Focusing on the liver, pancreas, and digestive fluids
Discovering some digestive system diseases
Just how does that pile of steak, potatoes, and salad on your plate become the tissues of your body? The digestive organ system gets it halfway there. (The cardiovascular system does most of the rest.)
Living systems constantly exchange energy. Physiological processes — anabolic, catabolic, and homeostatic — require energy. Ultimately, that energy comes from the light energy that plants use to transform carbon in the atmosphere (as CO2) into biological matter (as carbohydrates) in the process of photosynthesis. Humans get their energy by consuming this biological matter, either directly or by consuming other organisms that do. The digestive system takes apart this biological matter step by step and transforms it into a form that human cells can use. In this chapter, we explain the ins and outs of the process and the organs responsible for the chore.
Functions of the Digestive System
Digestion itself is a middle step. Other important functions of this organ system come before and after:
Ingesting: Although all animals ingest — take something into the body through the mouth — only humans, and possibly some of the great apes, appear to enjoy food as they ingest it.
As we discuss in Chapter 7, the perception of subtle flavors is more closely connected to olfaction than digestion. The perception of the five basic flavors is also considered neurosensory. Perception in the mouth is more about texture and is closely related to food’s protein and fat content. This concept is captured by the food industry term mouth feel. These sensory perceptions guide you in the selection of foods.
Sometimes, though, ingestion isn’t a feast for the senses — nothing delicious is available. The body still needs calories, though, so whatever’s available is chewed and swallowed just the same. (See the section “Starting with the mighty mouth” later in the chapter.)
Digesting: Eating is fun, and ingestion is bearable, but neither provides biological molecules that your cells can use. That task is accomplished by the interaction of physical and chemical forces. The digestive tract is a muscular tube lined with chemical factories that operate under the direction of their own dedicated neural structures and under hormonal control (see the upcoming section “Structures of the Digestive System”).
The digestive system processes everything down the same track, extracting fuel, biological molecules, and micronutrients from whatever you eat. (See the section “Moving through the intestines” later in the chapter.)
Exporting nutrients to the body: The end products of digestion are biological molecules such as glucose that are absorbed across the digestive membrane into the blood and then distributed in the body (see Chapter 9 for an overview of the cardiovascular system).
Eliminating: The elimination of digestive waste is part of digestion. Other organ systems have evolved to make use of the digestive system’s structures to eliminate metabolic wastes of other kinds. As they say, one big pile is better than two little piles.
The Alimentary Canal
The digestive tract, also called the alimentary canal (“alimentary” means food), or the gastrointestinal (GI) tract, is a tube through which ingested substances are pushed along for physical and chemical processing. The tube walls are made up of an outer fibrous layer, a muscular layer, a supportive connective tissue layer, and an inner layer (containing an epithelial lining), called the digestive mucosa. All the layers vary in thickness from one place to another along the digestive tract. The space inside the tube is the lumen, and its size varies, too.
The digestive system’s gross anatomy (no pun here) is comparable to that of an industrial smelter. Some structures bring in raw materials; other structures extract, process, and ship out specific substances; and still other structures export the unused part of the raw materials back into the environment. The body uses both mechanical and chemical mechanisms to break down the raw materials and export products to the larger system (the economy in the case of the smelter; the organism in the case of the intestine). These efficient systems are organized linearly — things keep moving along in one direction at a steady pace.
Strictly speaking, the lumen isn’t “inside” the body. Rather, the body itself is wrapped around a small piece of the environment — that is, the lumen. Neither the food that enters your mouth nor any of the partially digested substances that your digestive tract produces are inside the body, either. Fully digested biological molecules extracted from these substances and transformed into molecules that are usable by human cells cross out of the lumen and into the blood. At that point, they’re inside the body.
As you read about the organs that break down food to nourish your body, refer to the “Digestive System” color plate in the middle of the book to see where the organs are located.
Examining the walls of the digestive tract
The upper third of the esophagus contains skeletal muscle. Beginning in the middle third of the esophagus and extending to the anal sphincter, layers of smooth muscle comprise the digestive tract. This smooth muscle contracts in pulsating waves, pushing the lumen’s contents along in a single direction. This constant wave-like contraction is called peristalsis.
A mucous membrane lines the digestive system, running continuously from the mouth all the way through to the rectum. This membrane protects your digestive organs from the strong acids and powerful enzymes secreted in the digestive system. The membrane’s innermost cells (next to the lumen) are among those cells that are continuously replaced (see Chapter 2 for more on cell renewal).
The digestive mucosa secretes mucus to keep everything in the digestive tract moist, soft, and slippery, protecting the membrane and its underlying structures from abrasion and corrosion. The mucosa contains tissues and cells that secrete other substances as well, including gastric acid, hormones, neurotransmitters, and enzymes. The digestive mucosa also contains an extensive network of lymphatic tissue, as we discuss in Chapter 13.
The digestive mucosa takes an active role in the final stage of digestion. It delivers the products of digestion from the small and large intestine to the blood for distribution through the body. Every molecule that enters the bloodstream passes through the digestive mucosa.
The mucosa is continuous throughout the organs of the alimentary canal, but its structure varies. One important difference is in surface area. In the esophagus, the mucosa is smooth because its main role is merely transportation. In the small intestine, the mucosa is wavy, forming peaks called villi to increase the surface area; this provides more opportunity for absorption into the bloodstream despite the limited space.
Starting with the mighty mouth
Your mouth is the starting point of your digestive system, the gateway to your other digestive organs. Besides making eating a fun experience, your mouth (oral cavity) serves some important digestive functions.
Talking about your teeth and gums
Humans have 32 teeth — 16 on the top and 16 on the bottom. Your teeth begin mechanical digestion by tearing and grinding food into pieces small enough to swallow. They come in four basic types: incisors for biting, canines for tearing (especially meat), and premolars and molars for grinding.
The gingiva (gums) hold teeth in position, and a binding material called cementum embeds your teeth’s roots in your jawbone (see Figure 11-1). Blood vessels that run through the jawbone and up into the pulp of the tooth supply the teeth with blood. Dentin, a bonelike material, covers the pulp, and an extremely hard protective enamel covers the dentin.
Many jawbones have difficulty accommodating the last molar in each row of teeth. Typically, these wisdom teeth erupt far later than the other permanent molars, usually in mid to late adolescence, and often cause jaw pain and dislocation of other teeth. Quite often, they don’t erupt at all and remain “impacted” in the jawbone, which can also cause jaw pain.
Your tongue helps out
Your tongue is mainly skeletal muscle tissue. The muscle is covered on the upper surface by a mucous membrane, in which are embedded taste buds. (See Chapter 7 for more on taste buds.) The tongue muscles move the food around in your mouth to assist chewing. The mucus moistens and lubricates the bolus, the technical term for a mouthful of food in the process of being chewed.
Muscles attach your tongue to your skull bones, and a mucous membrane on the tongue’s underside attaches your tongue to the oral cavity floor. That stringy piece of membrane that you see when you touch your tongue’s tip to the roof of your mouth is the lingual frenulum.
The buccal membrane
The buccal membrane is that portion of the digestive mucosa that lines the inside of the mouth. Several salivary glands have ducts that course through the buccal membrane and secrete mucus and salivary amylase, a digestive enzyme, into the oral cavity. These glands often go into action before you take the first bite of your meal. A delicious aroma or even just the anticipation of eating something you enjoy can get those juices flowing.
The enzyme salivary amylase turns starch into sugar as you chew, beginning chemical digestion.
Pharynx and esophagus: Not Egyptian landmarks
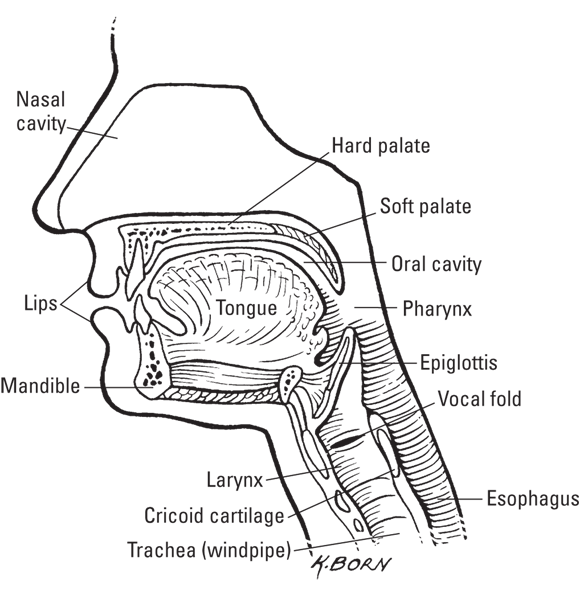
The pharynx, better known as your throat, leads to the esophagus, the tube that extends from the mouth to the stomach. When you swallow, the bolus bounces off a piece of cartilage called the epiglottis preventing entry into the trachea, routing it into the esophagus (see Figure 11-2).
The esophagus has two sphincters — one at the top and one at the bottom — that control the movement of the bolus into and out of the esophagus. The upper esophageal sphincter, composed of skeletal muscle, is usually contracted, keeping air out of the digestive tract. It opens to allow the bolus into the esophagus and peristalsis propels it along. The lower esophageal sphincter surrounds the esophagus just as it enters the stomach. It is also closed most of the time, preventing any stomach content from moving backward.
Stirring it up in your stomach
The outside of the stomach is a tough connective tissue layer called the serosa. Beneath the serosa is the muscular layer, which has three layers of smooth muscle fibers — oblique, circular, and longitudinal — that contract in different directions. Stretch receptors in this layer send nerve impulses to the brain when the stomach is full. These two layers support the structure of the stomach as a hollow organ.
When the lower esophageal sphincter relaxes, the bolus drops into the stomach, the widest and most flexible part of the alimentary canal. Food remains in the stomach about two to six hours, during which it’s churned in an acidic substance that the stomach secretes called gastric juice, ground up by thousands of strong muscle contractions. The muscular walls of the stomach contract rhythmically, similar to peristalsis, but propelling the food back and forth. The stomach is the only part of the alimentary canal that has a third muscle layer (oblique) to allow for the mixing movement. The “Stomach” color plate in the center of the book shows the various parts of the stomach.
The stomach lining has two mucosal layers, the submucosa and the mucosa. The submucosa contains nerves and blood vessels to provide control and resources to both the muscle and mucosal layers (this pattern is seen throughout the alimentary canal). Gastric glands in the mucosa secrete enzymes to break down large molecules, preparing them for absorption (see Table 11-1), as well as the other components of gastric juice. The mucosa is corrugated (like cardboard), increasing the surface area inside the hollow. The folds are called rugae. As the stomach fills, the rugae smooth out, allowing the stomach to expand.
The stomach’s muscular action is part of physical digestion, like chewing, swallowing, and peristalsis. Breaking the food up into smaller pieces is essential to allow access to all the nutrients; if it stayed in a big ball, we’d only be able to absorb the nutrients on the surface. But don’t overlook the stomach’s contribution to chemical digestion — it’s what really helps break down the food you eat.
As the stomach churns the bolus in the gastric acid, the material turns into an oatmeal-like paste called chyme. The chyme squirts into the small intestine through the pyloric sphincter, between the lower part of the stomach, called the pylorus, and the top of the small intestine, called the duodenum. This prevents too much of the chyme from entering at once.
Moving through the intestines
The intestine is a long muscular tube (up to about 20 feet, or 6 meters) that extends from the pyloric sphincter to the anal sphincter. How does 20 feet of tubing fit into a relatively small space that’s also crowded with other organs? It becomes narrow and convoluted. The intestines are classified as small and large based on their width, not their length (like hoses). The lumen of the small intestine is about 1 inch (2.5 centimeters) in diameter; the large intestine is about 2.5 inches (6.4 centimeters).
Overall, the intestine specializes in the import and export of biological substances of many kinds. As is usual for organs with import-export functions, the intestine has structures that maximize the surface area available for the exchange.
The intestine’s muscular outer walls lie coiled closely together within the abdominal cavity, held in place by the fibrous sheets of the peritoneum. With two layers of smooth muscle tissue, longitudinal and circular, the intestine specializes in strong, sustained peristalsis. Connective tissue between the curves of the small intestine, called mesentery, help prevent it from bunching up or kinking.
The intestinal mucosa is continuous with the rest of the digestive mucosa. It’s studded with specialized “work areas” that produce hormones, neurotransmitters, enzymes, and other substances integral to the digestive process.
The capillary beds found in the submucosa of the intestine define the interface of the digestive and cardiovascular systems. These capillaries are arrayed more or less continuously along the intestine’s lumen.
The lumen is lined by the villus (plural, villi), a structure that’s specialized for import and export processes and that’s characteristic of tissues in body locations where substances are exchanged. Villi are fingerlike projections of the mucosa that multiply the surface area available for exchange, much like wharves and piers extending into a harbor increase the area for harbor activities.
Villi line the entire length of the small intestine, projecting out into the lumen. Each villus has its own assigned capillary for absorbing materials from the intestine into the blood (flip to Chapter 9 for more on the cardiovascular system). Microvilli are even smaller projections on the epithelial cells of the mucosa.
Some of these processes require active transport — the expenditure of some energy in the form of ATP. For more on active transport and ATP, see Chapter 3.
Investigating the small intestine
The small intestine does a lot of the physical work of the digestive system, beginning with peristalsis. The small intestine is also majorly involved in digestive chemistry. It is an endocrine gland as well as a digestive organ, producing and secreting hormones that control digestion. Cells in the small intestine’s walls secrete the hormones secretin and cholecystokinin (CCK), which stimulate the release of digestive fluids such as bile from the gallbladder and pancreatic juice from the pancreas.
The small intestine is divided into three structures along its 10- to 20-foot (3- to 6-meter) length: the duodenum (about 1 foot long, or 0.3 meter), the jejunum (about 3 to 6 feet, or 1 to 2 meters), and the ileum (about 6 to 12 feet, or 2 to 4 meters). It is approximately 1 to 2 inches (2.5 to 5 centimeters) in diameter.
The small intestine can measure around 50 percent longer at autopsy because of the loss of smooth muscle tone after death.
The role of the duodenum is to complete chemical digestion. Brunner’s glands in its lining secrete mucus and bicarbonate directly into the lumen to help neutralize the gastric juice in the chyme (most enzymes require a near neutral pH). Other cells secrete digestive enzymes (refer to Table 11-1) that work with the bile and pancreatic enzymes to break the large molecules down into absorbable pieces.
The pyloric sphincter controls the release of chyme into the duodenum by the enterogastric reflex. The rate of flow is limited by the ability of the duodenum to neutralize the strong acid. The processes of chemical digestion run furiously. The carbohydrates, proteins, and fats are broken down into molecules such as glucose, amino acids, fatty acids, and glycerol. Peristalsis moves the almost-completely-digested chyme along into the jejunum and ileum, which are specialized for absorption.
The body handles the two products of fat digestion, fatty acids and glycerol, a bit differently. Short-chain fatty acids are shuttled directly to the capillary through the villus. Long-chain fatty acids are transported through the villus to the lymphatic system. In the cells, long-chain fatty acids are assembled into compounds called triglycerides. Glycerol is absorbed by the liver and is either converted to glucose or used in glycolysis (breaking down glucose into energy).
By the time the chyme works its way through all three parts of your small intestine, the nutrients that your body needs have been absorbed into the blood. At the ileum, the indigestible matter passes into the large intestine.
The work of the large intestine
Chyme oozes from the small intestine to the large intestine (also called the colon), passing out of the ileum through the ileocecal sphincter into the cecum, the first portion of the large intestine. The material is now called feces.
The large intestine is about 6 feet long (almost 2 meters) and is positioned anatomically like a “frame” around the small intestine. Beyond the cecum, the large intestine moves upward as the ascending colon, across as the transverse colon, and downward as the descending colon and finally into the sigmoid colon.
In the large intestine, water is reabsorbed from the feces by diffusion across the intestinal wall into the capillaries. Because electrolytes are dissolved in water, the large intestine functions to absorb those, too (but not nutrients). The removal of water compacts the indigestible material in the colon, and with the addition of mucus, forms the characteristic texture of the feces.
In addition to undigested food, the feces contain the remnants of digestive secretions like bile. The brown color of feces comes from the combination of greenish-yellow bile pigments, bilirubin (also from bile), and bacteria.
Your intestines are home to unimaginably large numbers of bacteria, including hundreds of species. Trillions of tiny (prokaryotic) cells ingest some of the undigested material in your feces, producing molecules that have a well-known odor. (It’s nothing to be embarrassed about, and nothing to be proud of, either.) Some of these bacteria produce beneficial substances like vitamin K, which is necessary for blood clotting. These substances are absorbed through the intestinal wall and transported into the blood via the capillaries. Check out Chapter 17 for more on microbes.
Passing through the colon and rectum
As the colon completes its work, peristalsis moves feces into the rectum, which is located at the bottom of the colon. Stretch receptors in the rectum signal to the brain the need to defecate (release feces) when the rectum contains about 5 to 8 ounces (142 to 227 grams). Pushed by peristalsis, the feces pass through the anal canal and exit the body through the anal sphincter.
Accessory Organs
The pancreas, liver, and gallbladder are often referred to as the accessory organs of digestion. They’re not part of the digestive tract; they never come into contact with ingested material, and they take no part in the mechanical aspects of digestion. They produce and make available to the digestive tract’s organs some of the chemical and biological substances that assist in digestion’s chemical aspects.
The liver delivers
The liver is one of the most important organs, not just in digestion but in many other functions. For example, it detoxifies the blood, metabolizes drugs, and regulates the supply of numerous molecules in the blood. The liver’s digestive function is the production and transport of bile, one of the digestive chemicals.
Many of the terms related to the liver’s structures and functions contain the prefix hepato-, meaning “liver.”
Liver anatomy
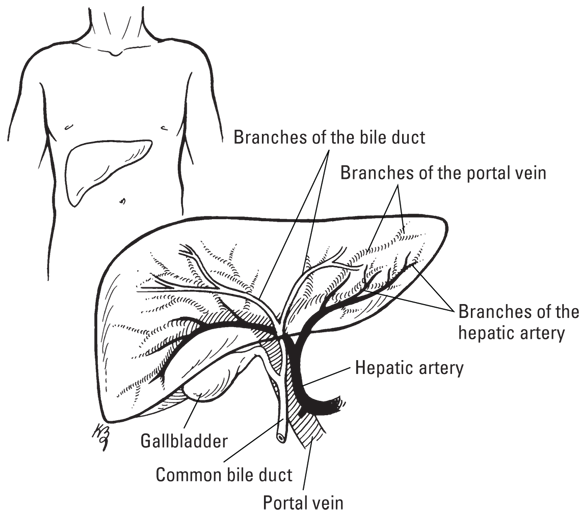
Your liver is both the largest internal organ and the largest gland in the human body. A healthy adult human liver weighs about 3 to 3.5 pounds (1.4 to 1.6 kilograms). It’s located under your diaphragm and above your stomach on the right side of your abdomen (see Figure 11-3). The liver is soft, pinkish-brown, and triangular, with four lobes of unequal size and shape: the right lobe, left lobe, quadrate lobe, and caudate lobe. The liver is covered by a connective tissue capsule that branches and extends throughout its insides, providing a scaffolding of support for the afferent blood vessels, lymphatic vessels, and bile ducts that traverse the liver.
The liver receives oxygenated blood through the hepatic artery, which comes from the aorta. It receives nutrient-rich blood through the portal vein, which carries blood from the capillaries of the digestive tract. This hepatic portal system allows the liver to process everything absorbed from the digestive system. Three hepatic veins drain deoxygenated blood from the liver, exiting the liver at the top of the right lobe and draining into the inferior vena cava.
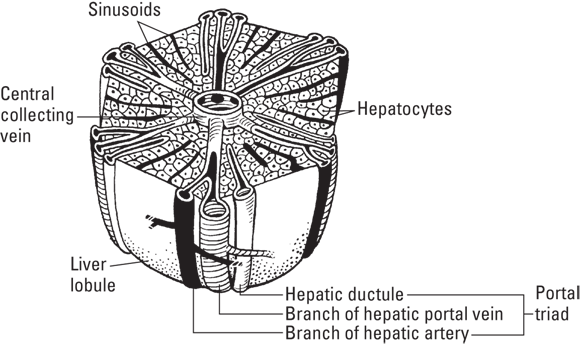
Each of the four lobes is made up of tiny lobules, about 100,000 of them in all. The hepatic lobule is the liver’s functional unit (see Figure 11-4). Each lobule is made up of millions of hepatic cells and bile canals and is supported and separated by branches of the capsule. At the lobule’s vertices (peaks) are regularly distributed portal triads that contain a bile duct, a terminal branch of the hepatic artery, and a terminal branch of the portal vein. The hepatocytes are in a roughly hexagonal arrangement, with a vein in the center that carries the lobule’s products out into the blood. On the surface of the lobules are ducts, veins, and arteries that carry fluids to and from them.
Among its other astounding powers, the liver possesses the ability to regenerate and regain its original size, structure, and function rapidly after partial resection surgery (removal) or massive injury. The human liver can fully regenerate from as little as 25 percent of its original tissue. This ability is unique among the major organs.
Live-donor transplantation, a procedure in which a healthy person donates a portion of his or her liver to a recipient whose liver is failing, has been performed successfully since 1989. Typically, the liver doubles in size in both the donor and recipient within only three to four weeks. Rapid replication of hepatocytes is the mechanism of growth.
Bile production and transport
The liver produces bile, a major factor in the digestion of fats and lipids of all kinds. The bile that some of the lobules produce is collected in bile canaliculi, which merge to form bile ducts. The intrahepatic (within the liver) bile ducts eventually drain from the liver through the common hepatic duct.
Bile can be released into the duodenum from the liver, but most often it heads to the gallbladder for storage. Your gallbladder is a pear-shaped sac tucked into the curve of your liver whose only function is to store bile and deliver it on demand to the small intestine. Bile both enters and leaves the gallbladder through the cystic duct. The cystic duct joins with the common hepatic duct to form the common bile duct, which releases bile into the duodenum.
Other functions of the liver
The liver functions in many other ways, affecting other organ systems. Here’s a brief overview of its many functions:
It processes and eliminates toxins. Toxic byproducts of some drugs, including alcohol, and other substances arrive from the digestive organs through the portal vein.
It processes and eliminates metabolic waste. The liver removes dying red blood cells from the blood and converts the hemoglobin to bilirubin and other byproducts. These are used to form bile. (The iron is recycled.)
It stores glucose in the form of glycogen and reconverts it when blood glucose levels get low. This function is mediated by insulin and glucagon. (Turn to Chapter 8 for more on the endocrine system.)
It stores vitamins and minerals.
It produces many kinds of protein, including protein hormones, the plasma proteins, and the proteins of the clotting cascade (see Chapter 9) and the complement system (see Chapter 13).
Pancreas
The pancreas sits in the abdominal cavity next to the duodenum and behind the stomach. We discuss the endocrine function of the pancreas in Chapter 8. The pancreas produces pancreatic juice, which is full of pancreatic enzymes, in response to CCK from the small intestine. Refer to Table 11-2 for information about pancreatic enzymes. Cells in the pancreas called acinar cells secrete pancreatic juice and passes it through the pancreatic duct into the duodenum. Cells along the pancreas’s internal ducts secrete bicarbonate (which is alkaline) in response to secretin (from the small intestine) to neutralize the acidic chyme.
Each part of the digestive system has its characteristic fluid, each a complex mixture of water, electrolytes, and biological substances with a specific role in digestion.
Mucus: Every inch of the digestive tract has mucus glands whose secretions keep everything in the digestive tract moist, soft, and slippery as well as protecting the lining from abrasion and corrosion.
Saliva: Saliva (or spit) is a clear, watery solution that the salivary glands produce constantly in your mouth. You produce about 2 to 4 pints (1 to 2 liters) of spit every day. Saliva moistens food and makes it easier to swallow. It’s also a component of the sense of taste — a food substance must be dissolved in the watery solution for its chemical signals to act on your taste buds (see Chapter 7).
Enzymes in saliva start starch digestion even before you swallow food. The combination of chewing food and coating it with saliva makes the tongue’s job a bit easier — it can push wet, chewed food toward the pharynx (throat) more easily.
Saliva cleans the inside of your mouth and your teeth. The enzymes in saliva also help to fight off infections in the mouth.
Enzymes: Thousands of enzymes are involved in digestion. Enzymes are specialized in their function — a given enzyme typically catalyzes one or only a few specific reactions. Digestive enzymes specialize in reactions that take specific molecules apart into component chemical entities. They can be broadly classified as proteinases and peptidases, lipidases, and various kinds of carbohydrate-active enzymes. Enzymes are part of the digestive fluids gastric juice and pancreatic juice.
The suffix –ase indicates an enzyme that breaks a molecule apart.
Gastric juice: Gastric juice is secreted from millions of tiny gastric glands in the gastric mucosa and enters the hollow of the stomach through gastric pits on the mucosa’s inner surface. Gastric juice contains hydrochloric acid (HCl), which is extremely acidic and kills bacteria that may have entered the body with food. It also contains the powerful proteinase pepsin, which can work only in this highly acidic environment.
Pancreatic juice: Pancreatic juice contains many types of digestive enzymes. Refer to Table 11-2 for some details.
Bile: Bile, also called gall, is a very alkaline, bitter-tasting, dark-green to yellowish-brown fluid produced by the liver. Bile may remain in the liver or be transported to the gallbladder for storage before being expelled into the duodenum.
The physiological function of bile is to emulsify fats — that is, to create an environment in which lipid-based substances can be mixed in a watery matrix for transportation and to make them available for chemical reactions to break them down. Bile’s high alkalinity helps neutralize the strongly acidic chyme that comes into the duodenum from the stomach. Another purpose of bile is to help absorb the fat-soluble vitamins K, D, and A into the blood.
The color of bile comes from the bilirubins and biliverdins that come from red blood cells (RBCs) dismantled in the liver. These pigments are deposited in the bile for elimination through the digestive tract. They play no part in chemical digestion, though recent research seems to support a role as antioxidants.
Hormones: The hormone gastrin regulates the secretion of HCl, mucus, and pepsinogen (which is turned into pepsin). As long as gastrin is flowing, your stomach continues to secrete gastric juice.
Cells in the small intestine’s walls secrete the hormones cholecystokinin (CCK) and secretin, which stimulate the release of bile and pancreatic juice.
Buffers: To lower the extreme acidity (raise the pH) of gastric acid and create a more hospitable environment for most digestive enzymes, the small intestine and the pancreas secrete sodium bicarbonate, the same compound found in baking soda.
Pathophysiology of the Digestive System
This section gives you some info on several common diseases and disorders of the digestive system.
Diseases of the oral cavity
Bits and pieces of food that remain in the mouth promote the growth of the normal bacteria present in the mouth. The bacteria in the mouth make themselves right at home, secreting a gelatinous matrix called a plaque into the spaces between the gingiva (gums) and the teeth. Within about a day, the secreted material hardens into calculus or tartar (both terms mean, basically, “hard stuff”). The accumulation of plaque and the overgrowth of the bacteria cause gingivitis (inflammation of the gingiva). Gingivitis is a major factor in tooth loss. Many otherwise healthy people live with this chronic, low-level inflammation, a risk factor for cardiovascular and other diseases, as we discuss in Chapter 13.
Over time, the acid byproducts of the bacteria’s metabolism erode the teeth’s enamel, creating a “cavity.” If the erosion continues, pathogenic bacteria can make their way into a tooth’s pulp, a condition called a tooth abscess.
Disorders of the stomach and intestines
The stomach and intestines take food in one end and push it out toward the other, with potential for trouble at every point along the way.
Constipation
Constipation results when the large intestine absorbs too much water out of the feces, which makes the feces dry, hard, and a bit painful on exit. Almost everyone experiences constipation at one time or another, and some people suffer chronic constipation. Underlying causes can be dietary (generally, too little fiber or too little water), a lack of exercise, certain foods and beverages, certain drugs, or the slowing of intestinal activity that can come with aging. The most common cause of constipation is ignoring your body’s signal to defecate. The feces remain in the colon too long, and too much water is absorbed into the intestinal lining, drying out the feces.
Diarrhea
An excessive amount of water remaining in the feces causes diarrhea. Something is preventing a normal amount of water from being absorbed through the large intestine and back into the blood. Although a bout of diarrhea is merely an inconvenience to adults in the developed world, it’s a major health concern in developing countries, particularly for children. Each year, diarrhea kills 1.5 million children around the world, and it’s one of the most common causes of death of children under 5 years old, according to the World Health Organization.
One possible cause of diarrhea is pathogenic bacteria that infect the large intestine (not the beneficial bacteria that normally inhabit the large intestine) through contaminated food. The rate of peristalsis increases in an attempt to eliminate the pathogen quickly, without the water being reabsorbed.
Another cause of diarrhea is stress, working through the hormonally driven mechanisms of the flight-or-fight response (see Chapter 8). Among the effects of adrenaline, the most important hormone in this mechanism, is the stimulation of peristalsis. In life-threatening situations, or those perceived as life-threatening, the lower intestines may expel their contents suddenly, presumably to jettison unproductive weight and permit faster running or harder fighting.
However, chronic stress can stimulate the chronic release of adrenaline, moving feces out of the large intestine too fast, impairing the reabsorption of water, and causing chronic diarrhea.
Appendicitis
Your appendix is a little sac attached to the cecum at the beginning of the large intestine. During the transfer of chyme from the small intestine to the large intestine, some material may flow into the appendix. Normally, this material makes its way out. But if it doesn’t come out, depending on the material and how long it remains, the appendix can become inflamed or infected by intestinal bacteria, causing appendicitis. Fortunately, appendicitis is severely painful; the nature and location of the pain is diagnostic for the condition. (Figure out where your appendix is, just in case. This life-threatening condition is quite common and is always a medical emergency.)
In the worst case, or if left too long untreated, the appendix swells and bursts. The boundary between the large intestine and the peritoneum is breached, causing life-threatening peritonitis and shock.
Gastric and duodenal ulcers
Gastric or duodenal ulcers are lesions in the mucosa of these tissues. Breaks in the thick protective mucus layer permit the highly acidic gastric juice to contact the lining’s cells, causing pain and further tissue damage.
For many years, emotional stress was considered to be the underlying cause of ulcers. Physicians and physiologists reasoned that the parasympathetic nervous system of a person under stress sent signals to secrete more gastric juice than was needed, leading to excess acid. A large industry was built around gastroenterologists prescribing antacid drugs to ulcer patients. Then, in the late 1980s, a group of Australian physicians and researchers demonstrated that these ulcers were the result of a bacterial infection. The species Helicobacter pyloris (translation: screw-shaped rod in the stomach) is moderately infectious and is present in many people; but when paired with excess acid, the bacteria are able to penetrate the mucous layer and embed in the epithelium. (They move through the mucus and embed in the epithelium by twisting, like a screw. In most stomachs, they don’t make it past the mucus layer.) A standardized antibiotic regimen is usually successful in eliminating the infection; the ulcers resolve as the mucosal lining is continuously replaced.
Bowel syndromes
Bowel syndromes are of two types: noninflammatory and inflammatory. We discuss both types in the following sections.
Irritable bowel syndrome (IBS)
In irritable bowel syndrome (IBS), irritation of the tissues results in a change in peristalsis. The rhythm of peristaltic contraction may either speed up or slow down. The patient may suffer diarrhea, constipation, or both. Stress reduction and a high-fiber diet usually are in the treatment plan. IBS is characterized as noninflammatory because autoimmunity and the inflammation response aren’t induced.
A syndrome is a collection of symptoms rather than a disease.
Crohn’s disease
Crohn’s disease is an inflammatory bowel disease, meaning that the intestinal lining becomes inflamed. (The inflammation response is part of the syndrome.) The mucosal layer, the muscular layer, the serosa (the covering tissue), and even the lymph nodes and membranes that provide blood supply to the intestine can be affected. As the intestinal lining swells, ulcers, fissures (cracks), and abscesses (pus-filled pockets) can form. Crohn’s can affect any part of the alimentary canal but is most common in the ileum.
In the disease’s early stages, sufferers have diarrhea and pain in the lower right side of the abdomen. The inflammation can spread through layers of the wall, which narrows the hollow space inside the intestine.
Crohn’s sufferers can develop nutritional deficiencies because of poor nutrient absorption. Usually, people with Crohn’s lose some beneficial intestinal bacteria, including those that synthesize vitamin B12. This chronic deficiency can lead to a condition called pernicious anemia.
Unfortunately, the cause is still unknown. But, treatment for Crohn’s includes dietary changes, rest, stress reduction, vitamin supplements, and medications to reduce inflammation and pain. Surgery sometimes is necessary to remove the affected portion(s) of the intestine.
Ulcerative colitis
Ulcerative colitis (colitis is inflammation of the colon) is a fairly common inflammatory bowel disease in which the intestinal lining becomes inflamed. (The inflammation response is part of the syndrome.) Although the symptoms are similar to Crohn’s, ulcerative colitis is limited to the colon and affects only the mucosa. Ulcers form in the lining of the large intestine, and the resulting inflammation leads to the production of a lot of mucus and pus. Abscesses can form in the lining, and the tissue surrounding them can become irritated, or damaged, or die. Ulcerative colitis can become a life-threatening condition.
Because of all this damage, the feces are often filled with blood and mucus. If the blood loss is severe enough, anemia (relative lack of red blood cells) can develop. As the disease progresses, the colon’s lining thickens and develops scar tissue, so absorption of water and electrolytes is reduced.
The cause of ulcerative colitis is under study. A problem with T lymphocytes appears to negatively affect the epithelial lining of the colon. Sometimes an infection may start the process. Although stress doesn’t cause ulcerative colitis, it can bring on an attack.
Diseases of the accessory organs
The organs producing digestive chemicals are subject to the malfunction of the powerful chemicals they themselves produce, as well as to infectious diseases, nutritional deficiencies, and imbalances originating in other organ systems. Malfunction in any of these organs can have far-reaching effects in physiology.
Systemic symptoms of liver disease
Because the liver has so many important functions in physiology, malfunction of this large organ can show up as signs and symptoms in other organ systems.
When the liver has failed, the bilirubin from aged RBCs isn’t eliminated properly from the body. Some may be deposited in the skin, where it causes intense itching, the most commonly reported symptom of liver failure. Yellow coloration of the sclera (whites) of the eyes is a well-recognized sign of liver disease, from which the common term jaundice (yellowing) is derived. The bilirubin may enter the urine at the kidney, giving the urine a dark color diagnostic of liver problems. The feces are pale because the metabolite of bilirubin that gives feces their brown color isn’t being produced and delivered to the large intestine.
Among the proteins made in the liver are most of the components of the clotting cascade (see Chapter 9) and those of the inflammation cascade (see Chapter 13). Impaired production of these proteins can result in bruising and excessive bleeding. Decreased concentrations of plasma proteins, especially albumin, soon brings on edema (fluid retention) in the abdomen, legs, and feet. A general loss of nutrients may result in chronic fatigue.
The liver is capable of considerable self-regeneration. These problems may self-correct by homeostatic mechanisms when the cause of the liver malfunction is eliminated.
Viral hepatitis
An inflammation of the liver is called hepatitis. Among the most common causes of hepatitis are the viral infections commonly named “hepatitis viruses A through E,” in order of their scientific discovery. The study of hepatitis viruses is an area of active biomedical research, and more hepatitis viruses may be identified and named. The viruses themselves aren’t related, but they all produce a similar set of symptoms. In the prodromal stage (immediate onset of infection, lasting about two weeks), the afflicted suffer from a sick feeling known as generalized malaise, as well as nervous system problems such as an altered sense of taste or smell, or light sensitivity. In the clinical stages, the liver is inflamed and enlarged, leading to abdominal pain, tenderness, indigestion, and accumulation of bilirubin.
The immune system discovered eons ago what medicine became aware of only recently: These viruses are all different. The immune system produces specific immunoglobulins (antibodies) against each virus. Some advanced diagnostic tools used in clinical diagnosis and public health identify the virus by identifying exactly which viral antibodies are present in the patient’s blood.
Some of the viruses that infect the human liver have effectively resisted the efforts of the immune system to eliminate them. Chronic infection can bring long-term morbidity, including extensive scarring of the liver, and early death.
You’ve got gall (stones)
Gallstones start as crystals of cholesterol or bile pigments forming in the gallbladder. Like pebbles in a jar, they reduce the gallbladder’s storage capacity. Worse, they can block the common bile duct, causing bile pigments to back up into the blood, a condition called obstructive jaundice. A laparoscopic laser technique called lithotripsy can obliterate the gallstones.
Painful pancreatitis
Inflammation of the pancreas (pancreatitis) may be mild or severe, acute or chronic. Pain associated with mild pancreatitis is centered around the navel and doesn’t lessen with vomiting. In severe pancreatitis, the pain is an unrelenting, piercing pain in the middle of the abdomen.
Acute pancreatitis can easily go on to become a condition called edematous pancreatitis (fluid accumulation) or a condition called necrotizing pancreatitis (death of cells and tissues in the pancreas). The cause of both is the same: Digestive enzymes produced in the pancreas are blocked from exiting into the intestine. Inflammatory changes in the ducts usually underlie the blockage.
Without the enzymes, digestion may slow or be incomplete, which may harm the body’s ability to maintain homeostasis. But worse, if the condition persists, the digestive enzymes are eventually turned loose on the tissues of the pancreas itself, destroying the body’s ability to produce and deliver the digestive enzymes ever again. Unlike the liver, the pancreas does not regenerate.
Sometimes, a bout of pancreatitis impairs the body’s ability to produce insulin, and diabetes results. (Turn to Chapter 8 for more on diabetes.)
 Explaining what the digestive system does
Explaining what the digestive system does Strictly speaking, the lumen isn’t “inside” the body. Rather, the body itself is wrapped around a small piece of the environment — that is, the lumen. Neither the food that enters your mouth nor any of the partially digested substances that your digestive tract produces are inside the body, either. Fully digested biological molecules extracted from these substances and transformed into molecules that are usable by human cells cross out of the lumen and into the blood. At that point, they’re inside the body.
Strictly speaking, the lumen isn’t “inside” the body. Rather, the body itself is wrapped around a small piece of the environment — that is, the lumen. Neither the food that enters your mouth nor any of the partially digested substances that your digestive tract produces are inside the body, either. Fully digested biological molecules extracted from these substances and transformed into molecules that are usable by human cells cross out of the lumen and into the blood. At that point, they’re inside the body.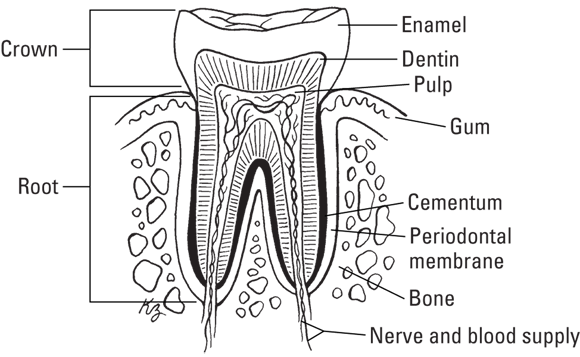
 The stomach’s muscular action is part of physical digestion, like chewing, swallowing, and peristalsis. Breaking the food up into smaller pieces is essential to allow access to all the nutrients; if it stayed in a big ball, we’d only be able to absorb the nutrients on the surface. But don’t overlook the stomach’s contribution to chemical digestion — it’s what really helps break down the food you eat.
The stomach’s muscular action is part of physical digestion, like chewing, swallowing, and peristalsis. Breaking the food up into smaller pieces is essential to allow access to all the nutrients; if it stayed in a big ball, we’d only be able to absorb the nutrients on the surface. But don’t overlook the stomach’s contribution to chemical digestion — it’s what really helps break down the food you eat. Many of the terms related to the liver’s structures and functions contain the prefix hepato-, meaning “liver.”
Many of the terms related to the liver’s structures and functions contain the prefix hepato-, meaning “liver.”