We are inundated with health information today—books, news articles, internet sites, tapes, support groups, newsletters, and many others. I enjoy having my patients bring in articles that have stimulated questions and we often discuss these new findings and approaches. One of the topics that comes up daily in my medical practice is “What about wild yam/progesterone creams?” There has been an exponential increase in over-the-counter progesterone creams and multilevel marketing schemes in the marketplace today, with incredible claims touting progesterone as a “wonder hormone” to prevent osteoporosis, lose weight, increase sex drive, and solve all of women’s problems.
What’s the scientific truth behind those claims? There is a wealth of good solid medical and basic science research going back fifty years to draw on in answering this question, and I think it is important to clarify these issues. There is so much emphasis on using progesterone for treatment of PMS, menopause, and pain problems that I think people who recommend such broad use of one hormone have forgotten that women have a variety of hormones with different functions, and each one has to be taken into account in our evaluation and treatment approaches. In this chapter, I have presented both the historical and the current worldwide research from reputable medical centers, menopause and PMS researchers, and neuroendocrine basic science researchers to describe which functions are known to occur with each of these major hormones. My goal is to give you a reliable “road map” through the maze of conflicting information out there.
In 1573, Volcherius Coiter first observed the presence of a yellowish body in the mammalian ovary, later called the corpus luteum in 1686 by Malpighi. Then Dr. Born first suggested that perhaps it was an endocrine organ concerned with maintaining pregnancy, and it was his student, Loeb, who showed in 1907 that the corpus luteum specifically prepares the uterus to receive a fertilized egg; that is, it is the cause of the “progestational” changes in the lining of the uterus whether followed by pregnancy or only by menstruation. It was in 1928 that Weichert demonstrated the actual existence of a hormone from this “yellow body” by injecting extracts of corpora lutea into uterine tissue, and this injection produced the changes described by Loeb. Then the pure hormone was isolated by Wintersteiner and Allen and others in 1929 and named “progesterone” for its pregnancy-promoting (“pro-gestational”) effects.
Since the quantity of this new hormone present in nature was so remarkably small—perhaps one part in 40,000 in the human corpus luteum or one part in 750,000 in the placenta (Duuyvene, 1939; Pratt, 1936), the greatest practical importance lay in finding a way to make this hormone by synthetic means. It was a significant advance for clinical medicine when Butenandt and Fernholz, in 1934, first prepared the pure corpus luteum hormone from the precursor stigmasterol found in soybeans. Allen found that diascorea, a precursor found in the wild Mexican yam could also be synthesized in the laboratory into the molecule of progesterone. Prior to these discoveries, the natural sources were quite limited. Finding “building block” substances in soybeans and yams meant that we now had a renewable natural source from plants that could be cultivated to provide the quantities needed for production of progesterone, and later synthetic progestins and various estrogens, for clinical use.
Progesterone is the primary hormone designed to prepare the female body to support a pregnancy. In the first half of the menstrual cycle (follicular phase) there is no significant amount of progesterone produced, and levels in women are about 0.3–0.9 ng/ml. When ovulation occurs, the ovum is released and becomes the corpus luteum (“egg”), which begins to secrete progesterone. Levels of progesterone in this half of the cycle (luteal phase) rise to about 15–30 ng/ml, or up to thirty times the level of the first half of the cycle. Levels in pregnancy are about fifteen times greater than luteal phase progesterone levels.
Studies done in the 1970s showed that an oral dose of 300 mg micronized progesterone given daily for one week would produce blood levels of progesterone equivalent to third trimester of pregnancy. Oral doses of 200 mg daily for ten to fourteen days are used in HRT to prevent endometrial hyperplasia. The progesterone secreted by the corpus luteum stimulates the lining of the uterus to thicken and become secretory in preparation to receive a fertilized egg and help it grow. If there is fertilization and pregnancy, the placenta becomes a hormone-producing factory, with increasing progesterone production throughout the months of pregnancy. With so many changes needed in a woman’s body for her to sustain a pregnancy, it is not surprising that progesterone has a wide range of metabolic effects on the whole body, not just the reproductive organs. Think about it. For a female to get enough nutrition for the growing fetus, she has to eat more. Progesterone is the hormone that stimulates appetite and drives the individual to eat more (both in a nonpregnant menstrual cycle, as well as throughout pregnancy). It also stimulates the desire for carbohydrates, which are more quickly converted to useable fuel.
In addition, progesterone relaxes the smooth muscles of the intestinal tract, which slows down the movement of food and allows greater absorption of nutrients. For a pregnancy, this is a beneficial effect. If you are not pregnant, you may experience this “slowing down” of the intestinal tract as constipation (especially if you don’t get enough fiber). Progesterone has been shown to have marked effects to increase total body fat, and this occurs in many different species studied, not just humans. This fat-storing effect has an obvious evolutionary advantage for survival to ensure that pregnant women have adequate fat stores to provide fuel for mother and baby through nine months of gestation. Another important effect of progesterone is to suppress the mother’s immune system so that the mother’s body will not “attack and destroy” the foreign protein of the developing fetus that contains the father’s genetic makeup and protein coding systems. This is a crucial function of progesterone for a pregnant woman, but not one that we want all the time.
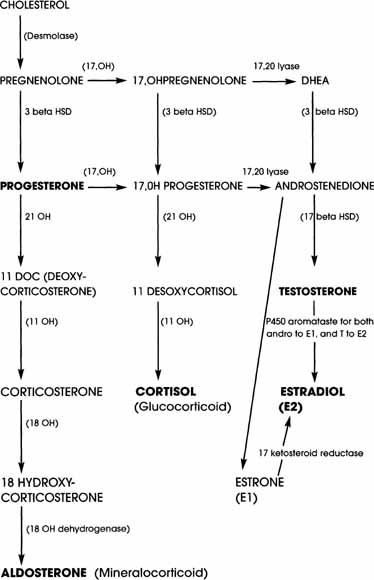
The chart that follows shows how the body makes progesterone and other ovary hormones from cholesterol. You have probably seen this chart in other health books, and I wanted to clarify some of the basic biology of how this works. Looking at this sequence, you may be tempted to believe some of the current books and tapes that say progesterone is the “mother” hormone women should be taking because it comes at the beginning of the pathway and all of the other hormones, including testosterone and estradiol, are made from this compound. Think about it. If that logic were really correct, we should be suggesting that men take progesterone, too, as they get older and their testosterone declines. But we clearly don’t do this for men. Why not? There are several aspects of this whole line of reasoning that are incorrect based on reputable medical science and reproductive hormone endocrinology. First of all, most of the conversion of progesterone down this pathway to the end products of testosterone and estradiol require the presence of functioning ovaries. If you have reached menopause, your ovaries are no longer functioning to handle these conversions.
If you had a severe viral illness, a prolonged stress that disrupted menses, a tubal ligation, or one of many other causes of gradual decline in ovarian function, then you may not be able to convert a load of precursor hormones to the end-product hormones. If you have had a hysterectomy with the ovaries removed, well . . . it is obvious you don’t have the ovaries to convert progesterone to the end hormones (estradiol, testosterone) that you need for optimal well-being. I think the important point here is that Mother Nature gave us a series of steps for the body to go through to get to the end result . . . we can’t assume that we can simply load up on one beginning step in the process and accomplish the same results as the body does when everything is working the way it is supposed to.
Another metaphor for this process comes to mind. Think about the many stages of growth and development that have to occur for a baby to become a child, then an adolescent, then an adult. I think of progesterone as the “baby” in our hormone-development process. It can’t carry out all the functions of the “adult” hormones estradiol and testosterone until it has been shaped and altered by the changes of this entire cascade of steps. Progesterone can’t be made into testosterone or estradiol directly; it has to undergo further changes to become the molecules that are the direct building blocks for testosterone and then estradiol. It’s very much like the life process—a baby can’t become an adult without going through the stages of childhood, and then adolescence. And without our ovaries to facilitate this “growth” of the “baby” progesterone so it can become the “adult” testosterone and estradiol, we are stuck with a molecule that doesn’t have the specific shape of estradiol or testosterone to activate the receptors for normal function. Remember, each of these molecules acts like a different key in various receptor locks throughout the body, so the proper shape to the molecule key is crucial to create the proper results.
Over the many years of research into steroid hormones and their function in the body, it has been known that relatively small changes in the molecule—number of carbons, side chains, number of unsaturated chemical bonds, other atoms added—can make an enormous difference in the way that molecule works in the human body. These small changes in the molecule can affect everything from desired effects to unwanted side effects. For example, once the progesterone molecule is changed in metabolism to a different arrangement of the molecule called pregnandiol, it is now completely inactive. Conversion to pregnandiol is one of the ways that the body clears excess progesterone and makes it possible to be excreted in the urine. Other breakdown products of progesterone (allopregnandiol, epiallopregnanolone) are also inactive and are excreted in the urine.
On the other hand, some metabolic changes in the molecule of progesterone lead to compounds that are even more potent, particularly at brain receptors, than even progesterone itself. This is seen with 3-alpha, 5-alpha THP (allopregnanolone), a highly potent sedative and depressant metabolite of progesterone. We see this issue of different effects happening with small changes in the molecule occur quite strikingly when the molecule of progesterone, as found naturally in the body, is chemically changed to make a synthetic group of compounds called progestins. There are several terms that many women find confusing, so I will clarify these to help you understand various options.
Progestogen is the broad term used to describe any substance that has chemical effects to sustain a pregnancy, called “progestational” activity.
Progesterone (found in humans and all vertebrate animals) is a biologically natural progestogen. Human progesterone is produced by the corpus luteum after ovulation, and to a much lesser extent by the adrenal gland (though adrenal production is not sufficient to prepare the body to sustain a pregnancy). Progesterone USP is the form of natural progesterone derived from “building block” molecules in soybeans and wild Mexican yams. These “building blocks” (stigmasterol, diascorea, and others) are changed chemically in the laboratory with a series of steps and purified to meet FDA standards for use as a medication. USP progesterone may be dissolved in oil to make an injectable form of medication, which has been available to physicians since the 1940s. USP progesterone is also available as a powder that is made into tablets (Prometrium), or vaginal gel (Crinone), as well as used by pharmacists to compound individual prescriptions of tablets, suppositories, and creams for patients. USP Progesterone is identical to the chemical molecule made by the ovary. When used for hormone therapy, it generally has far fewer unpleasant side effects than the progestins (such as Provera and others).
Disogenin (and others) is a plant precursor molecule found in wild yams, soybeans, and a variety of other foods, that has some very mild effects similar to both progesterone and estrogen. This is used in many nonprescription creams. These plant precursors are not the same chemical molecule as either progesterone or estradiol, and do not have the exact same effects in the body—even though the marketing hype will try to make you think otherwise. These phystosterols (phytoestrogens, phytoprogestins, etc.) can be made into progesterone or estradiol by chemical changes that are done is a laboratory. Our bodies do not have the enzymes needed to make these changes in the molecule, so our bodies cannot take the wild yam or soybean precursors and make them into the exact same molecules the ovaries make before menopause.
Progestins are man-made chemical molecules that have a different chemical structure from the molecules naturally found in the human body. They have many properties and actions similar to progesterone but because their molecules are “rearranged” slightly from progesterone, they have a number of different actions as well, and are many times more potent than natural progesterone. As a result, progestins can produce very different effects in the body that are at times quite desirable and needed, and other times quite bothersome and undesirable.
Progestins are technically a member of the larger group of progestogens because they all have some degree of progestational activity, but they are not compounds normally found in the human body. Progestins may be made from progesterone and are then called progestational progestins, such as Provera, Cycrin, Amen (generic name: MPA or medroxyprogesterone acetate). MPA was originally approved by the FDA in the 1960s for contraceptive use under the brand name Depo-Provera and has since been used to treat abnormal uterine bleeding and some types of amenorrhea. In more recent years, MPA and other progestins have been used for protection of the uterine lining in menopausal regimens.
Another group of progestins is made from the naturally occurring ovarian molecule of testosterone, and these are called androgenic progestins. This group includes medications like Aygestin and Micronor (generic name: norethindrone) as well as products that contain the androgenic progestin levonorgestrel (Norplant implant, some combination oral birth control pills). In addition to its progestational activity, this group has effects similar to testosterone and is often used when women are experiencing a loss of libido. The androgenic progestins have generally caused fewer problems with depressed mood and decreased libido than we see with Provera or other progestational progestins. Newer progestins like norgestimate and desogestrel are the most progestational and least androgenic of the synthetic progestins. This means they are less likely to cause acne, but more likely to cause weight gain, loss of libido, or depressed mood.
Synthetic progestins, whether in birth control pills or given in postmenopause, are the most common cause of unpleasant side effects associated with “hormone therapy.” Some of these are irritable mood, depressed mood, headaches, decreased energy, weight gain, bloating, and breast tenderness, among others. Two major factors are important in determining the balance of desirable therapeutic effects and undesirable side effects: (1) the relative balance of progestational and androgenic activity, and (2) the balance of progestin relative to estrogen in the preparation. Progestin-only products (that is, contain no estrogen) like Norplant and Depo-Provera, as well as pills such as Micronor, typically have the worst side effect profile of all, because you get all the negative effects of the progestin without any compensating benefits of the estrogen unless estrogen is added as a separate pill or patch.
Progestin-only options are particularly hard to use for women with FMS, vulvodynia, interstitial cystitis, or migraines because they tend to increase pain to a marked degree. This is especially true of the long-acting progestin-only contraceptives like Norplant and Depo-Provera. If I prescribe Micronor, for example, I always balance it with estrogen to avoid making FMS pain worse. My patients tell me that the androgenic progestins cause less bloating and breast tenderness than Provera and other ones in this group. The more androgenic progestins, however, may cause more acne and are not recommended for women with high cholesterol and low HDL, since the androgenic effects can worsen the risk of cardiovascular disease and decrease the benefits of estrogen. Finding the one that works best for your body is both an art and a science!
What about natural progesterone, chemically identical to what the body makes? Why even use the synthetic progestins if they tend to cause so many side effects? There are some situations and some women for whom the synthetic progestins actually work better or have fewer side effects. But there is another practical reason we haven’t had widespread use of natural progesterone in this country until more recently. It has to do with technology of delivery of the hormone, as well as expense. Progesterone itself is quickly inactivated by stomach acid and then isn’t absorbed into the bloodstream when taken by mouth. So it simply didn’t work to give progesterone orally until a new process, called micronization (which means making the hormone particles tiny enough to be absorbed before being inactivated), was developed in the 1960s. Only then could we provide more reliable absorption and the desired therapeutic effects of progesterone. The injectable form of progesterone is put in oil to promote absorption into the bloodstream and has been available in the United States since the 1940s. It is made by Upjohn, the company that also makes Provera and Depo-Provera, which were originally developed trying to find a tablet form that would be active when taken by mouth. The injectable form of progesterone USP in oil has been widely used by gynecologists for years, but most women understandably did not want to have to get an injection on a regular basis.
By the time micronization processes were developed, doctors were used to using Provera, and it was much cheaper for patients to buy than the newly invented micronized progesterone. From the 1970s through about 1998, micronized natural progesterone was primarily available through specialty compounding pharmacies in various forms (tablets, creams, suppositories). Since these forms were made according to individual prescriptions and not manufactured in huge quantities, they typically were not covered by health insurance plans and were significantly more expensive than the commercially available progestins like Provera. In addition to habit, the higher cost to patients was another reason more doctors continued using the synthetic ones. Then in 1998, the FDA approved Prometrium, a tablet form of micronized progesterone, and Crinone vaginal gel (also micronized progesterone), so more and more physicians are now using natural progesterone for menopause, PMS, and bleeding problems. These new commercial products of natural progesterone are advantageous since they are usually covered by health insurance plans, unlike compounded prescriptions. If Prometrium or Crinone don’t quite fit your body’s needs in terms of dose and form, then you can still get micronized progesterone tailored to your needs by compounding pharmacists. I have used natural progesterone in a variety of forms since I was a medical student in 1975. I have found that natural progesterone generally works well, when used properly, and has far fewer side effects than do the Provera-type medications.
I described in chapter 3 how estradiol produced before menopause is one of the primary hormones regulating the brain’s sleep center and facilitating the normal stages of sleep. When estradiol declines, the normal stages of sleep, especially periods of Stage IV deep sleep, are disrupted. So it is crucial for women to have adequate estradiol to regain normal deep sleep and muscle repair. But there are a number of metabolites of progesterone that have potent sedative effects, very similar to barbiturates and benzodiazepines. Remember the compound I mentioned in chapter 3 called 3-alpha-OH-DHP? It is about eight times more potent than the sedative methohexital, a potent barbiturate used for anesthesia. The liver provides most of the conversion of progesterone to these sedative compounds, so the sleep-inducing effects of progesterone will be increased if it is taken orally and goes through the liver “first pass” metabolism. So progesterone does have effects on brain receptors that help sleep, by acting like the medications you may already know: Klonopin, Ativan, Valium, and others in this group.
Progesterone’s effect on sleep is quite different from estrogen effects, so just taking progesterone doesn’t eliminate the need for estradiol to restore sleep pathways, as some books claim. Since progesterone can make you sleepy like Klonopin does, there may be times when it can be a useful addition to hormone therapy even if women do not have a uterus. But this has to be balanced against the unwanted, potentially negative metabolic effects of progesterone that I have discussed elsewhere in this chapter and in chapter 3. Some of the metabolites of progesterone have greater sedative effects on brain receptors than does Klonopin. If progesterone is used to improve sleep in a woman with FMS, I find that lower doses can be effective if estradiol has been restored to optimal levels. If you have a uterus, however, you and your doctor have to be certain that you are taking an appropriate dose of progesterone for the desired protective effects on the endometrial lining.
Both estradiol and progesterone have important effects on pain regulation in women. In this chapter I will review aspects of progesterone’s effects and talk about estradiol in chapter 5. As I mentioned earlier, several of progesterone’s metabolites act as central nervous system anesthetics, both by increasing endorphin production (such as late-stage pregnancy) and by enhancing the action of the inhibitory neurotransmitter, GABA. The analgesia of pregnancy has been extensively studied and has been shown to involve central nervous system opioid systems rather than peripheral (body) ones. Since opioid compounds from the body have only limited ability to cross the blood-brain barrier, it has been hypothesized that the estradiol-progesterone-triggered increase in analgesia seen in pregnancy primarily results from a direct effect of activating a brain endorphin system. In addition, the dynorphin system has also been shown to be activated in the analgesia of actual pregnancy. Giving estradiol and progesterone peripherally (oral, transdermal, etc.) has been shown to increase several measures of brain opioid activity; increases in opiate receptor density as well as the concentration of beta-endorphin in brain centers have been demonstrated.
In support of this theory of the female sex hormones as activators of pregnancy analgesia systems, it has been shown that the pregnancy concentration of progesterone in cerebral spinal fluid (CSF) increases eight fold, with a rapid decrease in the immediate postpartum period, along with the rapid drop in estradiol levels. In addition, there is more biologically active progesterone present in the later stages of pregnancy, since the percentage of unbound or free progesterone in spinal fluid was found to be three times greater than that in the blood in all three types of patients: pregnant, postpartum, and nonpregnant women. The abrupt drop in both progesterone and estradiol with the delivery of the placenta leads to an abrupt drop in the endorphins as well, which is one of the many changes contributing to the irritable, depressed mood, fragmented sleep, and increased pain in the early postpartum weeks. If the estradiol and progesterone levels remain low over a prolonged period of time following delivery, such as with nursing or due to a postpartum thyroiditis or postpartum viral illness, the low levels trigger increased sensitivity to pain. I am convinced that this is a primary factor triggering the postpartum fibromyalgia syndromes, along with the loss of important effects on sleep, muscle repair, and nerve tissue itself from the ovarian hormones. I have treated quite successfully a number of postpartum fibromyalgia patients with just proper hormone balancing, which would fit with the basic science data on these hormones’ multiple effects on pain pathways.
Frye and Duncan (1994) showed that, in rats, diminished pain sensitivity correlated well with the relative binding actions of various progesterone metabolites at the GABA receptor complex. They looked at several different compounds, and those that were strongly bound to GABA receptors showed the greatest reduction in pain, while the GABA antagonist compounds such as DHEA-S did not improve pain sensitivity. Both the sedative and analgesic effects of progesterone are gender-independent effects: They can also be observed when progesterone is given to men. It’s just that under normal conditions, the adrenal glands in men normally make only a tiny amount of progesterone, about a third of the lowest concentrations found in women during their bleeding days.
Even in nonpregnant women, progesterone, and estradiol as you saw in chapter 3, play roles in the brain endorphin pathways. When progesterone and estradiol levels both fall in the days just before bleeding starts, the drop in both hormones triggers a fall in brain-body endorphins as well as a lowering of our pain threshold that makes us more sensitive to pain. A cyclic variation in pain threshold in menstruating women has been found in a number of recent studies, which confirms the intuitive wisdom of my patients who have noticed this. Science finally catches up with women’s wisdom. This appears to be one of several reasons that women with FMS, vulvodynia, and IC have “flares” with the onset of menstrual bleeding. It is also one of the reasons I try to help my patients keep the estradiol level steady during these days. Progesterone has to drop in order to trigger bleeding, but I can help offset the drop in endorphins if I keep estradiol levels steady so that both hormones are not so low. This approach has been one that my patients tell me works really well to help keep the menstrually related pain “flares” in check. So, together the two primary ovarian hormones, estradiol and progesterone, play a significant role in modulating pain in women. It has also been found that for progesterone to exert some of these effects, the receptors need to be “primed” estradiol in the first half of the menstrual cycle. This is another reason to take hormones in a manner that closely mimics the sequence and ratios of a healthy menstrual cycle.
Numerous studies over the last three decades have shown that progesterone decreases growth hormone (GH) and increases insulin levels. This metabolic pattern is the same one seen in obese people, in Cushing’s disease (excess Cortisol), and after starting corticosteroid medication (such as for arthritis or asthma); it clearly isn’t a very desirable pattern to maintain. Higher levels of progesterone, such as in pregnancy or when taking large doses for PMS or menopause therapy, are associated with greater amounts of unbound, or free, cortisol in the blood, which further decreases GH and causes higher insulin levels with more insulin resistance. This is another reason that using progesterone regularly, in doses that give blood levels similar to pregnancy, can have negative health effects on a nonpregnant woman. Most of the women I have been treating for hormone imbalances aren’t pregnant and don’t want to be, so artificially creating high progesterone levels simply doesn’t make sense. The brain-body changes triggered by high progesterone levels can wreck havoc with maintaining healthy production of GH, insulin, and cortisol, leading to excessive weight gain and many other problems.
Muscle protein metabolism is affected by the hormone changes of the menstrual cycle. Studies of exercise effects on protein breakdown in women have been done, with calculations of the amount of breakdown products (urea and others) excreted in the urine based on whether the women were in the mid-follicular (high estradiol) phase or mid-luteal (high progesterone) phase. Such studies showed marked differences in the excretion of muscle breakdown products in the urine by cycle phase, with highest levels of urea in the urine occurring during the mid-luteal phase. Researchers have concluded that the high levels of progesterone in the mid-luteal phase of the menstrual cycle suggest that an elevated progesterone-to-estradiol ratio exerts a catabolic (breakdown) effect on body proteins. If this effect continues to be supported by future studies, it would suggest that women with muscle pain syndrome should be cautious about using progesterone on a regular basis to avoid any excess breakdown of protein and muscle tissue.
Another series of Canadian studies of muscle strength in women showed that in women between twenty and thirty years old, voluntary isometric muscle strength is highest around the time of ovulation, when estradiol levels are at their peak than was muscle strength at other times of the menstrual cycle (lower estrogen phase of bleeding or progesterone dominant luteal phase). At menopause, a significant decline in muscle strength was observed, but this decline was not found in women taking postmenopausal estrogen therapy. Again, these findings suggest that women who are having muscle pain syndromes may want to be careful about using daily progesterone to avoid loss of muscle strength.
Progesterone has interesting effects on connective tissues that make up our body’s ligaments and tendons. In pregnancy, as the mother’s body prepares for the baby’s body to be delivered through the birth canal, high levels of progesterone relax or loosen the supporting ligaments of the back and pelvis. This is an adaptive and desirable effect of progesterone to allow the pelvic bones to separate enough for the baby’s head to get through the birth canal. Relaxed ligaments have the unwanted effect of causing backaches in women who are on their feet a lot toward the end of pregnancy. The higher levels of progesterone during the luteal phase of the monthly menstrual cycle has a similar effect on ligaments of the back, hips, and knees, which is one reason we think women athletes have more exercise-related injuries in this phase of the cycle compared to the first half when progesterone is lower.
I recently did a consult for a woman with FMS who had low back pain due to laxity (excess relaxation or looseness) of the ligaments in her sacroiliac joints and pelvis. She had been getting prolotherapy to strengthen these ligaments. This is a series of injections using a sclerosing, or scar-forming, solution to make the ligaments form scar tissue to strengthen them. While prolotherapy can be quite painful, it has clearly helped some people by providing stronger ligamentous support and reducing back pain. The irony was that this woman had been using a daily progesterone cream, incorrectly prescribed at ten times the recommended dose. Here she was, getting painful and expensive injections that were being counteracted by the progesterone high-dose cream she was using. Until our consult, no one had talked to her about these effects of progesterone on connective tissues. She was aghast, and understandably, quite upset to find this out. But since her dose of progesterone cream was so high, she still had a month or more to slowly taper off the progesterone to avoid triggering withdrawal symptoms.
The menstrual cycle ebb and flow of hormones, and balance of progesterone relative to estradiol and testosterone, has effects on multiple metabolic pathways: glycogen storage, caffeine metabolism, protein metabolism, food selection, interleukin concentrations, to name a few. Progesterone and estradiol work together to regulate tissue mass and body composition, in part by altering the enzyme lipoprotein lipase (LPL) activity in fat cells (adipocytes). Estradiol acts to lower body fat (adiposity) by lowering LPL activity, while progesterone increases body fat storage by increasing the activity of the LPL enzyme. Progesterone’s effects to enhance fat storage help the expectant mother store enough fuel to nourish her and the developing baby. And you wondered why it is harder for women than men to lose weight, even with a good exercise program!
Estrogen and progesterone also play a role in insulin response to glucose. Multiple studies, in animal models as well as humans, have confirmed that both hormones increase the pancreatic insulin response to glucose, but estrogen and progesterone have very different effects on insulin sensitivity in other tissues. Progesterone has been shown to decrease insulin sensitivity and to cause resistance to the glucose-regulating effects of insulin. Progesterone’s effect on insulin is quite rapid and can be detected within ten minutes of administering the hormone. It appears to be a direct effect of progesterone on the pancreas itself. This is one of the reasons women often experience increased cravings for sweets in the second half of the menstrual cycle when progesterone rises. Estradiol, on the other hand, has been demonstrated in humans and a variety of animal species to increase insulin sensitivity and improve glucose tolerance. The effect of estradiol on improving glucose handling by the body occurs in both menstruating and postmenopausal women (if the latter are on the patch form of estradiol), as well as in diabetic women. The estradiol-induced improvement in insulin sensitivity has been shown to occur at both fat cells (adipocytes) and skeletal muscle and appears to occur by multiple pathways rather than a direct effect on the pancreas. In order to avoid making glucose control worse, women with diabetes need careful attention to optimal estradiol and the least amount of progesterone that will protect the uterine lining from hyperplasia.
In a normal menstrual cycle with optimal hormone ratios, the opposing actions of estradiol and progesterone on insulin tend to offset each other, which suggests that the E:P ratio is more influential in determining the net effect metabolically. This has been one of the key factors in determining degree of symptoms in the women whose hormone levels I have evaluated in my practice. When their premenstrual (luteal) phase hormone ratios are shifted toward progesterone dominance, and lower than optimal estradiol, they typically have more intense sweet cravings and more weight gain. Prolonged use of progesterone without adequate balance of estradiol has effects on insulin that result in a problem called insulin resistance, which causes weight gain around the middle of the body, increased total cholesterol, lower levels of good cholesterol (HDL), higher levels of bad cholesterol (LDL), and triglycerides (TG). Insulin resistance also causes high blood pressure and significantly increased risk of heart disease from plaque building up in the arteries. The potentially severe complications that occur with insulin resistance make it a crucial factor to consider in determining which hormones are given, and whether they are given orally or should be given in a way that allows them to be absorbed through the skin. I will talk more about insulin resistance in chapter 17, and I will explain how to help reduce this problem with the types of hormone and dietary approaches you select.
Current blood serum tests for progesterone are quite accurate and reliable. The amount of progesterone in the serum reflects the balance, or equilibrium, between the bound and free hormone and gives a total picture of the amount available for the body to use. Since there is a constant dynamic process between the part that is “free” (i.e., biologically active) and the part that is “bound” to carrier proteins, I have found it is important to measure this total amount. A few years ago, I tried using the saliva tests that are now being widely promoted for hormone testing. I initially thought this sounded like a good idea and would be easier for the patients to check at home. For a while, I did both saliva and blood serum tests at the same time in a number of patients to see how well the serum and saliva correlated, and to see if I could just use the saliva tests. I was surprised and quite disappointed to find that these saliva tests turned out to be almost useless. The serum levels were quite consistent and correlated very well with what the women themselves described about body changes that clued them into ovulation and rising progesterone. But the saliva levels were all over the place—from very high to very low and everywhere in between. The saliva results didn’t seem to have any connection with what symptoms the women were describing. I also have many patients who had already had the saliva tests done before coming to see me. Most of these women had been very good at keeping their own records of menstrual cycles and symptoms and had noticed that the saliva results typically were quite different from the body changes that suggested certain hormone levels.
I tried to get information from the companies that provide this testing to account for these differences, and neither Aeron Labs or Diagnos-Techs biochemists would provide the data I requested correlating serum and saliva hormone levels. As a result, I stopped using the saliva tests several years ago. I have continued to use the serum tests that are much more reliable and clinically useful in helping women design appropriate hormone strategies. My approaches are in keeping with the gold standard of using serum levels that is used in worldwide hormone research.
With all the books and multilevel marketing companies trying to sell you on progesterone, I know it is confusing to you as a layperson to sort it all out and determine who has accurate information. You have to remember that many people selling products may have a financial stake in selling you on the idea of using progesterone. You may have heard or read that progesterone has all these wonderful effects in a woman’s body and can be converted into all the other hormones we need. Then I come along and say something different. How are you to know who is right? Let me emphasize, I receive no financial gain from sales of any hormone product. My only desire is to present the most up-to-date, reputable medical research findings to help you “connect the dots” in your health picture. I have presented both the historical and the current worldwide research from reputable medical centers, menopause and PMS researchers, and neuroendocrine basic science researchers to describe in these chapters which functions are known to occur with each of these major hormones.
What you can do to sort out confusing and contradictory information:
First: Pay attention to your own body rhythms, look at a menstrual cycle chart of when each hormone is dominant, and ask yourself “When do I feel the best in my cycle each month?” That will give you an important clue as to whether you feel best when progesterone is the dominant hormone after ovulation until a few days before menses, or whether you feel best in the first half when progesterone is minimal and estradiol is the highest. Based on when you felt your best in the years of healthy menstrual cycles, you can know generally what balance of hormones gave you those good feelings.
Second: Check Medline on the Internet and look up copies of the research I have described and read the conclusions yourself to verify what I have said. Ask other practitioners to give you references and check them out, too.
Third: Ask your local public librarian to help you find a basic medical textbook as a reliable reference to check the list of body functions for these key hormones. There are lots of good ones available.
Fourth: Be skeptical. As in anything, if someone is trying to sell you a product and tell you something that sounds too good to be true, it probably is! I continue to be dismayed and alarmed about the grossly incorrect physiological effects listed in various consumer-oriented books and tapes. The health consequences for women can be disastrous, as we see daily in our practice.
Fifth: Don’t expect a “magic bullet” solution to complex health issues. Rubbing on a body cream containing progesterone simply isn’t adequate for something as complicated as all the metabolic changes that are going on in the premenopausal and menopausal years. I am certainly not recommending that estradiol is the only approach either. There are many complex issues to address, and you need/deserve a thorough medical evaluation with an integrated treatment approach tailored to your individual needs.
Sixth: Use common sense. A recent sales flyer a patient sent me from Florida had this headline: “Estrogen’s Lethal Effects.” Now really . . . would Mother Nature have given us women a hormone that was “lethal” for our entire reproductive lives? Of course not. As you may have guessed, this newsletter was selling . . . progesterone cream as a hormone cure-all. We women live with estrogen all our lives, and most of the serious health problems that affect our quality of life and our longevity don’t start to show up until the primary active estrogen (17-beta-estradiol) is decreasing. So if estrogen were truly “lethal,” most women would be dead long before menopause, since estrogen levels are their highest from puberty until perimenopause. I found the newsletter so ridiculously inaccurate as to be humorous, but the tragedy is that too many women believe it. Obviously, progesterone is an important hormone that plays a critical role in preparing the uterus each month for a possible fertilized egg to implant and in sustaining pregnancy, but being pregnant is not a woman’s only function.
There is so much emphasis on using progesterone, I think people who recommend such broad use of one hormone have forgotten that women have a variety of hormones with different functions, and each one has to be taken into account in our evaluation and treatment approaches. I have found through many years of testing hormone blood levels according to menstrual-cycle phase that the majority of women I have seen actually have low estradiol/high progesterone causing their symptoms. Obviously, if this ratio is the problem, adding more progesterone won’t help and will actually make matters worse. A smaller percentage of the women I have evaluated, perhaps about 5 percent, are found to have the high estradiol/low progesterone levels that were proposed by Dalton and others as the cause of PMS. These are the women I find that do quite well with just supplemental progesterone.
In addition, we have to also keep in mind that many of the same symptoms can be caused or aggravated by loss of thyroid hormone. It certainly doesn’t make sense to give progesterone to these women if the problem really lies in low thyroid function. I think there is a place for use of progesterone in some patients, but I think it has to be individualized, based on the type and pattern of the woman’s symptoms, and what her actual hormone levels show. As every woman knows, what’s crucial for our sense of well-being is the balance of our primary hormones.
Disease in man or woman is never exactly the same as disease in an experimental animal, for in humans the disease at once affects and is affected by what we call the emotional life.
SIR FRANCIS W. PEABODY, M.D.
Harvard Medical School, Boston, 1927
STRESS. For most of us, it conjures up awful images of body-wrecking effects: cancer, heart attacks, high blood pressure, infertility, allergies . . . the list goes on and on. But all of us live with stress, all of the time, both the stress of constant change going on within the body systems, and the stress of constant interchange with the outside world. Stress is a constant, necessary part of the life process itself. But what accounts for the fact that some people seem to thrive on the very stress levels that others would find overwhelming? What makes some people able to cope with catastrophic stress and others cave in with what appear to be rather trivial events? Physicians and scientists have debated these questions down through the ages. Louis Pasteur developed the germ theory of illness and believed that our exposure to external agents triggers disease. A physician and contemporary of his, Claude Bernaud, believed that the “soil” or environment of the body was the crucial factor. The two often debated who was right, but on his deathbed, Pasteur murmured, “Bernaud was right, it is the soil.”
Today, we are even more aware of the role our individual vulnerability brings to the question of who gets ill. Viruses, bacteria, carcinogens alone do not cause illness in every individual exposed to them. We now know that many other factors are involved: our attitudes, our diet, our hormone balance, how tired we are, our feelings of choice and control in our lives, our degree of social support, our faith—to name a few. A few diseases, such as cystic fibrosis, are almost entirely genetic, but most of the diseases we “moderns” develop are predominately affected by the physical and psychological environment of our bodies. Have we made our bodies a compromised host, a fertile “soil” for viral and carcinogenic invaders? Or have we developed lifestyle habits and thought patterns that serve as an inoculation against the development of disease? The balance between the risk factors we have and the “resistance resources” helps determine whether we stay healthy or develop an acute or chronic illness. So, as we shall see in later chapters, there is a lot we can take charge of now that will improve our ability to resist the ravages of stress causing adverse effects on our health. But now, let’s explore this idea of stress further, and understand how it plays a role with women’s overall hormonal health.
For both men and women, stress of whatever form—external situational and environmental stressors or internal body changes (physiological stressors)—that requires the body to continually adapt, affects the brain and body. Our body is the “final common pathway” through which all of these changes act and operate to produce necessary responses. Our brain constantly perceives and processes information coming to it from the world around us and also from moment-to-moment changes inside the body. Our brain is a physiological organ, as well as the psychological organ of “mind” expressing our personality and guiding our behavior. Since the brain is affected by outside stimuli (stressors) and by internal stimuli (stressors) or changes in the body, that means thoughts, moods, and behaviors governed by the brain can be caused by both physical and psychological causes.
I find that many times patients have been told that they have a psychological or psychiatric disorder simply because of changes in mood or behavior and such symptoms are assumed to have a psychological cause. But these same mood/behavior symptoms may in fact be caused by biochemical changes in our body’s physiological balance, and therefore have a physical cause. Likewise, psychological stress causes profound changes in every cell in the body, including our immune cells, pain-regulating neurotransmitters, nerve endings, brain chemistry, and so on. With prolonged stress of any kind—physical, environmental, situational, psychological, spiritual—the body’s balance, or homeostasis, is disrupted and we see symptoms that relate to overactivity of the “fight-or-flight” (adrenaline) pathways, such as headaches, acute muscle spasm and pain, high blood pressure, panic attacks, irritable bowel, colitis, angina, eczema, overwhelming fatigue, and many others. Diagram 2.3 in chapter 2 showed these important connections. The interconnections and the ways in which hormonal production may in turn be altered by stress on the body are often overlooked when women seek medical care. The two-way nature of these pathways is crucial to all facets of women’s health.
Another aspect of the problem of stress when it affects women is the role of chronic stress in decreasing the normal function and hormone production of the ovaries, as well as the thyroid gland. A variety of studies has shown a correlation between the presence of life stress in women’s lives and lower levels of their ovarian estrogen, testosterone, and as well as changes in the cyclic production of progesterone. While one can look at all the data on stress effects and conclude that psychosocial stress and poor coping skills may result in estrogen decline at menopause, it is possible that the opposite hypothesis may also be true about the connection between hormone levels and stress: Declining estrogen levels contribute to alterations in the function of norepinephrine, serotonin, dopamine, and acetylcholine, which regulate pain pathways, sleep, muscle repair, mood, behavior, and cognitive function. I think that the declining estrogen, as well as adverse effects on brain chemical messengers, contributes to the observed difficulty coping with psychosocial stressors by women who have previously been able to cope successfully. Once again, the role of stress is a two-way street: Life stress suppresses the ovaries, which decreases estrogen production, which affects sleep, which increases pain, and then increased pain disrupts sleep, decreases growth hormone production, and leads to further decline in ovary hormones, and so on. Normal declines in estrogen affect brain chemistry, which affects ability to cope with stress. It’s another one of those vicious cycles.
Stress also has adverse effects on the brain and body through mechanisms beyond the ovary hormones. Chronic persistent stress causes excessive outpouring of cortisol and other stress hormones from the adrenal glands. High levels of cortisol over time have many adverse effects: (1) suppression of normal immune function, (2) weight gain around the middle of the body (“apple” shape), (3) increased risk of heart disease by promoting plaque build-up, higher cholesterol and triglyceride levels, (4) increased risk of diabetes by stimulating high levels of blood glucose, (5) negative effects on pain pathways, such as increasing brain excitability, via release of excitatory amino acids (EAAs), glutamate, and aspartate. This effect occurs by the action of adrenal stress hormones on sodium, potassium, and calcium ion transport into and out of cells. Cortisol overactivity causes excessive buildup of the EAAs, which then mobilizes calcium in the postsynaptic neuron and leads to overactivation of calcium-dependent enzymes and free-radical-producing cascades. The end result of all this is that neurons begin to die, leading to impaired nerve conduction, abnormal pain regulation, and impaired memory, attention, and concentration. Sound familiar? As stress persists, cortisol effects continue to build up over time, further damaging astrocyte nerve cells in the hippocampus of the brain (memory center). This whole sequence is thought to be one way that memory loss gets worse in chronic pain sufferers, leading to what’s euphemistically called “fibro-fog” or “brain fog.”
In addition to toxic effects on neurons of the brain, excess cortisol impairs normal metabolism of collagen, which is the basis of healthy connective tissue, or fascia. This adverse effect on connective tissue is part of an overall response of the body to stress that leads to hyperglycemia or elevated blood sugar that over time can increase risk of diabetes. The accumulation of cortisol effects further disrupt the sleep cycle, which in turn means less muscle repair at night, aggravating the damaging effects of declining estradiol. Excess cortisol also interferes with normal thyroid function, leading to less of the available T3 that is so important for cellular metabolism in skeletal muscle, the brain, and other organs. High cortisol levels and prolonged stress also increase the body’s need for antioxidants, vitamins, and minerals as well as all the macronutrients. But when we are stressed and don’t feel well, we pay less attention to getting what we need nutritionally.
It is a complicated picture, and one that has profound implications for all aspects of women’s health. The cumulative effects of persistent high cortisol levels and chronic stress adversely affect practically every pathway in the body. I don’t have the space in this book to go into more detail on all the potential health consequences of chronically elevated cortisol and ongoing stress, but if you would like more information, I recommend the book Why Zebras Don’t Get Ulcers, by Robert M. Sapolsky, W. H. Freeman and Company, 1998. It is an excellent, and humorous, review of the damaging effects of excess corticosteroids over time.