We examined the specifics of the ventricular rhythms, and especially the VTachs, in Section 5, Ventricular Rhythms, of this text. As a whole, the VTachs are among the most life-threatening arrhythmias you will ever encounter in your clinical practice. They include monomorphic VTach, polymorphic VTach, bidirectional VTach, and torsade de pointes. It is important that you understand the principles and concepts presented in those chapters. If you need a quick review, now is the time to go back and review them again.
VTachs are defined as three or more consecutive ventricular complexes occurring at a rate of 100 beats per minute (BPM) or greater. VTachs can be either nonsustained (short bursts or salvos lasting less than 30 seconds) or sustained (lasting 30 seconds or more). Sustained VTachs are almost always hemodynamically unstable and will typically require some sort of intervention in order to terminate the rhythm.
As we mentioned earlier, when approaching a WCT, we need to focus primarily on identifying the presence of a VTach, and not on whether it is an SVT-A. The prime clinical reason for this is that VTachs, even if stable at the time, tend to decompensate rather quickly. We cannot afford to take the possibility that the strip is a misdiagnosed VTach too lightly; aggressive reevaluation of the patient and the strips is of paramount importance to achieving a successful clinical outcome. Never be so convinced of your diagnosis that you forget to continually reassess the patient. That type of hubris will cause you to miss some changes that pop up from time to time, signaling a rhythm change into a VTach. Remember, strips and ECGs are just short “video clips” of a much longer movie that can have a surprise ending.
History and Physical Examination
The history is always an extremely important component in evaluating any clinical case. Arrhythmia recognition is no exception to this rule. Many times, historical information will make the diagnosis for you. A prior history of an arrhythmia can guide you toward a better strategy for the acute or long-term management of the patient. In any case, remember to always try to get a history and a physical exam if your patient is stable and can tolerate a few minutes’ delay prior to treatment.
There are certain factors in the history and physical that point us in the direction of VTach. These include the following:
Presence of structural or ischemic heart disease or myocardial infarction (MI)
Prior history of cardiac arrhythmia
Patient age greater than 35 years
Family history of sudden cardiac death
Presence of a cardiomyopathy
Presence of congestive heart failure
Let’s take a look at these factors individually.
1. Presence of structural or ischemic heart disease or MI
As discussed in Chapter 35, Wide-Complex Tachycardia: The Approach, approximately 80% of all WCTs are VTachs.1-5 That leaves 20% for all the other causes combined. If the patient has a history of structural heart disease or has a history of either coronary artery disease or MI, the probability of the WCT being a VTach is over 90%.1-4 The increased chance of VTach is caused by two mechanisms that are both exacerbated by myocardial ischemia, injury, or infarct: (1) increased myocardial irritability and (2) the formation of micro- or macro-reentry loops.
As you can imagine, areas of ischemia cause a heightened state of irritability in myocardial tissue and cells. This is analogous to a cellular fight-or-flight syndrome where the cells enter a survival mode. Tens to hundreds of cellular pathways and channels have to accommodate for the lack of perfusion with oxygen and sugars that fuel the normal state of operation of each cell. Leaky membranes lead to increased automaticity at these potential ectopic ventricular foci until one of them begins to fire independently of the others. Thus, a tachyarrhythmia is born.
In Chapter 25, AV Nodal Reentry Tachycardia, we went into some detail on how reentry loops are created. Reentry circuits typically form around isolated islands of ischemic tissue (see the Additional Information box on the Relative Refractory Period found on page 126 in Chapter 8, Normal Sinus Rhythm) or around nonconductive myocardial structural defects, such as scars or infarcted areas. In addition to the mechanical obstructions created by the nonconductive scars, any other causative metabolic, physiologic, or pharmacologic processes that slow conduction in the tracts around the defect can create an area of decreased conduction, thus setting up the various components needed to create a self-propagating reentry loop.
We want you to take special note of the fact that scarring or infarct is a setup for the development of reentry loops because it forms the “track” used by the reentry circuit. Depending on the size of the scar, the circuits created can be found as either micro- or macro-reentry circuits.
2. Prior History of Cardiac Arrhythmia
If you have the time, you should always try to obtain any relevant direct or indirect history of prior arrhythmias from your patient. Direct history includes any previous diagnoses of prior arrhythmias or clinical syndromes that could lead to arrhythmias. Indirect history refers to the presence of presyncope, syncope, palpitations, light-headedness, or any hemodynamic compromise. Many times, the pattern and presentation of these indirect symptoms may lead you in the direction of certain arrhythmias.
A prior history of the presence of an accessory pathway or Wolff-Parkinson-White syndrome is very clinically relevant. This knowledge will certainly focus your thinking toward AVRT, either orthodromic or antidromic, or toward decompensated atrial flutter or fibrillation. This knowledge will also be extremely valuable in your decision regarding which pharmaceutical agents you could safely use on the patient. Accessory pathways favor SVTs as the cause of a WCT.
A prior history of VTach, either sustained or nonsustained, will lead you in the direction of a possible recurrence. In the same way, a history of multiple premature ventricular contractions (PVCs), couplets, or triplets will also steer you in the direction of a possible VTach rather than an SVT.
CLINICALPEARL
Ask your patient to tap out the cadence of their palpitations. Many times, patients will tap out an irregular rhythm that will be a great aid in narrowing the possibilities in your differential diagnosis.
3. Patient Age Greater Than 35 Years
As you get older, your risk of developing isolated areas of scarring or ischemia from any number of sources increases.
4. Family History of Sudden Cardiac Death
Family history of sudden cardiac death should make you immediately think about the possibility of a genetic defect being expressed by your patient.
INTERMEDIATE
Examples include long QT syndrome (LQTS), short QT syndrome (SQTS), Romano-Ward syndrome, and Brugada syndrome, to name a few. Cardiac malformations are also found in many genetic disorders, for example Down syndrome. In addition, certain genetic disorders are found more commonly in certain geographic locations around the globe.
5. Presence of a Cardiomyopathy
Cardiomyopathies of all types frequently lead to arrhythmia formation, including VTach. The anatomic abnormalities that are found in cardiomyopathies encompass a vast spectrum of anatomic presentations. These include the dilated cardiomyopathies with their large baggy hearts with multichamber enlargement and the hypertrophic cardiomyopathies that have thick focal areas of muscular hypertrophy. Structural heart abnormalities are also common in those with cardiomyopathy. In addition, the abnormally long, circuitous, atypical paths that the depolarization waves have to take create ample opportunity for the formation of reentry circuits.
6. Presence of Congestive Heart Failure
Congestive heart failure frequently leads to arrhythmia formation due to various reasons. Episodes of ischemia and infarcts frequently occur in patients with congestive heart failure as the fluid buildup in the lungs, pleural space, and abdominal cavity can lead to serious hypoxemia. Decreased pump function as well as atrial and ventricular chamber enlargement are also frequently found in these patients and are associated with arrhythmia formation. In addition, as we saw earlier, congestive heart failure can be a cause or a precursor to a dilated cardiomyopathy.
QRS Interval Width
VTach, by definition, starts from a ventricular pacemaker in the ventricular myocardium. The inciting focus, as we shall see later in this section, can be due to either a single pacing cell or to a micro- or macro-reentry loop. In general, the pacing focus fires and creates a depolarization wave(s) that radiates outward using direct cell-to-cell conduction. This slowly expanding depolarization wave produces a wide QRS interval in its wake.
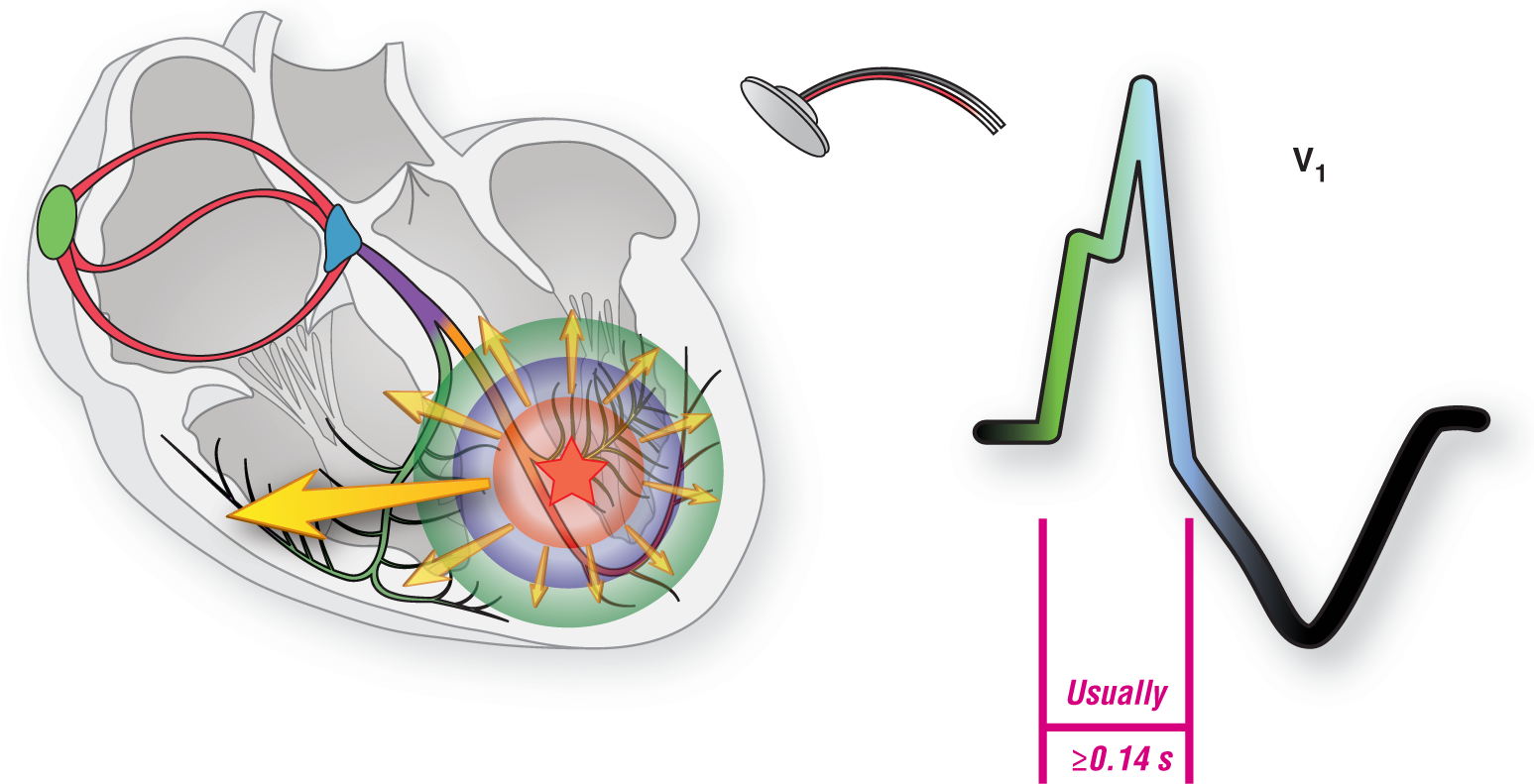
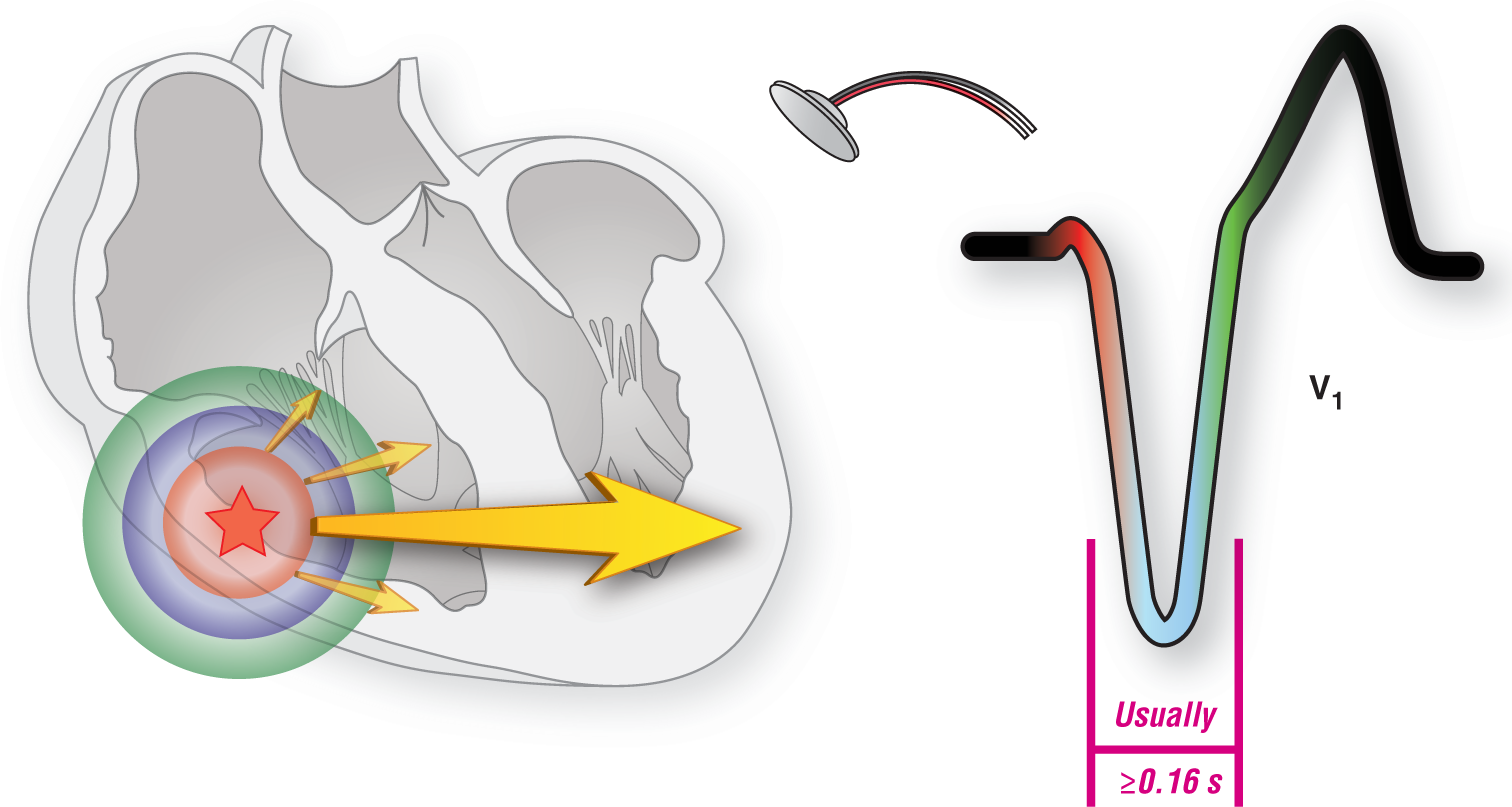
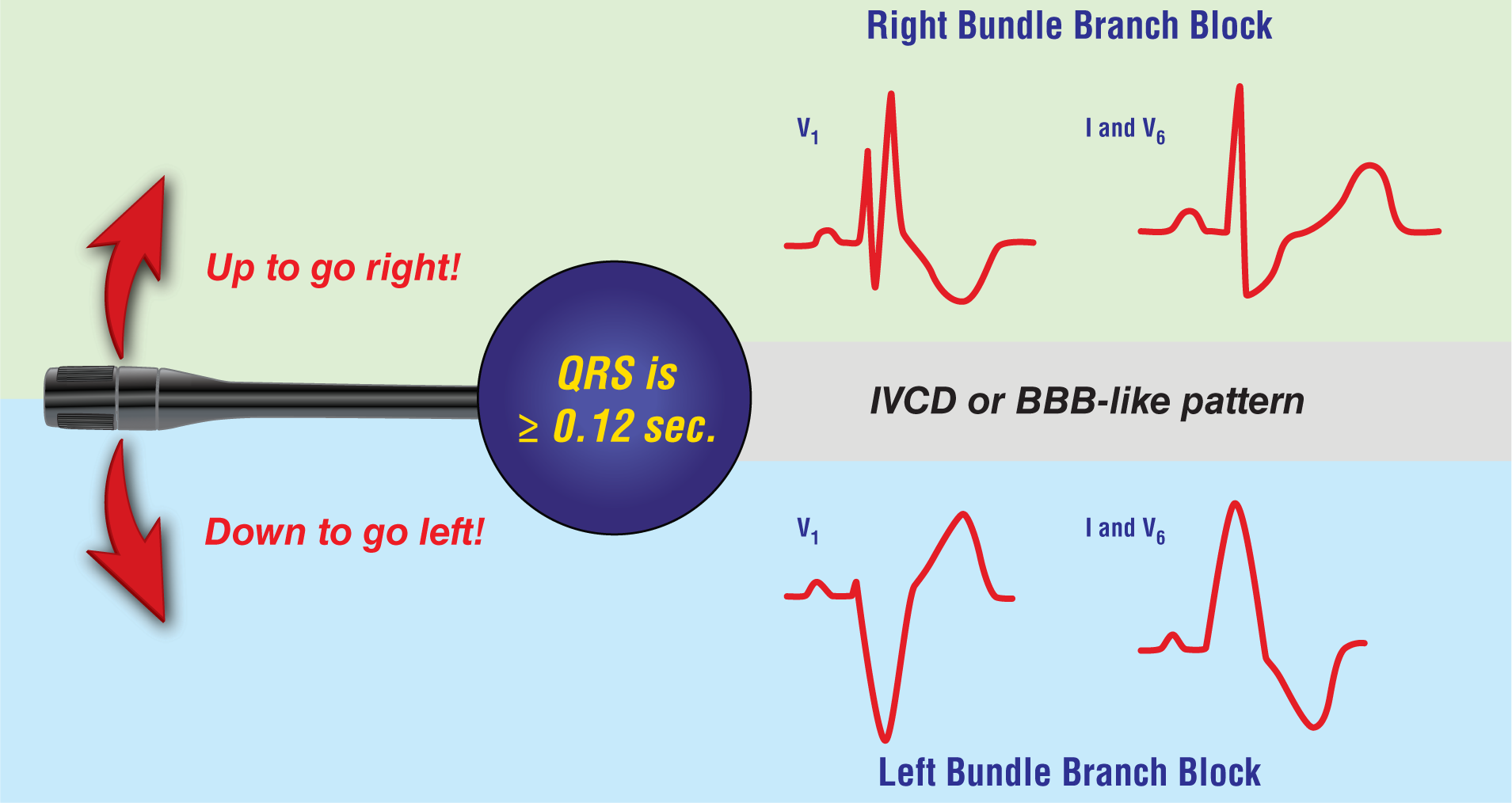
As a general rule, QRS intervals greater than or equal to 0.14 seconds (3½ small blocks) are more prone to occur in VTach. Right bundle branch block (RBBB)-like patterns typically are positive in lead V1 and have a QRS duration greater than or equal to 0.14 seconds (Figure 36-1). Left bundle branch blocks (LBBBs) and LBBB-like patterns typically are negative in lead V1 and have a QRS interval of greater than or equal to 0.16 seconds (Figure 36-2). The broader the QRS complex, the higher the chance that it is a VTach.
Figure 36-1 In an RBBB-like VTach, the ventricular pacer that starts the depolarization wave is typically found in the left ventricle or the left side of the septum. This leads to the formation of a depolarization vector that mostly travels to the right in an unopposed manner. Since a vector heading toward an electrode forms a positive deflection, this unopposed vector creates the appearance of an RBBB-like pattern with a positive complex in lead V1.
Figure 36-2 In an LBBB-like VTach, the ventricular pacer that starts the depolarization wave is typically found in the right ventricle or the right side of the septum. This leads to the formation of a depolarization vector that mostly travels to the left in an unopposed manner. This vector creates the appearance of an LBBB-like pattern with a negative complex in lead V1.
Keep in mind, however, that if the QRS complex is extremely wide and bizarre, you should always rule out other causative factors, including hyperkalemia, drugs (overdoses and adverse effects), and pacers, to name a few.
Regularity
Wide complex tachycardias can be either regular or irregular. The regular WCTs include monomorphic VTach (Figure 36-3) and the regular SVTs-A. However, slight variations in regularity are common and occur haphazardly at various spots on the strips but especially during the onset of the rhythm (the warm-up period) and at termination. Causes of the irregularities will be discussed further during the first part of the QRS morphology section coming up next.
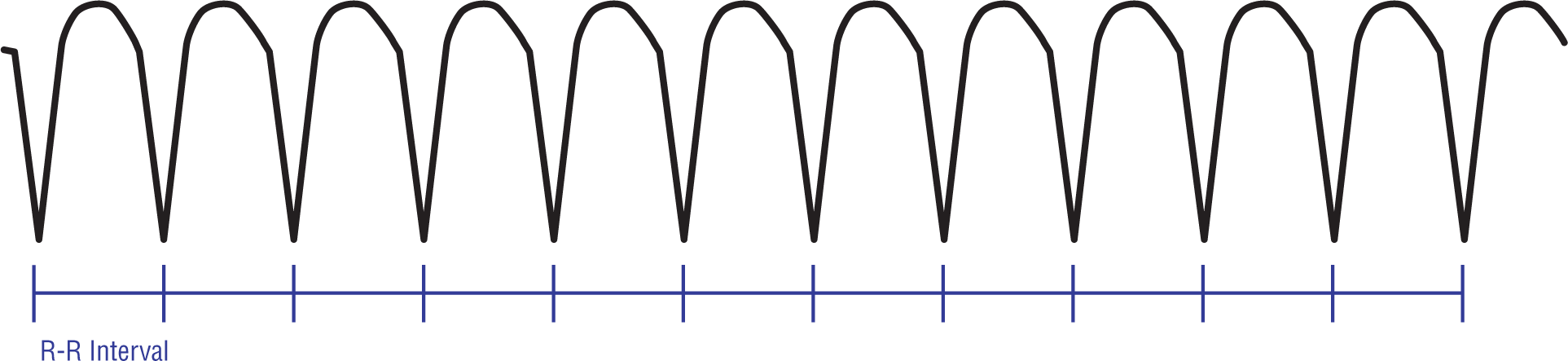
Figure 36-3 Ventricular tachycardia is very regular.
The irregular rhythms include polymorphic VTach, torsade de pointes, and the irregular wide-complex SVTs-A. However, if the rhythm is consistently irregularly irregular throughout the strip, then an uncontrolled rapid atrial fibrillation with aberrancy is the most likely candidate.
As a general rule, regularity and irregularity should not be used to rule in or rule out a VTach.
QRS Morphology
VTachs typically vary slightly in morphology and regularity at isolated spots throughout the strip.5-6 Slight variations can occur at any time due to factors like very rapid rates, respiratory variations in intrathoracic pressure, AV dissociation, and minor fluctuations in the routes taken by the depolarization waves conducted by direct cell-to-cell contact. These changes are more frequently seen during the onset (warm-up period) and termination of the arrhythmia.
The morphology and timing can also be altered by the presence of AV dissociation. AV dissociations are associated with buried P waves, capture beats, and fusion beats, any of which can cause partial resets of the pacemaker rhythm or variations in the route taken by the depolarization and repolarization waves.
The first complex of a salvo or run of VTach could be triggered by a PVC originating from either the same irritable focus that triggers off the VTach or from a separate focus with differing morphology and axis. PVCs originating in ectopic pacemakers are a frequent cause of reentry-related VTach. In these cases, the morphology of the VTach will be unstable for the first few beats and then they will eventually settle down into a more stable monomorphic pattern consistent with a single very rapid pacemaker. This period at the onset of the salvo is typically referred to as the “warm-up” period.
The morphologic appearance of a salvo of VTach may also be complicated by the presence of an R-on-T phenomenon. This phenomenon occurs when a PVC arrives during the relative refractory period of the previous complex’s ventricular repolarization period. An R-on-T phenomenon is considered an ominous finding and a harbinger of an impending VTach. R-on-T phenomena require an immediate shift in your approach to the patient; they trigger the need to provide additional levels of observation and care for these patients.
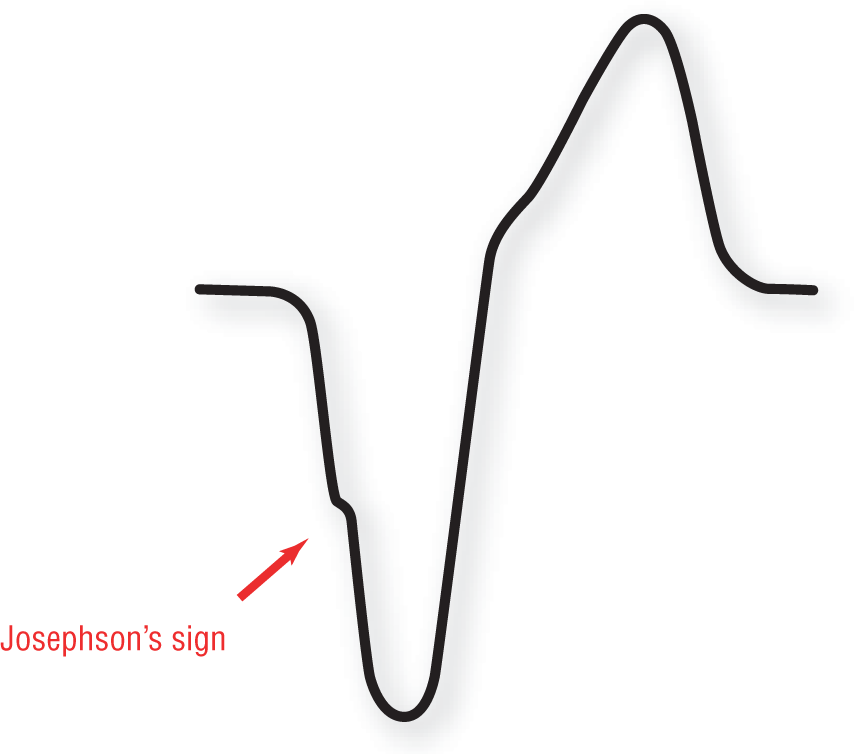
In leads where the QRS complexes are negative or have dominant S waves, there are two signs that favor VTach as the diagnosis: Josephson’s sign and Brugada’s sign.
Josephson’s Sign
Josephson’s sign refers to the presence of a notch in the downstroke of the S wave present in many complexes of ventricular origin (Figure 36-4). The presence of the notch is very useful in distinguishing a ventricular complex from an aberrantly conducted supraventricular complex or a complex with an underlying LBBB or RBBB.
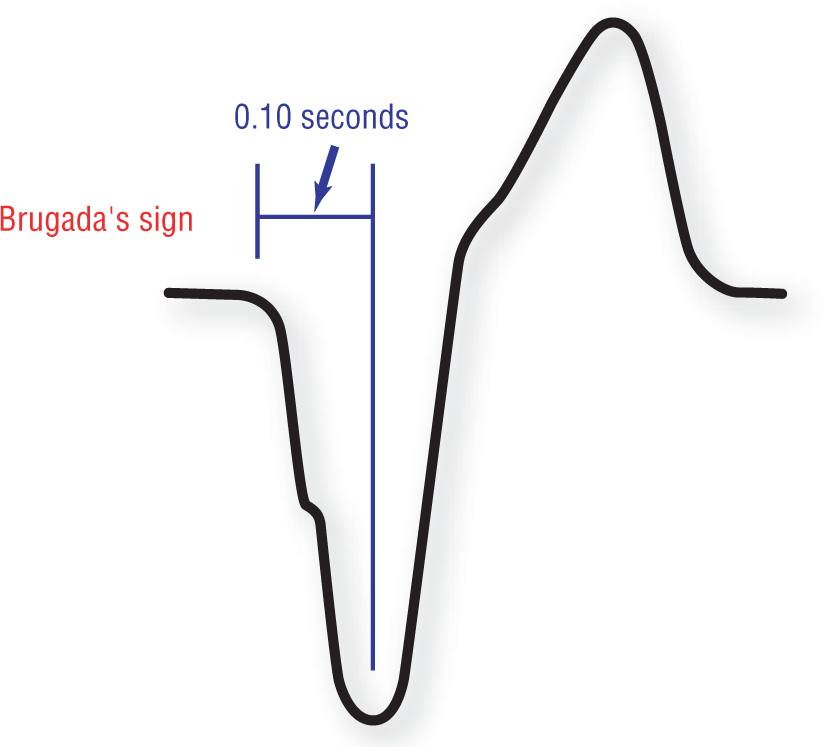
Brugada’s sign refers to a distance of at least 0.10 seconds (100 milliseconds, or 2½ small blocks) from the onset of the QRS complex to the nadir of the S wave that is present in many complexes of ventricular origin (Figure 36-5). The presence of this distance interval is a very useful sign in distinguishing a ventricular complex from an aberrantly conducted supraventricular complex or a complex with an underlying LBBB or RBBB.
Throughout our years of teaching arrhythmia recognition to students of all levels, we have noted an underlying trend toward confusion when discussing this topic. The confusion exists due to a failure in the literature of using an established, universally accepted nomenclature to describe the findings and also to the various authors’ nebulous focus on the leads in question.
Let’s start off by saying that strict morphologic criteria have been established in order to identify the LBBB and RBBB patterns in electrocardiography. A couple of the established criteria include the width of the QRS complex being greater than or equal to 0.12 seconds and the direction of the QRS complex in lead V1. There are, however, other criteria that we have covered multiple times already in this text. The main source of the confusion arises when the label RBBB or LBBB is assigned to a ventricular complex. The morphology of these complexes is not a true BBB pattern since the complexes originate in the ventricles and their main source of conduction was not through the normal electrical conduction pathway until a block was reached. More on this later.
Keep in mind, the ECG criteria for the BBBs were created assuming that the patient is in sinus rhythm and not in an arrhythmia. This is especially true in arrhythmias that are not conducted entirely through the normal electrical conduction system. Once the depolarization wave begins in an ectopic focus or leaves the conduction system and aberrancy takes over, our ability to correctly predict the paths taken by the depolarization wave vanishes. The other thing that disappears is the validity of the established criteria.
There is an exception to this criteria problem: If the patient has a preexisting BBB, that BBB would remain constant in a tachycardia unless another complication is occurring simultaneously. For example, take a patient with a preexisting RBBB. If that patient were to develop a tachycardia at 140 BPM, he would have a wide-complex SVT due to a preexisting BBB.
In discussing the VTachs, authors have erroneously referred to the presentations by the same term they use for a preexisting BBB. Negative complexes in V1 are typically erroneously referred to as having an LBBB pattern, LBBB appearance, or LBBB morphology. In reality, VTachs cannot have true LBBB or true RBBB patterns because they are of ventricular origin and are not true BBBs. The established ECG criteria do not apply here. Instead, until a more detailed nomenclature has been established, we should refer to the QRS morphology in VTach as having either an LBBB-like or an RBBB-like morphology. Therefore, only the BBB-like changes we will be discussing in this section are strictly limited to leads V1-2 and V6 as they appear in a VTach, unless otherwise stated.
Here’s a general rule for beginners that works as a starting point with both BBB and BBB-like patterns: If the wide QRS complexes are positive in lead V1, then you are dealing with an RBBB or RBBB-like pattern; if the wide QRS complexes are negative in lead V1, then you are dealing with an LBBB or LBBB-like pattern (Figure 36-6).
Figure 36-6 How do you use a turn signal? To go left, you move the lever down. To turn right, you move the lever up. Keeping this in mind, which way does the main QRS amplitude point in an RBBB or an RBBB-like pattern? Answer: Up. Which way does it point in an LBBB or LBBB-like pattern? Answer: Down. So, when in doubt, look at lead V1 and use your turn signal. Simple!
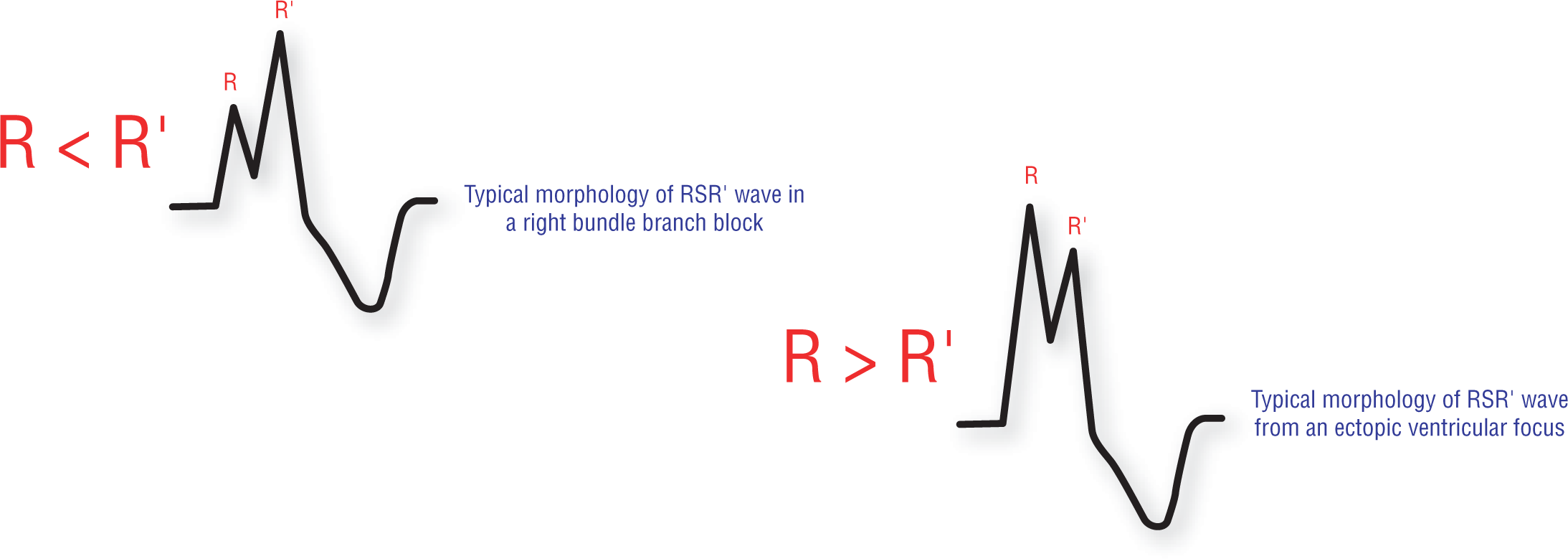
RBBB-Like Morphology in Lead V1-2. SVTs-A typically have a triphasic appearance of the RBBB pattern in lead V1, with an rsR′ pattern predominantly found. If the QRS complexes have an RBBB-like appearance (i.e., positive in lead V1), there are some additional clues to the possible presence of a VTach as the underlying rhythm. One of these additional clues relates to the height of the R′ wave.
Normally, in a patient with supraventricular complex and a BBB, the R′ is taller than the R wave (Figure 36-7). This is because the vector that causes the R′ is completely unopposed. Since there are no competing vectors that cancel out some of the amplitude, the R′ wave is almost always taller and wider than the R wave. In an ectopic ventricular complex, there is no rule as to whether the R or the R′ is taller. As a result of this discrepancy, we can state the following with some certainty: In a WCT with an RBBB-like morphology, the presence of R greater than R′ is highly suggestive of VTach.
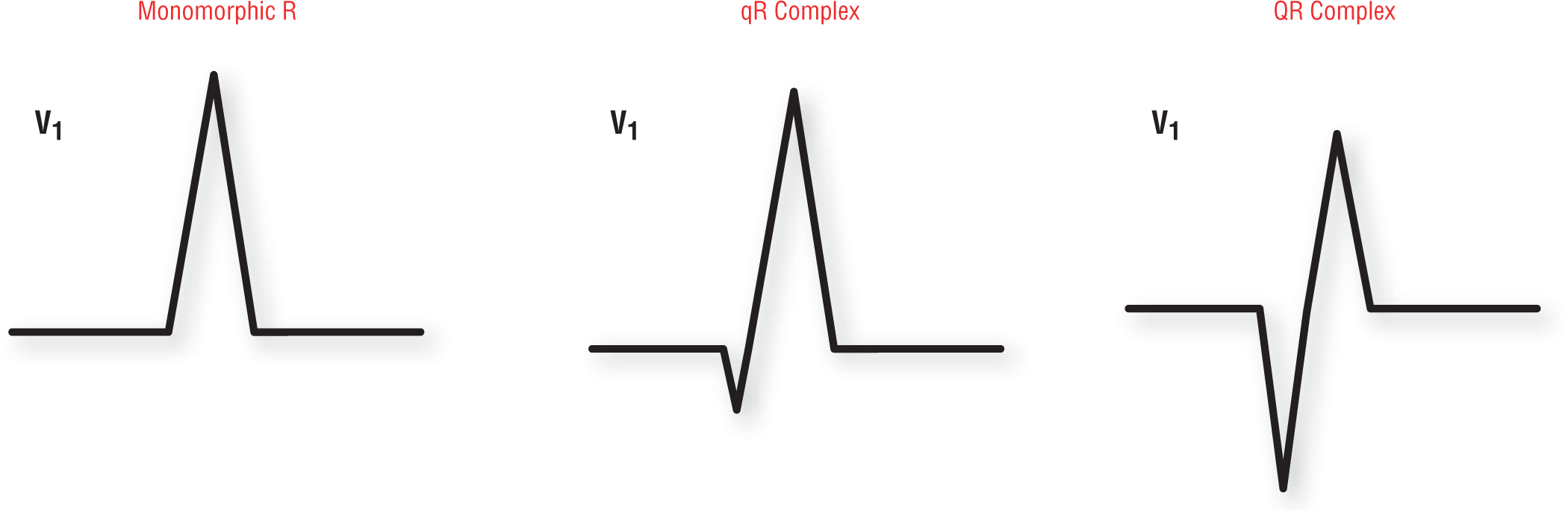
Some other things to look for include a monomorphic R, a qR, or a QR wave in lead V1 appearing in someone with a WCT with an RBBB morphology. These wave patterns are graphically represented in Figure 36-8. These findings are more commonly found in VTach than in patients with a wide-complex SVT.
Figure 36-8 Other morphologies to look for in a patient with wide-complex tachycardia and an RBBB morphology in lead V1.
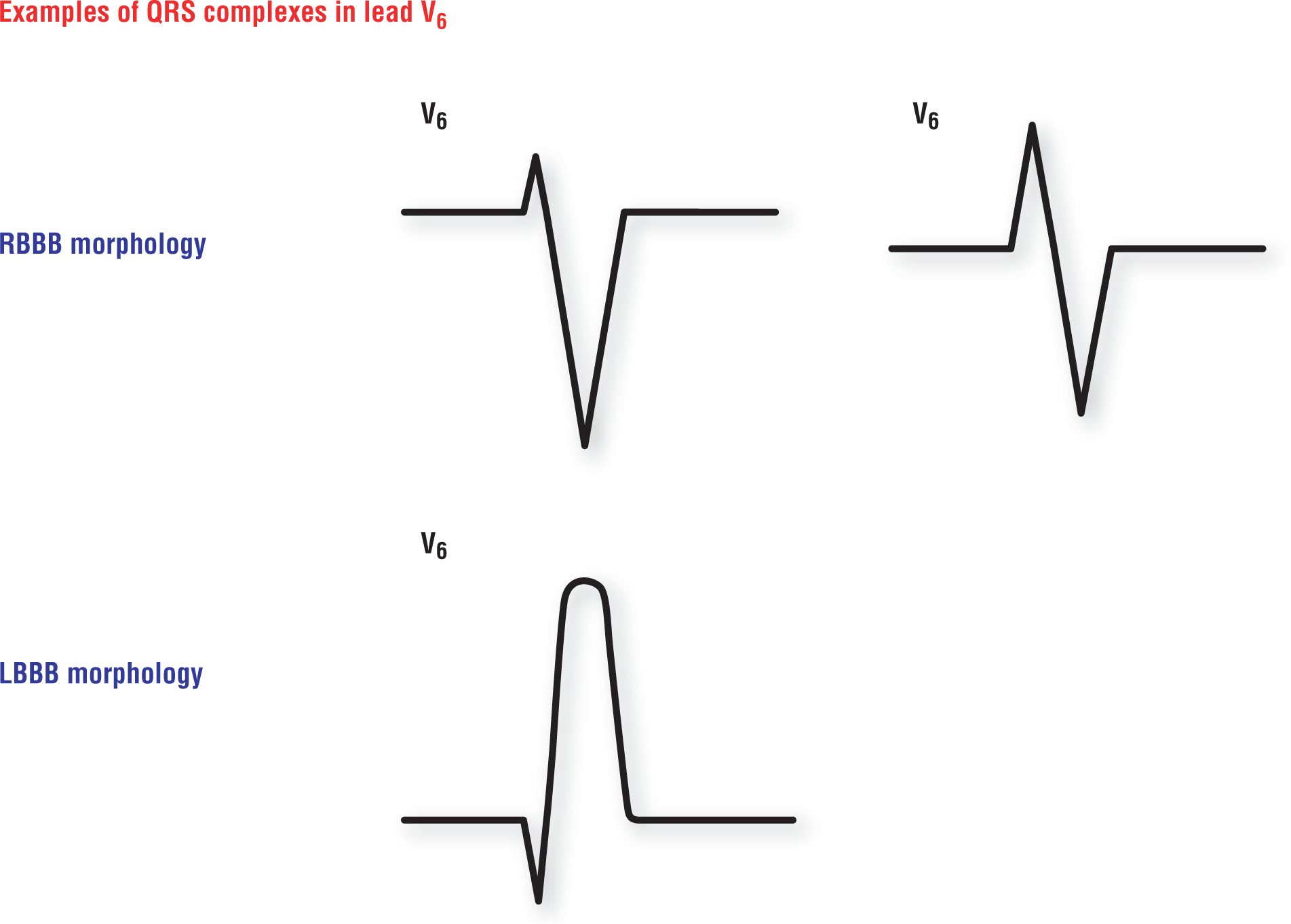
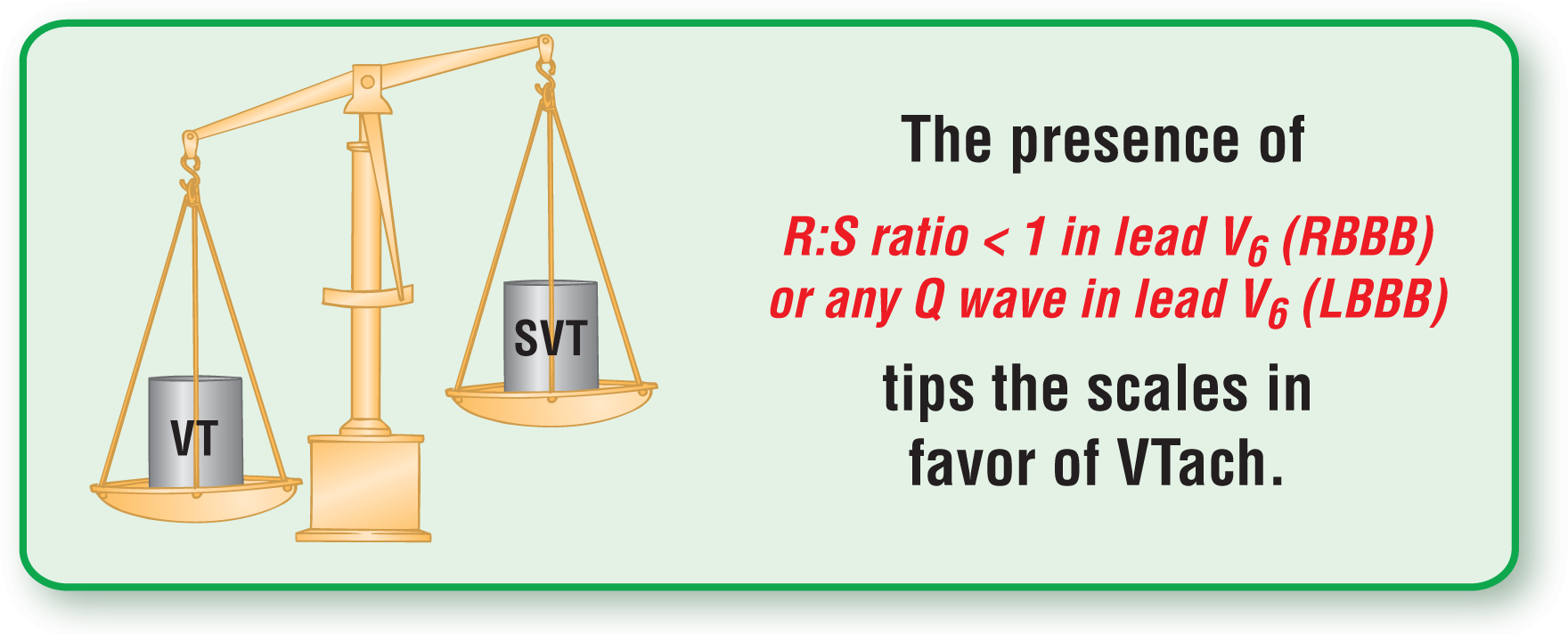
RBBB-Like Morphology in Lead V6. If the WCT has an RBBB morphology, the presence of an R:S ratio that is less than 1 in lead V6 can be indicative of a VTach. In other words, look at lead V6: If the S wave is deeper than the R wave is tall, there is a good chance it is VTach (Figure 36-9).
Figure 36-9 Morphologic appearances to look for in a patient with WCT and either an RBBB or LBBB morphology in lead V6.
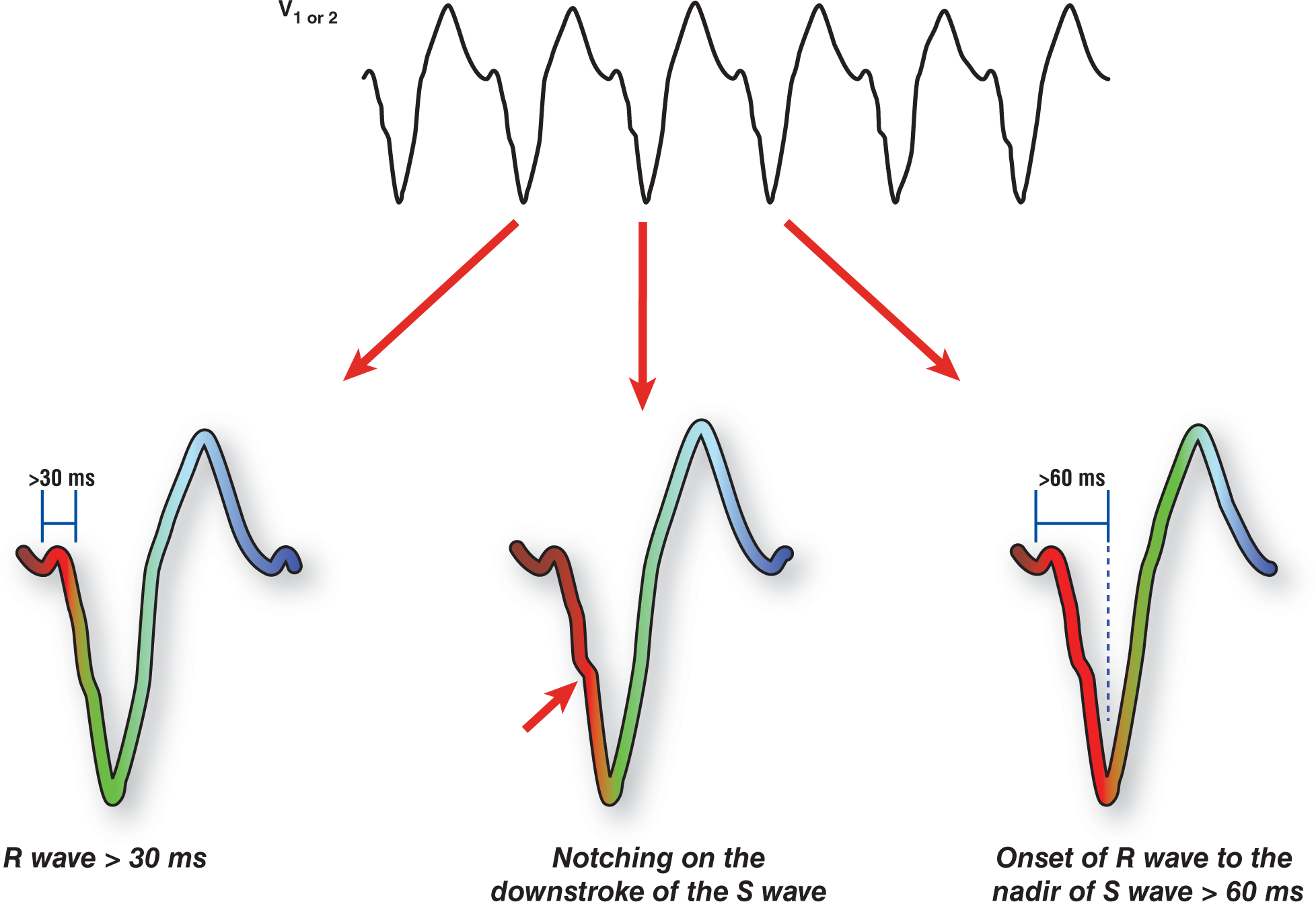
LBBB-Like Morphology in Lead V1-2. Dr. E. Kindwall and his associates,5 in their 1988 article, presented that if V1 or V2 shows an LBBB-like pattern, there are three considerations that will help guide you toward a diagnosis of VTach (Figure 36-10):
Figure 36-10 LBBB-like morphology in lead V1 or V2.
If you have broader-than-expected initial r waves of greater than or equal to 30 ms (0.03 seconds or ¾ of a small block), it points toward VTach.
If you have any notching or slurring of the downstroke of the S wave, it points toward VTach.
Measure the interval from the beginning of the r wave to the nadir (lowest point) of the S wave. If it is greater than 70 ms, it points toward a VTach.
LBBB Morphology in Lead V6. If the WCT has an LBBB-like morphology, the presence of any Q wave in lead V6 can be indicative of a VTach (Figure 36-9). Remember, LBBBs should be composed of a single monomorphic R wave in lead V6; therefore, there should never be any Q waves present in that lead.
INTERMEDIATE
Be extremely careful with this criterion, as Q waves could be found in a patient with LBBB and a lateral infarct. The Q wave, in these cases, would be indicative of the dead myocardium and scar formation in the lateral wall.
AUTHOR’S NOTE
Keep in mind that these findings are more common in patients with ectopic ventricular origins for their tachycardias. However, they are not diagnostic of VTach. In other words, these findings help to point your suspicions in the direction of VTach but do not make the diagnosis a certainty. Use them as another tool in your armamentarium. Remember to always interpret any arrhythmia based on all of the information, not just one or two isolated findings.
Morphology of the Associated PVCs
If the morphology of PVCs found in periods of normal sinus rhythm is identical to that of the WCT, then VTach is heavily favored. That is because most of the VTachs are monomorphic and originate from one ventricular pacing focus or reentry loop. Ventricular complexes originating from that single focus tend to produce complexes with an identical or nearly identical morphology.
As we saw earlier, identifiable PVCs that frequently occur during nontachycardic periods can provide a wealth of information that you can use to establish your diagnosis. If the morphology of the PVC is very similar or identical to the morphology of the wide complexes, then the rhythm is probably a monomorphic VTach. Unfortunately, this rule does not always hold true, as any PVC can cause a reentry circuit to be formed. However, this can be used as a good indicator of VTach.
AV Dissociation
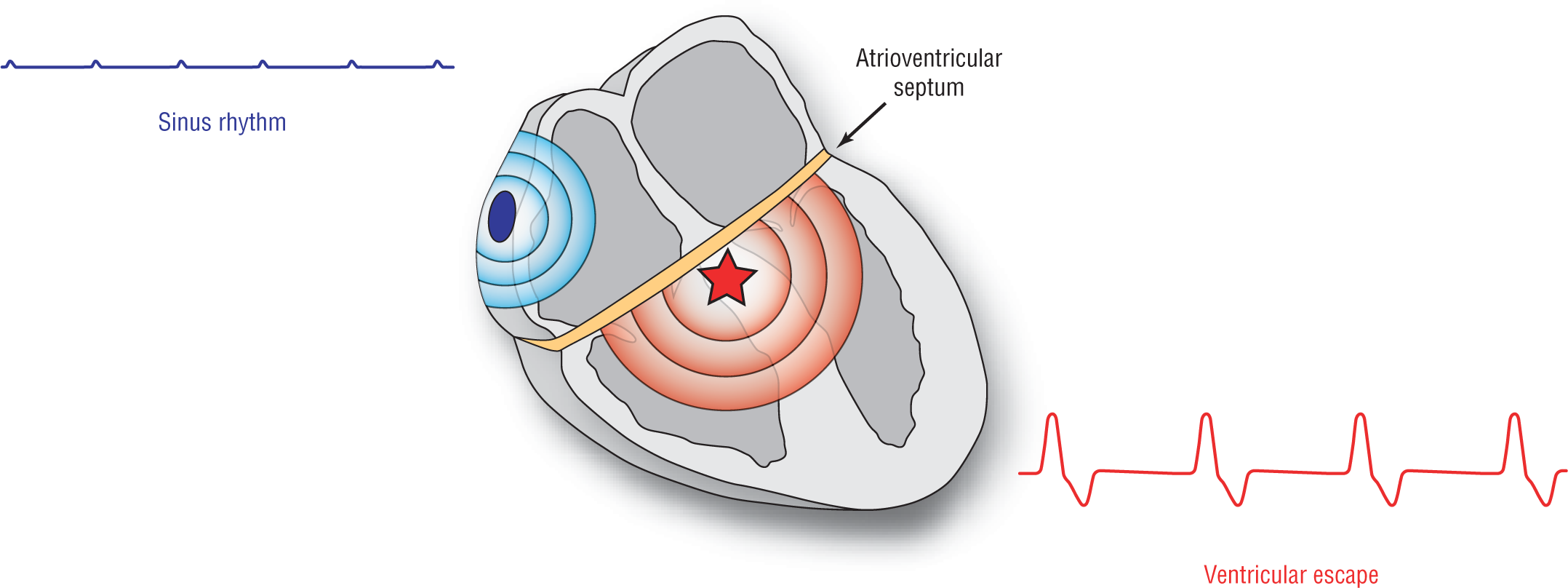
Electrocardiographically, a complete AV block develops because of a lack of communication between the atria and the ventricles. Essentially, the AV node shuts down all communication between them. The atrioventricular septum and the nonfunctional node essentially form an electronic barrier between the atria and the ventricles (Figure 36-11). The supraventricular pacemakers are, therefore, oblivious to occurrences in the ventricles and continue to fire normally to depolarize the atria. By the same token, the ventricular pacemakers, which are oblivious to occurrences in the atria, take over the pacing function for the ventricles as part of the fail-safe system, essentially creating their own ventricular rhythm. The net result is two separate rhythms occurring simultaneously. One is the regular sinus or any supraventricular rhythm, and the other one is of ventricular origin.
Figure 36-11 When the AV node is not conducting, it creates, functionally, a complete block at the level of the interventricular septum. The atria and the ventricles are completely oblivious to each other, and two separate pacemakers develop. Each pacemaker will keep its own intrinsic rate and control its respective chamber.
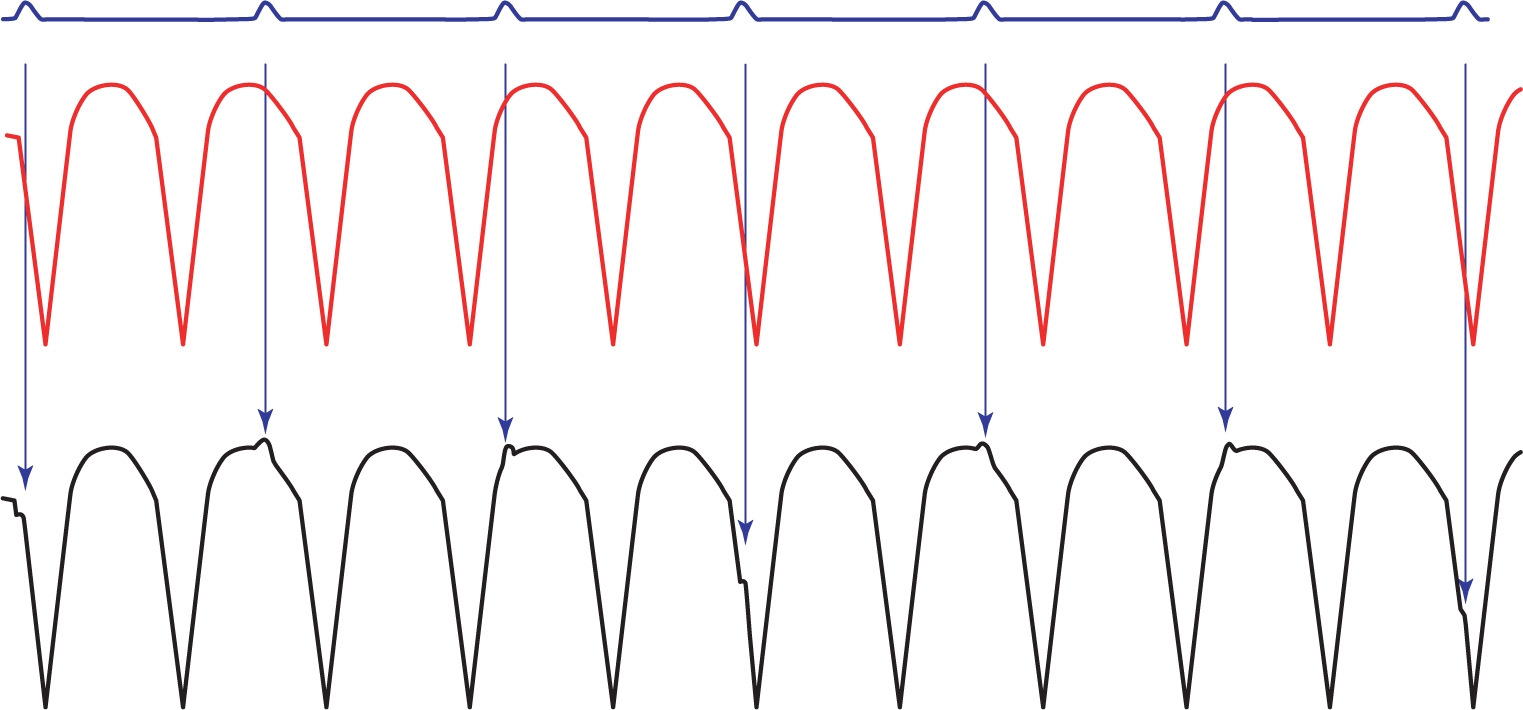
If the ventricles and the atria were completely noncommunicable, the atrial rhythm and the ventricular rhythm would still electrocardiographically fuse to form a VTach with P waves marching through it. But, in these cases the supraventricular rhythm would not affect the ventricular rhythm in any way. This can, and does, occur in many examples of VTach (Figure 36-12).
Figure 36-12 The atria and the ventricles are completely oblivious to each other and there are two separate pacemakers. Each pacemaker will keep its own intrinsic rate and control its respective chambers. The ECG fuses these two rhythms into one strip electrocardiographically (see strip in black). This is ventricular tachycardia with AV dissociation.
More commonly, instead of a complete block, the constant barrage from the rapid ectopic ventricular complexes created by a ventricular reentry circuit functionally close down the AV node by causing it to remain in an almost constant refractory state. In other words, the AV node will almost always be refractory to the supraventricular impulses because of the constant barrage from the ventricular complexes coming at it from below. In these cases, there can still be some form of communication between the atria and the ventricles because this is really not a pathologic AV node problem but a refractory or functional AV node problem.
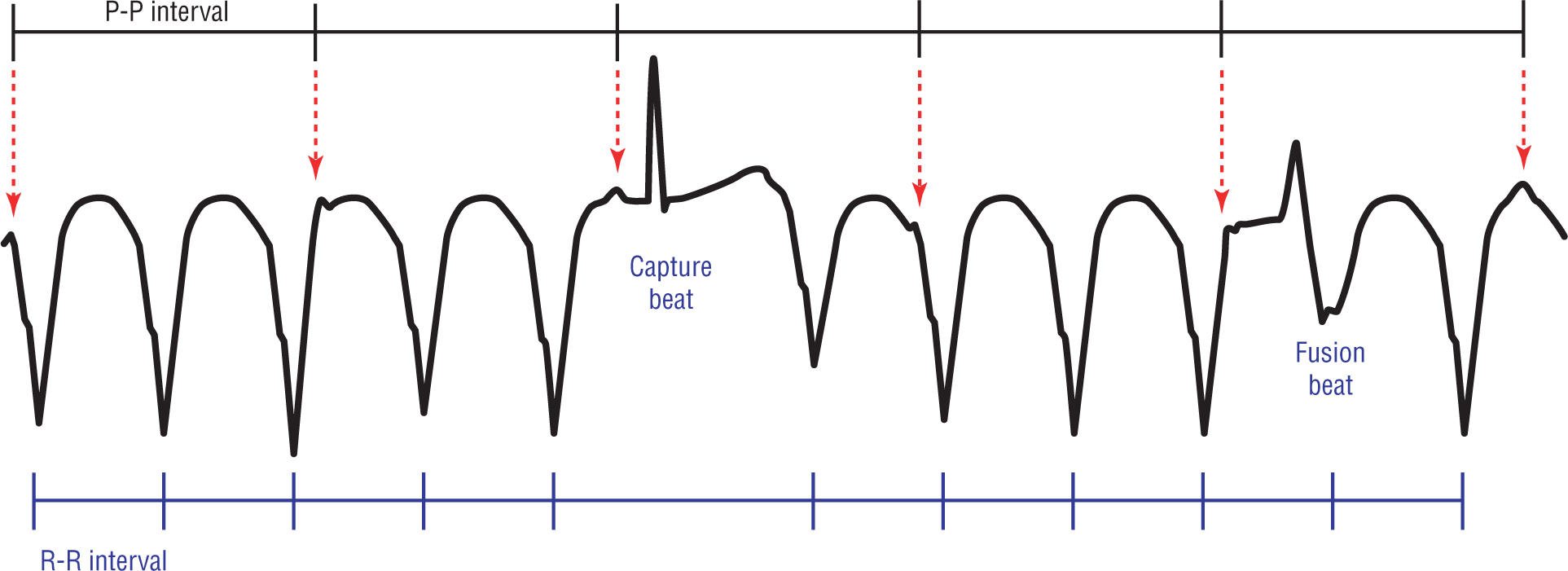
Since the AV node is still structurally normal (in most cases), an occasional supraventricular complex will reach the AV node during just the right millisecond and this one impulse will get through to completely capture the ventricles or cause a fusion complex (Figure 36-13). This type of partial communication between the atria and the ventricles is known as AV dissociation. The occasional transmission of a supraventricular impulse through the normal conduction system seen in AV dissociation is how capture beats and fusion complexes are formed.
Figure 36-13 Ventricular tachycardia is quite frequently associated with AV dissociation. Always look for P waves, capture beats, and fusion beats!
By definition, AV dissociation can never occur in the SVTs-A. That is because, under normal circumstances, the supraventricular rhythm controls the pace and regularity of the ventricular response. In fact, the name says it all: wide-complex supraventricular tachycardias with aberrancy. In the WCTs, the QRS complexes will always be wide either due to aberrancy or because they originate from a ventricular origin.
As we saw in Chapter 32, Ventricular Tachycardia, pages 518 to 519, AV dissociation is typically found because the atrial rates and ventricular rates are different, leading to different numbers of P waves and QRS complexes. As a matter of fact, the ventricular pacemaker is always faster (more QRS complexes) than the supraventricular pacer (P waves), as you would expect in a VTach. In fact, the higher ratio of QRS complexes to P waves found in AV dissociation is the most specific ECG feature for a VTach. The AV dissociation also leads to differences in the various intervals (P-P, R-R, and PR); the presence of a variable PR interval should always alert you to the possibility of AV dissociation when dealing with any WCT.
The presence of AV dissociation is the most powerful predictor of VTach. AV dissociation is found in approximately 20% to 50% of all VTachs and has a specificity approaching 100%.6 More importantly, as mentioned, it is not found in SVTs-A at all. The presence of AV dissociation is considered direct evidence for a VTach.
Indirect evidence of the presence of VTach also includes capture and fusion beats. The presence of either of them in a WCT is very highly suggestive of a VTach. Let’s do a quick review on these topics.
Capture Beats
Remember we mentioned that in AV dissociation some small amount of connection remained between the atria and the ventricles? Well, when a P wave falls directly in the right sweet spot, it can trigger normal conduction through the ventricles and the formation of a normally appearing, narrow QRS complex. The way capture beats typically present is that there will be a string of wide-QRS complex beats with a breakthrough narrow P-QRS-T complex falling somewhere along the run (see Figure 36-13). These complexes are typically found interspersed along the strip, but usually they do not appear sequentially. They are, however, associated with fusion complexes before and/or immediately after the capture beat.
The QRS complexes in capture beats are narrow because the P wave captures the ventricle and conduction occurs through the ventricles using the normal His-Purkinje system (HPS). Rapid conduction through the HPS always leads to narrow complexes. Finally, we’d like to reiterate that this phenomenon doesn’t happen on every complex, just the ones in which the P waves fall at just the right moment.
Fusion Beats
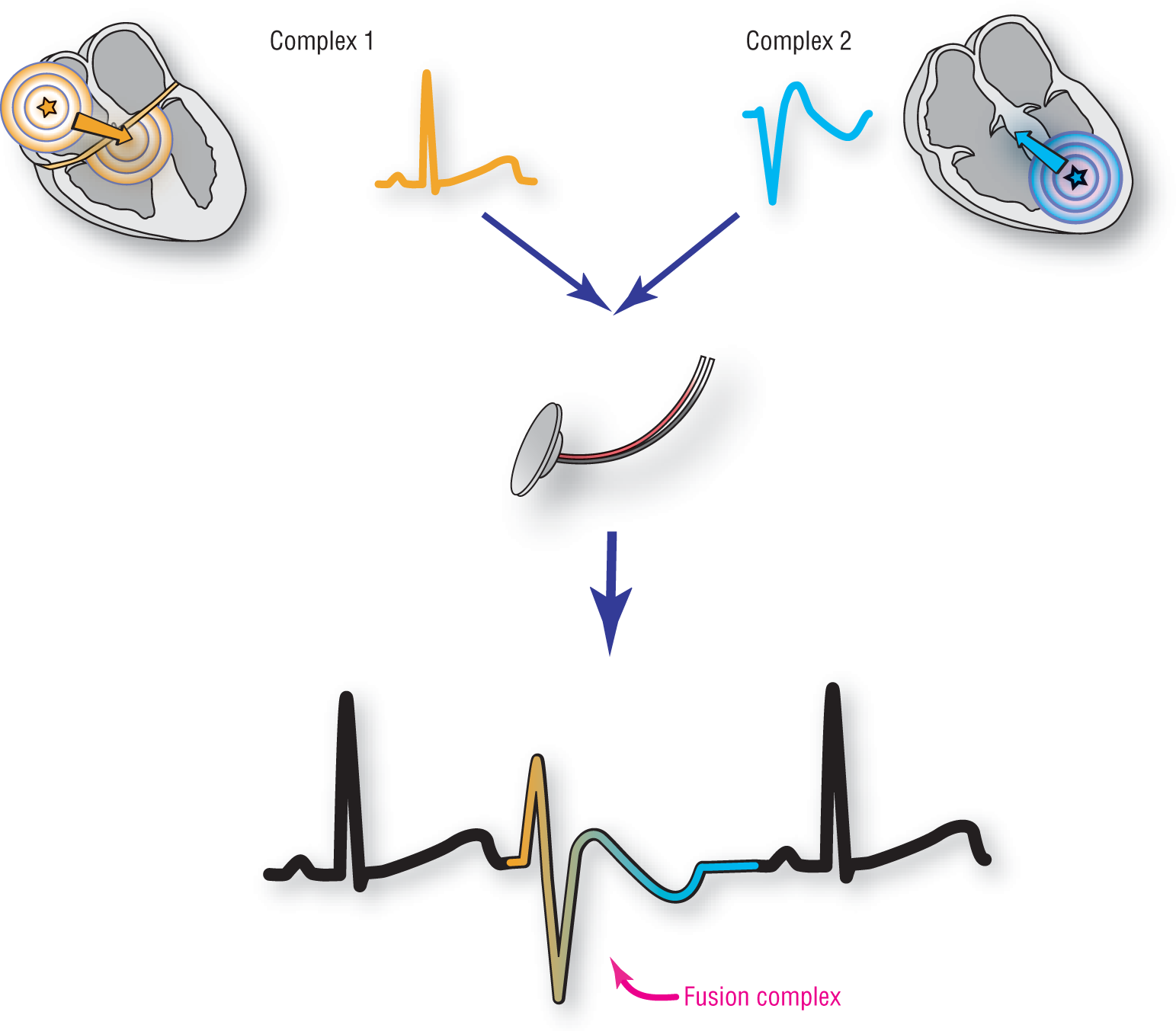
Fusion beats occur when you have two beats occurring simultaneously or almost simultaneously, causing the depolarization of the ventricles to occur from two different origins and directions. Usually, one of the complexes is triggered by a supraventricular focus and the other from a ventricular focus. The net result is that both of these waves occur at the same time and the ECG machine fuses their electrical vectors, morphing them into a totally different appearance than either of the parent waves (Figure 36-14).
Figure 36-14 Complex 1 is a supraventricular complex being normally transmitted to the ventricles. This complex would give rise to a nice, tight QRS complex. Complex 2 originates in an ectopic ventricular focus and will give rise to an aberrant, wide QRS complex. The ECG machine translates these bits of electrical information into the fusion complex below. Note that the resulting complex resembles both parent complexes slightly.
It’s good to think of fusion complexes through the eyes of genetics. The two parent organisms both have their own distinctive features and appearances. Each parent passes a number of genes to the offspring. Depending on how much of each gene is expressed, the offspring could look similar to one or the other of their parents, or could look like a mix of the two. Notice we said “similar” and not identical, because the offspring never have the parents’ exact genetic makeup. That is why the fusion complex will never have the exact, identical appearance of either the ventricularly paced complex or the capture beat (see Figure 36-13).
In many cases, however, the presence of AV dissociation is very difficult to spot on an ECG. The finding is commonly missed since the various waves can be fused, buried, or just simply hidden within other events. In addition, remember to look for the indirect evidence of AV dissociation in the form of capture and fusion beats. An example of a typical VTach with AV dissociation is shown in Figure 36-13. Always have a high index of suspicion for any WCT that has small areas of localized morphologic variation occurring at various points along the strip. Always use your calipers and try to map out everything. If the disturbances are found with a recurrent interval, you are probably dealing with an AV dissociation.
Concordance of the QRS Complexes in the Precordial Leads
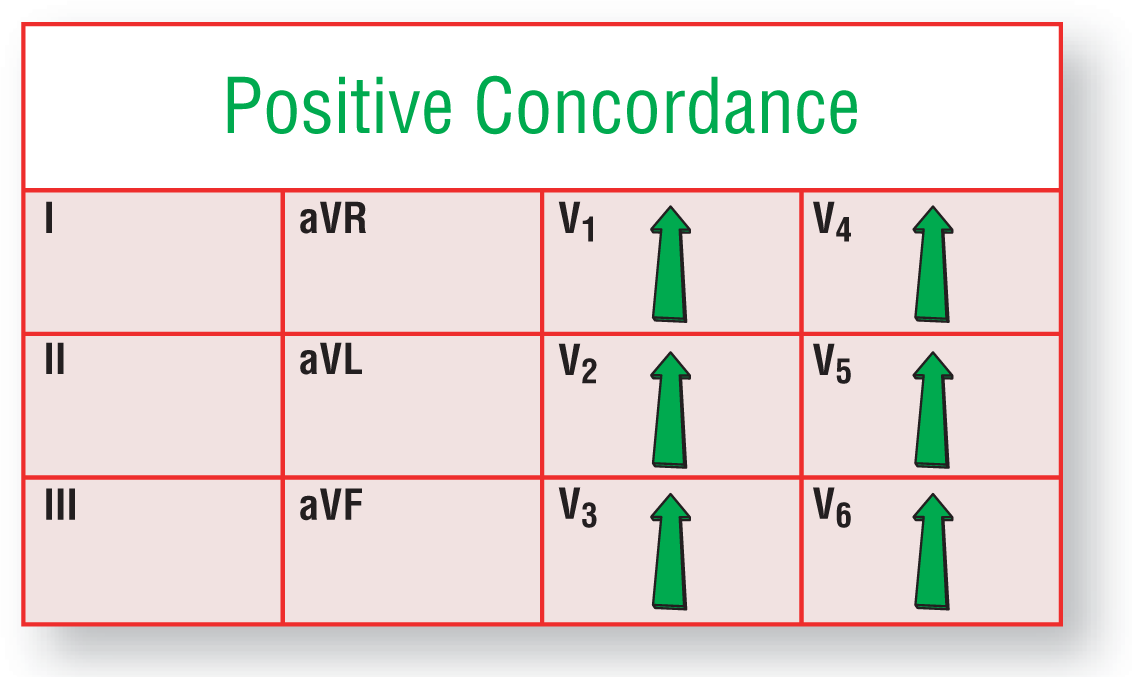
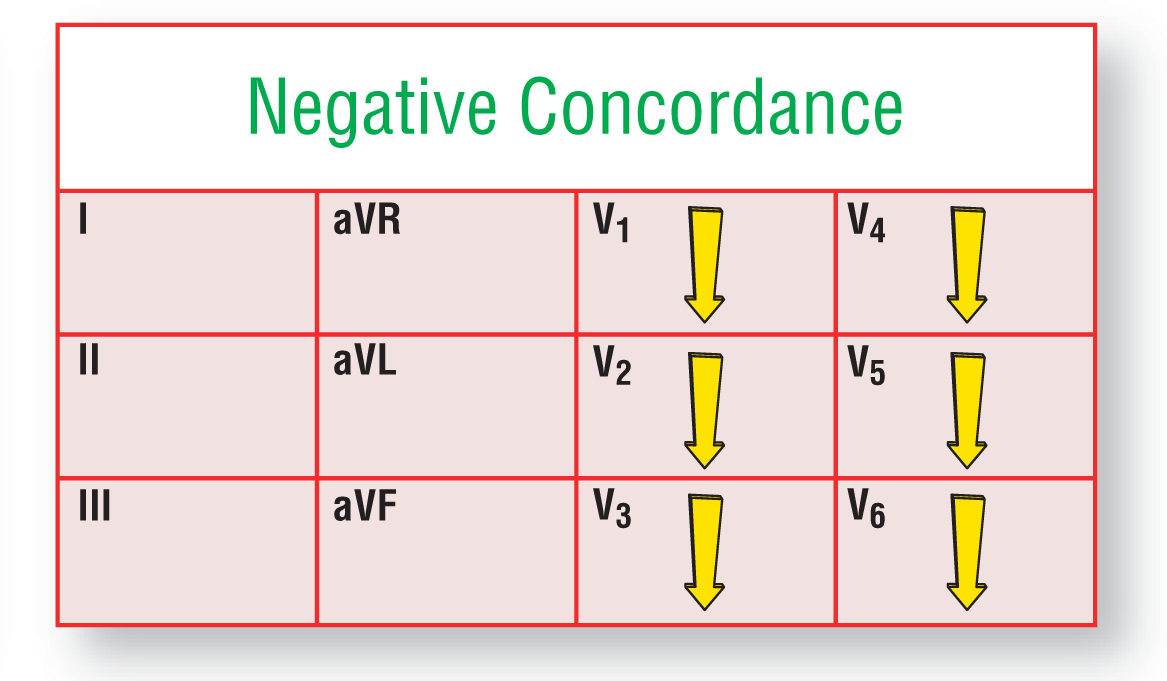
Concordance of the QRS complexes in the precordial leads refers to the presence of monophasic, wide QRS complexes in the precordial leads (V1 to V6) that all have the same polarity or direction. To put it a bit more simply, the QRS orientation is either all positive or all negative in the precordial leads. To continue, however, some critical criteria must be met. The monomorphic, wide QRS complexes must all be positive, tall, single R waves in all the precordial leads (Figure 36-15) or all negative, deep, single QS waves in all the precordial leads (Figure 36-16). You cannot have some tall ones and some deep ones or any combination of RS or QR waves anywhere in any of the precordials. If you have any of these combinations, the criteria for concordance are not met.
Figure 36-15 Positive concordance in ventricular tachycardia.
Concordance is found in approximately 15% of VTachs, so you probably won’t see it too often. However, if your strip is in that lucky 15% that does show it, the presence of concordance gives you a 90% specificity that you are dealing with a VTach. To make it simpler for us non-statisticians, if concordance is present, you have a 90% certainty that the WCT is a VTach. If you don’t have it, just move on. A word of advice: Never try to con yourself or anyone else into seeing something that is not actually there; the price of doing that is more than anyone can afford.
ADVANCED
To complicate matters a bit more, concordance is also found in antidromic AVRT. We mention this here because, normally, it is almost impossible to differentiate an antidromic AVRT from VTach on a regular surface 12-lead ECG. In these cases, we need to focus on the “company it keeps” and remember that 80% to 90% of WCTs are VTach.1-5 Always be vigilant in searching for any history or evidence of preexcitation or an accessory pathway.
Big J: I’ll take VTach versus SVT-A for $1,000, Alex.
Alex: Can QRS concordance occur if ventricular conduction occurs via the normal His-Purkinje system?
Big J: What is, “No way, Big A!”
Alex: Judges? . . . Can you elaborate on that for us, J?
Big J: Of course, Alex. The thing is, when conduction occurs via the normal HPS, you form at least three different vectors as a result of ventricular depolarization, each associated with its own magnitude and direction (see Chapter 8, Normal Sinus Rhythm, pages 123 to 124, Cycles 8 to 10). The placement of the electrodes along the chest wall sense any vector formed, regardless of its direction. Since vectors created using the normal HPS cannot be heading toward or away from all the precordial sensors at the same time, the polarity of all the QRS complexes in all the precordial leads cannot be either all positive or all negative. In other words, some vectors will head toward an electrode and lead to positive deflections, while at the same time other electrodes will see the same vector as heading away from it, recording the events as negative deflections. Therefore, some leads have to be positive, some are negative, and some are a combination of both, forming either RS or QR complexes, for example.
Since VTach originates in either a ventricular focus or reentry circuit, the resulting depolarization wave (vectors) heads outward from the initiating pacemaker. Therefore, depending on the location of the pacing site, a situation can develop that creates vectors heading either toward or away from the precordial electrodes. That is how concordance can be created.
Positive concordance typically occurs when the pacer is in the base of the heart, causing a depolarization wave to travel anteriorly and slightly leftward toward the apex. The direction of the resultant vectors allows for some component of the vector to always travel toward each of the precordial leads, hence positive deflections and positive concordance.
Negative concordance occurs when the depolarization wave travels from a pacemaker originating at the apex to head upward and to the back of the base of the heart. The direction of these vectors, therefore, leads away from the precordial electrodes and creates the negative deflections and negative concordance to appear on the 12-lead ECG.
INTERMEDIATE
Abnormal Axis Deviation
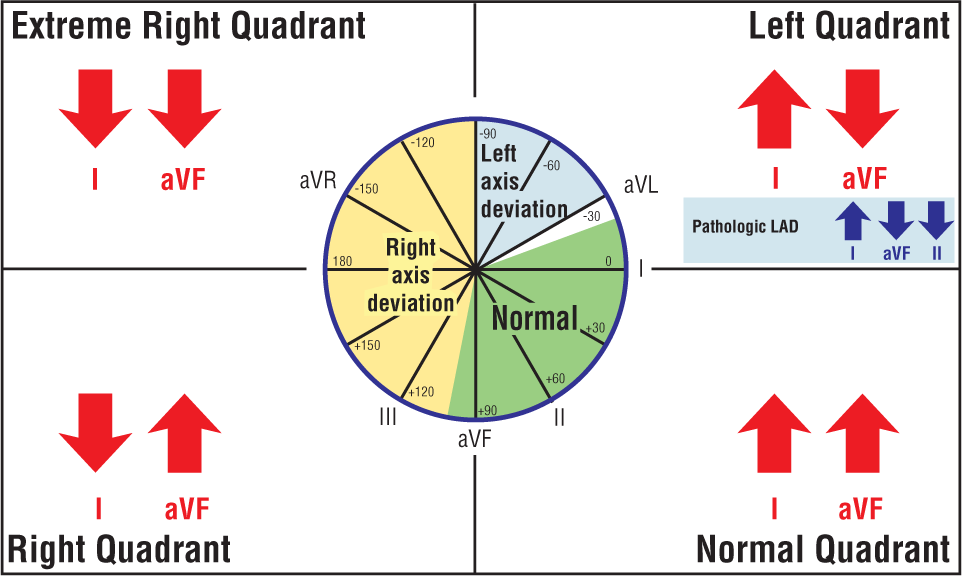
We discussed the electrical axis and how to roughly but quickly calculate it in Chapter 5, Introduction to 12-Lead ECGs, pages 67 to 70 and in the Additional Information box titled Axis Direction and Ventricular Tachycardia in Chapter 32, Ventricular Tachycardia, on page 521. As a brief review, the normal QRS axis is usually found between –30° and +90°. A left axis is considered present if the axis points between –30° and –90°. A right axis is between +90° and +180°. There is only one axis quadrant left, the extreme right quadrant (from –90° to –180°). This quadrant also goes by the names of northwest axis or “no man’s land” to indicate how uncommonly the axis lands in that quadrant (Figure 36-17).
Figure 36-17 An axis is found to be in the extreme right quadrant when the QRS complexes are negative in both leads I and aVF.
In general, WCTs that have their electrical axis in the normal, right, or left quadrant favor the diagnosis of SVT-A. If the axis lands in the extreme right quadrant, however, VTach is favored. The simple way to find out if your axis falls within the extreme right quadrant is to take a look at leads I and aVF. If the complexes are negative in both of those leads, the axis will be in the extreme right quadrant.
As a special note, when you are dealing with an LBBB pattern with a right axis deviation in a WCT, you are usually dealing with a VTach. It makes sense because the LBBB pattern can be created only if the depolarization wave starts from the right and moves leftward. A right axis deviation means that the major electrical forces of the heart are traveling rightward. Since these two presentations typically cannot occur at the same time, you must be dealing with a VTach.
Hemodynamic Status
Hemodynamic instability and signs of hypoperfusion can occur in either SVTs-A or VTachs. Although hemodynamic instability is typically seen in VTach, complete hemodynamic stability can also occur. Always keep in mind that the underlying cardiac status and the rate are the two most important determinants of the hemodynamic status for any patient. For that reason, the hemodynamic status of the patient should not be used to rule in or rule out the presence of a VTach. We can, however, state that hemodynamic instability does point us in the direction of VTach.
A patient who is hemodynamically stable with a WCT, with or without myocardial damage, is typically misdiagnosed as having a benign SVT. This is one of the most common and deadly clinical mistakes made in the evaluation of the WCTs. Patients with WCTs should always be considered true medical emergencies, as they can present in severe hemodynamic compromise or can decompensate into one within seconds. They always require your immediate attention.
Your priority in managing these patients is to ensure their hemodynamic stability first, and then worry about whether their WCT is a VTach or not. Words you don’t want to overhear when you go to the hospital: (1) “Oops!” (when muttered by a surgeon in an operating suite) and (2) “Great pickup on that strip, Dr. LaMorte! Shame you couldn’t get back in time to defibrillate him after you figured it out.”
Additional Information
Relative Hypotension
We would be negligent if we did not talk briefly about a particular clinical event: relative hypotension. Blood pressure is needed by the body to perfuse the organs and maintain life. In general, the patient should have blood pressure within the normal range. Hypertensive patients develop thickening of their arterial walls to maintain the high pressures needed to perfuse their organs. These patients can usually tolerate some very high levels during their normal everyday activities.
Elevated blood pressure is needed to maintain normal perfusion in these patients because of the thickened arterial walls. Because of that arterial thickening, what is normal for the average individual and what is normal for hypertensive patients are two different things. A blood pressure of 120/80 mm Hg is smack in the middle of the normal range. But, in a hypertensive patient, this same blood pressure may not be enough to adequately perfuse the organs, leading to cell and organ death. This situation is what we mean by relative hypotension.
Relative hypotension is the discrepancy that can occur for any given patient between the clinical signs and symptoms of hypoperfusion while being relatively normotensive. This condition is why you should never treat the number, but treat the patient. If the patient appears hemodynamically unstable, despite a normal-looking blood pressure, ask quickly about the patient’s resting blood pressure. If the patient is normally hypertensive, he or she could be relatively hypotensive. These patients should be treated as if they were hemodynamically compromised because they are hemodynamically compromised. Always use your clinical judgment when treating any patient!
ADVANCED
Other Adjuncts to the Diagnosis of WCT
Pharmaceutical Adjuncts
As we have mentioned repeatedly, the failure to correctly identify a VTach is the biggest danger in the evaluation of any WCT. Part of that danger is that diagnostic trial or treatment of a patient with verapamil or diltiazem for either VTach or a preexcited atrial fibrillation could lead to catastrophic hemodynamic compromise secondary to the formation of very rapid and uncontrollable ventricular rates or ventricular fibrillation. It is best to avoid those medications until you have clearly established what rhythm you are dealing with.
Likewise, it is important to remember that Class 1C drugs are associated with proarrhythmic effects that could alter the appearance of the rhythm or even worsen the situation. Once again, try to avoid these drugs in the emergent phase if at all possible or use them as diagnostic adjuncts unless you are sure of what you are dealing with.
You should approach any patient with a prolonged QT with extreme care when administering any drug that could potentially prolong the interval further. Remember, it is easier to treat normal sinus rhythm with a prolonged QT than a polymorphic VTach or torsade de pointes. A list of drugs that prolong QT can be found at the CredibleMeds website (www.crediblemeds.org).7 Bookmark the site now so you can access it quickly.
Adenosine, on the other hand, can be given safely as a diagnostic tool if you are dealing with a regular, monomorphic rhythm. The drug is typically hemodynamically well tolerated (although you should still be prepared for any outcome!) and may actually terminate the rhythm in some cases.
A great general rule to approach the pharmaceutical adjuncts is to treat every WCT as if it is a known VTach. You can never go wrong with that concept foremost in your mind. For further reading and current treatment guidelines, please refer to the 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients with Supraventricular Tachycardia.8
Electrophysiology Adjuncts
We will not spend much time on this topic, as it is beyond the scope of this text. It is important, however, that if there is any doubt as to the diagnosis or treatment of the WCTs, the patient should always be referred to a cardiologist who specializes in electrophysiology. Cardiac mapping and other studies will often be needed to fully evaluate a patient with life-threatening arrhythmias, and you should never hesitate to involve these resources early in the management of such patients.