The glands of the endocrine system and the hormones they release influence almost every cell, organ, and function of your body. The endocrine system is instrumental in regulating mood, tissue function, metabolism, and growth and development, as well as sexual function and reproductive processes.
In general, the endocrine system is in charge of body processes that happen slowly, such as cell growth. The nervous system controls faster processes like breathing and body movement. Throughout this chapter, you can see that the nervous system (which we cover in Chapter 7) and the endocrine system work closely together. The nervous system controls when the endocrine system should release or withhold hormones, and the hormones control the metabolic activities within the body. This chapter explains the functions of hormones, the glands that they come from, and common disorders of the endocrine system.
Homing In on Hormones
A hormone is an endogenous substance (one that’s produced within the body) that has its effects in specific target cells. Hormones are many and varied in their source, chemical nature, target tissues, and effects. However, they’re characterized by the fact that they’re synthesized in one place (gland or cell) and they travel via the blood until they reach their target cell. Hormones are bound by specific receptors on (or in) their target cells. The binding of the hormone on the receptor induces a response within the cell.
Among glands, the pituitary, thyroid, and adrenal glands are most well-known. These organs have no significant function other than to produce hormones. However, a number of other endocrine tissues and hormones, though less well-known, are just as important in controlling vital bodily functions. In fact, all the tissue in your body is, in some way, an endocrine tissue.
Hormones play a big part in homeostasis (see Chapter 2). When the blood passes certain checkpoints in the nervous system (such as the hypothalamus inside the brain), hormone levels are “measured.” If the level of a certain hormone is too low, the gland that produces that hormone is stimulated to produce more of it. If a hormone level is too high, the gland that produces the hormone either doesn’t receive any further hormonal stimulation or is “instructed” to stop or slow production. The hormone comes from the endocrine system, but the “instruction” comes from the nervous system.
Your body is always keeping tabs on the metabolic processes going on inside it. If your body temperature, glucose level, or pH level leaves the normal range, the checkpoints involved in homeostasis work with the endocrine system to bring your systems back into balance.
The following sections guide you through how hormones are structured chemically, where hormones come from, and how hormones work.
Hormone chemistry
Chemically, hormones fall into three types: those derived from lipids, from peptides, and from amines.
Lipid hormones: Lipid and phospholipid hormones are derived from fatty acids. The best-known lipid hormones are the steroids, such as estrogen, progesterone, testosterone, aldosterone, and cortisol, which are synthesized from cholesterol. Another group of lipid hormones is called prostaglandins.
Peptide hormones: Peptides are relatively short chains of amino acids. Peptide hormones include antidiuretic hormone (ADH), thyrotropin-releasing hormone (TRH), and oxytocin.
Other hormones are proteins (chains of peptides), such as insulin, growth hormone, and prolactin.
Glycoprotein hormones: More complex protein hormones bear carbohydrate side-chains and are called glycoprotein hormones. These include follicle-stimulating hormone (FSH), luteinizing hormone (LH), and thyroid-stimulating hormone (TSH).
Amine hormones: Amine hormones are derivatives of amino acids such as tyrosine and tryptophan. Examples are thyroxine, epinephrine, and norepinephrine.
Hormone sources
At one time, and not so long ago, by definition a hormone was produced in an endocrine gland (and an endocrine gland was a structure that produced one or more hormones). But as biologists have discovered and described more and more hormone substances and forms, they’ve expanded the definition to include similar, sometimes identical, substances that have a similar mechanism of action, wherever they’re produced. Check out all the sources of hormones:
Endocrine glands: An endocrine gland is an organ that synthesizes a hormone. It does so within a specialized cell type — the anterior pituitary gland, for instance, has cells that specialize in the production of such hormones as adrenocorticotropic hormone (ACTH), growth hormone, and TSH. Specialized cells within the thymus synthesize hormones that control the maturation of immune cells.
Various organs: A number of organs not usually included within the endocrine system by anatomists and physiologists have cells and tissues specialized for the production of hormones. For example:
While part of the pancreas is busy secreting enzymes for the digestion of food, other specialized cells of the pancreas produce insulin, and others produce glucagon.
The stomach and intestines synthesize and release hormones that control both physical and chemical aspects of digestion.
Specialized cells in the ovaries and testes transform cholesterol molecules into molecules of estrogen and testosterone, respectively.
Even the heart produces hormones, the secretion of which has an immediate strong effect on blood volume (fluid balance).
Neurons: Neurons make hormones that are neurotransmitters. This seems a bit surprising, but if you think of hormones as molecules that deliver messages with considerable subtlety, it makes sense. The transmission of nerve impulses across a synapse is exactly that (flip to Chapter 7 for more on the nervous system). The only difference between epinephrine synthesized in the adrenal glands and epinephrine synthesized in nerve cells is the distance the molecules travel to their target site.
Table 8-1 lists the body’s major hormones, their sources, and their functions. We provide more information about some of the individual hormones in the “Grouping the Glands” section later in this chapter.
TABLE 8-1 Important Hormones: Sources and Primary Functions
Hormone
Source
Function(s)
Adrenocorticotropic hormone (ACTH)
Pituitary gland (anterior part)
Stimulates secretion of corticosteroids by the cortex of the adrenal gland.
Antidiuretic hormone (ADH)
Pituitary gland (posterior part)
Stimulates the kidneys to reabsorb water, preventing dehydration.
Calcitonin
Thyroid gland
Targets the bones, kidneys, and intestines to reduce the level of calcium in the blood.
Epinephrine
Norepinephrine
Medulla of the adrenal gland
Stimulates the heart and other muscles during the fight-or-flight response; increases the amount of glucose in the blood.
Estrogen
Ovaries
Stimulates the maturation and release of ova; targets muscles, bones, and skin to develop female secondary sex characteristics.
Glucagon
Pancreas
Causes liver, muscles, and adipose tissue to release glucose into the bloodstream.
Glucocorticoids
Cortex of the adrenal glands
Stimulate the formation of glucose from fats and proteins.
Gonadocorticoids
Cortex of the adrenal glands
Stimulate the libido.
Growth hormone (GH)
Pituitary gland (anterior part)
Targets the bones and soft tissues to promote cell division, and synthesis of proteins.
Insulin
Pancreas
Allows glucose into cells, causes liver, muscles, and adipose tissue to store glucose as a way of lowering blood glucose level.
Melatonin
Pineal gland
Targets a variety of tissues to mediate control of biorhythms, the body’s daily routine.
Mineralocorticoids
Cortex of the adrenal glands
Targets the kidney cells to reabsorb sodium and excrete potassium to keep electrolytes (ions) within normal level.
Oxytocin
Pituitary gland (posterior part)
Social bonding, stimulates uterine contractions during childbirth and mammary glands to release milk.
Parathyroid hormone
Parathyroid glands
Stimulates the cells in bones, kidneys, and intestines to release calcium so that blood calcium level increases.
Progesterone
Ovaries
Prepares the uterus for implantation of an embryo and maintains the pregnancy.
Prolactin
Pituitary gland (anterior part)
Targets the mammary gland to stimulate production of milk.
Testosterone
Testes
Stimulates the production of sperm in testes; causes skin, muscles, and bones to develop male sex characteristics.
Thyroid-stimulating hormone (TSH)
Pituitary gland (anterior part)
Stimulates the thyroid gland to produce and release its important hormones, calcitonin and thyroxine.
Thyroxine
Thyroid gland
Distributed to all tissues to increase metabolic rate; involved in regulation of development and growth.
Hormone receptors
Hormones generally exit their cell of origin via exocytosis, which involves a sac or vesicle enveloping the substance and moving it across the cell membrane. The secreted hormone molecule goes directly into the blood and circulates until it binds with its specific receptor on the cell membrane. This activates a second messenger system, which leads to the cell’s response. Or, in the case of steroid and thyroid hormones, they enter the cell to bind with the receptor inside to stimulate the response.
The presence of a specific hormone receptor makes that cell a “target” for the hormone. Because hormones have very specific shapes, they’ll only bind to their matching receptor. Without the target receptor, the hormone has no effect.
The receptor may be on or embedded in the cell membrane, as is typically the case for peptide hormones. The hormone molecule, called the first messenger, latches on triggering a cascade of chemical reactions within the cell. Often, the series of reactions begins with the creation of cyclic AMP (adenosine monophosphate). This molecule, called the second messenger, then causes the target cell to produce the necessary enzymes (that is, to induce the expression of a certain gene).
A steroid hormone molecule doesn’t require a cell-membrane receptor. As a lipid, it enters a cell by diffusing through the membrane; thyroid hormones enter via facilitated diffusion (see Chapter 3). After it’s inside the cell, it binds with target receptor molecules either in the cytoplasm or inside the nucleus. Then, the hormone-receptor complex proceeds to its targeted gene and triggers the creation of a protein — which is the goal of the hormone.
Grouping the Glands
In general, a gland is a structure that synthesizes a product that’s exported from the cells. Endocrine (ductless) glands export their products (hormones) via the bloodstream to their target cells in anatomically distant organs. The following sections give you the lowdown on the endocrine glands. To see where these glands are located in the body, check out the “Glands of the Endocrine System” color plate in the center of the book.
The endocrine system, like any good communications system, functions in a very integrated way. That integration complicates the discussion of which anatomical structure belongs in what category. Remember that some organs carry out multiple function which leads to their placement in multiple organ systems.
Some physiologists use the term diffuse endocrine system to reflect the concept that many organs house clusters of cells that secrete hormones. The kidney, for example, contains scattered cells that secrete erythropoietin, a hormone essential for the production of red blood cells. The heart contains cells that produce atrial naturetic hormone, which is important in sodium and water balance.
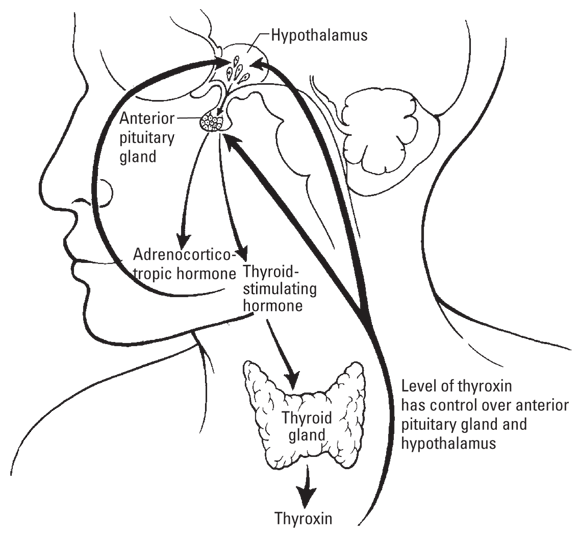
The taskmasters: The hypothalamus and pituitary
The hypothalamus-pituitary complex is the location where the nervous and endocrine systems meet. The hypothalamus and the pituitary gland adjoin in the central portion of the brain called the diencephalon. Under control of its “switchboard,” the hypothalamus, the pituitary is the endocrine system’s “master gland.”
Hypothalamus
The hypothalamus contains special cells that act as sensors that “analyze” the composition of the blood as it circulates through. It also contains other specialized cells that generate messengers (hormones) in response to the analysis. Tight pairing between these two types of cells is essential for homeostasis.
The hormones that the hypothalamus produces don’t have target cells in the body. The hypothalamus synthesizes releasing hormones and release-inhibiting hormones and secretes them into small blood vessels that connect to the anterior pituitary. The pituitary responds to releasing hormones by synthesizing and releasing its hormones, which have target cells in distant organs. It responds to release-inhibiting hormones by stopping its release of the corresponding hormones. Figure 8-1 shows the relationship between the hypothalamus and pituitary glands.
Illustration by Kathryn Born, MA
FIGURE 8-1: The working relationship of the hypothalamus and pituitary glands.
Pituitary
The pituitary gland has two parts, called the anterior pituitary and posterior pituitary that have different roles related to the hypothalamus.
The anterior pituitary gland secretes many hormones, including melanocyte-stimulating hormone (MSH). This hormone directly stimulates melanocytes to produce melanin pigment, which protects the skin from sunlight damage. This gland also secretes prolactin, which is responsible for the increase in size of the mammary glands in the breast and the production of milk.
The anterior pituitary also secretes the gonadotropic hormones FSH and LH, which target the ovaries and testicles, and ACTH, which targets the cortex of the adrenal glands. The function of these pituitary hormones is to stimulate the release of other hormones from their target glands. The same is true of growth hormone and TSH. They’re messengers that stimulate the action of other endocrine glands. (This information is summarized in Table 8-1.)
The posterior pituitary gland is directly connected to the hypothalamus (refer to Figure 8-1). The hormones that the posterior pituitary gland releases are actually synthesized in the nerve cell bodies of the hypothalamus. The hormones travel down the axons that end in the posterior pituitary and are released from there.
One such hormone is ADH. When the blood’s fluid volume falls below the ideal range, the hypothalamus produces ADH, which travels down the axons into the posterior pituitary gland. Released by the pituitary into the blood, ADH reaches its target kidney cells. ADH binds to receptors on the cells of the tubules and alters the cells’ metabolism so that more water is removed from the urine and added to the blood.
The posterior pituitary also releases oxytocin, the “love hormone.” Its release leads to social bonding — particularly between parent and child. It also plays a major role in the progression of uterine contractions during labor, as well as milk letdown (release of milk from the mammary glands). In males, it has been shown to cause contraction of the spermatic duct during ejaculation.
Controlling metabolism
Two relatively small organs exert a major effect on the availability of energy for physiological processes: the thyroid and adrenal glands.
Thy thyroid and thou
Thyroid hormones affect almost every physiological process in the body. Your thyroid gland looks somewhat like a butterfly that straddles your trachea (windpipe). (It’s pictured in Figure 8-1 and in the “Glands of the Endocrine System” color plate in the center of the book.) Each lobe of the thyroid gland — the butterfly’s wings — is adjacent to the trachea; a stretch of tissue called the isthmus connects the lobes. Simple cuboidal epithelium lines the follicles within the lobes and secretes a jellylike substance called thyroglobulin. Thyroglobulin “traps” iodine ions (consumed in food) in the colloid (internal fluid of the follicle) and promotes the formation of the amine hormones thyroxine (T4) and triiodothyronine (T3). When TSH from the anterior pituitary binds the target receptors in the thyroid, the thyroid hormones are released slowly into the bloodstream.
The thyroid hormones regulate the following physiological reactions. We discuss some of the problems that arise from the malfunction of these hormones in the “Pathophysiology of the Endocrine System” section later in the chapter.
The thyroid hormones
Control the body’s basal metabolic rate (the amount of energy needed to keep the body function at rest).
Increase the rate at which cells use glucose for energy.
Help maintain body temperature by increasing or decreasing metabolic rate.
Regulate growth and differentiation of tissues in children and teens.
Increase the amount of certain enzymes in the mitochondria that are involved in oxidative reactions.
Influence the breakdown rate of proteins, fats, carbohydrates, vitamins, minerals, and water.
Stimulate mental processes.
Increase the rate of protein synthesis.
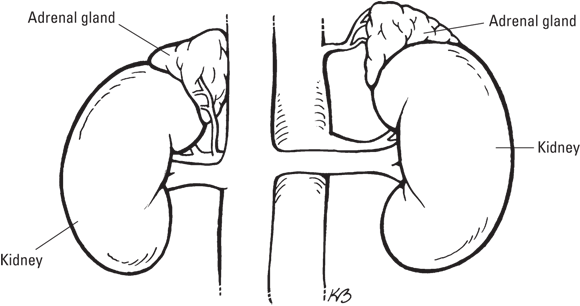
Topping the kidneys
The root renal means “kidney”; the prefix ad means “near.” So the adrenal glands are near the kidneys. More specifically, they sit on top of the kidneys (see Figure 8-2 and refer to the “Glands of the Endocrine System” color plate in the center of the book). Like the skin on a kidney bean, a thin capsule covers the entire adrenal gland. Inside, each adrenal gland has two parts: the cortex (outer layer) and the medulla (middle portion), which have different functions.
The adrenal cortex secretes corticosteroids, which include mineralocorticoids, glucocorticoids, and gonadocorticoids (refer to Table 8-1). One of the most important mineralocorticoids is aldosterone, which is responsible for regulating the concentration of electrolytes, such as potassium (K+), sodium (Na+), and chloride (Cl-) ions. This regulation keeps the blood’s salt and mineral content within the ranges required for homeostasis.
Electrolytes are substances that split apart into ions (atoms or molecules with a positive or negative charge) when in solutions, such as the watery tissue fluid around your cells or the cytoplasm within your cells. As their name suggests, electrolytes are capable of conducting electricity.
Aldosterone targets the kidneys’ tubules and stimulates the resorption of sodium ions. When the sodium ions are reabsorbed into the bloodstream, chloride ions quickly follow. Na+ and Cl- love to be together as NaCl, commonly known as “salt.” And where salt goes, water follows. If salt ions move into the bloodstream, water does too, increasing the blood’s fluid volume. Ultimately, the fluid and electrolyte balance affects blood pressure (see Chapter 9 for everything you wanted to know about the cardiovascular system).
The gonadocorticoids were named such because they are identical to the steroid hormones made by the gonads, the testicles, and ovaries. The gonadocorticoids consist of testosterone, estrogen, and progesterone. If you thought that as a woman you didn’t have any testosterone or as a man you didn’t have any estrogen or progesterone, you’re wrong. Admittedly, these are secreted in small amounts and have little influence on the development of the reproductive system. Apparently, their primary responsibility is to heighten sex drive. Increased production of their usually low amounts can lead to feminization in the male and masculinization in the female.
Cortisol, the main glucocorticoid hormone, regulates the metabolism of proteins, fats, and carbohydrates. Your body releases cortisol when you’re stressed emotionally, physically, or environmentally (hence its being dubbed the “stress hormone”). Cortisol affects metabolism in the following ways:
It breaks down protein, decreases protein synthesis, and moves amino acids from tissues to liver cells to promote gluconeogenesis (creation of glucose) and the formation of glycogen.
It moves fat from adipose tissue to the blood.
It reduces the rate at which cells take in glucose.
Cortisol and other corticosteroids affect the immune system by decreasing the number of circulating immune cells and decreasing the size of the lymphoid tissue. It also acts as an anti-inflammatory. Under severe stress and with large amounts of glucocorticoids circulating in the blood, the lymphoid tissue is unable to produce antibodies (see Chapter 13 for more on the lymphatic system). The role of corticosteroids in susceptibility to infectious disease is an active area of medical research.
ADRENAL MEDULLA
The adrenal medulla developed from the same tissues as the sympathetic nervous system (we cover the nervous system in Chapter 7). Some of the adrenal medulla’s functions involve regulating actions of structures of the sympathetic nervous system, including a class of hormones called the catecholamines, of which epinephrine and norepinephrine are the best known.
Epinephrine, also called adrenaline, initiates the “adrenaline rush” of the fight-or-flight response. It stimulates the release of free fatty acid molecules from your adipose tissue. Your muscles — including your heart muscle and respiratory system muscles — use these fatty acid molecules for energy, saving glucose for use by your brain. After all, if you’re fighting or fleeing, you need to think.
Unlike most hormones, epinephrine produces its effect almost instantaneously.
Like epinephrine, norepinephrine is a catecholamine that’s tied to the nervous system. Norepinephrine causes vasoconstriction — that is, tightening of the blood vessels. Norepinephrine is released to increase blood pressure when the hypothalamus senses hypotension (low blood pressure), as well as when you’re stressed. (Your body still prepares to run or fight, even when these responses aren’t quite appropriate.)
Getting the gonads going
Your gonads — ovaries if you’re female or testes if you’re male — produce and secrete the steroid sex hormones — estrogen and progesterone in females and testosterone in males. Your body secretes sex hormones throughout your lifetime at different levels. Their production increases at puberty and normally decreases as you age.
You may think that estrogen is limited to female animals, but you’d be wrong. Estrogen can be detected in the urine of male animals, and even, surprisingly, in growing plants! Just as men also have some estrogen, women also have some testosterone.
Estrogen
In women, the increased production of estrogen at puberty is responsible for initiating the development of the secondary sex characteristics, such as the enlargement of the breasts. Bone tissue grows rapidly, and height increases. Estrogen helps this process, causing calcium and phosphate to be transported in the bloodstream so they can be used for bone growth and for stimulating the activity of the osteoblasts (see Chapter 5).
Estrogen also allows the pelvic bones to widen to allow passage of an infant during childbirth. In addition, estrogen increases the deposition of fat around the body, thus giving women a more rounded appearance than men.
Estrogen is actually a category — referring to the steroid hormones made by the ovaries. Use of the term refers to all three variants, the most common of which is estradiol.
Progesterone
Progesterone works to prepare the uterus for implantation of a pre-embryo by causing changes in uterine secretions and in storing nutrients in the uterus’s lining. Progesterone also contributes to breast development.
Testosterone
Testosterone causes the development of secondary sex characteristics in males. As a boy hits puberty, his muscle tissues start to grow, his sex organs enlarge, hair develops on his chest and face, and the hair on his arms and legs becomes darker and coarser. For more on development during puberty, turn to Chapter 15.
These hormones also play a key role in the development of gametes, or sex cells (egg and sperm). This is discussed in Chapter 14.
Enteric endocrine
Much of the endocrine function is enteric (related to digestive processes). Precise control of nutrient intake and storage and the excretion of toxins and digestive byproducts is essential for homeostasis and metabolism.
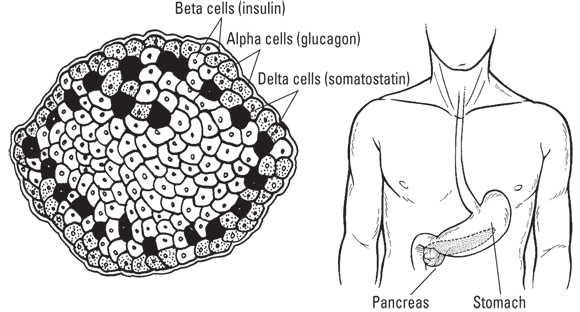
Flat as a pancreas
Your pancreas is a fibrous, elongated, flat (as a pancake) organ that lies nestled in your abdomen near your kidneys, stomach, and small intestine (see Figure 8-3 and the “Glands of the Endocrine System” color plate in the center of the book). Its two tissue types have different functions:
Digestive function: It produces digestive enzymes that it secretes into the small intestine. This tissue is arranged around ducts (see Chapter 11).
Endocrine function: It produces the hormones insulin and glucagon, which it secretes into the blood. This tissue is arranged in clusters called islets (see Figure 8-3).
Glucose travels in the blood, making it available as an energy molecule for all cells. But too much glucose in the blood is harmful to the small vessels, especially those in the extremities, in the kidneys, and in the retina of the eye. The body must keep the concentration of glucose in the blood within limits. The pancreas’s endocrine tissues produce insulin and glucagon, which work together to balance the blood’s glucose level — insulin acts to lower it, and glucagon acts to raise it. The regulation of blood glucose is a classic example of a hormone mechanism of homeostasis. Refer to the “Pathophysiology of the Endocrine System” section later in this chapter for a discussion of disorders in this system.
Insulin secretion is an example of a negative feedback mechanism. As the blood’s glucose level declines, the body slows the secretion of insulin until the next surge of blood glucose following a meal or snack.
Insulin is released when the blood’s glucose level rises. It acts by stimulating glucose uptake in cells. Without insulin, most cells would not be able to take in glucose, which is required for cellular respiration (see Chapter 2). So, in addition to the damage done by excess glucose in the blood, cells cannot generate enough ATP to power their processes. Insulin also stimulates glucose uptake activity in the energy storage cells in the liver, muscle cells, and adipose (fatty) tissue.
A low blood glucose level stimulates the pancreas to secrete insulin’s partner glucagon, which pulls glucose from cells where it’s stored and releases it into the blood. In particular, it stimulates the liver to break down glycogen, the storage form of glucose, leading to more sugar in the blood. Glucagon keeps the metabolic fires burning at a steady level.
Stomaching another gland
Yes, the stomach is a key organ in digestion (Chapter 11 covers the digestive system in detail), but it also secretes hormones that are used during digestion, making it a gland. The stomach secretes a group of hormones called gastrins. Many types of gastrin molecules — small, medium, and large — are responsible for stimulating the secretion of gastric acid. Gastrins also control the sphincter muscle at the bottom of the esophagus, thereby controlling when food can be passed into the stomach. Other cells in the stomach produce the hormone ghrelin, which targets the brain to stimulate the hunger.
Testing the intestines
The intestines secrete powerful digestive enzymes, but they require a pH much higher (less acidic) than the extremely acidic stomach acids. The small intestine produces the hormone secretin that stimulates the release of neutralizing substances, such as bile from the gallbladder and pancreatic bicarbonate. Other cells in the small intestine produce cholecystokinin (CCK), which triggers the release of digestive enzymes from the pancreas and gall bladder.
Other endocrine glands
Other endocrine glands secreting important hormones include the following:
Parathyroid: The parathyroid glands are four small glands that secrete parathyroid hormone (PTH), which increases the concentration of calcium in the blood, making it available to the muscle fibers and neurons. The parathyroid essentially helps the nervous and muscular systems function properly. Calcium is the primary element that causes muscles to contract, and calcium levels are very important to the communication between neurons.
The four parathyroids are typically found on the backside of the thyroid. They’re about the size and shape of a grain of rice. They are related to the thyroid in their function of maintaining calcium levels, as the thyroid produces the hormone calcitonin, which decreases blood calcium levels.
Pineal gland: The pineal gland is a small oval gland in the brain between the cerebral hemispheres that’s considered part of the epithalamus of the diencephalon. The pineal gland secretes the hormone melatonin, which plays a role in regulating the body’s circadian rhythm — the normal fluctuation of physiology over the day-night cycle. The secretion of melatonin is influenced by the perception of light within the gland.
Thymus: The thymus is a lobed gland situated in the thoracic cavity, just below the collarbones and just above the heart. The thymus’s main function is to stimulate the maturation of T lymphocytes from the bone marrow into T cells (see Chapter 13). The thymus produces a group of hormones called thymosins that are involved in differentiating and stimulating the immune system’s cells.
Pathophysiology of the Endocrine System
The body depends on its chemical messaging system to maintain control over its physiological processes. Malfunctions in the messaging system can disrupt target organ systems and the cardiovascular system that transports the hormones between the gland and the target organs via the blood.
Abnormalities in insulin metabolism
The following abnormalities in insulin metabolism cause blood glucose to rise and remain at high levels. This extra glucose damages the smallest blood vessels, like those in the retina of the eye and the glomeruli of the kidney. It can also lead to acidosis, a drop in the pH of the blood, which damages numerous tissues including nerves.
Metabolic syndrome
Insulin moves glucose into cells. However, sometimes the cells develop a “resistance” to insulin’s effects, and larger and larger concentrations of insulin are required to produce the same results. As long as the pancreas is producing enough insulin to overcome this resistance, blood glucose levels remain within the homeostatic range. Eventually, the pancreas can no longer produce enough insulin to overcome the resistance, initially after meals, when blood glucose levels are highest. Insulin resistance is thought to contribute to the accumulation of abdominal fat and other developments that increase risk for diabetes and cardiovascular disease. This set of risk factors is called the metabolic syndrome.
Diabetes mellitus type 1
Type 1 diabetes, previously called juvenile diabetes, is the result of the destruction of the pancreatic cells that produce insulin. The ultimate cause of the cell destruction has been an active area of medical research for a century. The effects of untreated type 1 are ultimately fatal. The development of intravenous insulin for treatment of this condition was one of the medical breakthroughs of the last century.
Diabetes mellitus type 2
Type 2 diabetes is caused by insufficient blood insulin concentration, either because insulin production is impaired or insulin resistance has developed. The high levels of blood glucose slowly damage small blood vessels, leading to impairment or failure of numerous organs and systems.
Diabetes insipidus
Diabetes insipidus is caused by the inability of the hypothalamus to produce the proper amount of antidiuretic hormone (ADH), which is responsible for stimulating the kidney to return water to the bloodstream. Without ADH, very little water is returned, and the concentration of glucose in the blood rises (along with that of other dissolved substances). Large amounts of watery urine lead to dehydration and thirst and carry electrolytes right out of the body. This disorder can be treated by administration of ADH therapy.
Gestational diabetes
Gestational diabetes is high blood glucose that develops at any time during pregnancy in a woman who doesn’t have diabetes. Women who have gestational diabetes are at high risk for type 2 diabetes and cardiovascular disease later in life.
Thyroid disorders
The pervasive role of the thyroid hormones in metabolism can be seen by the widespread physiological effects of thyroid disorders.
Hypothyroid disorders
The prefix hypo means “below.” The result of low levels of the thyroid hormones is hypothyroidism. This low level can result from a defect in the thyroid gland (primary hypothyroidism), or the hypothalamus or pituitary glands may not be sending the proper messaging hormones to the thyroid (secondary hypothyroidism). People with primary hypothyroidism may have inflammatory conditions similar to arthritis, or chronic conditions, such as Hashimoto’s thyroiditis (a disease in which the body’s immune system attacks the thyroid gland’s cells). Dietary deficiency of iodine and medications that negatively affect the thyroid gland also may cause secondary hypothyroidism.
Hypothyroidism has many signs and symptoms because the thyroid hormones have such a widespread effect. Nearly every cell in the body is stimulated by the hormone thyroxine, which regulates the rate of metabolism. Symptoms of hypothyroidism are shown in Table 8-2.
Weight gain without increase in food intake or decrease in exercise
Muscle cramps
High cholesterol, poor circulation, heart problems
Constipation
Numbness or tingling sensations
Dry skin and hair, some hair loss; brittle, grooved nails
Memory problems
Impaired fertility
Weak colon, intestinal obstruction, anemia
Myxedema is a life-threatening complication of hypothyroidism. As metabolism slows, the exchange of carbon dioxide and oxygen slows. As the amount of carbon dioxide in the blood rises, the patient is at risk of slipping into a coma, which may be fatal.
Whether primary or secondary, hypothyroidism has profound effects on metabolism in several organ systems (refer to Table 8-2). Treatment for people with hypothyroidism involves lifelong administration of a synthetic thyroid hormone. However, therapy must begin gradually so the heart isn’t negatively affected.
Hyperthyroid disorders
Abnormally high levels of the thyroid hormones is the condition of hyperthyroidism, also called Graves’ disease. Hyperthyroidism makes a person irritable, nervous, and unable to sleep. The thyroid gland may enlarge into a goiter, and swelling of the eye muscles may make the eyeballs protrude somewhat. Treatment options for patients with hyperthyroidism include oral medications, a single dose of radioactive iodine, or surgery to reduce the size and activity of the thyroid gland.
Androgen insensitivity
Androgen insensitivity syndrome (AIS) is a disorder caused by mutation of the gene for the receptor that binds testosterone, which regulates the expression of genes that stimulate male sexual development. Affected individuals are chromosomally XY but have a feminine phenotype and are sterile. AIS completely or partially prevents development of male sexual characteristics in the fetus, despite the presence of the Y chromosome. The extent of the syndrome ranges from complete androgen insensitivity and development of normal external (but not internal) female sexual anatomy, to partial insensitivity with altered or ambiguous male or female genitals, to mild insensitivity with normal male genitals, enlarged breasts, and possibly impotence.
 Understanding what hormones do and how they work
Understanding what hormones do and how they work Your body is always keeping tabs on the metabolic processes going on inside it. If your body temperature, glucose level, or pH level leaves the normal range, the checkpoints involved in homeostasis work with the endocrine system to bring your systems back into balance.
Your body is always keeping tabs on the metabolic processes going on inside it. If your body temperature, glucose level, or pH level leaves the normal range, the checkpoints involved in homeostasis work with the endocrine system to bring your systems back into balance. Some physiologists use the term diffuse endocrine system to reflect the concept that many organs house clusters of cells that secrete hormones. The kidney, for example, contains scattered cells that secrete erythropoietin, a hormone essential for the production of red blood cells. The heart contains cells that produce atrial naturetic hormone, which is important in sodium and water balance.
Some physiologists use the term diffuse endocrine system to reflect the concept that many organs house clusters of cells that secrete hormones. The kidney, for example, contains scattered cells that secrete erythropoietin, a hormone essential for the production of red blood cells. The heart contains cells that produce atrial naturetic hormone, which is important in sodium and water balance.