you look at it. Regardless, on each hand the thumb is referred to as the first digit.
Getting a leg up on your lower limbs
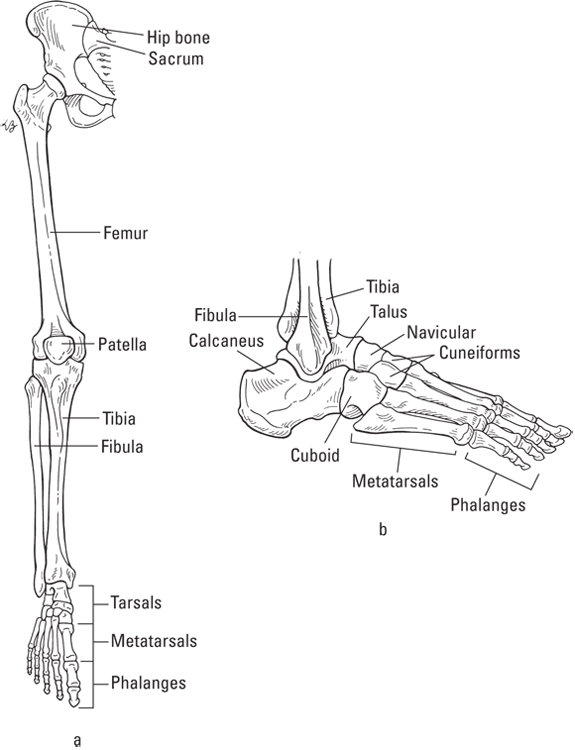
Your lower limb consists of the femur (thigh bone), the tibia and fibula of the leg, the bones of the ankle (tarsals), and the bones of the foot (metatarsals and phalanges; refer to Figure 5-8).
Illustration by Kathryn Born, MA
FIGURE 5-8: The bones of the lower limb (a), ankle, and foot (b).
The term phalanges refers to the finger bones and the toe bones.
The femur is the strongest bone in the body; it’s also the longest. The head of the femur fits into a hollowed out area of the hip bone called the acetabulum. In women, the acetabula (plural) are smaller but spread farther apart than in men. This anatomic feature allows women to have a greater range of movement of the thighs than men. The greater and lesser trochanters of the femur are surfaces to which the muscles of the legs and buttocks attach. Trochanters are large processes found only on the femur. The linea aspera is a ridge along the back of the femur to which several muscles attach.
The femur forms the knee along with bones of the lower leg. The patella (commonly known as the kneecap) articulates with the bottom of the femur. The femur also has knobs (lateral and medial condyles) that articulate with the top of the tibia. The ligaments of the patella attach to the tibial tuberosity. The bottom, inner end of the tibia has a bulge called the medial malleolus, which forms part of the inner ankle.
The tibia, also called the shinbone, is much thicker than the fibula and lies on the medial (inside) portion of the leg. Although the fibula is thinner, it’s about the same length as the tibia. The bottom, outside end of the fibula is the lateral malleolus, which is the bulge on the outside of your ankle.
Your foot is designed in much the same way as your hand. The ankle, or tarsus, which is akin to the wrist, consists of seven tarsal bones. However, only one of those seven bones is part of a joint with a great range of motion — the talus. The talus bone joins to the tibia and fibula and allows for the movements of your ankle. Beneath the talus is the largest tarsal bone, the calcaneus, which is the heel bone. The calcaneus and talus help to support your body weight. The remaining tarsals are the cuboid on the outside, the navicular, and the lateral, intermediate, and medial cuneiforms.
The instep of your foot is akin to the palm of your hand, and just as the hand has metacarpals and phalanges, the foot has metatarsals and phalanges. The ends of the metatarsals on the bottom of your foot form the ball of your foot. As such, the metatarsals also help to support your body weight. Together, the tarsals and metatarsals held together by ligaments and tendons form the arches of your feet. Your toes are also called phalanges, just like your fingers. And, just as your thumbs have only two phalanges, your big toes have only two phalanges. But, the rest of your toes have three: proximal, middle, and distal.
Joints and the Movements They Allow
A joint, or articulation, is a connection between two bones. Some joints move freely, some move a little, and some never move. This section tells you about the different joint structures and the movements they allow.
Categorizing the types of joints
Joints, which vary greatly in their size and shape, can be classified by the amount of movement they permit or by their structure.
Structural groupings
Joints fall into three categories based on the type of connective tissue present where the bones meet:
Fibrous: Bones held tightly together by dense connective tissue containing numerous collagen fibers
Cartilaginous: Bones held together with either hyaline or fibrocartilage
Synovial: Bones, which are lined with hyaline cartilage, are held together by a connective tissue capsule
Immovable joints
Synarthroses are joints that don’t move, such as those between the bones of the skull. A thin layer of fibrous connective tissue, called a suture, joins them together. The sutures in the cranium are named as follows:
Coronal suture: Joins the parietal bones and the frontal bone
Lambdoidal suture: Joins the parietal bones and the occipital bone
Sagittal suture: Between the parietal bones
Squamosal sutures: Between the parietal and temporal bones
Most fibrous joints are synarthroses.
Slightly movable joints
Amphiarthroses are slightly movable joints connected by fibrocartilage or hyaline cartilage. Examples include the intervertebral disks, which join each vertebrae and allow slight movement of the vertebrae.
Most cartilaginous joints are amphiarthroses.
Freely movable joints
Diarthroses are joints that are freely movable. The numerous types of diarthroses are shown in Table 5-3.
A joint in which the ball-shaped head of one bone fits into a depression (socket) in another bone
Circular movements; can move in all planes, and rotation is possible.
Shoulder, hip
Condyloid joint
A joint in which the oval-shaped condyle of one bone fits into the oval-shaped cavity of another bone
Can move in all planes, but can’t rotate.
Knuckles (joints between metacarpals and phalanges)
Gliding joint
A flat or slightly curved surfaces joint
Sliding or twisting; movement in two planes.
Joints between carpal bones (wrist) and between tarsal bones (ankle)
Hinge joint
A joint in which a convex surface joins with a concave surface
Up and down motion in one plane; can bend (flex) or straighten (extend).
Elbow, knee
Pivot joint
A joint in which a cylinder-shaped projection on one bone is surrounded by a ring of another bone and ligament
Rotation is only movement possible.
Joint between radius and ulna at elbow and joint atlas and axis at top of vertebral column
Saddle joint
A joint in which each bone is saddle shaped and fits into the saddle-shaped region of the opposite bone
Many movements are possible; can move in different planes but can’t rotate.
Joint between carpal and metacarpal bones of the thumb
All diarthroses are also synovial joints. The joint capsule creates a cavity between the two connecting bones which is filled with synovial fluid, to help lubricate and cushion the joint. The ends of the bones are cushioned by hyaline cartilage and the range of movement allowed depends greatly on their shape.
Knowing what your joints can do
You know that certain types of joints can perform certain kinds of movements. The movement of a body part — say, raising your hand — often has an opposing movement to return it to its original position, like putting your hand down in frustration when you don’t get called on. Here’s a quick overview of those special movements:
Abduction: Moves a body part to the side, away from the body’s middle. When you make a snow angel and you move your arms and legs out and up, that’s abduction.
Adduction: Moves a body part from the side toward the body’s middle. When you’re in snow angel position and you move your arms and legs back down, that’s adduction — you’re “adding” your body back together.
Flexion: Decreases the joint angle. When you flex to show off your biceps, you move your forearm to your arm, decreasing the angle at the elbow.
Extension: Makes the angle larger. Returning your arm from the flexed position increases the angle and the elbow and is, thus, extension. Hyperextension occurs when the body part moves beyond a straight line (180 degrees) like tilting your head back in exasperation.
Elevation: The upward movement of a body part, such as shrugging your shoulders.
Depression: The downward movement of a body part, such as the downward movement after shrugging your shoulders.
Eversion: Happens only in the feet when the foot is turned so the sole is facing outward.
Inversion: Happens only in the feet when the foot is turned so that the sole is facing inward.
Supination: Happens only in the arm, when the forearm is rotated to make the palm face upward or forward (think about holding a bowl of soup).
Pronation: Happens only in the arm, when the forearm is rotated to make the palm face downward or backward.
Rotation: The movement of a body part around its own axis, such as shaking your head to answer, “No.” The partnered motions are medial rotation (movement toward the midline) and lateral rotation (movement away from the midline).
Circumduction: The movement of a body part in circles, like doing arm circles in gym class.
Pathophysiology of the Skeletal System
Bones and joints are very strong, but they’re prone to injuries, the effects of aging, and disease, just like any other body part. This section gives you some information on a few of the most common problems that occur in bones and joints.
Abnormal curvature
Abnormal curvatures of the spine can cause plenty of pain and can lead to several problems. When the curve of the lumbar spine is exaggerated, the abnormal condition is lordosis, more commonly known as swayback. The lumbar spine of a pregnant woman becomes exaggerated because the woman needs to balance the pregnant belly on her frame. However, sometimes the curve remains after pregnancy, when weakened abdominal muscles fail to support the lumbar spine in its normal position. Developing the habit of holding the abdominal muscles in (rather than letting it all hang out, so to speak) helps to strengthen the body’s center and prevent swayback. Losing the beer belly helps, too.
Older men and women sometimes develop a condition called kyphosis (commonly known as hunchback), an abnormally curved spine in the thoracic region. Normal degeneration and compression of the vertebrae tends to straighten the cervical and lumbar regions of the spine and push out the thoracic vertebrae, thus causing kyphosis. Osteoporosis (see the next section) amplifies this.
You may recall being checked for scoliosis during junior-high gym class. The reason for that inspection is because scoliosis (abnormal lateral curvature) first becomes obvious during the late childhood/early teen years — just when people are most self-conscious. Normally, when you look at the spine from the back, it appears to be straight — the curvature is evident only when you view the spine from the side. However, in people with scoliosis, the spine curves side to side (laterally) and looks S-shaped when viewed from the back.
Osteoporosis
Osteoporosis is a disease in which bones become fragile, progressively and painlessly. To some extent, the process is inevitable with age, but when too much bone density is lost and small fractures appear, you have osteoporosis. The continuous process of bone resorption (osteoclasts breaking down the matrix) continues, but the osteoblasts (bone-building cells) become less and less active, so more bone is lost than replaced. Osteoporosis occurs most often in postmenopausal women because they lose the protective effect of estrogen on the bones.
Osteoporosis affects all bones, but of special concern are fractures of the hip and spine. A hip fracture almost always requires hospitalization and major surgery. It can impair a person’s ability to walk unassisted and may cause prolonged or permanent disability or even death. Spinal or vertebral fractures also have serious consequences, including loss of height, severe back pain, and deformity.
Cleft palate
A cleft palate is a relatively common birth defect that occurs when the palatine bones (a pair of the facial bones) or the maxilla bones fail to fuse during fetal development. This defect creates a problem in which the nasal cavity and oral cavity are open to each other. This problem can affect the palatine bones only or can be part of a syndrome of development problems. Cleft palate, also called hare-lip, is treated with surgery, usually when the child is very young.
Arthritis
Arthritis is a name for any of numerous conditions characterized by inflammation of the joints. The inflammation is painful in itself, and it also makes movement difficult and painful. The chronic inflammation can eventually erode the joint’s tissues (bone and cartilage). Treatment consists of controlling pain, reducing inflammation, and slowing the progress of joint damage.
Arthritis conditions are closely associated with immunity: Inflammation is a normal response of the immune system, but chronic inflammation of the joints is pathophysiological. Several arthritis conditions are autoimmune disorders. (See Chapter 13 for a discussion of autoimmunity.) Here are the common forms of arthritis:
Osteoarthritis (OA) is the most common form. As the joints age and the ravages of normal use accumulate, low-level inflammation sets in. Eventually, the inflammation causes the joint’s cartilage to become thinner and lose elasticity. It can affect people at any age. Many people develop some osteoarthritis of the finger joints in late middle age.
Rheumatoid arthritis (RA), an autoimmune condition, starts with inflammation of the synovium (joint lining). Later, often years later, the inflamed cells of the synovium begin to produce enzymes that actively destroy both bone and cartilage, restricting movement and increasing pain further.
Juvenile arthritis (JA), the most common form affecting children under 16, is an autoimmune condition. Most likely, JA is several different autoimmune conditions that vary in the number of affected joints and the age of onset. As with other forms of arthritis, the symptoms are inflammation, joint pain, and stiffness. Sometimes, JA causes the limbs to grow to different lengths.
Ankylosing spondylitis (AS) affects the spine and the sacroiliac joints. The severity of the pain and inflammation varies, but in its worst form, the chronic inflammation can cause the spine to fuse into a rigid, brittle column, prone to fracture. The eyes, heart, lung, and kidneys can also be affected.
Gout is a form of arthritis caused by crystallized deposits of uric acid in the joints. Think “sand in the gears.” As the uric acid crystals fill the joints, they damage cartilage, synovial membranes, tendons, and even the muscles adjoining the bone. Complications include kidney stones, nerve damage, and circulatory problems. Drugs are available that reduce the amount of uric acid in the blood, preventing its deposition in the joints.
Fractures
When bones absorb more force than they can handle, they break. Fractures are classified by the shape of the break, whether or not it spans the whole bone, and if breaks through the skin (called compound if it does; closed if it does not). Not all fractures are visible lines, though. Compression fractures, where the bone crumples but doesn’t literally break, are a common type of pathological fracture — those that have their root in disease (rather than trauma).
The body has its own fracture-repair process similar to remodeling, but key to proper healing is reduction (the correct realignment of the bone) and immobilization (which is maintained by applying casts or other equipment, such as plates or screws).
 Listing the functions of your skeleton
Listing the functions of your skeleton Keep in mind the difference between bone tissue and a specific, named bone. Both the femur (thigh bone) and the humerus (arm bone) contain bone tissue, but each bone has its own specialized configuration of the components of bone tissue.
Keep in mind the difference between bone tissue and a specific, named bone. Both the femur (thigh bone) and the humerus (arm bone) contain bone tissue, but each bone has its own specialized configuration of the components of bone tissue.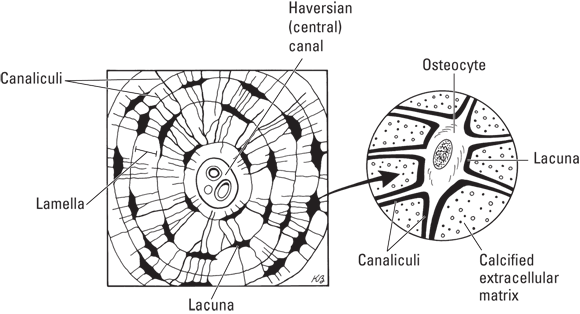
 There is a third type of cartilage: elastic cartilage. Unlike the other two types, it contains numerous elastic fibers, making it much more flexible. You can find elastic cartilage in your epiglottis and your external ear.
There is a third type of cartilage: elastic cartilage. Unlike the other two types, it contains numerous elastic fibers, making it much more flexible. You can find elastic cartilage in your epiglottis and your external ear.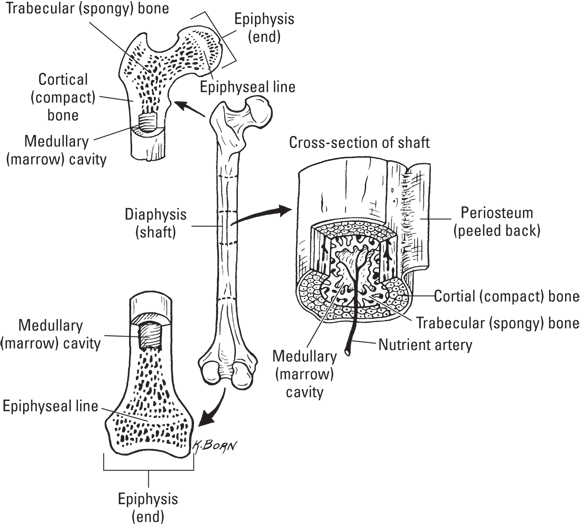
 You can differentiate these two important bones by recalling the Greek story about Atlas, who held the world on his shoulders. Your atlas holds your head on your shoulders. To remember the number of vertebrae in each region, think: breakfast, lunch, and dinner.
You can differentiate these two important bones by recalling the Greek story about Atlas, who held the world on his shoulders. Your atlas holds your head on your shoulders. To remember the number of vertebrae in each region, think: breakfast, lunch, and dinner.