25 Shoulder & Arm
Bones of the Upper Limb
Fig. 25.1 Bones of the upper limb
Right limb. The upper limb (membrum superius) is subdivided into three regions: arm (brachium), forearm (antebrachium), and hand (manus). The cingulum pectorale (clavicula and scapula) joins the upper limb to the thorax at the art. sternoclavicularis.
Fig. 25.2 Bones of the cingulum pectorale in normal relation to those of the trunk
Clavicula & Scapula
 The cingulum pectorale (clavicula and scapula) connects the bones of the upper limb to the cavea thoracis. Whereas the cingulum pelvicum (paired ossa coxarum) is firmly integrated into the axial skeleton (see pp. 228–229), the cingulum pectorale is extremely mobile.
The cingulum pectorale (clavicula and scapula) connects the bones of the upper limb to the cavea thoracis. Whereas the cingulum pelvicum (paired ossa coxarum) is firmly integrated into the axial skeleton (see pp. 228–229), the cingulum pectorale is extremely mobile.
Fig. 25.3 Clavicula
Right clavicula. The S-shaped clavicula is visible and palpable along its entire length (generally 12 to 15 cm). Its medial end articulates with the sternum at the art. sternoclavicularis (see p. 299). Its lateral end articulates with the scapula at the art. acromioclavicularis (see p. 299).
 Clinical box 25.1
Clinical box 25.1
Foramen scapulae
The lig. transversum scapulae superius (see Fig. 25.13, p. 301) may become ossified, transforming the incisura scapulae into an anomalous bony canal, the foramen scapulae. This can lead to compression of the n. suprascapularis as it passes through the canal (see p. 377).
Fig. 25.4 Scapula
Right scapula. In its normal anatomical position, the scapula extends from costa II to costa VII.
Humerus
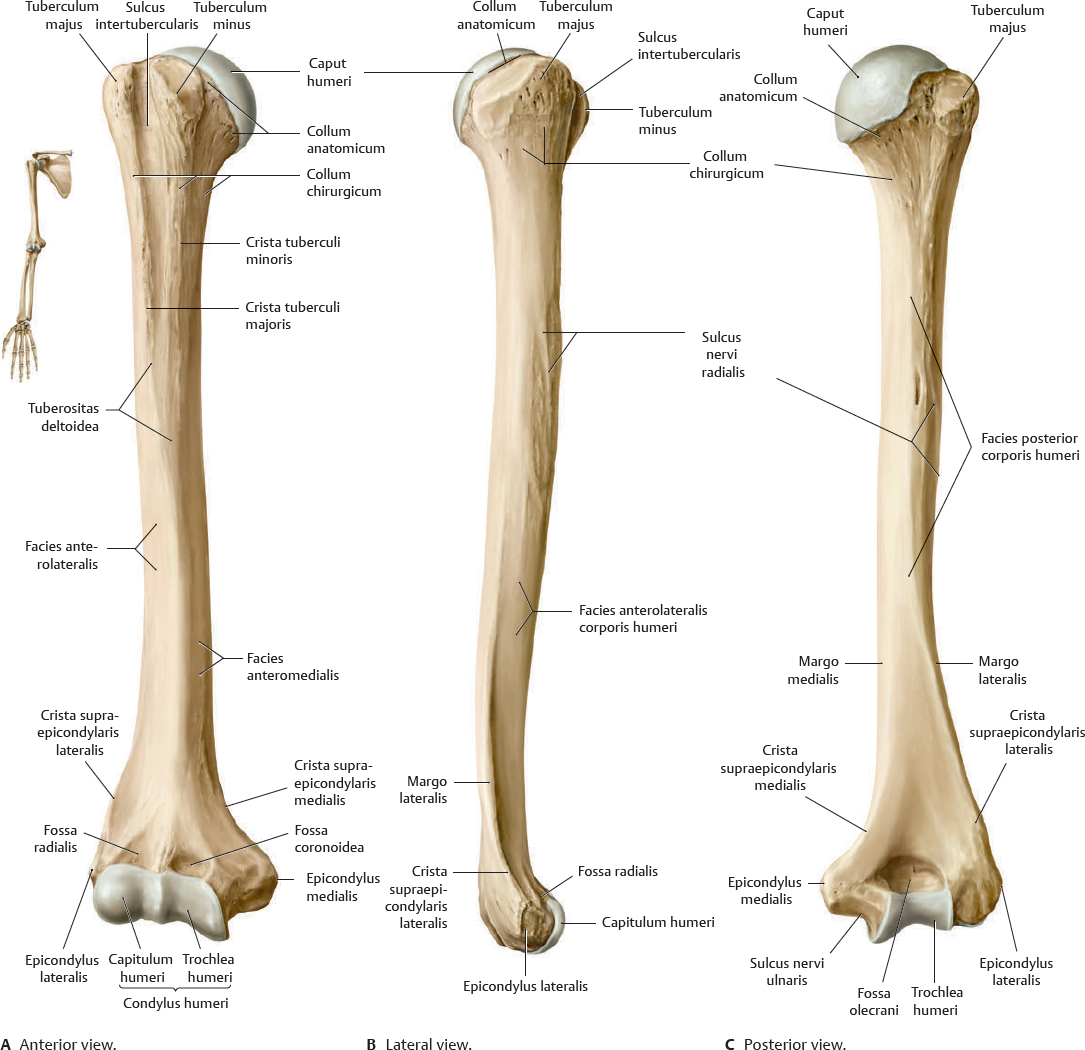
Fig. 25.5 Humerus
Right humerus. The caput humeri articulates with the scapula at the art. humeri (see p. 300). The capitulum and trochlea of the humerus articulate with the radius and ulna, respectively, at the art. cubiti (see p. 322).
Clinical box 25.2
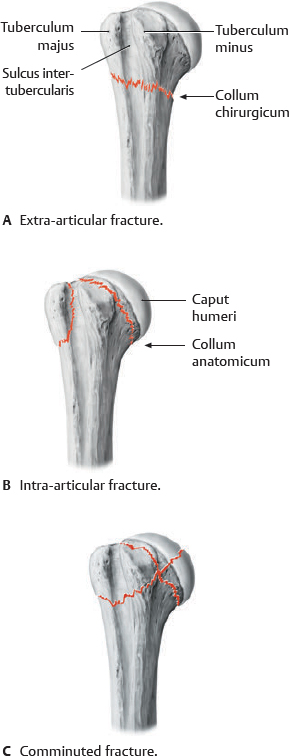
Fractures of the humerus
Anterior view. Fractures of the proximal humerus are very common and occur predominantly in older patients who sustain a fall onto the outstretched arm or directly onto the shoulder. Three main types are distinguished.
Extra-articular fractures and intra-articular fractures are often accompanied by injuries of the blood vessels that supply the caput humeri (aa. circumflexae humeri anterior and posterior), with an associated risk of post-traumatic avascular necrosis.
Fractures of the corpus humeri and distal humerus are frequently associated with damage to the n. radialis.
Joints of the Shoulder
Fig. 25.6 Joints of the shoulder: Overview
Right shoulder, anterior view.
Fig. 25.7 Joints of the cingulum pectorale
Right side, superior view.
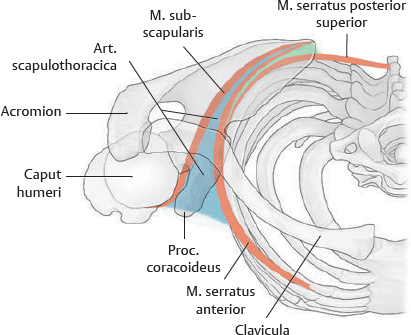
Fig. 25.8 Articulatio scapulothoracica
Right side, superior view. In all movements of the shoulder girdle, the scapula glides on a curved surface of loose connective tissue between the mm. serratus anterior and subscapularis. This surface can be considered a scapulothoracic joint.
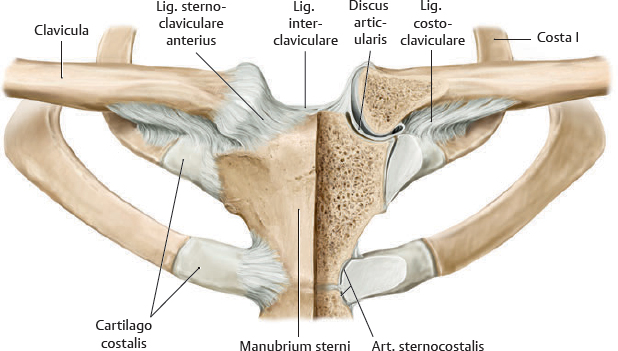
Fig. 25.9 Articulatio sternoclavicularis
Anterior view with sternum coronally sectioned (left). Note: A fibrocartilaginous discus articularis compensates for the mismatch of surfaces between the two saddle-shaped articular facets of the clavicula and the manubrium sterni.
Fig. 25.10 Articulatio acromioclavicularis
Anterior view. The art. acromioclavicularis is a plane joint. Because the articulating surfaces are flat, they must be held in place by strong ligaments, greatly limiting the mobility of the joint.
Clinical box 25.3
Injuries of the articulatio acromioclavicularis
A fall onto the outstretched arm or shoulder frequently causes dislocation of the art. acromioclavicularis and damage to the ligg. coracoclavicularia.
Joints of the Shoulder: Articulatio Humeri
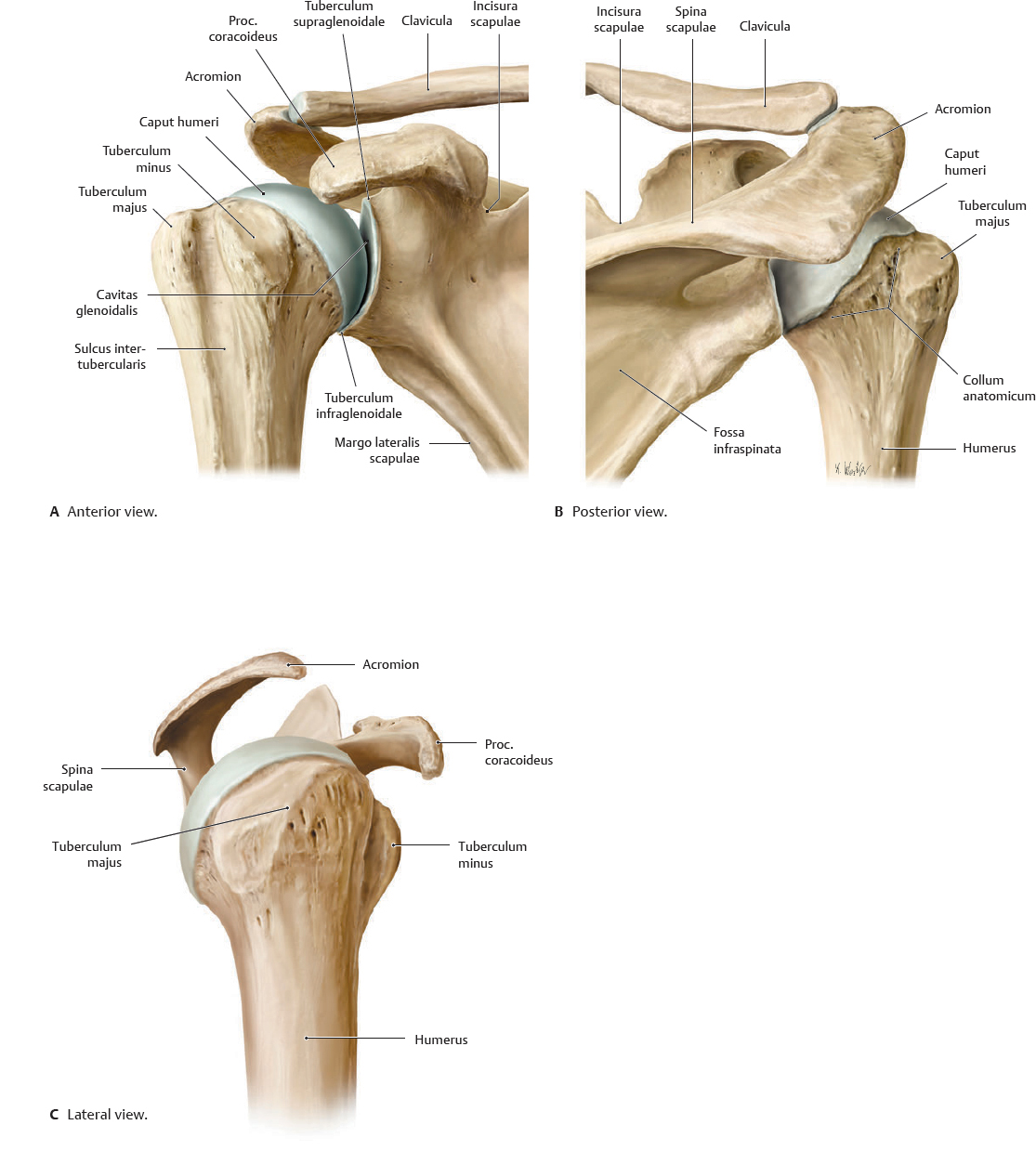
Fig. 25.11 Articulatio humeri: Bony elements
Right shoulder.
Fig. 25.12 Articulatio humeri cavity
Fig. 25.13 Articulatio humeri: Capsula articularis and ligaments
Right shoulder.
Fig. 25.14 Ligaments reinforcing capsula
Schematic representation of the ligaments reinforcing the capsula articularis after removal of the caput humeri. Right shoulder.
Subacromial Space & Bursae
Fig. 25.15 Subacromial space
Right shoulder.
Fig. 25.16 Bursa subacromialis and cavitas glenoidalis
Right shoulder, lateral view of sagittal section with humerus removed.
Fig. 25.17 Bursae subacromialis and subdeltoidea
Right shoulder, anterior view.
Anterior Muscles of the Shoulder & Arm (I)
Fig. 25.18 Anterior muscles of the shoulder and arm
Right side, anterior view. Muscle origins are shown in red, insertions in blue.
Anterior Muscles of the Shoulder & Arm (II)
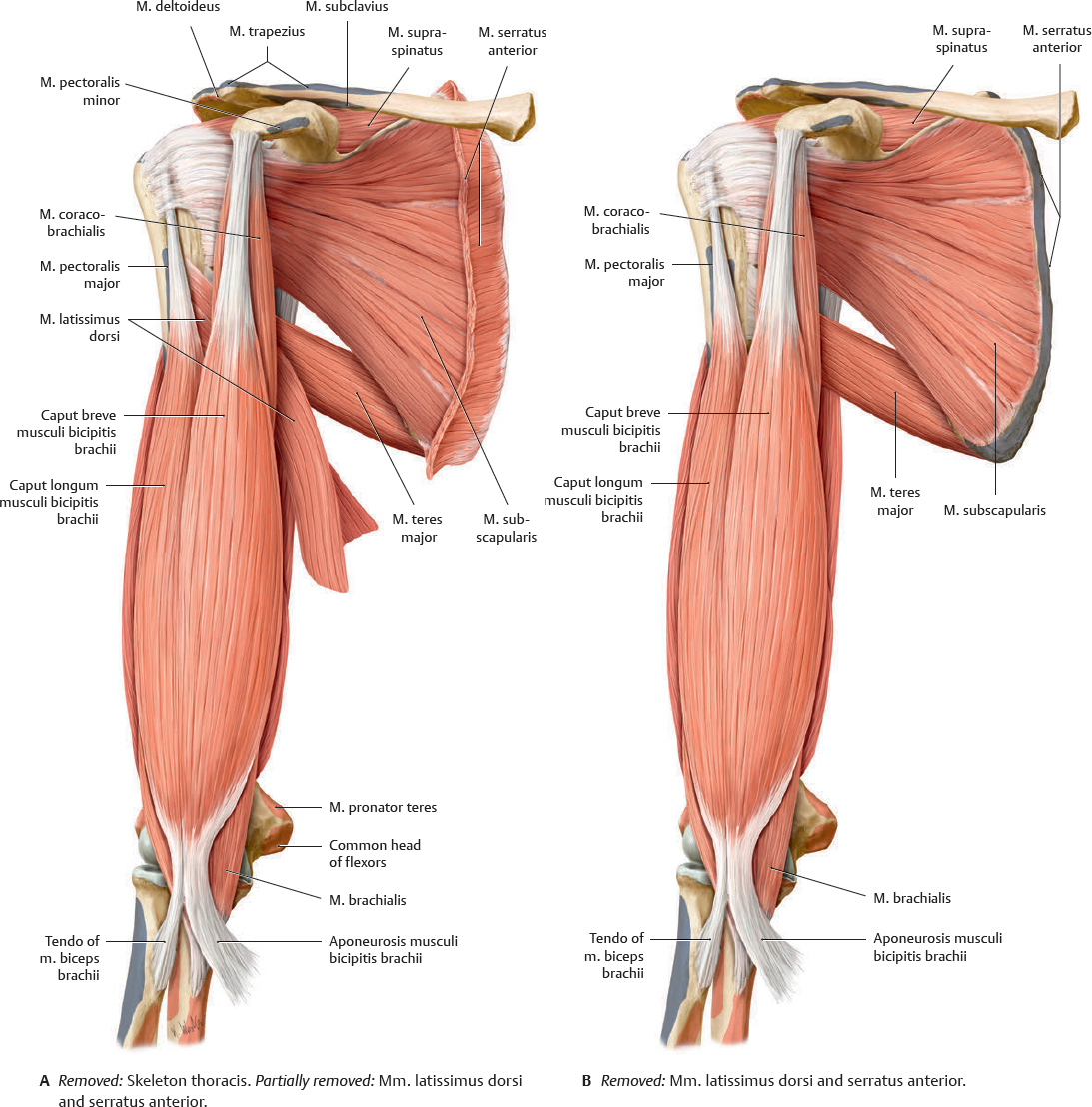
Fig. 25.19 Anterior muscles of the shoulder and arm: Dissection
Right arm, anterior view. Muscle origins are shown in red, insertions in blue.
Posterior Muscles of the Shoulder & Arm (I)
Fig. 25.20 Posterior muscles of the shoulder and arm
Right side, posterior view.
Posterior Muscles of the Shoulder & Arm (II)
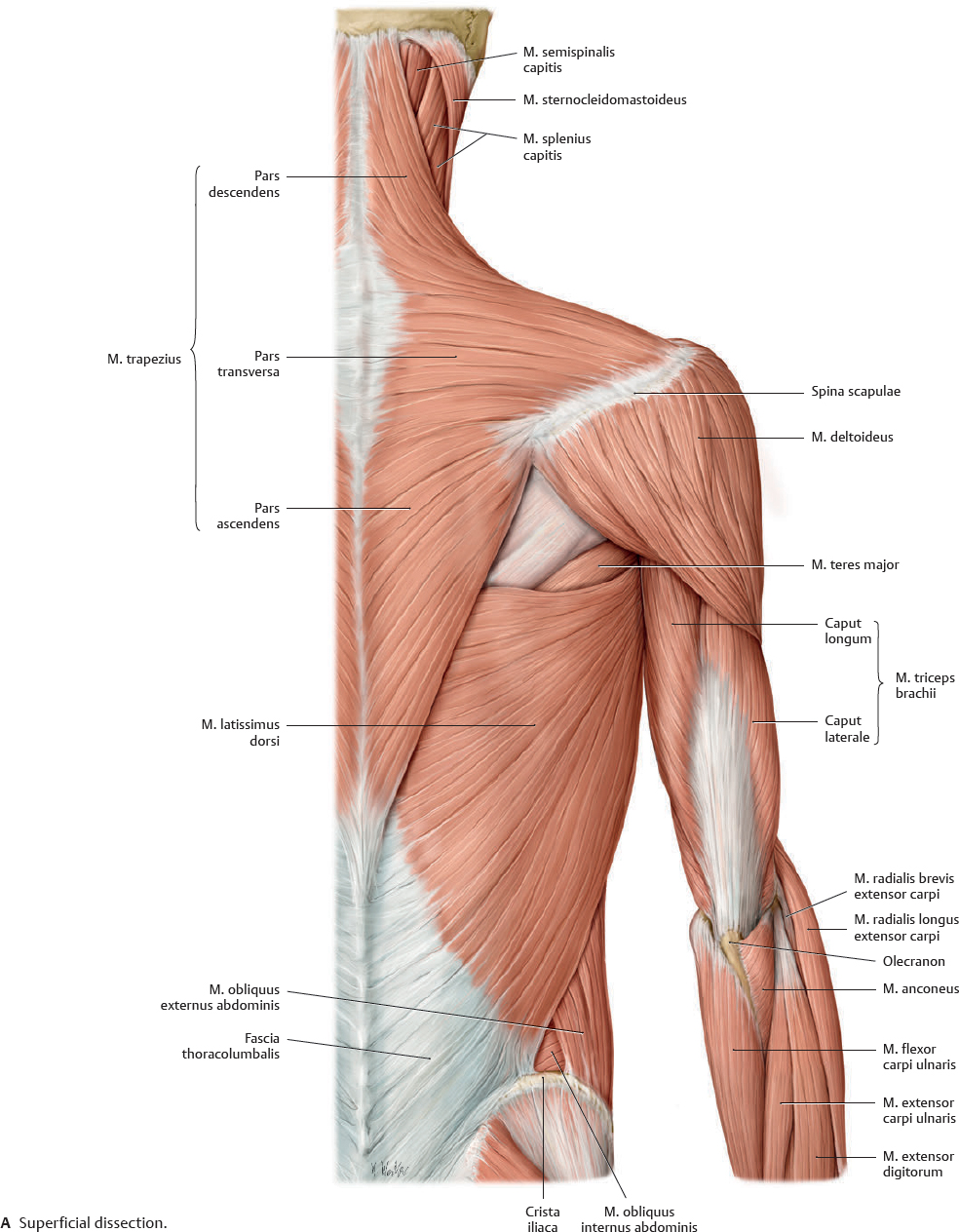
Fig. 25.21 Posterior muscles of the shoulder and arm: Dissection
Right arm, posterior view. Muscle origins are shown in red, insertions in blue.
Muscle Facts (I)
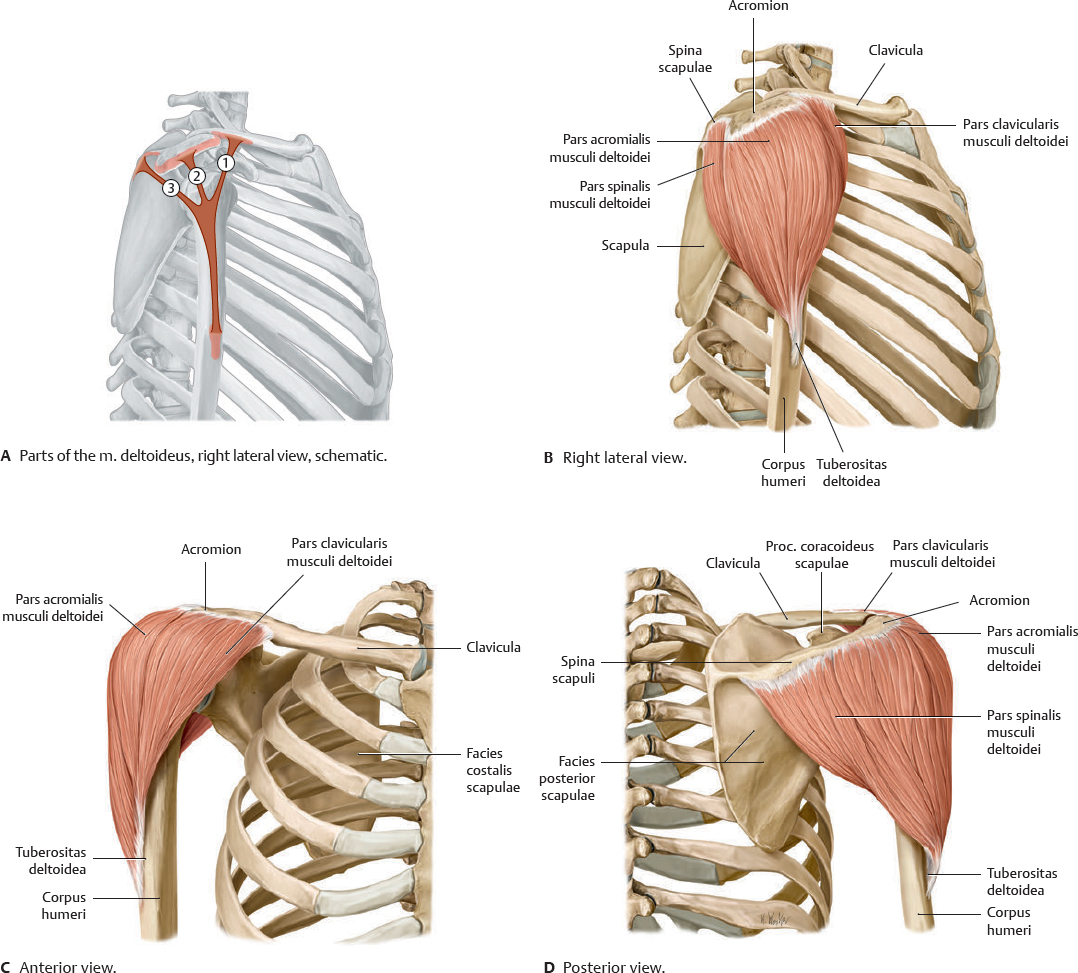
The actions of the three parts of the m. deltoideus depend on their relationship to the position of the humerus and its axis of motion. At less than 60 degrees, the muscles act as adductors, but at greater than 60 degrees, they act as abductors. As a result, the parts of the m. deltoideus can act antagonistically as well as synergistically.
Fig. 25.22 Musculus deltoideus
Right shoulder.
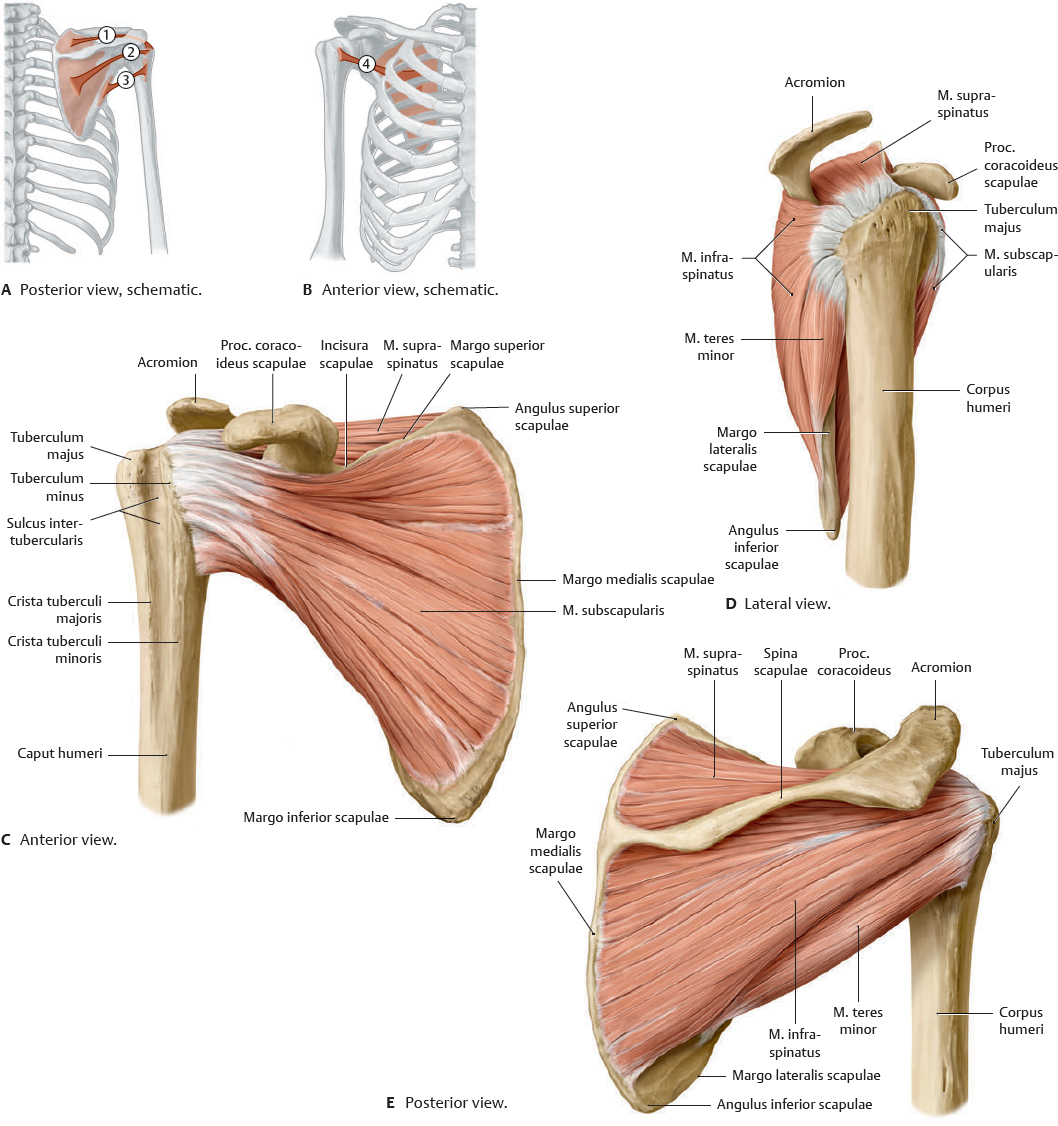
Fig. 25.23 Rotator cuff
Right shoulder. The rotator cuff consists of four muscles: mm. supraspinatus, infraspinatus, teres minor, and subscapularis.
Muscle Facts (II)
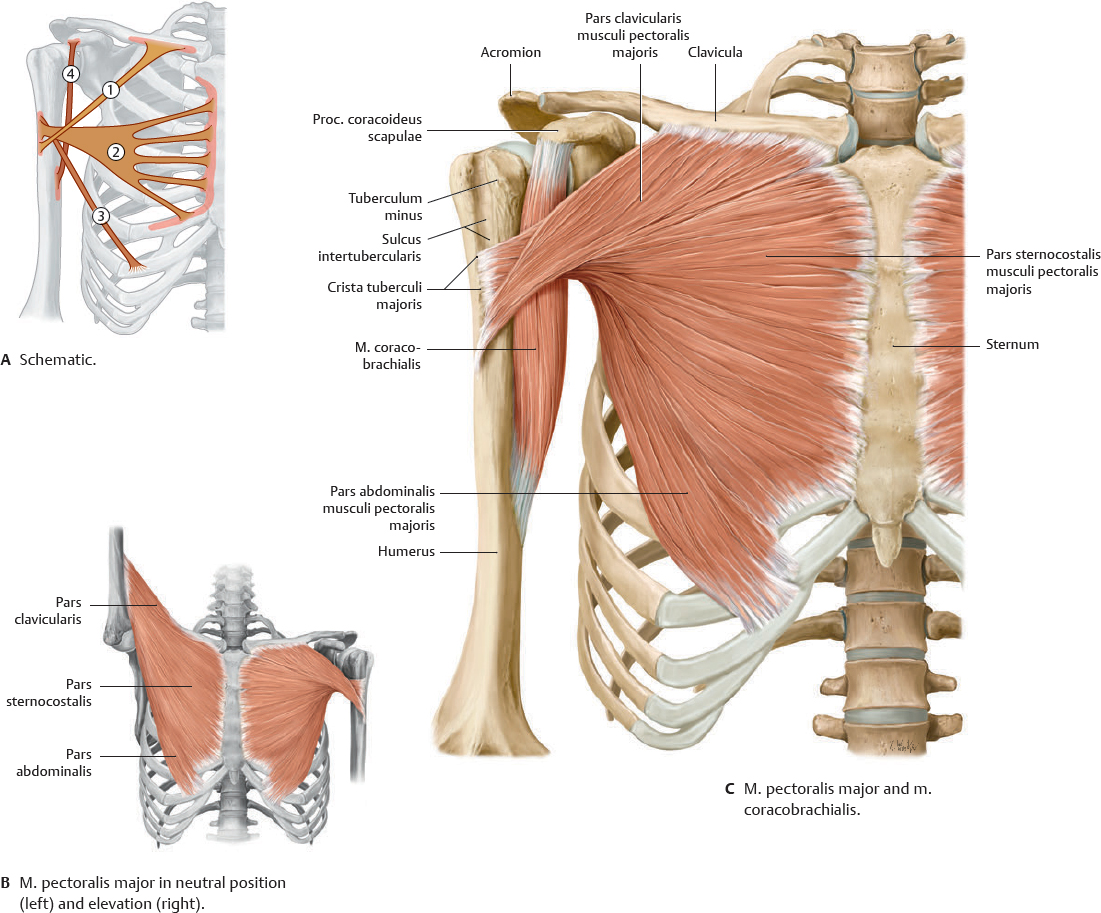
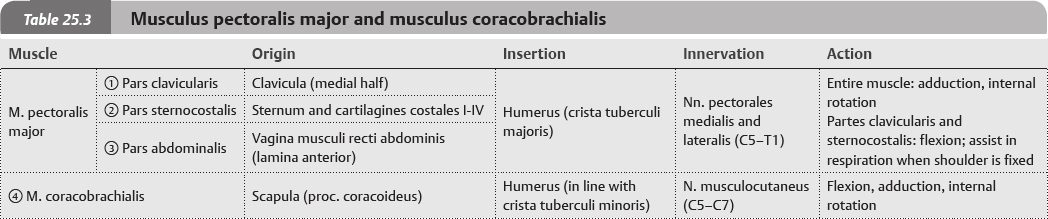
Fig. 25.24 Musculus pectoralis major and musculus coracobrachialis
Anterior view.
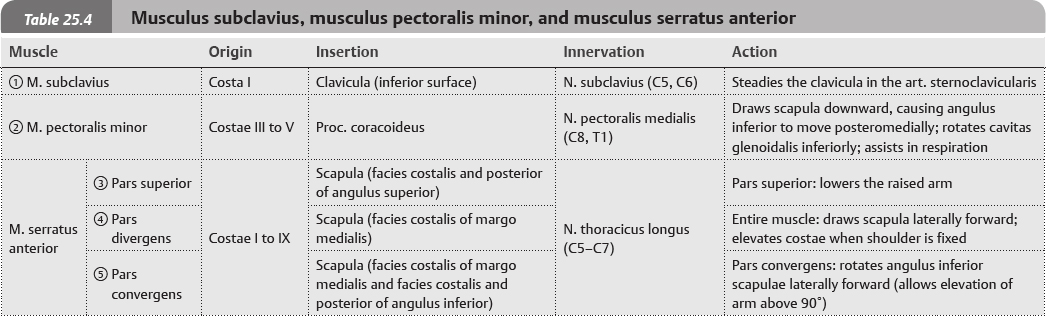
Fig. 25.25 Musculus subclavius and musculus pectoralis minor
Right side, anterior view.
Fig. 25.26 Musculus serratus anterior
Right lateral view.
Muscle Facts (III)
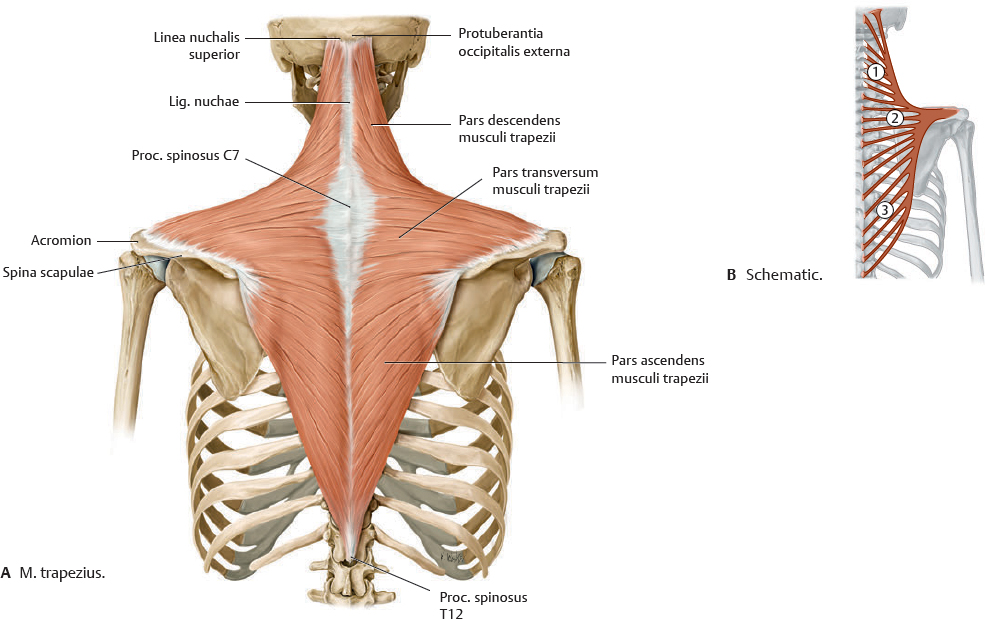
Fig. 25.27 Musculus trapezius
Posterior view.
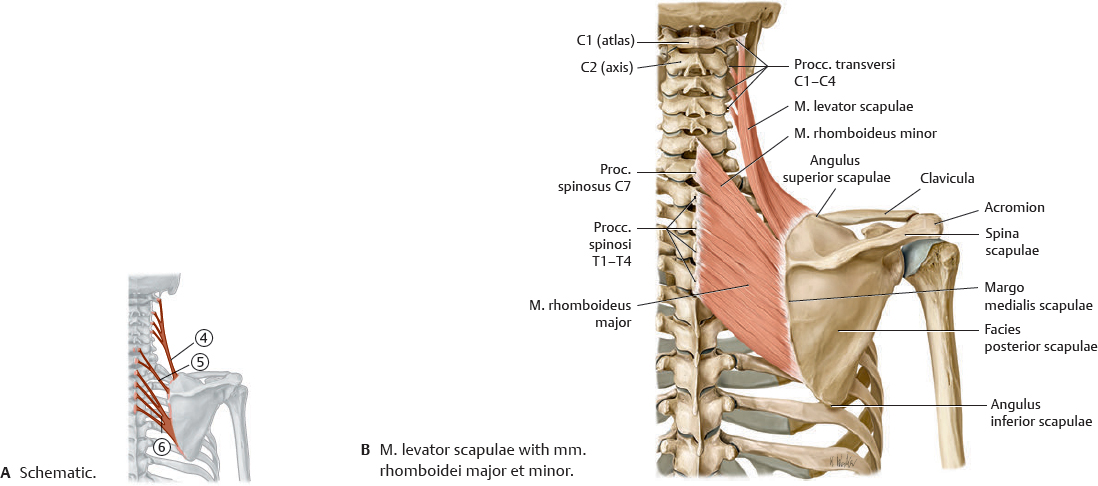
Fig. 25.28 Musculus levator scapulae with musculi rhomboidei major et minor
Right side, posterior view.
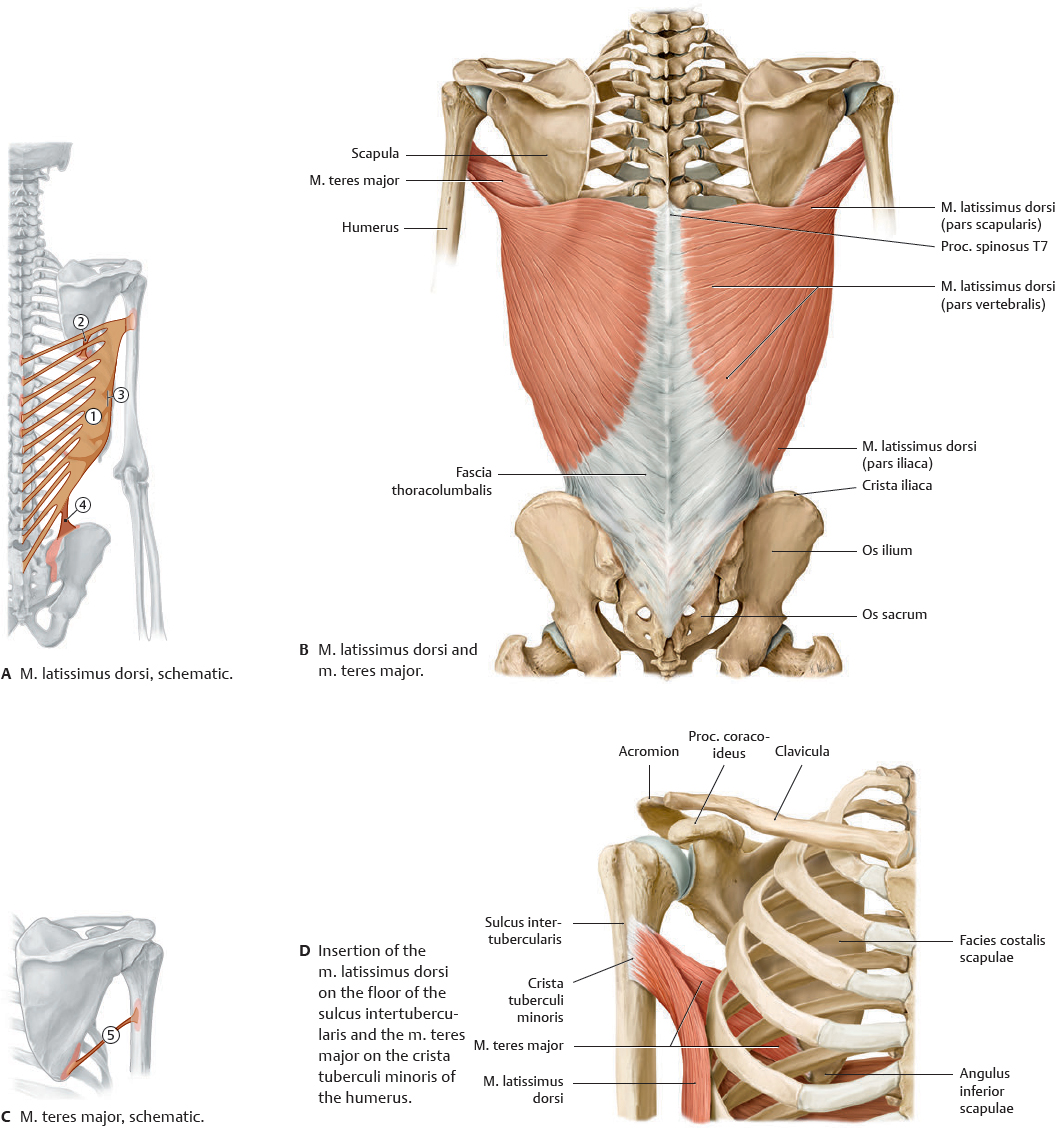
Fig. 25.29 Musculus latissimus dorsi and musculus teres major
Posterior view.
Muscle Facts (IV)
The anterior and posterior muscles of the arm may be classified respectively as flexors and extensors relative to the movement of the art. cubiti. Although the m. coracobrachialis is topographically part of the anterior compartment, it is functionally grouped with the muscles of the shoulder (see p. 314).
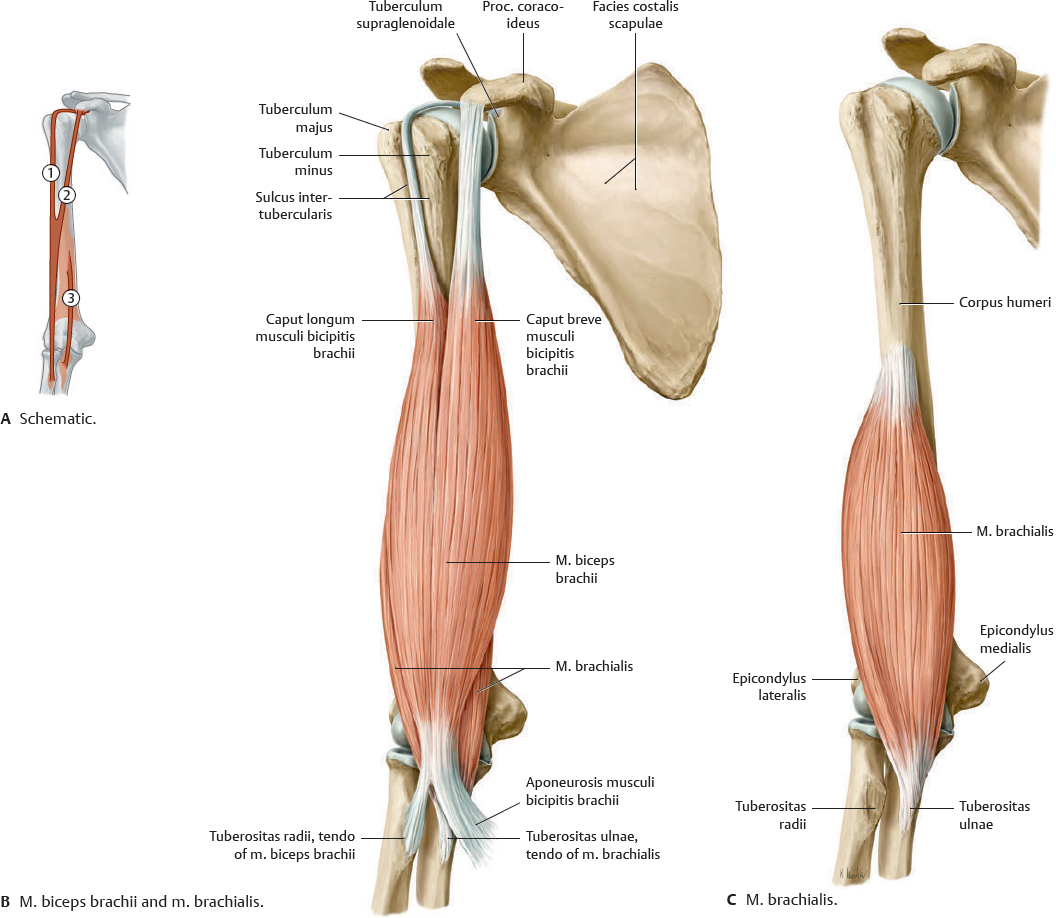
Fig. 25.30 Musculus biceps brachii and musculus brachialis
Right arm, anterior view.
Fig. 25.31 Musculus triceps brachii and musculus anconeus
Right arm, posterior view.