The digestive system has its own means of preparing and disposing of the wastes from what we consume — but what about the wastes our body creates itself? This is the role of the urinary system.
In this chapter, we take you on a tour of the urinary system, reveal the makeup of urine, explain how the kidneys help your body maintain homeostasis, and look at some of the problems that affect the urinary system.
Functions of the Urinary System
Most of the waste products of cellular metabolism and many other substances exit your body via your urinary system. Urine is the body’s primary waste product, and urination (the release of urine to the environment) is the final step of metabolism.
Doing the dirty work: Metabolic wastes are toxic and would cause harm to the cell if they were allowed to accumulate inside. Cells continuously excrete their wastes into the surrounding fluid. As this extracellular fluid is absorbed into the capillaries, the waste substances enter the blood. While carbon dioxide is excreted via respiration (see Chapter 10), other wastes (byproducts of cellular metabolism) stay in the blood. The kidneys remove these toxic byproducts from the blood and put them in our urine (see the section “Putting out the trash: Kidneys” later in this chapter).
The term excretion can mean the movement of material from the inside to the outside of a cell, as well as to the release of material from the inside to the outside of the body.
Making and expelling urine:Urine is a watery solution produced by your kidneys. It’s the means through which the waste products of metabolism are removed from the blood and eliminated from the body. Urine also helps maintain the chemical equilibrium of the blood because harmful substances can be purposefully dumped there. The fluid is then transported and held in the bladder until it is released.
Balancing water content: Around half of your body weight is water, contained in intracellular (inside the cell) and extra cellular fluid (outside the cell).Your kidneys precisely regulate the release and retention of water in order to maintain blood volume and its chemical composition. In other words, they maintain the homeostasis of the blood (see the “Maintaining Homeostasis” section later in the chapter).
Performing endocrine functions: The adrenal glands sit atop the kidneys, but they’re an independent organ. They produce numerous hormones, including some that influence the kidneys:
Regulating RBC production: The hormone erythropoietin, which stimulates RBC (red blood cell) production (erythropoiesis) in the bone marrow, is produced in the kidney (and liver). Erythropoietin also has other physiological functions related to wound healing and recovery (flip to Chapter 9 for information on blood cell production).
Regulating bone growth:Calcitriol, the physiologically active form of vitamin D, is synthesized in the kidneys. Calcitriol regulates, among other things, the concentration of calcium and phosphate in the blood, which promotes the healthy growth and remodeling of bone (Chapter 5 has more on bone growth).
Regulating blood pressure: The kidneys also produce renin, a hormone involved in the renin-angiotensin system (RAS) that works to increase blood pressure. This is discussed in detail in the “Fluid Balance and Blood Pressure” section later in this chapter.
Structures of the Urinary System
The urinary system is quite compact. Unlike some other organ systems, you can identify the point where it begins and another point, not too far away, where it ends. See the “Urinary System” color plate in the center of the book.
Like the alimentary canal, the urinary system is essentially a system of tubes through which a substance passes, undergoing a series of physiological processes as it does so. The familiar tissue layers — an outer fibrous covering, a muscular layer, and a mucous layer lining the interior surface — are seen throughout the urinary system, beginning at the ureter. The mucus protects the tissues from the urine, which is slightly acidic.
Putting out the trash: Kidneys
The urinary system begins with the kidneys, fist-sized paired organs, reddish-brown in color, located just below the ribs in your lower back. The kidney is shaped like an elongated oval; actually, it’s shaped just like a kidney bean. (Coincidence?) The inner curve of the kidney is called the hilum where a number of vessels enter or exit, including the ureter, renal artery, renal vein, lymphatic vessels, and nerves. A connective tissue membrane called the peritoneum, as well as adipose (fat) tissue, attach your kidneys to your posterior abdominal wall. (The term renal comes from the Latin “ren,” meaning “kidney.”)
Beneath the peritoneum, a lining of collagen called the capsule encloses the kidney. Fibers of this layer extend outward to attach the organ to surrounding structures.
The kidneys are retroperitoneal. That is, they attach to the posterior side of the abdominal cavity’s lining, on the outside of the cavity. Your back muscles on either side of your vertebral column help to protect your kidneys, as do your lowest ribs. Still, a hard blow to the back can damage a kidney fairly easily.
Renal blood supply
Some blood from the abdominal aorta is diverted into the renal blood supply. The renal artery brings blood to the kidney for filtering. The renal vein drains filtered blood out of the kidney, emptying it into the inferior vena cava. The kidneys receive about 20 percent of all blood pumped by the heart each minute.
Kidney tissues
Under the capsule, the kidney’s various tissues are arranged in more or less concentric layers. The outermost layer, just beneath the capsule, is the cortex. Beneath the cortex is the medulla, a series of fan-shaped structures, called renal pyramids, alternating with the renal columns. The spaces between each pyramid, the columns, allow blood vessels through to reach the cortex. The pyramids are comprised of microscopic tubes that drip urine into saclike structures. The innermost layer contains these sacs and is called the renal pelvis, which channels the urine into the ureter. See the “Kidney and Nephron” color plate in the middle of the book to see the locations of these structures.
Nephron
Microscopic in size (about a million of them exist in each kidney), the nephron is the kidney’s filtration unit. Each nephron has two parts: the renal corpuscle and the renal tubule. The renal corpuscle also has two parts: the glomerulus (plural, glomeruli), a special kind of capillary bed derived from arterioles branching from the renal artery, and the glomerular capsule (or Bowman’s capsule), a double-walled epithelial cup that partially encloses the glomerulus.
Leading away from the corpuscle, the nephron loops up, forming the proximal convoluted tubule, or PCT. The tube then straightens, pushing down into the medulla and looping up again (the loop of Henle). At the top, it loops again into the distal convoluted tubule (DCT). This tubule connects to a collecting duct that carries the urine through the renal pyramids into the renal pelvis.
The nephrons are surrounded by the peritubular capillaries, which perform an important role in direct secretion, selective reabsorption, and the regulation of water. See the “Selectively reabsorbing” section later in the chapter, and take a look at the “Kidney and Nephron” color plate in the middle of the book to see the nephron’s individual parts.
Make sure you keep the kidney capsule and the glomerular capsules straight. The kidney has one kidney capsule on the outside and a million microscopic glomerular capsules inside.
Holding and releasing
Fortunately, we have a storage tank for our urine over which we have voluntary control. When urine exits the kidneys, it is transported for storage until it is transported for release. This part of the urinary system, called the urinary tract, begins at the top of the ureter and ends with the urethra.
Ureters
The ureters are tubes that transport the urine from a kidney to the bladder. The ureter emerges from the renal pelvis.
The walls of the ureter are similar in structure to those of the intestines: The muscular layer contracts in waves of peristalsis to move urine from the kidney to the bladder.
Bladder
The bladder is a hollow, funnel-shaped sac into which urine flows from the kidneys through the ureters. The bladder has a capacity of about 20 ounces (about three-fifths of a liter). It lies in the pelvic cavity, just behind the pubic bones and centered in front of the rectum. In females, it’s in front of the uterus.
Like other organs in the urinary and digestive systems, the bladder is made up of an outer protective membrane, several layers of muscles arranged in opposing directions, and an inner mucosal layer. The muscle layers contract to expel urine into the urethra. The mucosa is made up of a special kind of epithelial tissue called transitional epithelium in which the cells can change shape from cuboidal to squamous to accommodate larger volumes of urine (see Figure 12-1). Stretch receptors in the muscle layer send impulses to the brain when the bladder is becoming full. Flip to Chapter 3 for more details about epithelial tissue.
Illustration by Kathryn Born, MA
FIGURE 12-1: Transitional epithelium lines the bladder.
Urethra
The urethra is the tube that carries urine from the bladder to an opening (orifice) of the body for elimination. The mucosa (epithelium) of the urethra is composed of transitional cells as it exits the bladder. Farther along are stratified columnar cells, followed by stratified squamous cells near the external urethral orifice.
The male and female urethrae are adapted to interact with the respective reproductive systems and therefore differ from each other in some aspects of anatomy and physiology.
In both males and females, a sphincter at the proximal end of the urethra (between the bladder and the urethra) keeps urine in the bladder. This ring of smooth muscle, called the internal urethral sphincter, is under the control of the autonomic nervous system. It opens to release urine into the urethra for urination.
Where the urethra passes through the pelvic floor, there’s another sphincter made of skeletal muscle, called the external urethral sphincter, which is under voluntary control.
Female urethra: In females, the urethra is about 1.5 inches (3.8 centimeters) long. It runs along the anterior wall of the vagina and opens between the clitoris and the vaginal orifice (opening). The external sphincter is located just inside the exit point.
Male urethra: In males, the urethra is about 8 inches (20 centimeters) long, from the bladder to its opening at the tip of the penis, called the urethral meatus. The male urethra is divided into three named sections, based on anatomical structures:
The prostatic urethra contains the internal sphincter and passes through the prostate. Openings in this region allow for sperm and prostatic fluid to enter into the urethra during orgasm.
The membranous urethra contains the external sphincter. It is only about 1 inch (2.5 centimeters) in length.
The cavernous urethra, or spongy urethra, runs the length of the penis, ending at the urethral meatus.
The Yellow River
Urine is a bodily fluid with specific functions, just like blood and lymph. But unlike those, you see urine in the normal course of everyday events. Here’s everything you always wanted to know about how it gets to be its own sweet self.
Composition of urine
Urine is about 95 percent water, in which many wastes are dissolved. These include urea, other nitrogenous (nitrogen-containing) and various other compounds including electrolytes (ions). Its odor comes from ammonia and other substances derived from ammonia, like urea. See Table 12-1 for more about the nitrogenous components of urine.
TABLE 12-1 Nitrogenous Components of Urine and Their Sources
Nitrogenous Component
Source
Urea
A byproduct of the breakdown of amino acids
Creatinine
A byproduct of the metabolism of creatine (present in large quantities in muscle cells, used to make ATP)
Ammonia
A byproduct of the breakdown of proteins
Uric acid
A byproduct of the breakdown of nucleic acids
Urine is yellow because it contains urobilinogen, a compound formed from the breakdown of red blood cells (see Chapter 9). The normal color range of urine is some shade of yellow, from nearly clear to dark amber, depending mostly on the level of hydration. When you’re abundantly hydrated, lots of water goes into the urine, making it more diluted and therefore paler. When you’re less than optimally hydrated, the kidneys put less water into the urine. The urine becomes more concentrated and appears darker.
Ingested food, beverages, and pharmaceutical products influence the composition of urine. Urine contains hippuric acid, produced by the digestion of fruits and vegetables, and ketone bodies, produced by the digestion of fats. Some foods, beverages, and drugs impart color and odor to urine. Some physiological conditions and disorders affect the composition of urine, and urine has long been analyzed for diagnosis. For example, glucose in the urine is a sign of diabetes.
Filtering the blood
The renal corpuscle, which contains the glomerulus (capillaries) and the glomerular capsule, is the area of interface between the cardiovascular system and the kidney. That’s where your body filters blood.
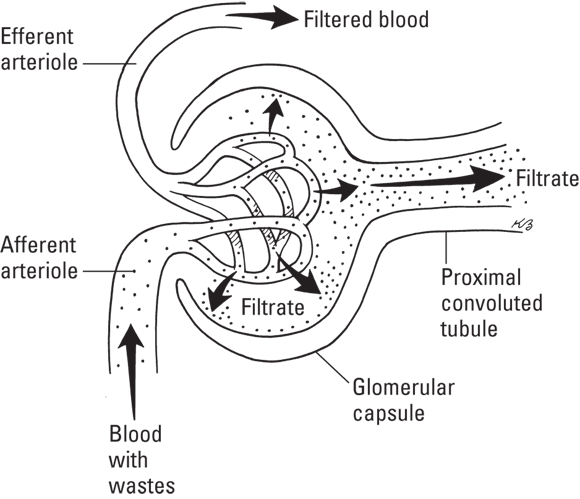
Blood enters the glomerulus via the afferent arteriole. Now in the glomerular capillaries, the plasma is forced out and caught by the capsule; this process is called glomerular filtration. The blood pressure in these capillaries is higher than in other capillaries, and it pushes the blood up against the glomerular wall with some force. The blood remaining in the capillaries exits the glomerulus via the efferent arteriole and continues on its path through the kidney.
The thin, permeable wall of the glomerulus acts as a filtration membrane. Plasma passes through into the capsule, bringing along small-molecule solutes, including wastes and toxins like urea and creatinine and useful small-molecule substances like glucose, amino acids, and electrolyte ions. The plasma captured by the capsule, now called filtrate, is then routed into the nephron (see Figure 12-2).
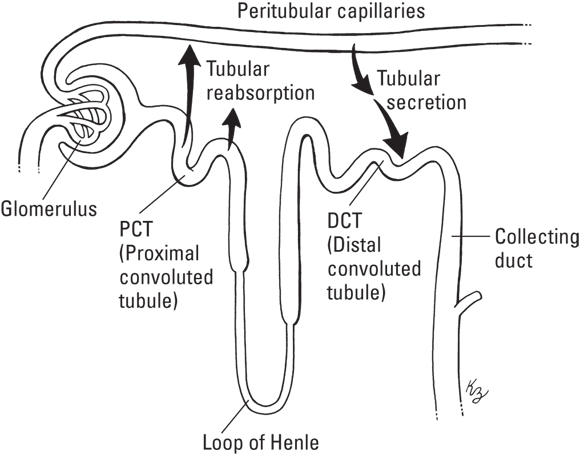
Now, many of the wastes are in the filtrate instead of the blood. Unfortunately, so are some molecules we’d like back, such as glucose, amino acids, and electrolytes. Additionally, since about 7 liters of water are pushed out during glomerular filtration every hour, we better get most of it back because we couldn’t possibly consume enough to replace it. The main role of the nephron is to get all those things back into our blood while leaving the wastes in the filtrate to be excreted as urine. As you read through this next section, refer to Figure 12-3 to help guide you.
Microvilli line the nephrons, increasing the surface area within the tubule where substances can enter and leave the filtrate. This is also why the tubules are so convoluted. More surface area means more opportunities to get substances in or out.
PCT
On its journey through the nephron, the filtrate first enters the proximal convoluted tubule (PCT). Here, the main goal is tubular reabsorption — that is, we want to pull out water and other useful molecules from the tubule so they can be placed back into the bloodstream. There are pumps along the PCT that actively transport water and ions into the cortex of the kidney. Here, the peritubular capillaries can reabsorb them.
Loop of Henle
The filtrate then continues into the loop of Henle (nephron loop). The main goal here is water retention. Positive ions, such as sodium are pumped out and chloride ions follow. The two ions bond to form a salt, making the fluid surrounding the nephron into a hypertonic solution (see Chapter 2). As a result, water leaves the loop of Henle via osmosis and is, again, reabsorbed by the peritubular capillaries.
Water cannot be directly moved from one place to another. Our bodies do not have a means to target it. However, water readily performs osmosis — moving to where there is lower concentration (less water). We can pump specific ions into an area, and ions can form salts, so we can encourage water to follow. Increasing the solute concentration of the interstitial fluid of the medulla decreases water concentration in that area, thus water flows out of the nephron.
DCT
Now, the filtrate enters the distal convoluted tubule (DCT). The reabsorption of water can occur here as well, but the main goal is tubular secretion. Some of the metabolic wastes, hydrogen ions, are too numerous to be filtered out at the glomerulus. Others, such as proteins like histamine, are too large. These wastes are still in our blood even after glomerular filtration. As a result, pumps along the peritubular capillaries target these wastes — secreting them from blood flow and into the DCT.
Collecting duct
Finally, the filtrate enters the collecting duct. This is our last chance to get water out of the filtrate and back into our blood. Whatever is left, now urine, drips down the duct (through the medulla) and into the renal pelvis.
The amount of water reabsorbed from the filtrate back into the blood depends on the hydration situation in the body. However, even in cases of extreme dehydration, the kidneys produce around 16 ounces (about half a liter) of urine per day just to excrete toxic waste substances. Numerous other substances are returned to the blood at specific points, conserving them and maintaining the blood’s chemical environment. Over 99 percent of the filtrate produced each day can be reabsorbed.
The terms “tubular reabsorption” and tubular secretion” can easily be misinterpreted. It’s not what the tubes are doing. Remember the perspective — we care about the blood. We reabsorb from the tubules and secrete into them.
Expelling urine
The urine that drips down the nephron’s collecting ducts enters into the renal pelvis. From there, it moves along the ureter and into the bladder. As the urine accumulates, the pressure receptors in the lining send signals to the brain. The first message is sent when the bladder is about half full (around 6 to 8 ounces, or 177 to 237 milliliters). At a volume of 12 ounces (354 milliliters), the messages become stronger, and it becomes difficult to control the external urethral sphincter.
When the time is right to empty the bladder, the brain sends an impulse through the autonomic nervous system to open the internal urethral sphincter and contract the bladder muscles. Urine flows out of the bladder, through the urethra, and out of the body. This process is known as micturition.
Maintaining Homeostasis
The chemistry of life, stunningly complex and precise, requires a tightly controlled environment to proceed optimally. The kidneys, under hormonal control, are key organs for maintaining the homeostasis of blood and other body fluids. The endocrine system has a huge range of subtle and interacting mechanisms for controlling kidney function. (See Chapter 8 for more on the endocrine system.)
Fluid balance and blood pressure
Aspects of fluid balance that involve the blood include blood volume and the amount and nature of the electrolytes in the plasma. These factors are linked, as we discuss in the following sections.
Blood volume (water content)
Blood volume is an important factor in circulation. The greater the blood volume, the harder the heart must work to pump the blood and the greater the pressure in the arteries. The less the blood volume, the lower the blood pressure, decreasing the amount of resources that reach the tissues. A low blood pressure will also weaken the pressure filtration in the glomeruli. However, the urinary system, when functioning properly, maintains blood volume. It does so by actually controlling electrolyte concentrations to influence water movement either into or out of the blood, even if that requires putting some strain on other systems.
The adult body contains about 23 pints (11 liters) of extracellular fluid, constituting about 16 percent of body weight, and about 6 pints (almost 3 liters) of plasma, constituting about 4 percent of body weight. Blood plasma and extracellular fluid are very similar chemically and, in conjunction with intracellular fluid (fluid inside the cells), help control the movement of water and electrolytes throughout the body. Some of the important ions found in interstitial fluid (fluid outside of the cells but within the tissues) are: Na+, K+, Cl–, and Ca2+.
Hormonal mechanisms to control blood volume
The renin-angiotensin system (RAS) (also called the renin-angiotensin-aldosterone system [RAAS]) is called into action when stretch receptors in the kidney sense low blood pressure — especially in the glomerulus. Specialized kidney cells secrete the enzyme renin, which sets off a series of reactions in different organ systems, eventually resulting in the production of the hormone angiotensin II, a powerful vasoconstrictor. When the diameter of the blood vessels decreases (vasoconstriction), blood pressure increases. This keeps the blood circulating, giving the kidneys time to solve the volume problem.
Angiotensin II also triggers the secretion of the hormone aldosterone from the adrenal cortex, which causes Na+ to be reabsorbed from the nephrons into the blood. Where salt goes, water follows. The movement of water into the blood increases the blood volume. This, along with the vasoconstriction, raises blood pressure and thus restores the effectiveness of the glomerular filtration.
Some medications for hypertension (high blood pressure) act by blocking the production of the enzyme that leads to the production of angiotensin II. These are the so-called angiotensin-conversion-enzyme inhibitors (or ACE inhibitors). Without angiotensin II, no vasoconstriction takes place, and the kidneys don’t receive the signal to increase the water content of the blood.
Furthermore, the pituitary gland is stimulated by angiotensin II to secrete ADH (anti-diuretic hormone). Sodium is reabsorbed by the nephrons but not enough water follows, so ADH causes more water to be reabsorbed from the collecting duct, which decreases the amount of urine and helps maintain normal blood volume and pressure.
Atrial natriuretic peptide (ANP) hormone is a peptide hormone secreted by heart muscle cells in response to signals from sensory cells in the atria that blood volume is too high. ANP prevents the kidneys from secreting renin. In fact, the overall effect of ANP is to counter the effects of the RAS. It acts to reduce the sodium reabsorption in the kidney. This leads to more water being released in the urine, thereby reducing blood volume and, thus, pressure.
Regulating blood pH
The homeostatic range for blood pH is narrow; the optimum value is around 7.4. Alkalosis (increase in alkalinity) is life-threatening at 7.8. Acidosis (increased acidity) is life-threatening at 7.0. To maintain the blood pH within its homeostatic range (7.3 to 7.4), the kidney can produce urine with a pH as low as 4.5 or as high as 8.5.
Neutral pH is 7.0, the value for water.
While the body has buffers circulating in the blood to resist pH changes, acids and, to a lesser extent, alkalis (bases) are byproducts of metabolic processes. The digestion of fats produces fatty acids. The carbon dioxide produced by cellular respiration can form carbonic acid if it reacts with water. Muscle activity produces lactic acid. Some acids are ingested in food and drink. The kidneys respond to changes in blood pH by excreting acidic (H+) or basic (OH–) ions into the urine.
Your body has buffering processes in which the kidneys are involved. A buffer is a type of chemical that binds with either acid or base as needed to increase or decrease the solution pH. Buffers are made in cells and available in the blood.
Three mechanisms work together to maintain tight control over blood pH:
Minor fluctuations in pH are evened out by the mild buffering effects of substances always present in the blood, such as the plasma proteins.
When sensors in the kidneys detect that the blood is too acidic, they induce the breakdown of the amino acid glutamine, releasing ammonia, a basic substance, into the blood. When the ammonia arrives at the kidney, it’s exchanged for Na+ in the urine and eliminated.
By far the most important buffer for maintaining acid-base balance in the blood is the carbonic-acid-bicarbonate buffer. The body maintains the buffer by eliminating either the acid (carbonic acid) or the base (bicarbonate ions). Carbonic acid concentration can be reduced within seconds through increasing respiration — the excretion of carbon dioxide through the lungs increases pH. Bicarbonate ions must be eliminated through the kidneys, a process that takes hours.
The pH scale measures the concentration of hydrogen ions (H+) in a solution. The scale ranges from 0 (extreme acidity, high concentration of hydrogen ions) to 14 (extreme alkalinity, low concentration of H+, and consequently, high concentration of OH–). Solutions with balanced amounts of these two components have a pH in the neutral range.
Pathophysiology of the Urinary System
When things go wrong in the urinary system, the healthy functioning of the entire body is affected.
Kidney pathologies
The kidney is a complex and delicate organ, crucial to physiology but vulnerable to injury. Because of the kidneys’ importance in homeostasis, kidney problems can be underlying problems in other disorders, especially those of the circulatory system.
Calculating kidney stones
The proper name for a kidney stone is a renal calculus, meaning “pebble” or “hard.” A kidney stone is literally a little pebble made from common waste molecules in the urine. A common cause of kidney stones is chronic dehydration. When urine is more concentrated, solutes, such as uric acid, tend to precipitate (fall out of a solution and clump together). Crystals of uric acid may develop into kidney stones, or they may travel to your joints, causing gout (turn to Chapter 5 for more about gout). Small stones, up to about 0.1 inch (.3 centimeters) diameter, can flow more or less quietly out through the urinary tract. Larger stones can cause considerable pain, sometimes for several days, when passing, and sometimes damage the ureters or urethra. The largest stones, 0.3 inch (.8 centimeters) or greater, frequently become impacted — lodged in the urinary tract and unable to be passed through the urine stream. An impacted kidney stone may cause a backup of urine in the kidney, ureter, bladder, or urethra (see the “Urinary tract obstruction” section later in the chapter) and requires medical intervention.
Alcohol hangover
Among its many physiological effects, alcohol inhibits the release of ADH from the pituitary gland. As we discuss earlier in the chapter, ADH regulates the kidney’s action in restoring water to the blood. Without ADH, too much water is excreted in the urine, and blood volume falls below the optimum range. The resulting dehydration causes dizziness, headache, and other symptoms associated with a hangover. Homeostatic mechanisms will restore fluid balance over a period of hours after the consumption of alcohol ceases. So, no matter what remedies you’ve heard, the only cure for a hangover is rehydrating yourself.
Urinary tract pathologies
Obstructions, blockages, and colonization by life forms with their own agendas plague all tubal systems, biological and inanimate. At least your body can fight back against these threats to the smooth flow of urine in the urinary tract.
Urinary tract obstruction
The urinary system’s various tubes are vulnerable to an obstruction that blocks the flow of urine. The smaller the tube, the greater the risk of obstruction. The obstructing object is sometimes a stone (see the “Calculating kidney stones” section earlier in the chapter). Impacted kidney stones require immediate medical attention to avoid the risk of infection or more severe kidney damage.
Urinary tract infection
The urinary tract is subject to infection, known as UTI. Numerous pathogenic bacteria are adept at entering the body through the external opening of the urinary tract (urethra) and establishing infection in any structure of the urinary system. A bladder infection is known as cystitis, a kidney infection is pyelonephritis, and a urethra infection is urethritis.
UTIs are very noticeable and uncomfortable, so patients often seek treatment immediately, before the infection spreads higher up into the urinary system. The kidney is particularly vulnerable to damage from invading bacteria. If the pathogen is able to invade the bloodstream through the close connection with the kidney, the infection, then called septicemia, can be extremely serious. Septicemia can lead to septic shock, which can be life-threatening.
Urethral blockage
As men age, the prostate gland enlarges, usually starting around age 50. If the prostate gland enlarges too much, it can press on the urethra and block the flow of urine. The blockage can lead to UTIs in men, and it often causes painful urination (technically called dysuria). As the bladder becomes stressed from the blocked urethra, urine may leak out, or, more commonly, the urge to urinate becomes more frequent and sudden.
Incontinence across the continents
Incontinence is the inability to control the release of urine. There are four types of incontinence:
Stress incontinence: Urine leaks out when pressure is put on the bladder, such as when a person runs, coughs, lifts something heavy, or laughs. This type is relatively common among women who have given birth (vaginally) because the muscle supporting the bladder weakens and the sphincter muscle of the urethra stretches.
Urge incontinence: Also called overactive bladder, this type of incontinence is a sudden involuntary contraction of the bladder’s muscular wall that brings on an urgent need to urinate, possibly accompanied by a sudden release of urine. Often, these contractions occur regardless of the amount of urine in the bladder. This condition affects about 1 in 11 adults, particularly older adults. Underlying causes may be nervous system diseases, bladder tumors, bladder infection, and bladder irritation.
Overflow incontinence: In this condition, patients never feel the urge to urinate, the bladder never empties, and small amounts of urine leak continuously. This type is prevalent in older men with an enlarged prostate and is rare in women. The upper portion of the urethra passes through the prostate, so when the gland becomes enlarged, it may obstruct the passage of urine through the urethra.
Total incontinence: Some structural problems, spinal injuries, or diseases can cause a complete lack of bladder control. The sphincters of the bladder and urethra don’t operate, and urine flows directly out of the bladder.
 Understanding what the urinary system does
Understanding what the urinary system does The term excretion can mean the movement of material from the inside to the outside of a cell, as well as to the release of material from the inside to the outside of the body.
The term excretion can mean the movement of material from the inside to the outside of a cell, as well as to the release of material from the inside to the outside of the body. The kidneys are retroperitoneal. That is, they attach to the posterior side of the abdominal cavity’s lining, on the outside of the cavity. Your back muscles on either side of your vertebral column help to protect your kidneys, as do your lowest ribs. Still, a hard blow to the back can damage a kidney fairly easily.
The kidneys are retroperitoneal. That is, they attach to the posterior side of the abdominal cavity’s lining, on the outside of the cavity. Your back muscles on either side of your vertebral column help to protect your kidneys, as do your lowest ribs. Still, a hard blow to the back can damage a kidney fairly easily.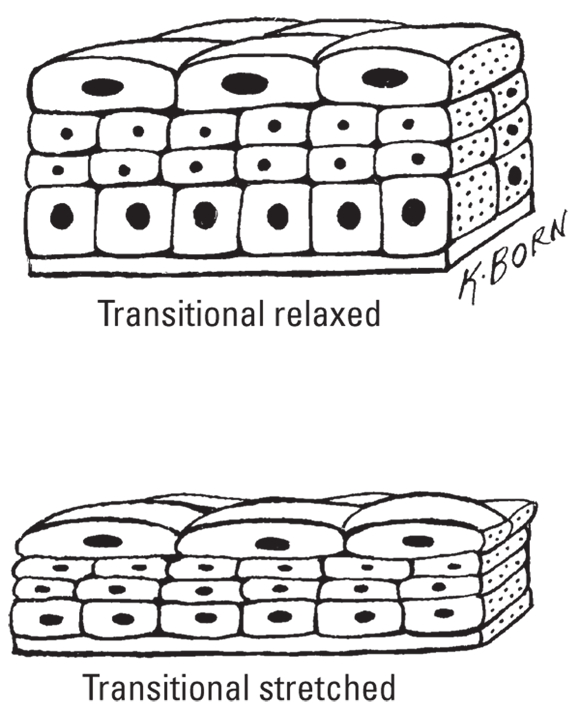
 The terms “tubular reabsorption” and tubular secretion” can easily be misinterpreted. It’s not what the tubes are doing. Remember the perspective — we care about the blood. We reabsorb from the tubules and secrete into them.
The terms “tubular reabsorption” and tubular secretion” can easily be misinterpreted. It’s not what the tubes are doing. Remember the perspective — we care about the blood. We reabsorb from the tubules and secrete into them.