Exploring immune system cells, molecules, and mechanisms
Looking at some immune disorders
Your lymphatic system is all that stands between you and a planetful of invasive microorganisms that regard you, metaphorically speaking, as a large serving of biological molecules that could feed their own processes. Your body calls on the immune processes of the lymphatic system to protect itself from invading microbes, such as bacteria and viruses, other foreign cells, and your own cells that have gone bad (such as cells that have become cancerous).
By this point, you may have wondered to yourself, “Where is the immune system?” That’s a valid question, especially because many people learn that the immune system is one of the 11 body systems. However, just as the circulatory system is now called the cardiovascular system (to shift focus to the heart and blood vessels) and the excretory system no longer exists (both the urinary and digestive systems perform the function of excretion), the immune system is now redefined as a subset of the lymphatic system. Immunity is a key function of the lymphatic system, but it’s not the only one. The lymphatic tissues play a vital role in circulation as well. We still have much to learn about this system. Case in point: It wasn’t until 2015 that we discovered a network of lymphatic vessels in the brain!
Functions of the Lymphatic System
The lymphatic system consists of a variety of components: a body-wide network of vessels and organs through which flows an important body fluid called lymph; a variety of very peculiar cell types; and several types of biological molecules, some of them just as peculiar. It drains and filters interstitial fluid (the fluid located outside of cells but within the tissues) and is the battleground for our immune defense.
Confronting marauders: Whether you’re well or ill, your immune system is always alert and active. That’s why none of the bacteria, fungi, parasites, and viruses that are present by the uncountable millions in the air you breathe, on surfaces you touch, and on your food, are eating you. Sure, you have lots of ways of keeping the invaders from entering your body in the first place. But disease organisms have evolved their own devious means to get past your defenses. (That’s why they’re “diseases” and not just “bugs.”) Plenty get through. When your immune system is functioning properly, most don’t stay for long. The immune system hunts them, destroys them, and wraps their cellular remains for elimination from the body.
Stopping renegades: The second major function of the immune system is to recognize and destroy cells of your own body that have “gone rogue” and have become potential seeds for cancerous growth. Cells go rogue every day. Most cancers can take hold only when the immune system malfunctions and fails to eliminate them, as happens with aging.
Loving Your Lymphatic System
The lymphatic system plays a crucial role in circulation by draining the fluids that pour out into the extracellular space during capillary exchange and returning them to the blood. The lymphatic system is more than a drainage network, though. It removes toxins, helps transport fats, and stabilizes blood volume despite environmental stresses. Possibly its most interesting functions are those related to its role in immunity, fighting biological invaders. To understand the extent of the lymphatic system, turn to the “Lymphatic System” color plate in the center of the book.
Lymphing along
In Chapter 9, you read about the cardiovascular system as a transportation network that brings substances to cells and takes their waste products away. In Chapters 8, 10, and 11, you find out how organ systems “make use of” the blood to distribute their anabolites to the target tissue. During capillary exchange, much of this cargo is pushed out through the walls of the capillaries: oxygen, ions, glucose and other nutrients, proteins, hormones, and so on, all in a watery solution. This section is about the watery solution.
The watery solution, called interstitial (extracellular) fluid, is the fluid in between cells, about 2 to 4 pints (1 to 2 liters) total volume at any given moment. (Interstitial means “in-between spaces.”) It is essentially the same fluid you met in Chapter 9, introduced as plasma, the fluid matrix of blood.
Like plasma, interstitial fluid is continuously flowing: The pressure of the heartbeat pushes this watery solution across the capillary walls and out into the interstitial space, a total of about 50 pints (24 liters) per day. Much of it is reabsorbed into the blood at the venous end of the capillaries. The rest goes on a detour through the lymphatic system. The fluid coursing through the lymphatic system is called lymph. After passing through the lymphatic system, the fluid rejoins circulation at the subclavian veins, and it is plasma again.
Plasma, interstitial fluid, and lymph are all the same watery solution of plasma proteins, electrolytes (ions), and various dissolved and undissolved substances. The fluid circulates around the body. The name it’s called by depends on where it is.
We need the fluid in our tissues, but we also don’t want it to remain stagnant. Plus, the volume that returns to the bloodstream at the capillaries is less than what was pushed out. If we didn’t drain it, excess fluid would gather, called edema. So, we continuously drain it, passing it through several filters before adding it back to the blood.
Structures of the lymphatic system
The structures of the lymphatic system resemble those of other organs and systems that function to move fluids around. The lymphatic system has its own tubes, pipes, connectors, reservoirs, and filters. It lacks its own pumping organ but, like venous circulation, makes use of skeletal muscle action for this purpose. Figure 13-1 is a schematic showing the lymphatic structures and their relationship to blood flow.
The lymphatic vessels are the tubes that carry lymph. They form a network very similar to the venous system. You could even think of the lymphatic system as an alternative venous system, because the lymph that the vessels transport comes out of the arterial blood and is delivered back into the venous blood. Like the venous system, the lymphatic system’s vessels start small (the lymph capillaries) and get larger (the lymphatic vessels), and even larger (the lymphatic ducts). Like veins, lymphatic vessels rely on skeletal muscle action and valves to keep the fluid moving in the right direction. The structure of the lymphatic vessel wall is similar to that of the veins, but thinner. Lymph vessels are distributed through the body, more or less alongside the blood vessels.
Lymphatic ducts
The largest of the lymphatic vessels, the lymphatic ducts, drain into two large veins. The right lymphatic duct, located on the right side of your neck near your right clavicle, drains lymph from the right arm and the right half of the body above the diaphragm into the right subclavian vein. The thoracic duct, also called the left lymphatic duct, which runs through the middle of your thorax, drains lymph from everywhere else into the left subclavian vein.
Lymph nodes
Lymph nodes are bean-shaped structures located along the lymph vessels (see Figure 13-2). Dense clusters of lymph nodes are found in the mouth, pharynx, armpit, groin, all through the digestive system, and other locations. Each lymph node is encapsulated (covered) by a fibrous connective tissue capsule. Afferent lymphatic vessels cross the capsule on the convex side, bringing lymph into the node. The node’s efferent vessel, which carries the filtered lymph out of the node, emerges from the indentation on the concave side of the capsule, called the hilum.
On the inside, the capsule sends numerous extensions that divide the node internally into structures called nodules. A nodule is filled with a meshlike network of fibers to which lymphocytes and macrophages (another immune system cell type) adhere. As the lymph flows through the node, pathogens, cancerous cells, and other matter in the lymph are engulfed and destroyed by macrophages targeted by lymphocytes. The cleaned-up lymph travels toward the venous system in the efferent vessels.
The lymph nodes also provide a safe and nurturing environment for developing lymphocytes. (See the “Lymphocytes” section later in the chapter.)
Lymph nodes are sometimes mistakenly called lymph glands. They don’t secrete anything, so they don’t meet the definition of glands.
Swelling and tenderness in the lymph nodes, especially of the pharynx, is a symptom of an infectious disease. Swollen lymph nodes (“swollen glands”) is not itself a disease or pathological condition. It’s the immune system doing its job.
The splendid spleen
The spleen is a solid organ, located to the left of and slightly posterior to the stomach. It’s roughly oval in shape, normally measuring about 1 by 3 by 5 inches (3 by 8 by 13 centimeters) and weighing about 8 ounces (23 grams). Essentially, its structure is that of a really large lymph node, and it filters blood in much the same way the lymph nodes filter lymph, removing pathogen cells along with exhausted RBCs and many kinds of foreign matter.
The spleen is enveloped by a fibrous capsule that extends inside creating chambers called lobules. It has a hilum, a spot where several different vessels cross the capsule. The spleen’s hilum contains the splenic artery, the splenic vein, and an efferent lymph vessel, a similar configuration to the lymph node. Note that the spleen has no role in filtering lymph (only blood) and no afferent lymph vessels.
Inside, the spleen is divided into functional subunits by outgrowths of the capsule’s fibrous tissue. Within each subunit, an arteriole is surrounded by material called white pulp — lymphoid tissue that contains lymphocyte production centers. Farther toward the outer edges of each compartment, similar masses called red pulp surround the arteriole. The red pulp is a network of channels filled with blood, where most of the filtration occurs. (It’s also the major site of destruction of deteriorating RBCs and the recycling of their hemoglobin.) Both white pulp and red pulp contain leukocytes that remove foreign material and initiate an antibody-producing process.
Give us a “T”
A T cell, that is. The thymus gland overlies the heart and straddles the trachea, sitting just posterior to the sternum. It produces thymosin, a hormone that stimulates the differentiation and maturation of T cells. (See the “Lymphocytes” section later in the chapter for more on T cells, and flip to Chapter 8 for more on hormones.) The thymus is relatively large in childhood; it decreases in size with age.
Identifying Immune System Cells
Immune system cells are special in many ways. In shape and size, they’re far from the compact epithelial or muscle cell types. Immune system cells have about a dozen distinctive shapes and many different sizes, and some have the ability to transform themselves into other, even weirder forms and to multiply extremely rapidly. See Table 13-1 for an overview of the different types of immune system cells.
40%–70% of total WBCs; first responders to infection site.
Basophil
Defense against parasites; mediates inflammation.
1% of total WBCs.
Eosinophil
Destroys antigen-antibody complexes.
1%–4% of total WBCs.
Monocyte
Matures into a macrophage, which phagocytizes bacteria and viruses.
4%–8% of total WBCs; largest of WBCs.
Macrophage
Phagocytizes pathogens and dead cells; stimulates the production of other WBCs.
Monocytes produce macrophages in large quantities in the early stages of the inflammation response.
B lymphocyte (B cell)
Produces antibodies.
Combined, B and T lymphocytes account for 20%–45% of total WBCs.
T lymphocyte (T cell)
Attack pathogen directly.
Ts and Bs can from memory cells for quick response if the pathogen returns.
NK cell
Destroys cancerous cells and cells infected by viruses.
Only lymphocyte involved in innate immunity.
Mast cell
Initiates inflammation response by releasing histamine at the site of injury.
Responds to allergens.
Over the past few decades, immunologists and cell biologists have discussed immune system cells in terms of several classification systems that have not held up well on further investigation. Forming and discarding theories and classification systems based on new knowledge is expected and welcome in immunology, as in any science. The structure and physiology of immune system cells will be under study for the foreseeable future. The following discussion of specific types of immune system cells gives you some idea about some established concepts. Keep this limited goal in mind, especially when checking out Table 13-1.
Our numerous immune cells are constantly patrolling our bodies, floating in the bloodstream, hanging out in the interstitial fluid, moving through the lymph, and some post up in the lymph nodes acting like guards checking everyone coming through a security gate. Most often, our bodies are able to destroy the pathogen before they can unpack their bags and start making us sick. This is the strategy of the innate immune system. If a pathogen makes it past our first line of defense — mechanical and chemical barriers (see the “Patrolling our borders” sidebar, earlier in this chapter) — we have a barrage of cells at the ready. All but the B and T cells fall into this category. If the pathogen is especially prolific or finds a good hiding place, we start to feel the characteristic symptoms of the infection. The battle is not lost, though, we have a secret weapon: the adaptive immune system. We enlist the B and T cells to mount a targeted attack on the pathogen, minimizing the collateral damage to our own cells that the innate strategies inevitably cause.
Looking at leukocytes
Immune system cells are called leukocytes (“white cells”), because they appear white in color under a microscope. Although all blood cells, red and white, develop from hematopoietic stem cells in the red marrow, the leukocytes contain no hemoglobin and no iron. Unlike RBCs, all leukocytes retain their nuclei, organelles, and cytoplasm through their life cycle. Fewer leukocytes are produced than RBCs, by a factor of around 700.
Also called white blood cells (WBCs), leukocytes are present everywhere and functioning at all times. You notice their presence in the acute phase of certain diseases — the immune response, not the invader directly, produces the well-known symptoms of flu. They function not only in the blood (really, in the plasma), but also in the interstitial fluid and the lymph. They’re never far from a site of injury or infection because they’re everywhere. When a splinter pierces your finger, a contingent of local WBCs arrives at the site instantaneously.
Sometimes it’s difficult to remember that these bizarre warrior cells with their amazing superpowers are your cells — are you — just like your skin cells and your blood cells. Discussing them is difficult without resorting to language that makes them seem like a quasi-military force from outside your body. These cells are acutely aware (metaphorically speaking) that “they” are “self” (you). In fact, that’s the primary distinction that matters to them: self or nonself. The overarching mission of a leukocyte is to protect self from other biotic (living) nonself, destroying the invaders when possible. They are necessary to establish more or less mutualistic relationships with other life forms as well (such as the beneficial bacteria living in our gut). It’s hard not to picture a disciplined army, but that’s a useful metaphor to remember when exploring the roles of the different leukocytes.
Lymphocytes
The lymphocytes are one group of leukocytes (WBCs) that includes the B cells, T cells, and NK cells. These cells work in conjunction with each other during infection — each using a different mode of attack. NK cells are the only ones in this category that are an innate strategy, attacking cancerous cells and cells infected by viruses. Once activated, B cells produce antibodies and some T cells directly attack pathogens. This is our adaptive strategy and is discussed in detail in the “Adaptive Immunity” section later in this chapter. The surfaces of lymphocytes are covered with receptors, which are molecules that fit with a specific antigen. (Check out the “Examining Immune System Molecules” section later in the chapter for an explanation of antibodies and antigens.)
All lymphocytes originate in the red marrow from the same type of hematopoietic stem cell. B lymphocytes and NK cells leave the marrow fully differentiated and enter the blood and lymph. T cells travel to the thymus gland to complete their differentiation in an environment rich in the hormone thymosin. Then they move to a lymph node, where they further differentiate into one of several different cell types, each with its own function in the immune response: helper T cells, cytotoxic (cell killing) T cells, or suppressor T cells.
Phagocytizing leukocytes
Several different types of WBCs utilize phagocytosis as part of their strategy, engulfing and digesting any foreign material. This strategy is discussed in further detail in the “Immune System Mechanisms” section.
Neutrophils
Neutrophils are the most numerous of the WBCs (40 percent to 70 percent of the total number) and are continuously present and active in the blood and lymph. Neutrophils squeeze through the capillary walls and into infected tissue, where they phagocytize the invading bacteria. They also utilize a chemical attack by a mechanism called degranulation, which we discuss in the “Immune System Mechanisms” section.
Neutrophils are the leading candidate for the Cell with the Shortest Life Span Award. They circulate for about a day and then undergo apoptosis (programmed cell death). If they’re signaled to an infection site, they function for another day or two, but that’s it.
Monocyte and macrophage
Monocytes aren’t really stem cells, but they have some functions in common with stem cells — they exist to produce other specialized cells on demand. Monocytes divide to produce two other kinds of immune cells, macrophages and dendritic cells. In a homeostatic state, the monocytes replenish these cells as necessary. In response to inflammation-response-related stimuli, monocytes travel to the site and begin to turn out vast numbers of its daughter cells.
Macrophages (literally, “big eaters”) are large phagocytic cells that target pathogens and dead self-cells. In the early stages of the immune response, macrophages initiate the mass production of other types of WBCs. Dendritic cells, along with macrophages, serve as the bridge between innate and adaptive immunity.
Examining Immune System Molecules
As noted earlier in the chapter, leukocytes are difficult to classify either by structure or by function because the structure and physiology of leukocytes are stupefyingly complex and astoundingly flexible. Most leukocytes, even those that phagocytize, also produce chemicals of many kinds that modulate the functional activities of many other cell types. Immune response involves a lot of cell-to-cell communication, and leukocytes make and use proteins, enzymes, hormones, and neurotransmitters. Some of these molecules are familiar from the physiology of other organ systems. Others are special creations of the immune system and have no other functions.
Histamine
Histamine is a nitrogen compound with several physiological functions but is best known for its role in local immune responses. Histamine is produced by basophils and by mast cells found in nearby connective tissues as part of the inflammatory response. It plays a major role in many allergic reactions because they get overstimulated. As part of the inflammation response, histamine dilates small blood vessels, activates the vascular endothelium, and increases blood vessel permeability to WBCs and inflammatory proteins. It also irritates nerve endings, leading to itching or pain.
The itchy bump on your skin after a mosquito bite is caused not by the bite but by the histamine that’s released to initiate the process by which the antigens that the mosquito introduced are destroyed. It’s also why scratching them makes the itch worse — you damage the surrounding tissue, leading to more inflammation!
Chemical defense
Numerous chemicals are produced by leukocytes to destroy a pathogen or to communicate with other immune cells. Table 13-2 contains a brief overview of some of these chemicals.
Gather pathogens together for more efficient phagocytosis
Cytokines
A group of chemicals, including interleukins, that communicate with the other immune cells
Defensins
Punch holes in the cell wall/membrane of pathogens; especially useful on bacteria
Interferons
Block replication of viruses and cancerous cells; stimulate other immune cells
Perforins
Poke tiny holes in cell membranes
Antigens
Antigens are molecules that stick out from the surface of a cell. They can be proteins, carbohydrates, or a combination of the two and come in a large variety of shapes and sizes. The term antigen is often confused with pathogen (for example, “WBCs attack the antigen”). Antigens, in fact, aren’t a bad thing at all — they’re actually essential. It’s like every living cell is always wearing its own, personalized hat, and that’s how we recognize them from non-self.
Antibodies
An antibody is a type of protein molecule with immune function that is made exclusively by B cells.
Antibodies, also called immunoglobulins (abbreviated Ig), are produced in activated B cells in response to the presence of a pathogen. Only a B cell that has a receptor that matches the pathogen’s antigen will be activated. It will then manufacture numerous antibodies that will only latch on to the specific pathogen for attack. The healthy human body has thousands and thousands of antibodies, each specific to one antigen, and is capable of producing large quantities of some of them on demand.
The membranes of lymphocytes are covered with receptors for thousands of different antigens, including antigens they haven’t encountered. When a B cell encounters a new antigen (a membrane receptor binds it), the B cell multiplies prodigiously and (almost) all the new cells are devoted to the production and release of antibodies specific to that antigen. The antibodies circulate, efficiently binding and disabling their target. The antigen-antibody complex calls in the phagocytes and may activate the complement system. To protect you from further infection, antibodies saturate your tissues.
B cells are manufactured with random receptor shapes in hopes that any pathogen we may encounter will have a matching B cell. Statisticians argue that the chances of our having a match are so astronomically high that it’s safe to say there’s one in our body somewhere. The problem is finding it before the pathogen does irreversible damage.
Antibody specificity
What makes one antibody specific to one antigen? In a word, shape.
Antibodies are proteins, and like those other useful proteins, the enzymes, they do their jobs by binding very tightly to a counterpart molecule of very specific configuration.
Antibody molecules are Y-shaped, with a binding site on each of the short arms. A binding site, in turn, has a specific and intricate shape. An antibody can bind only an antigen that has the complementary shape. A common metaphor for this is a lock-and-key mechanism: Just as a key has a specific shape and can fit only one lock, the antibody can bind only antigens that match its shape.
Antibody function
Antibodies work in three general ways: promoting inflammation, activating the complement system, and direct attack. Inflammation, in addition to bringing more WBCs to the area for battle, helps prevent the pathogen from moving elsewhere in the body. The complement cascade works to destroy the pathogen in numerous ways described in the next section. Antibodies’ direct attack has three effects:
Neutralization: Prevents the pathogen from binding to our own cells
Agglutination: Clumps numerous pathogens together for more efficient phagocytosis
Precipitation: Makes the antigens insoluble so it’s easier for a phagocytic cell to find and engulf it
IgG antibodies
Immunoglobin molecules come in five classes, named, with great imagination, IgA, IgD, IgE, IgG, and IgM. IgG antibodies are the most important class, accounting for about 80 percent of the antibodies. They’re the type most involved in the secondary immune response as they circulate in the blood and the other body fluids. IgAs are found in exocrine secretion (like tears and bile), while IgDs are found on the surfaces of B cells (forming the receptors). IgMs are specialized for blood compatibility, and IgEs promote inflammation. The overproduction of IgEs causes allergic reactions.
Complement system proteins
The complement system supports the activity of antibodies to clear pathogens. The system is composed of about 26 proteins. The process is similar in many ways to the clotting cascade in response to blood vessel injury (see Chapter 9). In fact, some of the very same proteins are involved.
The complement system must be activated by one of two very specific mechanisms, involving either antigen-antibody complexes, called specific immune response, or antigens without the presence of antibodies, called nonspecific immune response.
The recent and continuing development of technological tools for microbiology and molecular biology has permitted observations of the previously unimagined details of the immune system’s mechanisms. Our conceptual understanding of them follows a little behind. The following sections introduce you to the subtlety and complexity of immune system mechanisms.
Phagocytosis
Phagocytosis is the simplest of immune response mechanisms and probably older than multicellular life: The invader or foreign matter is just surrounded and digested. Phagocytosis is probably the body’s most frequently used mechanism, too, because the most numerous of the leukocytes, the neutrophils work this way. (Refer to the “Phagocytizing leukocytes” section earlier in the chapter.)
Degranulation
Various types of WBCs have granules in their cytoplasm. Granules aren’t chemicals but little packets of chemicals, such as histamine, cellular toxins (see Table 13-2), enzymes, and other proteins. Cell biologists have identified several different types of granules with very specific chemical contents.
A process called degranulation moves the granules out of the cell, releasing the chemicals into the interstitial space (via exocytosis; see Chapter 3). After they’ve been absorbed into the interstitial fluid, these chemicals carry out a range of specialized immune functions. Some destroy invaders directly. Some regulate immune system processes.
Granules in eosinophils play a crucial part in the immune response to enteric (intestinal) parasites through their release of toxic proteins (our own natural pesticides!). Eosinophil numbers increase during allergic reactions and parasitic infections. Eosinophils also perform a limited phagocytic function in the destruction and elimination of antigen-antibody complexes.
Neutrophils, discussed above as phagocytizing cells, contain granules in their cytoplasm that release many powerful substances. Because neutrophils are the most numerous of the WBCs, their granulocytic properties are very important in the immune response, especially to bacterial infection.
The degranulation of basophils releases histamine and heparin (an anticoagulant). This is a source of the histamine found at the site of inflammation and allergic reactions. Like eosinophils, basophils play a role in both parasitic infections and allergies.
Mast cells are present in most tissues, characteristically surrounding blood vessels and nerves, and are especially numerous near the boundaries between you and the outside world, such as in the skin and in the mucosa of the respiratory and digestive systems. Mast cells are granular cells that play a key role in the inflammatory process. When activated, a mast cell rapidly releases the contents of its granules and various hormonal mediators into the extracellular space. They’re involved in allergic reactions, anaphylaxis, and autoimmunity.
Inflammation is swell
The last time you got a thorn or a splinter in your hand or foot, you may have noticed that the site of entry became red, hot, swollen, and tender. These are signs and symptoms of an inflammation response. The inflammation response is a basic way the body reacts to infection, irritation, or injury, a mechanism for removing the injurious object and initiating the healing process. Inflammation has recently been recognized as a type of innate immune response.
When the splinter punctures your skin, the injured cells release mediator chemicals, particularly histamine and bradykinin, which initiate the inflammation response. Histamine also activates the complement system. The induction of the first complement protein stimulates the production of others, which stimulate still others, continuing in a rapid but controlled chain reaction until the full-blown inflammation response is raging. Immune system cells, mainly monocytes and other phagocytic cells, rush to the site to fight any microbes that were carried in on the thorn or entered through the skin opening.
When histamine is released, the chemical bradykinin is released along with it. Bradykinin causes the nerves to send pain messages to the brain. Thanks, bradykinin, we guess.
Adaptive Immunity
When the mechanisms of our innate immunity do not eliminate the pathogen, our adaptive mechanisms join in the battle. The trigger for this requires an antigen-presenting cell (APC); usually a macrophage or dendritic cell. When an APC comes across an unrecognized pathogen (meaning it has not been affected by any sort of immune response) it engulfs and digests it. However, it preserves the antigens and displays them on its own cell membrane. It then flows around our fluids hunting for a T cell that has a matching receptor, thus activating the adaptive immune response.
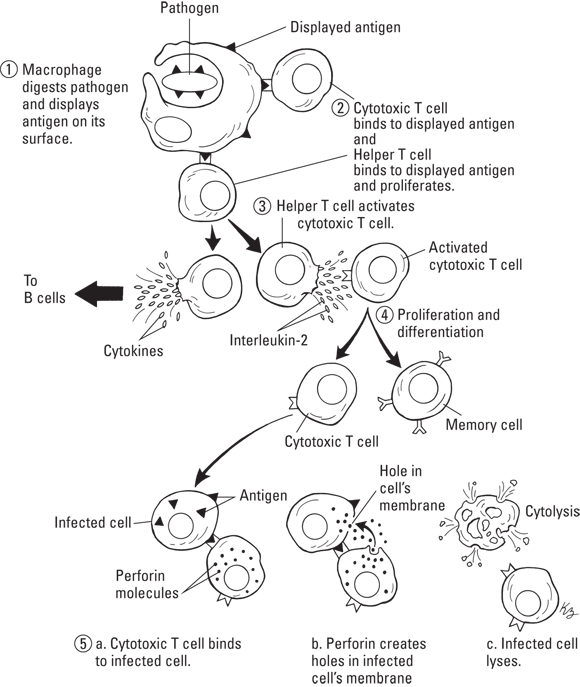
Cell-mediated immunity
The matching helper T cell that has just been sitting around waiting to be called into action now begins to proliferate (make a bunch of copies of itself). The new helper T cells release cytokines, which activate the matching cytotoxic T cells. This will then proliferate into an active cytotoxic T cell and a memory T cell (which won’t do anything at this point). The cytotoxic T cell will then bind to the antigens on the pathogens and release perforins to destroy it. This process is illustrated in Figure 13-3.
The T cell process, or cell-mediated immunity, creates an army of cells that will attack the pathogen that initiated the process. Their mode of attack is much like sending soldiers to the front lines to battle the enemy with weapons. It is especially effective for viruses and cancerous cells.
Humoral immunity
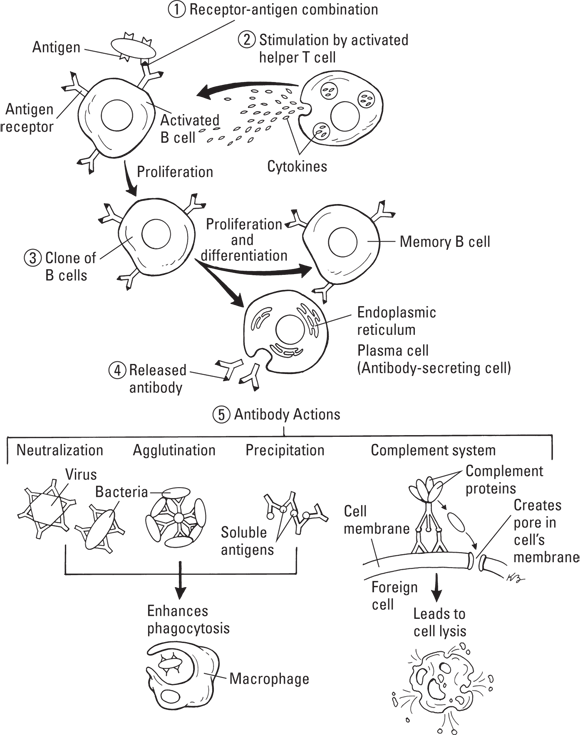
Humoral immunity, also called antibody-mediated immunity, is our adaptive defense that utilizes the B cells. It works in conjunction with (rather than after or instead of) the cell-mediated process. The strategy here, to continue the army metaphor, is to turn the B cells into bomb-making factories.
B cells will bind to the matching antigen of a pathogen, but until they’re activated, nothing else will occur. When the helper T cell releases cytokines during the cell-mediated process, they activate this bound B cell, leading to proliferation. The new cells become either memory B cells (which again, do nothing right now) or plasma B cells. The plasma B cells then go about their task of manufacturing antibodies. Figure 13-4 illustrates the process of humoral immunity.
Illustration by Kathryn Born, MA
FIGURE 13-4: Humoral immunity and antibody actions.
Secondary immunity
It’s the upside of infection and disease, at least some infections and diseases. After your immune system has dealt with certain pathogens, it produces the condition of immunity. Immunity is the condition of being able to resist infection by a particular pathogen because your body has defeated it before.
Both the cell-mediated and humoral mechanisms produce memory cells during the primary response. These cells hang out in your body, particularly in the lymph nodes, monitoring the fluid for their matching pathogen (with its matching antigen). Should these memory cells come across it, they reactivate and attack in their corresponding ways. Because this often occurs after exposure to the pathogen but before it can generate any symptoms, you’re immune to it.
Immunization
Immunization is the process of inducing immunity to specific antigens by inoculation. Inoculation is the introduction of an antigen into the body to stimulate the production of antibodies. The antigen is introduced, often by injection but sometimes orally or intra-nasally, in a preparation called a vaccine that contains a sample of the pathogen either killed or in an attenuated (alive but weakened) form. Essentially, vaccination induces a very mild primary response (so mild you may not be aware of it) so the secondary response can be activated rapidly when you encounter the antigen again in the environment. Researchers have developed vaccines for many infectious diseases and are developing more all the time.
Pathophysiology of the Immune System
Malfunction or failure in any part of the immune system is a threat to homeostasis and continued existence in any organism. But other animals just don’t have the same problems as humans do. The peculiarities of immune-related diseases in humans are due, in part, to human culture, which permits so many to survive to experience the age-related decline in immunity and requires continuous close contact between individuals that can sustain endemic or promote epidemic microbial diseases.
The immune system and cancer
Speaking of cancer as one disease is no longer possible, but all cancers are similar in that they represent a failure of the immune system to detect and destroy malignant cells. Often, the underlying cause of immune malfunction is simply the aging of the immune system. Malignant cells, by definition, divide and reproduce rapidly and in an uncontrolled way. The immune system destroys those cells as fast as it can. A young and vigorous immune system may eliminate all the malignant cells. Eventually, however, the immune system slows down and makes mistakes. A malignancy that arises may steadily gain ground and finally defeat it.
The immune-compromised patient is vulnerable to cancers of many kinds. The high incidence of an otherwise rare cancer called Kaposi sarcoma was among the first clues to emerge of the deadly new epidemic in the early 1980s and a strong clue that the target of the new virus was the cells of the immune system (see the “HIV and AIDS” section later in the chapter).
An organ transplant recipient must be on a regimen of immunosuppressant drugs his or her whole life. Besides other debilitating side effects, these drugs make the patient vulnerable to cancers of many kinds. Some patients suffering from autoimmune diseases are treated with immunosuppressants, too, and have the same vulnerability.
Immune-mediated diseases
Immune-mediated diseases are conditions that result from abnormal activity of the immune system. Autoimmune diseases are disorders caused by the immune system mounting an attack on its own cells. Allergy is, essentially, an overreaction of the immune system to a harmless substance in the environment.
Autoimmune diseases
Like a real-life horror movie, the awesome coordinated power that stands ready to engage any and all biological invaders in deadly combat instead attacks and destroys the body’s own tissues. Autoimmune diseases are an active area of basic and clinical research, but on a fundamental level, what causes the immune system to turn on its “self” remains obscure. In most cases, a combination of factors is probably at work. For example, a viral infection may activate (or deactivate the suppression of) a genetic error. Certain autoimmune disorders affect many more women than men, so hormone activity is probably a factor.
Autoimmune disorders are many and various in terms of the pathophysiology. An autoimmune disease can be relatively benign, like vitiligo, in which the immune system destroys melanocytes (pigment-making cells), resulting in white patches of skin on different parts of the body. Other autoimmune diseases are far more serious. They can affect any part of the body, including the heart, brain, nerves, muscles, skin, eyes, joints, lungs, kidneys, glands, digestive tract, and blood vessels. Clinical experts disagree among themselves about whether certain conditions should be classified and treated as autoimmune conditions. The list of “accepted” autoimmune disorders numbers several dozen, some of which we mention in other chapters of this book.
Allergy
An allergic reaction is acquired (brought about by exposure to a triggering substance called an allergen) and rapid. Mild allergies are common in all human populations. Severe allergic reactions can be life-threatening.
Exposure to the allergen causes IgE antibodies to set off an excessive activation of certain types of WBCs (mast cells and basophils), which release excessive histamine. Histamine causes swelling of mucous membranes, such as in the nose and throat. The swelling causes nasal congestion and that annoying itch in the throat. Congestion and swelling can trap bacteria in the nasal cavities and lead to sinus infections or ear infections. The inflammatory response can lead to such symptoms as eczema, hives, and hay fever. Allergies are a significant factor in asthma.
Anaphylaxis is a rapid, severe, whole-body allergic reaction. Anaphylaxis results from an acquired hypersensitivity to an allergen. An initial exposure, called the sensitizing dose, to a substance like bee sting toxin or a protein in a food, produces no symptoms but sensitizes the person’s immune system to the allergen. A subsequent exposure, called a shocking dose, sets off anaphylaxis. Anaphylactic shock is anaphylaxis associated with vasodilation (dilation of the blood vessels) over the whole body, which results in low blood pressure and severe broncho-constriction to the point where the person has difficulty breathing. Respiratory failure, shock, and heart arrhythmias can lead rapidly to death. The treatment is immediate administration of epinephrine. (Turn to Chapter 8 for information about epinephrine.)
Chronic inflammation
The inflammation response is an important mechanism in the body’s natural defense system against infection and disease. Chronic inflammation, on the other hand, is a disease. In chronic inflammation, the mechanisms that destroy invaders are turned on the body’s own tissues.
Even low-level inflammation, such as occurs in a moderate case of gingivitis, can cause problems, and not just at the inflammation site. The proteins of the inflammatory response and the complement system can travel in the blood and harm cells and tissues anywhere in the body. Chronic inflammation is now widely recognized as an underlying disorder that contributes to many and diverse conditions, including cardiovascular disease; neurological diseases such as clinical depression and Alzheimer’s; diabetes; many kinds of cancer; and even premature labor and preterm birth. The list of diseases and disorders that are now recognized to have an inflammatory component is getting longer all the time.
Infectious diseases
Some microbes not only commandeer your body for their own purposes; they use your body as a platform from which to launch invasions into the bodies of all your closest associates. This is a brief look at two different types of chronic infectious viral diseases.
HIV and AIDS
HIV is a species of virus that attacks cells of the human immune system, specifically the helper T cells. The immune system mounts a response, as it does to any other infection, and it may fight the virus to a standstill for years. But, as far as is known, the immune system is unable to eliminate the virus entirely. Like herpes viruses (see the next section), HIV hides out within cells. But as reactivated herpes viruses damage the nerve cells they hide out in, HIV damages the immune system cells, inhibiting the functioning of the immune system itself.
The diagnosis of acquired immune deficiency syndrome (AIDS) is made partly on the patient’s status regarding certain infections that a healthy immune system has no difficulty beating back (opportunistic infections). Eventually, the response to pathogens and malignant cells is inadequate, and the patient succumbs to an opportunistic infection, cancer, or other disease.
Herpes viruses
Herpes viruses are a leading cause of human viral disease, second only to influenza and cold viruses. People living to middle age usually have antibodies to most of the eight known human herpes viruses, whether or not they’re aware of having been infected.
The immune system is capable of suppressing the herpes viruses but not of eliminating them. After a patient becomes infected by a herpes virus, the infection remains in the body for life. Following the primary infection, the virus may migrate to the ganglia (nerve bundles) and establish a latent infection, which may reactivate at any stage. Reactivation is frequently, but not always, associated with further disease. Immunocompromised patients are at risk for serious disease and death from reactivated herpes viruses, which are prominent among the opportunistic infections that have been the actual cause of death in many AIDS patients.
The Varicella-Zoster virus, the herpes virus that causes chickenpox, is usually acquired in childhood (unless the child has been vaccinated), and more than 90 percent of the population of the United States carries antibodies. The virus is spread by respiratory aerosols (inhaled particles) or by direct contact with the skin lesions of an actively infected patient.
For several days following initial infection, the virus sits in the respiratory mucosa, where it infects macrophages and lung cells. At this stage, no symptoms appear. The virus spreads to lymphocytes and monocytes, and then to epithelial sites throughout the body. The virus reaches the surface of the skin, and lesions, typically hundreds, form on the skin and mucosa, usually most pronounced on the face, scalp, and trunk. The disease is more severe in older children and adults and can be very severe in immune-compromised patients.
Reactivation of the virus may occur in late life. The recurrence of viral replication is accompanied by severe pain in areas innervated by the latently infected ganglia. Symptoms include chronic burning, itching pain and increased sensitivity to touch (hyperesthesia) called post-herpetic neuralgia or shingles. The pain may last months or years. Reactivation can affect the eye and the brain via certain cranial nerves.
 Figuring out what the lymphatic system does
Figuring out what the lymphatic system does Plasma, interstitial fluid, and lymph are all the same watery solution of plasma proteins, electrolytes (ions), and various dissolved and undissolved substances. The fluid circulates around the body. The name it’s called by depends on where it is.
Plasma, interstitial fluid, and lymph are all the same watery solution of plasma proteins, electrolytes (ions), and various dissolved and undissolved substances. The fluid circulates around the body. The name it’s called by depends on where it is.

 Lymph nodes are sometimes mistakenly called lymph glands. They don’t secrete anything, so they don’t meet the definition of glands.
Lymph nodes are sometimes mistakenly called lymph glands. They don’t secrete anything, so they don’t meet the definition of glands.