DIAGNOSIS
Anger and aggression are fundamental reactions throughout the animal kingdom. Defending against intruders and hunting for the next meal are traits that were essential for the survival of our ancestors. However, some individuals are too aggressive. We all know a few dogs (and relatives for that matter) that are easily agitated and quick to bite. Animals and people with this tendency are a significant social problem.
Terms such as road rage, spouse abuse, and school violence are all too common in our daily papers. Yet, the Diagnostic and Statistical Manual (DSM) does not include a category for inappropriate anger. It has been suggested this is because men created DSM and they do not see anger as a problem. (PMS, on the other hand, is now a disorder!)
The absence of a diagnostic category is clinically relevant. For example, a small Danish pharmaceutical company in the 1970s was pursuing a treatment for aggression, called serenics. In spite of promising results, the company shelved the medication when it became clear the US Food and Drug Administration would not approve the medication because aggression is not a specific disorder. Consequently, although psychologists and other counselors provide treatment for “anger management,” there is no sanctioned pharmacologic intervention for excessive anger and irritability.
Aggression is clearly influenced by one’s culture and upbringing. Violence on TV and early physical abuse increase the likelihood a person will be aggressive. Alternatively, the context in which an assault occurs determines the appropriateness of the aggression. For example, fighting on the ice at hockey games is accepted, but fighting in the stands is not. These are issues beyond the scope of this text. We are interested in the processes in the brain that generate or fail to impede violence toward another.
Two Kinds of Aggression
Working with cats, Flynn at Yale, and Siegel at the University of Medicine and Dentistry of New Jersey, identified two types of aggressive behavior. One is more predatory—similar to hunting—the cat quietly and calmly stalks his prey. The other type of aggression is defensive. Here the cat is agitated and makes a big display of his feelings, in part to avoid a fight, but is also ready to respond if provoked. In the cat, these different responses can be elicited by electrical stimulation of different regions of the hypothalamus.
MECHANISMS IN THE BRAIN
Hypothalamus
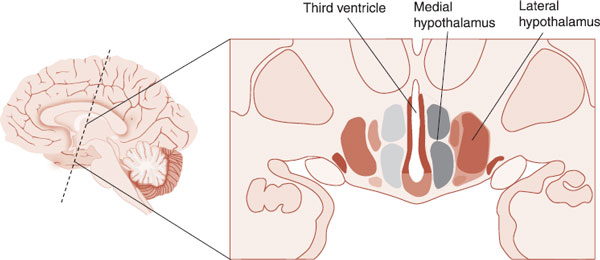
In a series of experiments over many years, Flynn and Siegel placed electrodes into the hypothalamus of cats and searched for the regions that would, with stimulation, elicit aggression. Remarkably, they found separate regions that elicited the two kinds of aggressive behaviors observed in cats. Figure 14.1 shows the location of the hypothalamus and the two general areas (lateral and medial) on either side of the third ventricle that correspond with predatory and defensive aggression.
Figure 14.2 shows an example of predatory aggression elicited in a cat by stimulation of the lateral hypothalamus. The bite to the back of the neck is preceded by quiet, stealthy circling of the rodent. It is worth noting that the researchers used cats in these experiments that would not bite the rat before the hypothalamic stimulation.
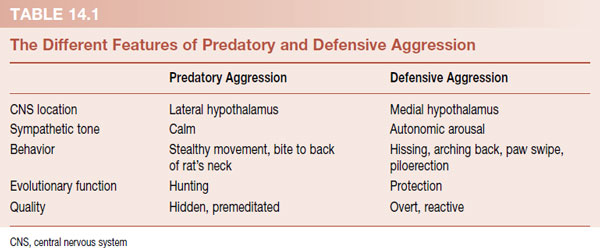
Figure 14.3 shows the defensive type of aggressive behavior induced by stimulating the medial hypothalamus. In this case, the cat becomes aroused (high sympathetic tone, increased heart rate, dilated pupils, etc.) and displays hostile behavior (hissing, growling, arching back, piloerection, etc.). The different features of each kind of aggression are summarized in Table 14.1.
FIGURE 14.1  The medial and lateral regions of the hypothalamus.
The medial and lateral regions of the hypothalamus.
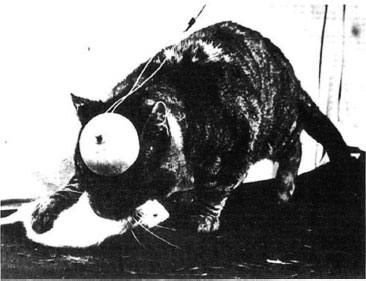
FIGURE 14.2 Predatory attack (quiet bite) against a rat induced by stimulating the lateral hypothalamus. (From Flynn JP. The neural basis of aggression in cats. In: Glass DC, ed. Neurophysicology and Emotion. New York: Rockefeller University Press; 1967:40–60.)
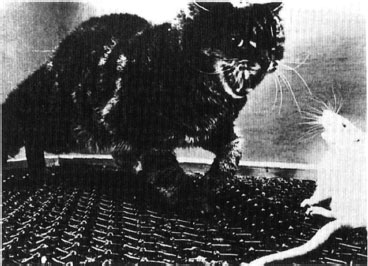
FIGURE 14.3 Defensive attack elicited by stimulating the medial hypothalamus. (From Flynn JP. The neural basis of aggression in cats. In: Glass DC, ed. Neurophysicology and Emotion. New York: Rockefeller University Press; 1967:40–60.)
These two pathways and subsequent behavior elicited in the cat also describe the two basic kinds of aggression seen in humans. Analysis of playground behavior, spousal abuse, and serial killers supports the dichotomy of a reactive/impulsive/defensive type of aggression and a stealthy/premeditated/hunting type of aggression, although a combination of the two types is a common finding in any specific aggressive act (see Treatment box, page 166).
Frontal Cortex
Random acts of aggression are a problem for any species. The brain has mechanisms to modify aggressive behavior either by putting on brakes or by applying an accelerator. The frontal cortex is well known for controlling the impulsive behavior. Impairment of the frontal cortex is the equivalent of taking off the brakes on aggressive impulses. The most famous example of this is Phineas Gage. Gage was a foreman at a railroad construction company in Vermont in 1848. A tamping iron was blown through his left frontal skull when a spark inadvertently ignited the explosive powder.
Gage’s skull has been preserved, and Figure 14.4 shows a reconstruction of the path the tamping iron took through his skull. Remarkably, he recovered, was out of bed within a month, and lived another 12 years. However, his personality had drastically changed. While before the accident he had been efficient, balanced, and responsible, now he was fitful, impulsive, unfocused, and easily agitated.
If we imagine that the frontal cortex applies the brakes to the array of primitive impulses that arise from the subcortical brain, then we can see how taking the brakes off (due to a poorly functioning frontal cortex) allows the expression of feelings that would normally be subdued. Specifically, a poorly functioning frontal cortex allows more aggressive impulses to be expressed. Alternatively, a healthy, active frontal cortex puts the “brakes” on inappropriate aggressive behavior.
Experiments out of Siegel’s lab provide alternative evidence of the important role the frontal cortex plays in restraining aggression. In this study, a cat has one electrode in his lateral hypothalamus and one in the lateral aspect of his frontal cortex. What is being measured is the time until the cat attacks the rat after stimulation of the electrodes. With just hypothalamic stimulation, the cat only waits approximately 12 seconds before attacking. However, with stimulation of both the hypothalamus and the frontal cortex, the time to attack is doubled (Figure 14.5).
This study was repeated with many cats with electrodes in different locations of the frontal cortex. Similar results were found. Clearly, the frontal cortex has an inhibitory effect on aggressive expressions. It is unfortunate that we have not found a way to “beef up” a wimpy frontal cortex.
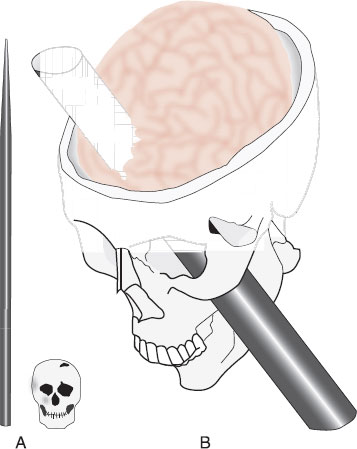
FIGURE 14.4 A. The skull of Phineas Gage and the tampering iron that exploded through his head in 1848. B. Drawing of a computerized reconstruction of the path the rod took through his skull and brain. The damage involved both left and right prefrontal cortices. (Adapted from Damasio H, Grabowski T, Frank R, et al. The return of Phineas Gage: clues about the brain from the skull of a famous patient. Science. 1994;264:1102-1105.)
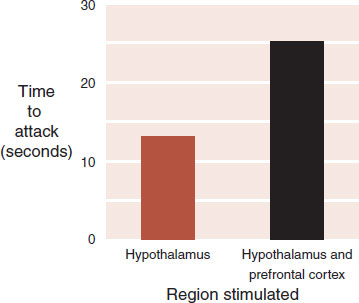
FIGURE 14.5 The time it takes a cat to attack a rat after the hypothalamus is stimulated is greatly increased when the frontal cortex is simultaneously stimulated. (Adapted from Siegel A, Edinger H, Dotto M. Effects of electrical stimulation of the lateral aspect of the prefrontal cortex upon attack behavior in cats. Brain Res. 1975;93:473-484.)
PSYCHOSURGERY
There are few studies in the medical literature involving the hypothalamus and aggression in humans, with the exception of a few reports of psychosurgery. For example, in Japan, Sano and Mayanagi performed 60 posteromedial hypothalamotomies in the 1960s for aggressive behavior. Most patients also had a history of seizures and mental retardation. In a follow-up report conducted in 1987, Sano and Mayanagi reported the absence of violence and aggression in 78%, with apparently normal endocrine function. Although a drastic procedure, it accentuates the central role of the hypothalamus with aggressive behavior.
One of the most consistent findings with humans and violence is frontal lobe dysfunction. With the advent of neuroimaging capabilities, many researchers have looked at the activity in the prefrontal cortex (PFC) in men with violent histories. In a review of the literature on the topic, Brower and Price concluded that significant frontal lobe dysfunction is associated with aggressive dyscontrol—in particular, impulsive aggressive behavior.
A study of convicted murderers by Raine et al. provides further insight on this topic. Raine separated a group of murderers into those who committed planned, predatory violence and those who perpetrated affective, impulsive violence. Positron emission tomography scans were conducted on these subjects along with normal controls, examining the activity in the frontal cortex. The results are shown in Figure 14.6. Both groups of murderers had less activity in the PFC compared with controls, but the impulsive, affective group had the least. One wishes there was a way for men in prison to exercise and strengthen their frontal cortex as much as they exercise their biceps.
Amygdala
There is conflicting information about the role of the amygdala and aggressive behavior. Although better known for being activated during fearful situations, the amygdala may have a broader function in processing emotional stimuli. Early studies with monkeys showed that the bilateral removal of the amygdala produced an animal that was placid—neither frightened nor aggressive. This is called the Klüver-Bucy syndrome, after the two researchers who performed the experiments. This and other research suggest that the amygdala is instrumental in recognizing whether a stimulus is threatening and that an overactive amygdala can lead to excessive defensive aggression.
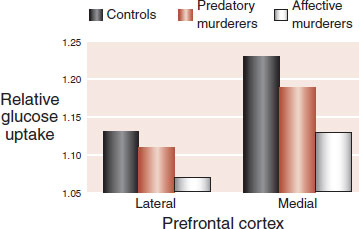
FIGURE 14.6 The relative activity in the lateral and medial aspect of the prefrontal cortex of predatory and affective murderers compared with normal controls. (Adapted from Raine A, Meloy JR, Bihrle S, et al. Reduced prefrontal and increased subcortical brain functioning assessed using positron emission tomography in predatory and affective murderers. Behav Sci Law. 1998;16(3):319-332.)
There are reports in the literature of bilateral amygdalotomies for untreatable aggression in humans. Some of the reports are disturbingly optimistic. A group from India reported on 481 cases, stating that 70% showed excellent or moderate improvement after 5 years (see Prefrontal Lobotomy box, page 18 for another example of psychosurgery hyperbole). A report about two cases in Georgia provides a more balanced assessment of the procedure.
Two individuals who were essentially institutionalized because of aggressive behavior received amygdalotomies after years of failed medical therapies. The procedures resulted in reductions but not elimination of the assaultive behavior. Pre- and postassessments demonstrated reduced autonomic arousal as measured by skin conductance. The authors concluded that the procedure resulted in a “taming effect,” which they attributed to reduced perceptions of threats. In other words, an overactive amygdala causes the individual to perceive threats where they do not exist. Removing the amygdala decreases the false perceptions.
DISORDER
VIOLENCE AND AGE
Age has a profound effect on the likelihood of being violent. The incidence of violent crime rises rapidly until the ages of 18 to 22 and then gradually declines over the next three decades. The very young and very old are the least violent. There are many sociocultural variables that contribute to this trend. However, the delay in the maturing of the brain compared with the fully developed physical body provides one explanation (see Figure 8.7). The young adult does not have enough containment by the frontal cortex of his aggressive impulses.
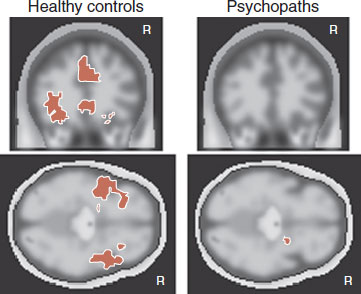
Other research suggests that the amygdala is underactive in those with aggressive problems (see section “The Psychopath” in the subsequent text). Recent imaging studies have found that amygdala dysfunction is associated with criminal psychopaths. One study in Finland showed decreased volume of the amygdala in a group of psychopaths. Another study used functional magnetic resonance imaging to examine the activity of the amygdala during memory tasks involving negatively charged words. The psychopaths showed less amygdaloid activity compared with controls (Figure 14.7). These studies suggest that an underactive amygdala may facilitate aggression.
The work by Siegel with his cats may shed light on the conflicting data about the role of the amygdala in aggressive behavior. We must remember that the amygdala is not just one organ but is made up of multiple nuclei (see Figure 2.7). Siegel found with cats that stimulating the lateral and central groups facilitates predatory attacks and suppressed defensive rage. Conversely, stimulation of the medial aspect of the basal complex has just the opposite effect. This subtle difference within the amygdala would be hard to identify in humans with current imaging technology. The amygdala may be overactive with different subtypes of aggression and underactive with others. Alternatively, it could be that different nuclei are activated for the different types of aggression.
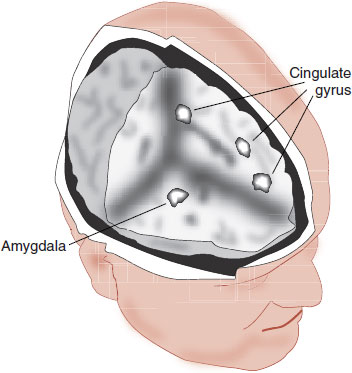
FIGURE 14.7 Criminal psychopaths showed less activity in the amygdala along with parts of the cingulate gyrus when recalling negative affective words compared with controls. (Adapted from Kiehl KA, Smith AM, Hare RD, et al. Limbic abnormalities in affective processing by criminal psychopaths as revealed by functional magnetic resonance imaging. Biol Psychiatry. 2001;50:677-684.)
An old case recently came to our attention that emphasizes the points of this section. Charles Whitman was described as an intelligent, loyal young man who was leading an uneventful life until he started to struggle with episodes of anger in his early twenties. In March 1966, he sought psychiatric help at the University of Texas Medical Center, but failed to return after the initial, psychoanalytic evaluation. In August, after killing his mother and wife—whom he professed to love—he climbed the tower at the University of Texas and shot 48 people, killing 16. At autopsy, a walnut-sized glioblastoma was discovered beneath the thalamus pressing on the hypothalamus. The tumor also extended into the temporal lobe and was compressing the amygdala.
It is impossible to identify what caused the emergence of Whitman’s unimaginable violence. He was abusing amphetamines (Dexedrine) at the time of shooting and was raised in a dysfunctional family with an abusive father. However, it is likely that some of the murderous rage resulted from the tumor’s compression of the hypothalamus and amygdala.
HORMONES AND NEUROPEPTIDES
Testosterone
Everyone “knows” that testosterone stimulates aggression. Males fight more than females. It seems like a “no-brainer.” Fortunately, the role of testosterone and aggression is not as simple as it first seems.
In 1849, Arnold Adolph Berthold, a German physician, conducted an experiment that is considered the first formal study of endocrinology (Figure 14.8). With this elegant little study, he demonstrated the importance of a substance from the testes (later discovered to be testosterone) and aggressive behavior.
Berthold knew that male chicks grow into roosters with typical secondary sexual characteristics, displaying sexual and aggressive behavior. In the experiment, Berthold removed the testes from chicks, which curtailed their normal development and eliminated the sexual and aggressive behavior. In a second group, he reimplanted the testes into the abdominal cavity. If the testes could establish a blood supply, the chick would develop into a normal rooster with the usual sexual and aggressive tendencies. Berthold concluded that the testes release a substance that affected the male body structures and behaviors.
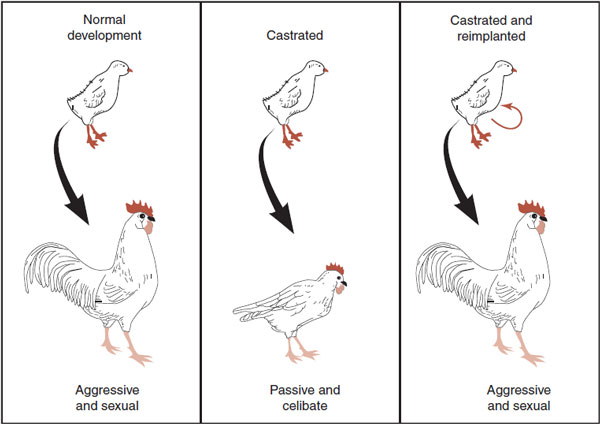
FIGURE 14.8 Berthold established in 1849 that a substance in the testes was necessary for the development of male behavior and body structure. (Adapted from Rosenzweig MR, Breedlove SM, Watson NV. Biol Psychol. 4th ed. Sunderland, MA: Sinauer; 2005.)
Research with laboratory animals in the years since Berthold have consistently demonstrated similar correlations between testosterone and aggressive behavior. A good example by Wagner et al. shows the effect of castration on bite attacks on an inanimate target for adult male mice (Figure 14.9). Before castration and with testosterone replacement, the male mice will frequently bite the target. However, in the absence of the hormone, bite attacks drop close to the frequency seen with females.
For humans, it is not so easy to establish a direct link between plasma testosterone and magnitude of hostility. Conflicting results are found throughout the literature. In particular, it is hard to establish the cause and effect. For example, a popular study is to compare testosterone levels in male prisoners with their crimes. As expected, the more aggressive prisoners have higher levels of testosterone, but so do the socially dominant, non-aggressive inmates. A recent study with baboons sheds light on this issue. The researchers followed the changing social rank for 125 adult males from five social groups over 9 years. Simultaneously, they collected fecal samples to measure testosterone as well as glucocorticoid (stress hormone). Their results are shown in Figure 14.10. It appears that plasma testosterone rises as one ascends the social ladder. The inverse is true for the glucocorticoids except for the highest ranking male. (Sapolsky, in an editorial on this article, expressed sympathy for the poor CEO [alpha male] who, although at the top of the pyramid, is more stressed than his immediate subordinate.)
Another popular belief is that exogenous steroids that some athletes take to enhance performance increases aggression in most men: “roid rage.” This too is murky. In the best study of the effects of supraphysiologic doses of testosterone on normal men, Tricker et al. found no difference in anger for those on either testosterone or placebo, as noted by the spouse or by self-report after 10 weeks. Likewise, studies of sexual predators treated with antiandrogens have demonstrated remarkable decreases in libido but with little change in aggression.
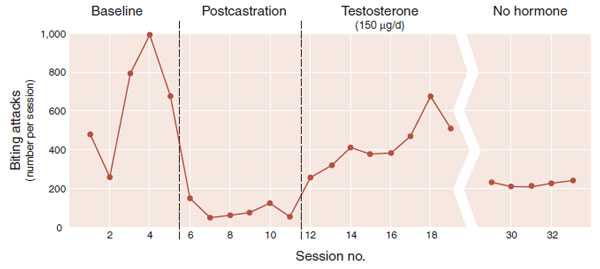
FIGURE 14.9 Baseline bite attacks for male mice are markedly diminished with castration. This effect can be reversed temporally with testosterone replacement. (Adapted from Wagner GC, Beuving LJ, Hutchinson RR. The effects of gonadal hormone manipulations on aggressive target-biting in mice. Aggress Behav. 1980;6:1-7.)
It appears that testosterone, besides its physical affects on sexual characteristics, has behavioral affects that might best be described under the umbrella of dominance behavior, that is, a display of behaviors to achieve and maintain a higher social status. There are a host of behaviors such as staring, tone of voice, cajoling, projecting confidence, and monopolizing the conversation that can advance one’s social position. These behaviors, what we sometimes call “mojo,” might be enhanced by testosterone. This is in stark contract to the traditional view of testosterone as a hormone that incites antisocial, egotistical, and even aggressive behaviors.
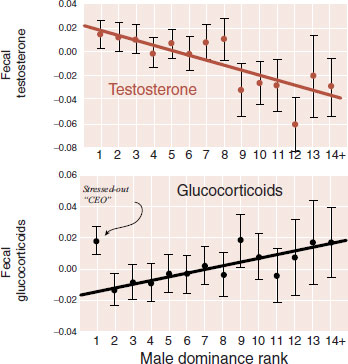
FIGURE 14.10 Testosterone levels rise as baboons ascend in social rank. Glucocorticoids, with the exception of the alpha man, descend with rank. (Adapted from Gesquiere LR, Learn NH, Simao CM, et al. Life at the top: rank and stress in wild male baboons. Science. 2011;333:357-360.)
Vasopressin
Vasopressin, better known for its role as an antidiuretic hormone and its physiologic effect on water retention and bedwetting, is increasingly recognized as playing an important in social attachment. Many neuropeptides have multiple functions in the brain: both physical and behavioral. We are only beginning to understand the role of vasopression in the aggressive behaviors. When given to hamsters, rats, and voles, for example, vasopressin will increase their aggressive display. Alternatively, vasopressin receptor blockers will decrease aggression.
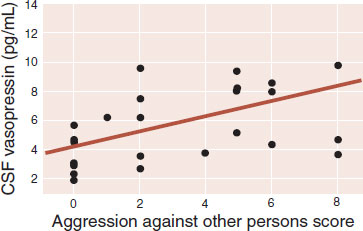
A remarkable study by Coccaro et al. has looked at cerebrospinal fluid (CSF) vasopressin and aggression in 26 subjects with personality disorders. Figure 14.11 shows the correlation between CSF vasopressin and a life history of aggression against other people. The importance of vasopressin in social interactions goes beyond aggression. We also see this peptide involved with bonding and will discuss it further in Chapter 17. In the future, this may be a neuropeptide with great interest for the mental health community.
FIGURE 14.11 Cerebrospinal fluid vasopressin levels correlate with aggression in subjects with personality disorders. (Adapted from Coccaro EF, Kavoussi RJ, Hauger RL, et al. Cerebrospinal fluid vasopressin levels: correlates with aggression and serotonin function in personality-disordered subjects. Arch Gen Psychiatry. 1998;55:708-714.)
Nerve Growth Factors
It is interesting to ask whether fighting changes the brain. That is, does winning or losing alter the structure of the brain in a manner that develops aggressive or submissive personalities? We know there is a strong relationship between experience and neurobiology, for example, enriched environments cause enhanced nerve cell growth (see Figure 8.5). Likewise, we know that the growth and development of neurons are enhanced by nerve growth factors (NGFs). Finally, we know that animals that are repeatedly on the losing side of fights will develop a syndrome called conditioned defeat.
A group in Italy has examined the effect of winning and losing on growth factors in mice. Figure 14.12A shows the rapid and sustained release of NGF into the bloodstream immediately after a fighting episode. Further studies looked at growth factors in areas that are known for the proliferation of new nerve cells, for example, the subventricular zone (SVZ) (see Figure 8.3). The researchers found enhanced levels of NGF as well as brain-derived neurotropic factor (BDNF). However, the levels depended on who won the fight.
Figure 11.12B shows the results of NGFs in the SVZ after three consecutive days of fighting episodes. It was only the subordinate mouse that had increases in NGF. The dominant mouse had increased levels of BDNF. These results suggest that winning or losing turns on different genes which may affect which growth hormones are released and which nerves are “fertilized.” If this is true, it may explain why winners and losers behave differently.
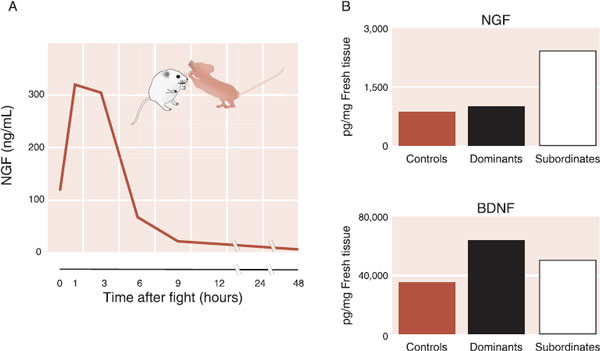
FIGURE 14.12 A. Fighting results in an increase in nerve growth factor (NGF). B. In the subventricular zone, NGF only increases for the subordinate mouse, whereas brain-derived neurotropic factor (BDNF) increases for the dominant mouse. (Adapted from Fiore M, Amendola T, Triaca V, et al. Fighting in the aged male mouse increases the expression of TrkA and TrkB in the subventricular zone and in the hippocampus. Behav Brain Res. 2005;157(2):351-362 and Branchi I, Francia N, Alleva E. Epigenetic control of neurobehavioural plasticity: the role of neurotrophins. Behav Pharmacol. 2004;15(5-6):353-362.)
LITHIUM
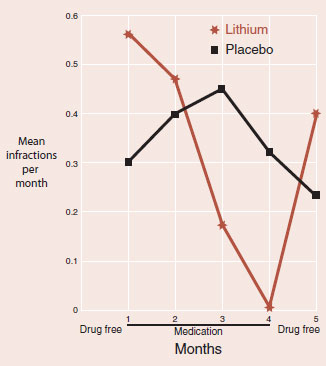
One of the most unique treatment studies for aggressive behavior was conducted in a prison in Connecticut in the 1970s. Volunteers with a history of violence were randomly assigned to receive lithium or placebo. The exclusion of inmates with psychosis was the only psychiatric criterion applied to this study. The number of infractions reported by the institutional staff that was blind to the treatment administered served as the measure of response. The following figure shows the results.
Although the study has methodological problems (small n, high dropout rate for those on lithium), it nonetheless demonstrates the powerful effect that lithium has on violent behavior. This is consistent with lithium’s well-documented capacity to decrease suicide—which can be considered violence against oneself. What lithium does in the brain to reduce violence remains a mystery.
SEROTONIN
There is actually a more robust association between low serotonin and aggression than between low serotonin and depression. Because there is no feasible way to directly measure serotonin in humans or animals, most studies examine the correlation between violence and CSF 5-hydroxyindoleacetic acid (5-HIAA), a metabolite of serotonin.
Studies with monkeys have found high rates of wounding, violence, and inappropriate aggression in subjects with low CSF 5-HIAA. Analysis of these monkeys has shown that they are not necessarily uniformly more aggressive. However, they are more likely to engage in rough interactions that escalate into unrestrained aggression with a high probability of injury. This behavioral trait can be viewed as poor impulse control, which could underlie the aggressive tendency.
A group has studied the relationship between 5-HIAA and violence in a longitudinal study of free-ranging rhesus monkeys secluded on a small island on the coast of South Carolina. The researchers captured 49 two-year-old males and measured their CSF 5-HIAA. Two years is the age for a monkey that corresponds to middle to late childhood in humans and is a particularly dangerous age for male monkeys. This is a phase of life when males move from their group of origin to a new social group. The monkeys were followed for up to 4 years.
By the time most of the subjects had reached young adulthood, 11 had died. Figure 14.13 shows the percentage of subjects that died and the percentage that had survived, separated by their CSF 5-HIAA concentrations at the start. Note that all those in the high concentration group were still alive. The researchers observed that those monkeys with the lowest levels of 5-HIAA were much more likely to engage in risky behavior, including aggressive acts directed at older, larger males. They would pick fights they could not win. They were not only aggressive but also impulsive.
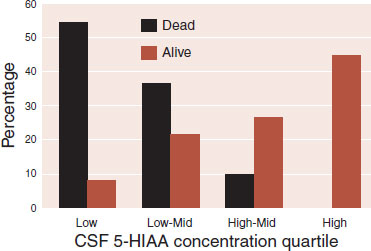
FIGURE 14.13 The percentage of 2-year-old monkeys who are still alive after 4 years, separated by the metabolite of serotonin (5-HIAA) in the CSF. (Adapted from Higley JD, Mehlman PT, Higley SB, et al. Excessive mortality in young free-ranging male nonhuman primates with low CSF 5-hydroxyindoleacetic acid concentrations. Arch Gen Psychiatry. 1996;53(6):537-543.)
Studies with humans are equally impressive. A variety of researchers from many different sites have shown the following results:
1. Lower 5-HIAA correlates with greater suicide intent and higher lethality in those who have attempted suicide.
2. 5-HIAA levels show an inverse correlation with lifetime histories of aggression.
3. Low 5-HIAA levels predict recidivism for violent offenders.
4. Acute tryptophan depletion, which causes a transient decline in brain serotonin, will result in increased irritability and aggression.
Most relevant for the practicing clinician are the studies with selective serotonin reuptake inhibitor (SSRIs) and aggression. Several double-blind, placebo-controlled studies have found reduced aggression with SSRIs in patients with personality disorders, autism, schizophrenia, and dementia. While there are no medications with FDA approval for treating aggression, a serotonin reuptake inhibitor might not be a bad place to start.
THE PSYCHOPATH
Being violent is not the same as being cruel or mean. Violence in defense of oneself or one’s family is not even considered a crime. Alternatively, there are many examples of violence that seems to have no purpose other than being mean and inflicting emotional or physical pain.
Psychopathy is the closest definition we have in psychiatry to describing cruel or mean behavior. It is not included in the DSM. The Psychopathy Checklist-Revised created by Robert Hare defines psychopathy and is made up of two factors. The first factor includes impulsive aggression and a wide variety of offenses, which correlates closely with antisocial personality disorder in the DSM.
The other factor defines the emotional shallowness of the psychopath: superficial, egotistical, lack of remorse, lack of empathy, and manipulative. This factor has a smaller correlation with antisocial personality disorder and more closely resembles what we would consider cruel and mean. It tends to persist as the subject ages, although the impulsive, aggressive factor decreases with maturity. The older psychopath is no more empathetic or remorseful, but less likely to be violent.
Hare has suggested that the psychopath lacks some internal control. We know very little about this which is unfortunate because psychopaths are a huge drain on society and there remains no effective treatment. However, the advent of functional imaging studies brings some insight to the neural workings of the average psychopath.
Raine has shown that men with antisocial personality disorders have decreased prefrontal gray matter when compared with normal controls or substance abusers. This suggests a lack of containment from the frontal cortex, similar to what has been discussed earlier. Unique to the psychopath are findings showing low autonomic arousal and less activity in the amygdala.
Resting Heart Rate
One of the most consistent physiologic findings in psychiatry is the correlation between low resting heart rate and aggressive behavior in children. Furthermore, a low heart rate in a child is predictive of future criminal behavior independent of all other psychological variables. Some people speculate that the low heart rate reflects a fearless, stimulus-seeking temperament. A fascinating study from Europe supports this conclusion.
The study is based on Pavlovian (classical) conditioning. When presented repeatedly with a neutral stimulus followed by an aversive stimulus, most people will show some anxiety when seeing the neutral stimulus in anticipation of what will follow. Birbaumer et al. scanned 10 criminal psychopaths out on bail and 10 healthy controls repeatedly presented with neutral pictures followed by painful stimuli. The controls showed increased activity in areas underlying conditioned fear response: amygdala, orbitofrontal cortex, insula, and anterior cingulate (Figure 14.14). Remarkably, the psychopaths showed almost no activity in these areas. This disconnect between emotion and cognition may be the neural basis for the cold, detached demeanor of psychopaths. It is also one more reason your authors will never be successful criminals.
The Pleasure of Violence
The lack of fear alone does not seem sufficient for some of the cruel actions perpetrated by psychopaths. Many people can utilize their fearless temperament to help others. For example, decorated bomb-disposal operators have been shown to have unusually low heart rates during experimental simulations. We can imagine that other high-stress professions are overly represented with individuals who are innately calm: firefighters, air-traffic controllers, trauma surgeons, etc. Something else is needed to understand the behavior of the psychopath. A study with rats suggests a possible neurologic mechanism to explain what else may be aberrant with psychopaths.
FIGURE 14.14 Healthy controls show a robust fear response in anticipation of an adverse stimulus. Psychopaths fail to develop a similar fear. (Adapted from Birbaumer N, Veit R, Lotze M, et al. Deficient fear conditioning in psychopathy: a functional magnetic resonance imaging study. Arch Gen Psychiatry. 2005;62(7):799-805.)
First, we must acknowledge that many people enjoy violence. One has to only look at what is popular at the movies, in video games, and on the news to recognize that blood sells. Second, as we described in Chapter 12, the nucleus accumbens lights up with dopamine during pleasurable activities: cocaine, sex, gambling, and so on. It seems logical that violence induces a squirt of dopamine at the nucleus accumbens.
The missing study is shown in Figure 14.15. In this experiment, male rats were implanted with micropipettes that sampled the extracellular concentration of dopamine at the nucleus accumbens every 10 minutes. The sampling was done during an aggressive encounter with a naive male intruder in which two to six bites and at least 140 seconds of aggressive behavior were displayed by the rat under study. The graph shows that dopamine significantly rose above baseline for up to 60 minutes after the encounter. The thrill of victory?
DISORDER
TEMPORAL LOBE EPILEPSY
There is a subgroup of patients with temporal lobe epilepsy who have aggressive outbursts between seizures. Some have attributed this to an interictal syndrome often called episodic dyscontrol. However, many of these patients have alternative explanations for their aggression, for example, low IQ and antisocial personality disorder. The concept remains controversial but may apply to a few patients with seizure disorder.
More appealing is the prospect that patients with aggressive outbursts may be having unrecognized subclinical temporal lobe seizures. Unfortunately, this has been difficult to substantiate. However, the anticonvulsants do show some positive effects as treatment for aggression, although the benefits are primarily limited to those with impulsive aggressive acts rather than premeditated acts.
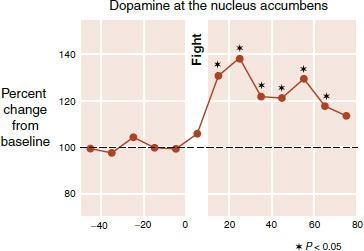
FIGURE 14.15 Increase in dopamine at the nucleus accumbens following an aggressive encounter with another rat. (Adapted from van Erp AM, Miczek KA. Aggressive behavior, increased accumbal dopamine, and decreased cortical serotonin in rats. J Neurosci. 2000;20:9320-9325.)
Imaging studies of humans suggest similar neural mechanisms. Researchers in Switzerland set up an elaborate study to examine the activity in the brain when a subject is playing a game with an untrustworthy partner. In instances when the subject wants to retaliate after the partner keeps all the money, there was increased activity in the dorsal striatum—an area that contains the nucleus accumbens. Furthermore, the stronger the activity in the striatum the more willing the subject was to incur a deficit to make the other person suffer.
Using these data, we can conceptualize in an overly simplified manner that violence and aggression give a squirt of pleasure to the aggressor. This could explain why some people seem to enjoy watching or inflicting acts of aggression. Furthermore, the psychopath may experience the most joy of all.
In summary, the neurobiology of the psychopath may be a constellation of problems: inadequate constraint from the frontal cortex, insufficient fear of consequences, and too much activation of the nucleus accumbens. It could be that psychopathy, like alcoholism or cocaine dependence, is an addiction—although in this case the addiction is to violence. This could explain why psychopathy, like other addictions, is so difficult to treat and does not respond well to traditional interventions.
1. When dealing with a patient with an anger problem and trying to make the right diagnosis, which of the following do you not do?
a. Refuse to treat him because there is no DSM diagnosis for anger.
b. Call it a variation of bipolar disorder.
c. Call it a wastebasket term, such as depression not otherwise specified (NOS) or anxiety NOS.
d. Call it intermittent explosive disorder because it sounds good, even although you know it does not actually apply.
2. Which of the following is not associated with predatory aggression?
a. Activation of the lateral hypothalamus.
b. Stealthy movement.
c. Autonomic arousal.
d. Premeditated.
3. In simple terms, the frontal cortex plays what role with anger?
a. Activates the autonomic neuron system.
b. Applies the brakes on the impulses.
c. Modulates the nucleus accumbens.
d. Activates the lateral hypothalamus.
4. All of the following apply to the amygdala and aggression, except
a. Klüver-Bucy syndrome.
b. Shows less activity with criminal psychopaths.
c. Different nuclei could be activated with different subtypes of aggression.
d. Facilitates the expression of the serotonin receptor.
5. Testosterone
a. Is the primary cause of fighting.
b. Increases plasma levels for the loser.
c. May show a better correlation with social dominance.
d. Stimulates overt hostility in weight lifters.
6. After a fight, the dominant mouse has which of the following?
a. Decreased testosterone and decreased NGF.
b. Decreased testosterone and increased BDNF.
c. Increased testosterone and decreased NGF.
d. Increased testosterone and increased BDNF.
7. All of the following statements about low CSF concentration of the serotonin metabolite 5-HIAA are true, except
a. Common with major depression.
b. Correlates with greater lifetime history of aggression.
c. Predicts relapse for criminal offenders.
d. Associated with greater suicide intent.
8. The psychopath can be conceptualized as having all of the following, except
a. Low resting heart rate.
b. Activated frontal cortex.
c. Hypofunctioning amygdala.
d. Increased activity at the nucleus accumbens.
See Answers section at the end of the book.